
Abstract
Introduction
Autologous iliac crest bone grafting (ICBG) is the gold standard for pediatric alveolar cleft repair.1,2 The most common techniques for pediatric ICBG harvest are the conventional open technique and minimally invasive trephine harvest.3–5 Despite reports of surgeon and institutional preferences, evidence-based consensus on the outcomes of these techniques does not exist.
Trephine harvest of ICBG in the adult population has been well studied, 4 and several pediatric centres have adopted this technique. Reported benefits include shorter surgical time with a smaller incision, shorter time to ambulation and discharge, and decreased postoperative opioid use.3–5 Within a pediatric group, it is unclear whether this technique achieves sufficient volume of cancellous bone, if there is a notable risk of visceral organ damage, and whether the donor morbidity is comparable to open techniques.1,6–8
Our institution has recently developed a novel clinical care pathway for pediatric alveolar cleft repair. As part of this process, we sought to identify the optimal surgical approach for ICBG harvesting. A systematic review was conducted, comparing the use of trephine to conventional open ICBG harvest in pediatric patients undergoing alveolar cleft repair.
Methodology
A systematic review was conducted as per Preferred Reporting Items for Systematic Review and Meta-Analyses principles (PRISMA) specifications. 9 MEDLINE, EMBASE, and Scopus databases were searched on January 24, 2021. Manuscripts were included if they compared open to trephine ICBG harvest in a pediatric population (Defined as a mean study age under 18), undergoing alveolar cleft repair. Exclusion criteria were review articles, case series, commentaries, editorials, abstracts, and articles with a focus on adult populations. Search terms were created with the assistance of a medical librarian (H.L.R.). (Full MEDLINE search terms in Appendix 1). Two investigators independently reviewed all citations for selection for full-text review (A.R.T. and S.F.).
Data were organized based on outcome variables selected a priori, including patient demographics, operative time, time to unassisted ambulation, length of hospital stay, postoperative pain control and pain scores, volume of bone harvested, use of bone supplements, and complications. Quantitative results were not amenable to meta-analysis due to heterogeneity in outcome reporting. As such, ranges of the selected outcome values were reported based on the minimum and maximum of the means reported in each study. Analysis was organized into three themes: (i) donor site morbidity; (ii) volume and type of harvested bone; and (iii) safety.
Results
Of 422 manuscripts initially screened, five studies were ultimately included in the analysis (Figure 1: PRISMA flow diagram).5,10–13 Reasons for exclusion of full-text reviewed articles were: Non-ABG patient population (3), Case Study (1), Technical descriptor/no comparison (6), Alternative minimally invasive technique (3), Alternate grafting technique (1). Of the papers reviewed, they included 257 patients; 116 patients underwent conventional open harvest and 141 patients underwent trephine harvest. The average of the mean reported ages was 11.5 years in the trephine group (range 6.5-30 years), and 11.1 years in the open (range 6-25 years). The open technique included 74 patients with unilateral clefts and 45 patients with bilateral clefts (total 164 sites for grafting). Trephine groups included 88 patients with unilateral clefts, and 56 patients with bilateral clefts for a total of 200 sites (Table 1).
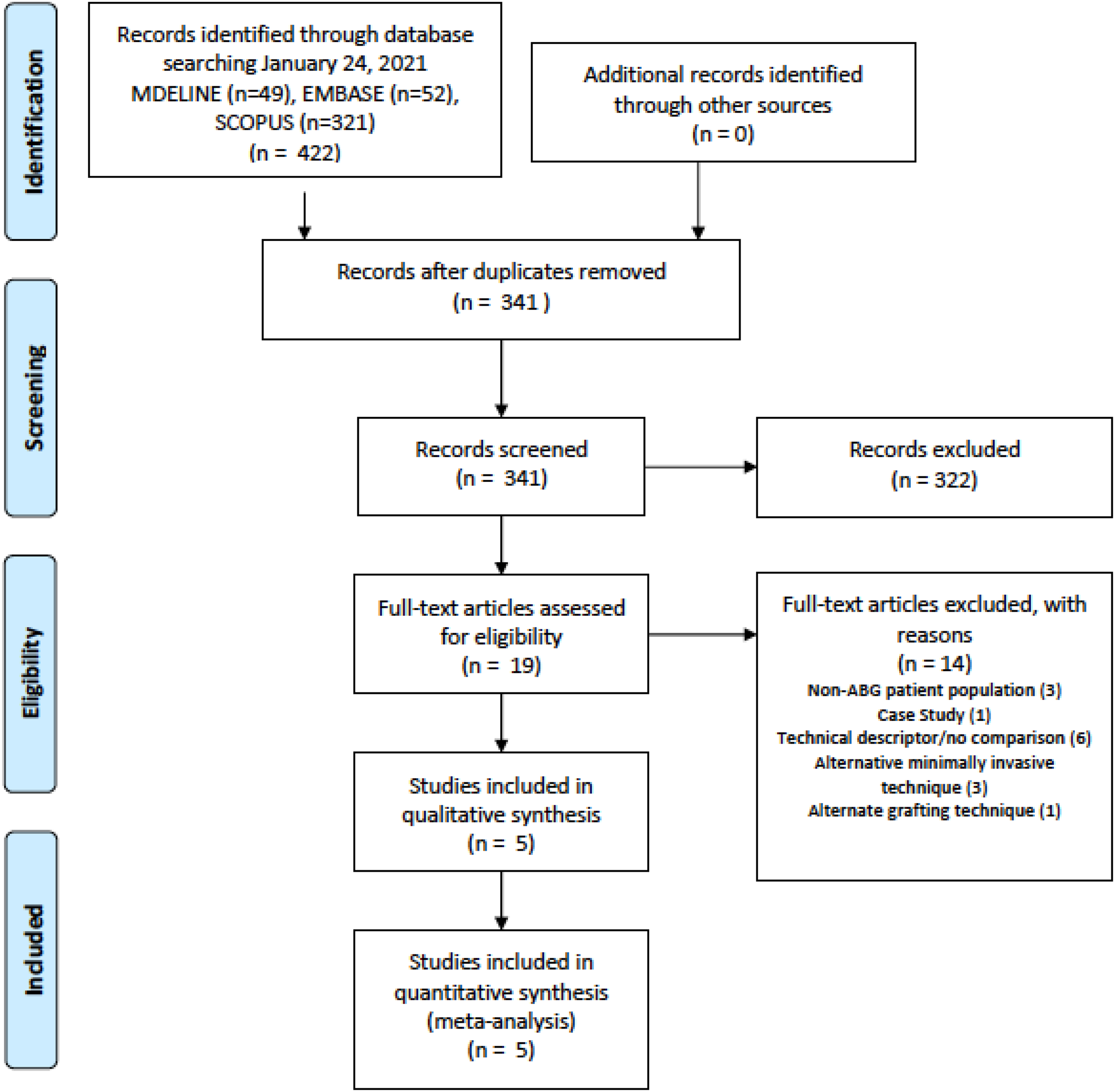
PRISMA flow sheet.
Open Versus Trephine Iliac Crest Bone Graft Harvest.
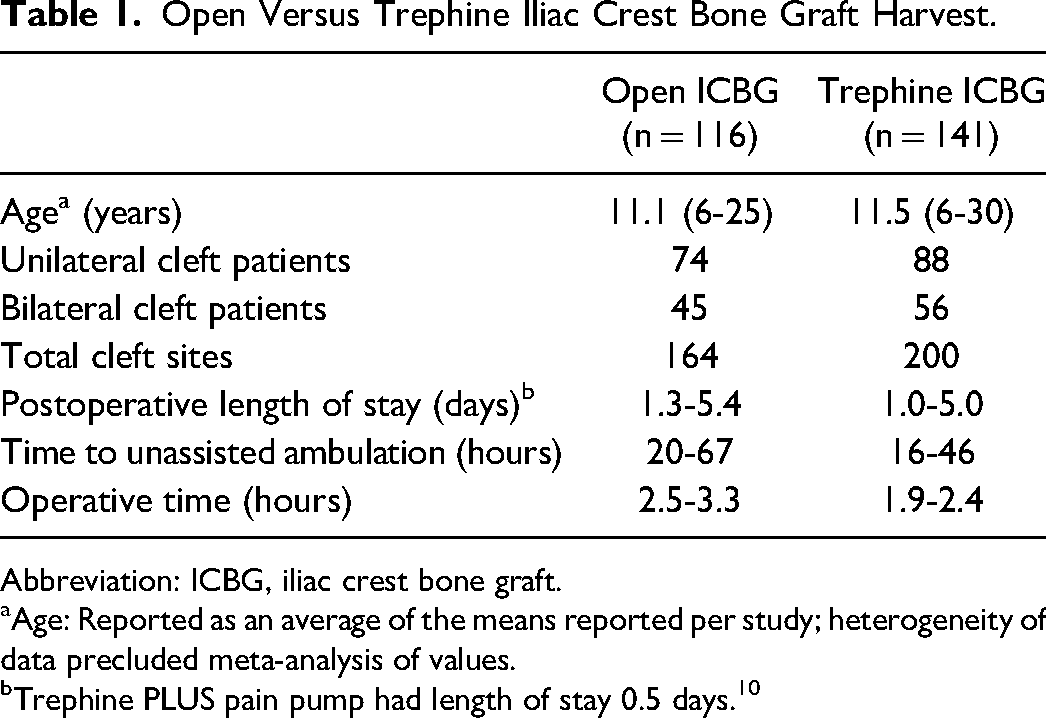
Abbreviation: ICBG, iliac crest bone graft.
Age: Reported as an average of the means reported per study; heterogeneity of data precluded meta-analysis of values.
Trephine PLUS pain pump had length of stay 0.5 days. 10
Operative Time
Patients undergoing trephine harvest had a reduced length of stay (range: 1.0-5.0 days vs 1.25-5.4 days for open harvest), and shorter time to unassisted ambulation (range: 16-46 hours vs 20-67 hours for open harvest) (Table 1). Total operative time was shorter in the trephine harvest group (1.9-2.4 hours vs 2.5-3.3 hours).5,10,11 One study reported the operative time required for the harvest portion only, reporting 11.4 minutes for trephine harvest versus 20 minutes for open harvest. 12
Pain Control
Peri- and postoperative pain control varied widely between studies. In three studies, there was no reported use of pain adjuncts, such as local anesthetic or regional blocks.5,11,13 In the study by Bykowski et al, the analgesic approach varied between three study groups; the open group received no pain adjuncts, while the “trephine-only” group had GelFoam® collagen sponge (Pfizer) impregnated with bupivacaine placed at the donor site. 10 They additionally compared these to a trephine harvest with pain pump group, in which patients received an infraorbital nerve block, IV acetaminophen infusion, GelFoam® at the donor site, and a catheter infusion of ropivacaine. 10 They found that the addition of an anesthetic infusion at the donor site significantly reduced the length of hospital stay and pain scores on both open and trephine harvest groups (length of stay for open 2.4 days, vs trephine 2.7 days, vs trephine plus pain pump 0.5 days, vs no harvest control 0.9 days). 10 Intraoperatively, Burstein et al used local infiltration with bupivacaine subcutaneously and in the deep periosteal plane, as well as placed GelFoam® impregnated with bupivacaine at the donor site. 12 Postoperative analgesic ranged from the use of acetaminophen and codeine most commonly,5,10,12 to the use of patient-controlled analgesia (PCA) as needed, 5 or acetaminophen and meperidine 11 (Table 2).
Summary of Included Studies.
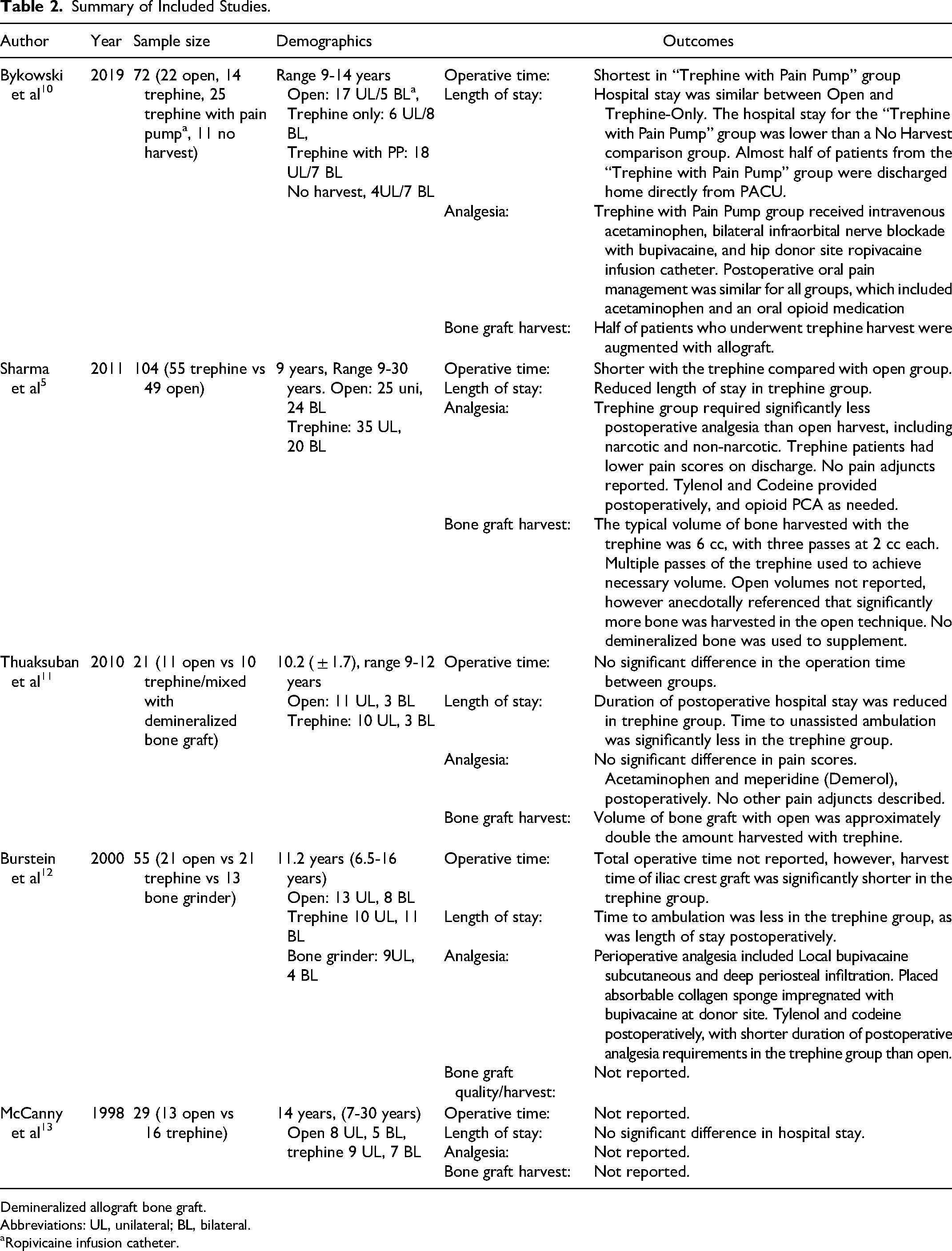
Demineralized allograft bone graft.
Abbreviations: UL, unilateral; BL, bilateral.
Ropivicaine infusion catheter.
Postoperative narcotic consumption and pain scores were reported in two studies.5,10 One study found reduced narcotic use post operatively in the trephine group (0.31 vs 1.64 mg/kg IV morphine). 5 They also reported higher pain scores for open harvest at time of discharge (3.1/10 vs 0.26/10). 5 Another study reported shorter duration of postoperative analgesia in the form of acetaminophen and codeine in the trephine versus open groups (16.5 hours vs 26 hours). 10
Bone Graft Harvest Volume
The volume of cancellous bone harvest was reported in two studies. The volume harvested in one study was 2.53 mL in the open group and 1.22 mL in trephine group. All patients undergoing trephine harvest required supplementation with deproteinized bovine bone (DBB). 11 Another study supplemented with demineralized bone graft in 54% of patients who underwent trephine harvest; however, none from the open harvest group required supplementation. 10 Three studies did not report any augmentation of graft volume with demineralized bone graft.5,12,13 Sharma and colleagues reported that sufficient graft volume could be achieved with trephine harvest, estimating up to 6 cc through three passes with the trephine (estimated 2 cc per pass). 5
Complications
Although no complications were reported in the trephine group, there were a small number in the open harvest patients: one postoperative infection, one hematoma, one report of paresthesia at donor site, and three cases of painful ambulation. Also reported was one case of idiopathic urinary retention, and one case of seizure activity.
Discussion
Compiled results of the five manuscripts that met our inclusion criteria demonstrated that patients undergoing trephine bone harvest had shorter lengths of stay, shorter operative time, and lower postoperative narcotic requirements as compared to open bone graft harvest. These results have been similarly demonstrated in adult studies. 4 However, the volume of cancellous bone harvested by trephine was less than that harvested by the traditional open technique, and often required augmentation with demineralized bone graft. Complications were rare with both techniques but more common in the open harvest group.
Donor Site Morbidity
Although trephine harvest was associated with decreased pain scores and reduced opioid consumption in all included studies, there were significant discrepancies in the use of adjunctive pain control modalities among these studies. Several institutions routinely employed local anesthetic infiltration, intravenous analgesics, regional nerve blocks, anesthetic infusion pumps, or intraoperative placement of collagen sponges (ie, GelFoam®) infiltrated with local anesthetic. As all of these adjuncts are independently associated with reduced postoperative pain, this likely confounds the comparative findings of postop pain reduction, time to ambulation, and length of stay.14–17
Recent work has assessed the effects of analgesic adjuncts independent of harvest techniques. Shenoy and colleagues reported significantly reduced postoperative pain scores in ICBG patients who received ultrasound-guided transversus abdominis plane (TAP) blocks, as compared to those who received local anesthetic infiltration alone. 17 Patients with a TAP block also had a shorter time to ambulation, which was felt to be due to reduced pain at the donor site. 17 Bykowski et al found that addition of an anesthetic infusion at the donor site significantly reduced length of hospital stay and pain scores on both open and trephine harvest groups, although more so in the latter. 10 These results highlight the importance of pain adjuncts for minimizing postoperative morbidity, regardless of harvest technique. 10
Historically, reported complications of open ICBG harvest have included intraoperative blood loss, dysesthesias, contour deformity, and persistent pain or gait abnormality.18,19 Many of these reports were published more than 20 years ago. In both groups reported here, there were very few complications. Contemporary studies have focused on a minimally invasive approach to the open technique, which attempts to limit pain by using a smaller incision, harvesting the medial table, and limiting periosteal stripping. This technique has led to significantly improved outcomes in donor site morbidity.1,2,6,20–23
Volume and Type of Harvested Bone
Mean volumes of cancellous bone obtained with trephine harvest were less than with the open technique and often required supplementation with demineralized bone graft, or multiple passes with the trephine to achieve the desired volume. 10 Although we limited our inclusion criteria to studies comparing open harvest and trephine, other authors have examined the use of either trephine alone or open alone (without control groups for comparison). In an early description of the use of trephine harvest, McGurk et al suggested that up to 6 cc of cancellous bone could be harvested. 24 Missiuna et al reported that 4 to 5 dowels with a 4.5 mm trephine would typically be sufficient for alveolar grafting, and rarely, a second incision was made to harvest additional bone; the volume harvested, however, was not reported in this study. 25
Stranix et al assessed the potential volume of cancellous bone graft harvest based on CT measurements. 8 The maximum cancellous volume they projected that could be safely harvested increased with age, with 12 cc in 8-year-olds, to 17 cc in 12-year-olds, using a 42 mm drill bit. 8 Despite these predictions, such harvest yields were not corroborated in clinical studies. Caminiti et al performed a study using 4 mm motorized trephine in adult cadavers, as well as 11 live patients. 7 On average, they achieved 0.46 cc of cancellous bone per core sample in the patient population, for a total of 2.3 to 3.2 cm 3 with 5 to 7 passes of the trephine. 7
Although most studies focus on cancellous bone graft harvest, many surgeons routinely utilize small segments of cortical bone for the reconstruction of the nasal floor defect. The trephine harvest approach limits access to obtaining cortical bone, and thus may be seen as a disadvantage to this technique. The typical trephine size used in pediatric patients would only allow for a very small cortical cap to be harvested, and furthermore, this area is generally cartilaginous in children and thus not suitable as a cortical bone graft.
Insufficient bone graft harvest, and the need for bone substitute have been separately assessed based on CT imaging of alveolar bone height. There is some evidence to suggest that bone substitutes and autogenous bone graft (or a combination) may have similar bone height in the long term, which may obviate the need for a donor site altogether.26,27
Safety
None of the studies included in our analysis reported significant complications with either the trephine or open technique. Stranix and colleagues investigated the theoretic risk of visceral injury using CT imaging, comparing drill size and trajectory. 8 This group reported no cases of visceral injury in 129 patients who underwent trephine bone graft harvest. They postulated that limiting the trephine depth to 3 cm reduces the risk of visceral injury based on their CT findings. 8 Caminiti et al corroborate these results, stating an increased risk of fracture to the inner or outer table with trephine depth more than 30 mm. 7
Missiuna et al describe the use of a Steinman pin as a trochar inserted into the iliac crest, over which they guided the circular trephine during bone graft harvest. 25 They state that “occasional breach of the iliac wall” occurred during harvest, and while the frequency of this occurrence was not reported, they did not report any incidence of nerve or visceral injury. 25
The current trend in ABG surgery is toward operative intervention in younger age groups, including patients as young as 6 years of age. 15 Computed tomography studies have shown that the cancellous bone width increases significantly from 8 to 12 years of age (7.21 to 10.97 mm, P < .001). 8 Although there have been few reported complications with trephine use in the studies reported here, the safety profile in this cohort with a thin iliac crest is still largely unknown and requires larger studies.
Study Limitations
This systematic review was limited by the small number of studies that met inclusion criteria for direct comparison of open versus trephine harvest technique. Many studies with descriptive techniques, but lacking in comparative analysis, were included in the discussion to further expand on our findings and nurture discussion on the topic. Furthermore, these studies employed a variety of different postoperative pain control strategies making accurate and objective comparison difficult. Small sample sizes may limit the ability to identify rare, but potentially serious, complications such as visceral organ injury.
There may also be some limitation in the applicability of results, as the mean ages reported were 9.0 to 14.3 years. Although debate remains about the ideal time for alveolar grafting, it is typically recommended during the period of mixed dentition, prior eruption of the cleft-side canine.15,28
This review did not assess less commonly used techniques for ICBG harvest, including percutaneous needle, cylindrical osteotome, Volkmann curette, modified bone core biopsy trocar, motorized CORB needle, bone grinder, grinding harvester, or mechanized coring. It is possible that these techniques have utility in specific clinical situations.
Conclusions
Although there are potential advantages to the trephine harvest of ICBG in children, these must be balanced against the significant risk of unpredictable harvest volume and the inability to obtain cortical bone. The limited literature available indicates reduced operative time, time to ambulation, length of hospital stay, and a favorable safety profile for trephine harvest despite the theoretical risk of visceral organ injury in children. Importantly, the evidence would also suggest that employing minimally invasive techniques during open harvest, as well as pain adjuncts such as regional blocks, would abate the historically referenced disadvantages of open harvest. Clinical equipoise still exists regarding the optimal approach for ICBG in the pediatric population and thus will be influenced by operator comfort, preference, and institutional experience.
This systematic review has informed the development of a clinical care pathway for alveolar cleft repair at our institution. We feel that the reported benefits of trephine harvest do not outweigh the disadvantage of limited or unpredictable volumes of cancellous bone and lack of cortical bone access. Consequently, we perform a minimally invasive, short incision open technique for ICBG harvesting, and routinely obtain a section of cortical bone from the inner table for nasal floor reconstruction. Importantly, we have also increased our focus on a standardized and thorough perioperative pain pathway and employ the use of multiple pain adjuncts, including local and regional anesthetic, and placement of GelFoam® with bupivacaine at the donor site.
Footnotes
Acknowledgments
Helen Lee Robertson, Medical Librarian University of Calgary; Golpira Elmi Assadzadeh, PhD, Statistical Analyst, University of Calgary.
Author Contributions
ART and SF independently conducted the systematic reviews and a priori data extraction, and ART performed analysis with help of a statistician. ART and TRC were largely responsible for manuscript writing, with significant contributions and edits from ARH and FOGF.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.