
Abstract
Background
With over 2.3 million cosmetic surgical procedures performed in the U.S. in 2020 alone, the exponential growth of the field in recent years is undeniable. 1 Given this rise in popularity and the elective nature of these procedures, plastic surgeons are increasingly striving to surpass the high expectations of their cosmetic surgery patients. One of the important determining factors of patient satisfaction is post-operative complications. 2 Therefore, surgeons adhere to standards of excellence and up-to-date guidelines with the hope of minimizing these complications. 3
Minimizing the risk for complications becomes even more of a focus given that the aesthetic practice is based on solely elective procedures, and thus foreseeable complications should be avoided at all costs. One way to decrease the risk of complications is by meticulous patient selection and patient counselling regarding known risk factors.
Tobacco smoking remains one of the most cited risk factors for post-operative complications, and a major public health concern in general.4–6 Aesthetic surgeons should therefore be able to have evidence-based discussions with their patients regarding the specific risks associated with smoking. However, due to the unfeasibility of running prospective trials and the exclusion of smokers in many studies for fear of complications, there is a lack of strong evidence regarding the specific effects of smoking on different types of aesthetic surgeries. 7 While previous studies have assessed the effects of smoking on post-operative complications in cosmetic surgery,8–12 their results have been limited by small sample sizes, heterogeneous cohorts (including both reconstructive and cosmetic procedures) and a paucity of higher level of evidence studies.
To that end, the goal of this study is to systematically review and meta-analyze the literature to elucidate the impact of smoking on individual cosmetic surgical procedures. This data will help provide recommendations for pre-operative smoking cessation specific to a procedure, improve patient selection and ultimately provide the best surgical care for patients.
Materials and Methods
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 13 a systematic search of PubMed, Embase and Cochrane was conducted with the following search strategy, restricted to English: ([tobacco] OR [smok*]) AND ([breast augmentation] OR [breast reduction] OR [mastopexy] OR [mammoplasty] OR [lipofilling] OR [liposuction] OR [facelift] OR [rhytidectomy] OR [blepharoplasty] OR [rhinoplasty] OR [otoplasty] OR [arm lift] OR [thigh lift] OR [body contouring] OR [abdominoplasty]). Following duplicate removal, retained studies’ title and abstracts were screened, and then assessed in full text for eligibility according to strict inclusion and exclusion criteria. All studies for which raw numbers for surgical outcomes among cohorts of tobacco smokers and non-smokers could be isolated for a single type of aesthetic surgery were included. Exclusion criteria included non-aesthetic surgeries, studies with less than 10 patients, studies that did not stratify results based on procedure type or smoking status, and those that did not report surgical complications or only reported Odds Ratio (OR) with no raw data. All studies were assessed for level of evidence according to the Oxford Centre for Evidence Based Medicine criteria. 14 This entire process was carried out independently between two authors and any discrepancies were resolved through consensus. Data regarding study type, qualitative conclusions and quantitative surgical outcomes between smoker and non-smoker cohorts were then extracted from the included studies. Patients were categorized as either smokers or non-smokers. If studies reported a cohort of previous smokers, we pooled them with the non-smoker group. Given that most primary studies reported on cohorts of smokers vs. non-smokers and that smoking status was largely self-reported, we favored the assumption that previous smokers at the exact time of data collection were likely reported as non-smokers. When not directly provided in the text, the overall complication rate was computed by pooling the complication(s) reported by the study in question.
Statistical Analysis
Studies were grouped by procedure, among which different types of surgical complications were also pooled. A meta-analysis of these, stratified by procedure and complication type, was conducted on Review Manager (RevMan) v5.4 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Due to the heterogeneity of the data, a random effects model was used in conjunction with the Mantel-Haenszel statistical method, in order to determine pooled OR. 15 Of note, procedures with 3 or less cohorts were not meta-analyzed (but still reported in the systematic review) due to paucity of data which would render results of questionable power. Pooled OR estimates with 95% confidence intervals were computed, with statistical significance set at p ≤ 0.05. Heterogeneity was computed using the chi-square test and formally quantified by the I2 statistic. Although the effect in OR and confidence interval for each individual complication with enough data was calculated, the effect of the overall complication rate was further demonstrated using forest plots for each surgical category.
Results
Search Outcome
Following duplicate removal, 1794 initial studies were screened, leading to 217 being assessed in full for eligibility. An additional five studies were added to the full text review from manual search of relevant references. A total of 82 studies met our selection criteria and were included in this review (
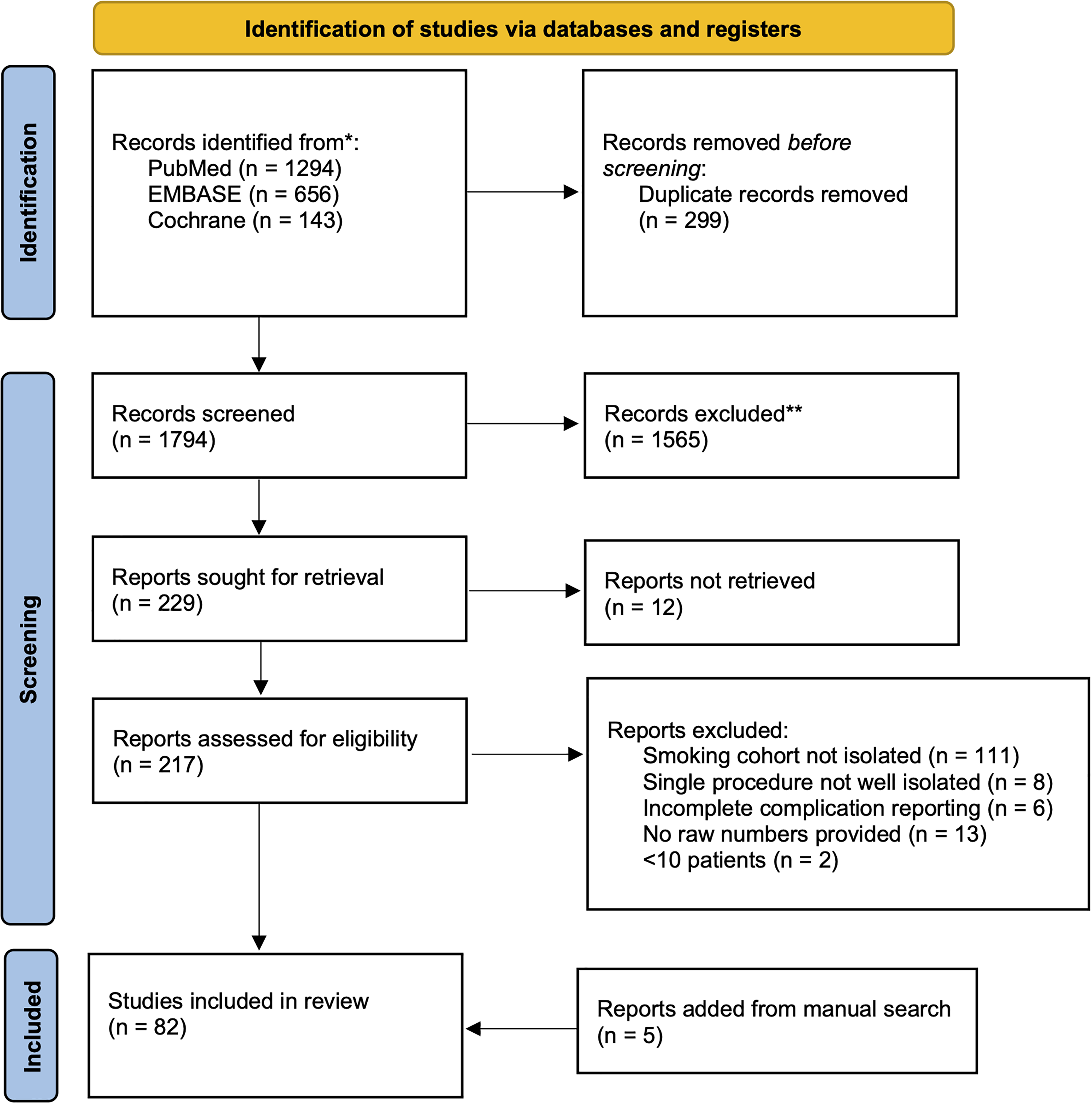
PRISMA Flow Chart for Systematic Review.
Body Contouring Surgery
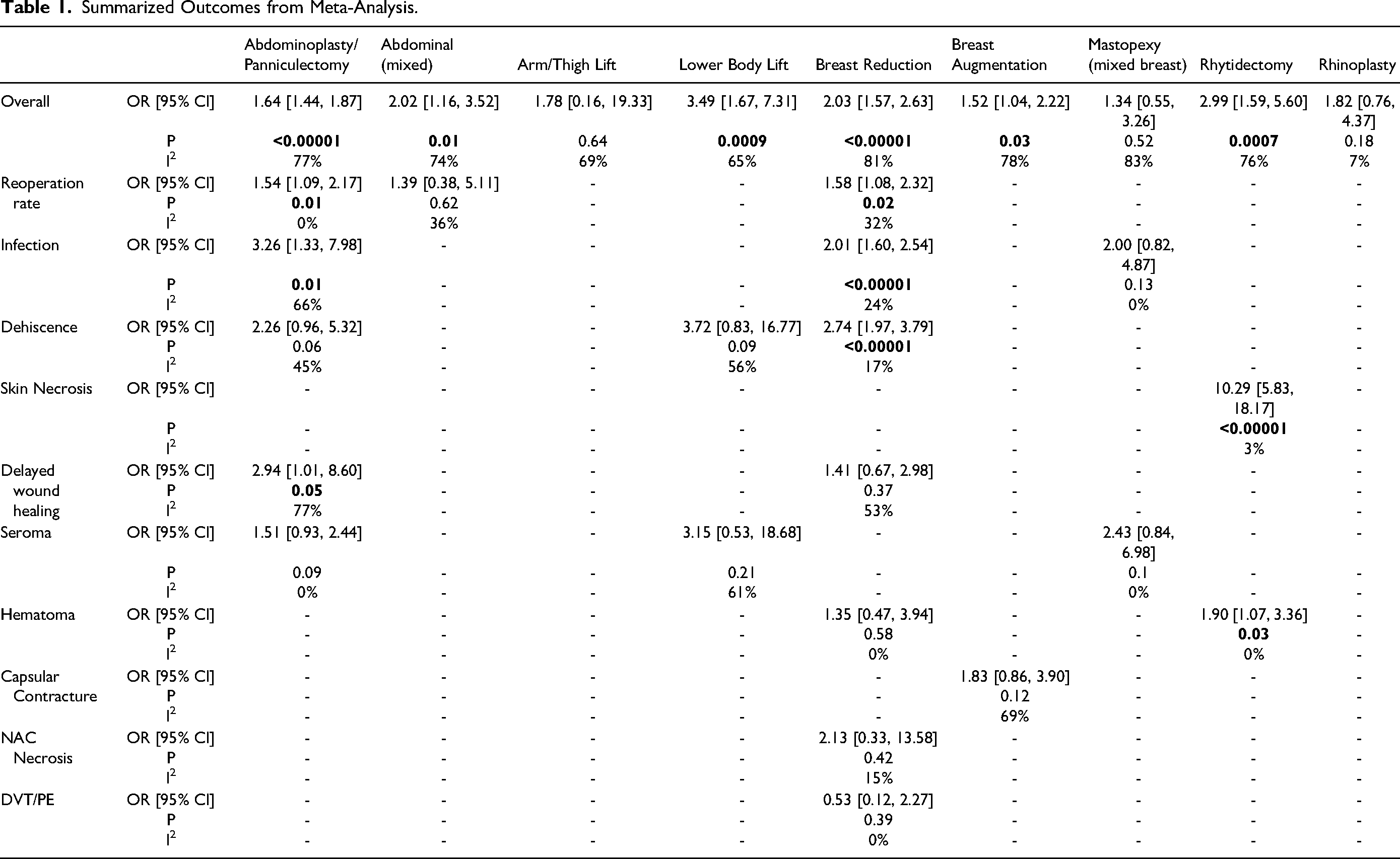
Among the abdominoplasty & panniculectomy category, smoking was associated with an increased risk of overall complications (OR: 1.64 [1.44, 1.87] [p < 0.00001] (
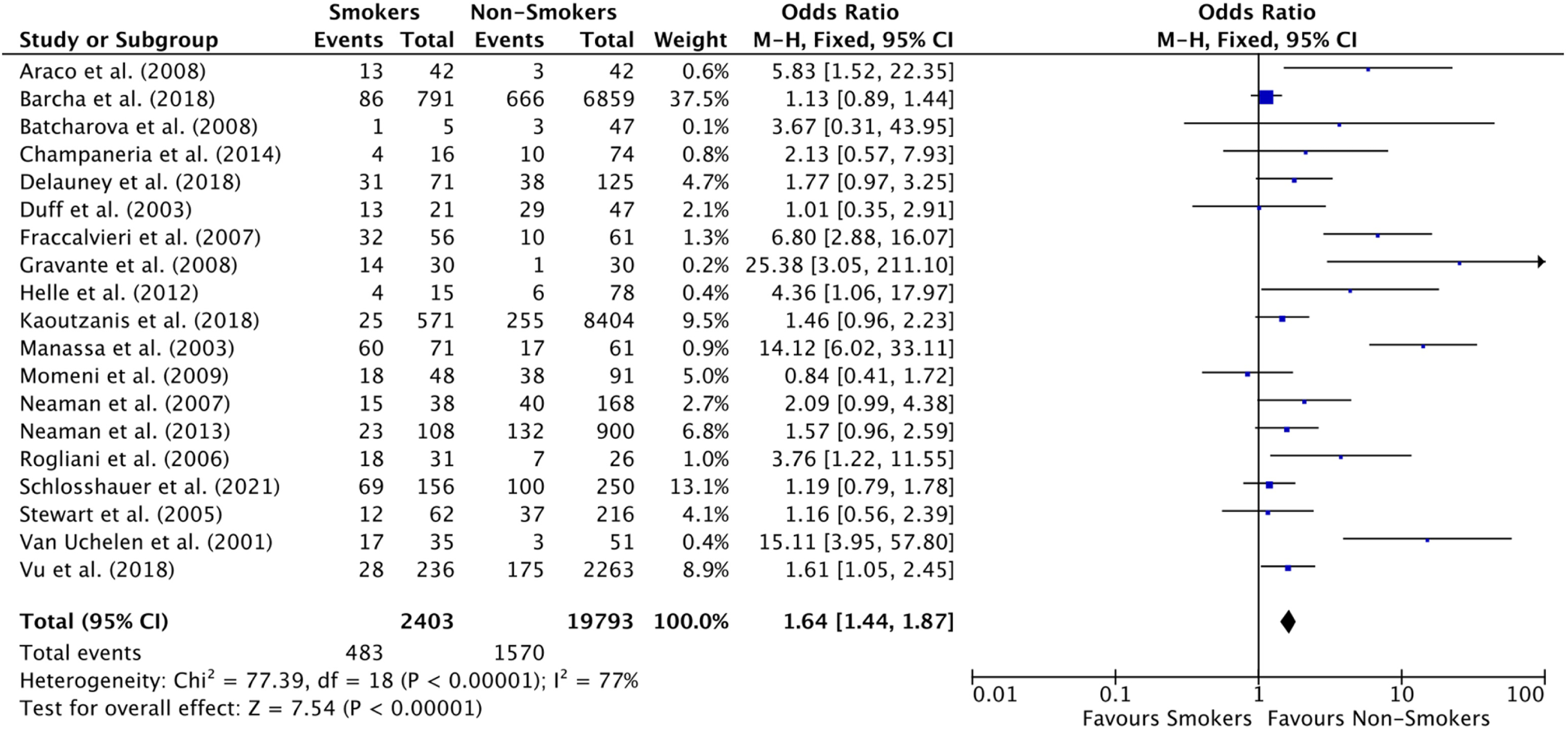
Forest Plot for Overall Complicate Rate in Abdominoplasty & Panniculectomy studies.
Forest Plot for Overall Complicate Rate in Abdomen (with concomitant procedures) studies.
Forest Plot for Overall Complicate Rate in Lower Body Lift studies.
Summarized Outcomes from Meta-Analysis.
Breast Surgery
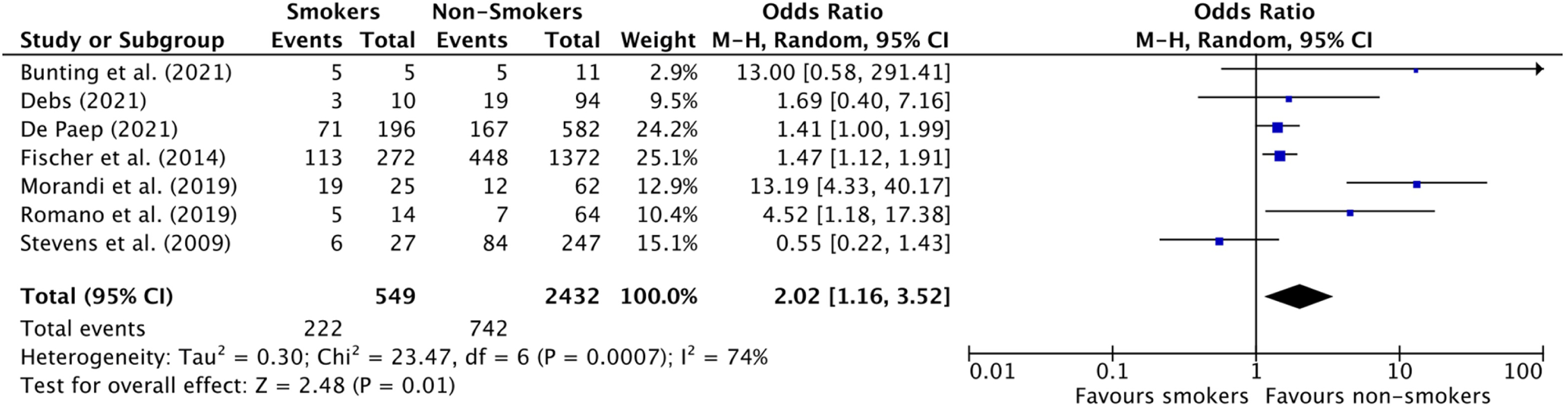
In the breast reduction category, smoking was associated with an increased risk of overall complications (OR: 2.03 [1.57, 2.63] [p < 0.00001]) (
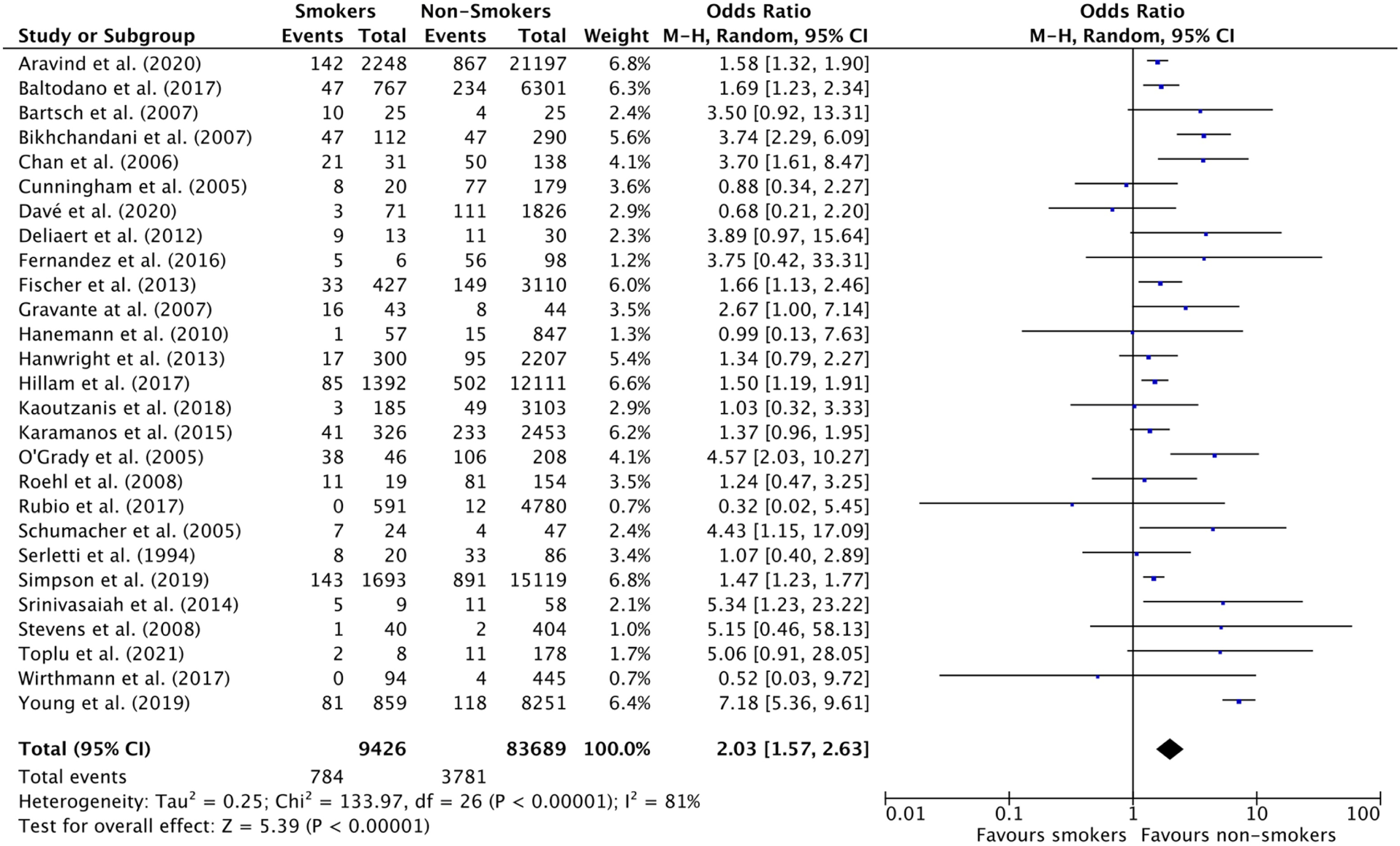
Forest Plot for Overall Complicate Rate in Breast Reduction studies.
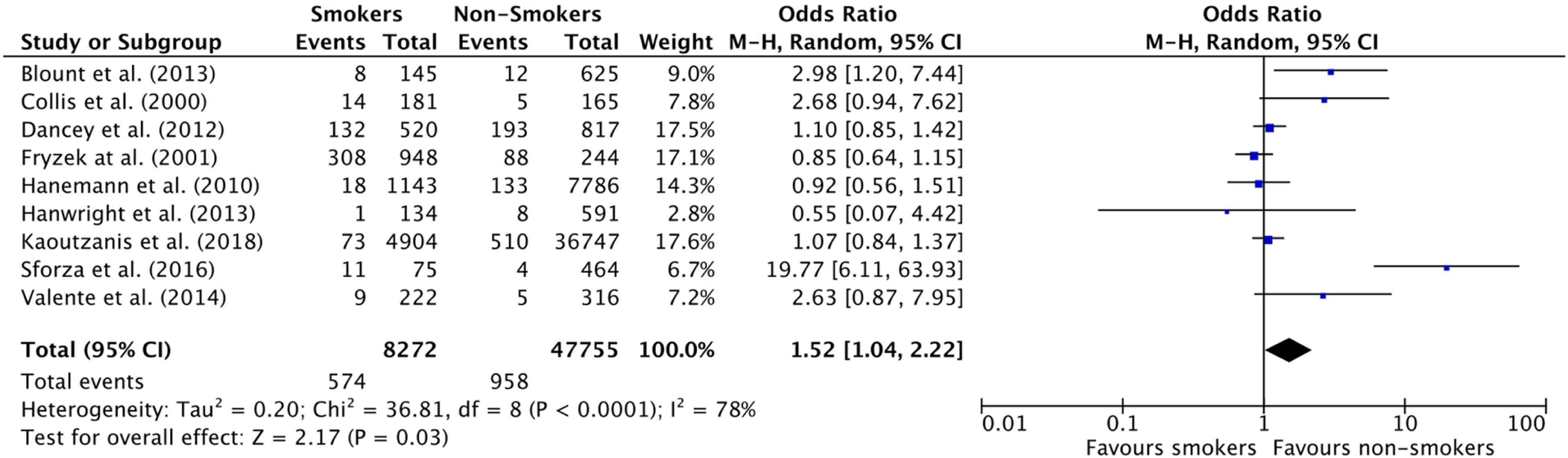
Similarly, smoking in breast augmentation was associated with an increased risk of overall complications (OR: 1.52 [1.04, 2.22] [p = 0.03] but not an increase in any specific complication (
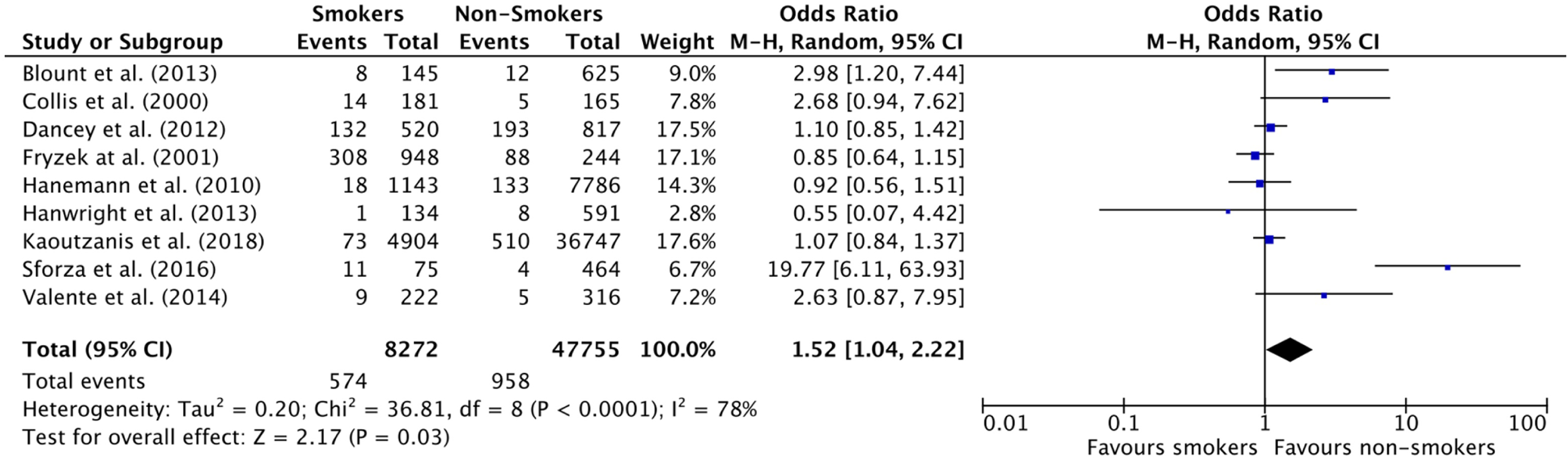
Forest Plot for Overall Complicate Rate in Breast Augmentation studies.
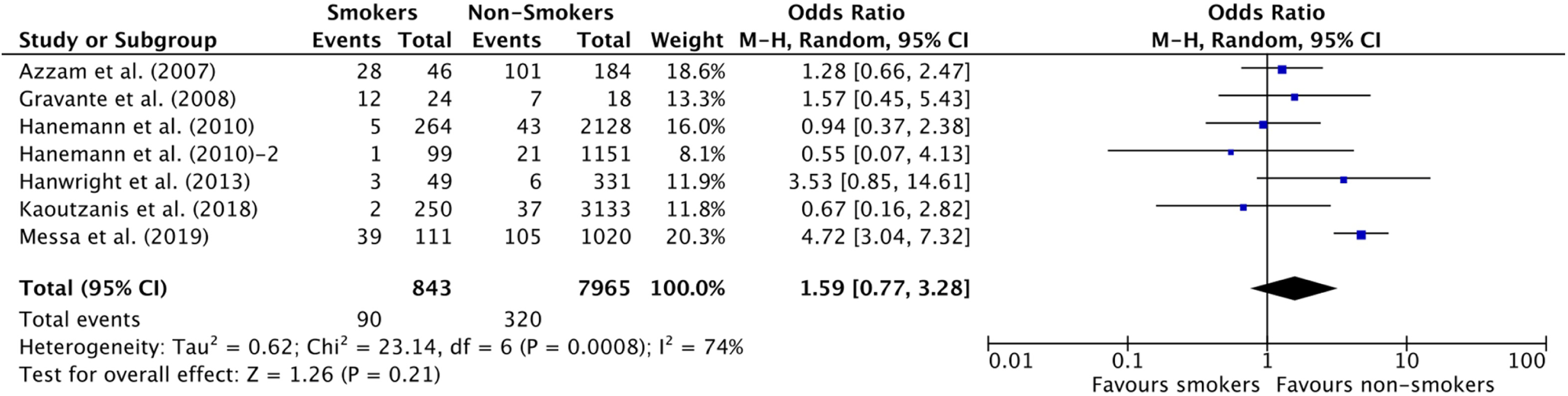
Forest Plot for Overall Complicate Rate in Mastopexy (& other breast procedures with concomitant mastopexy) studies.
Facial Surgery
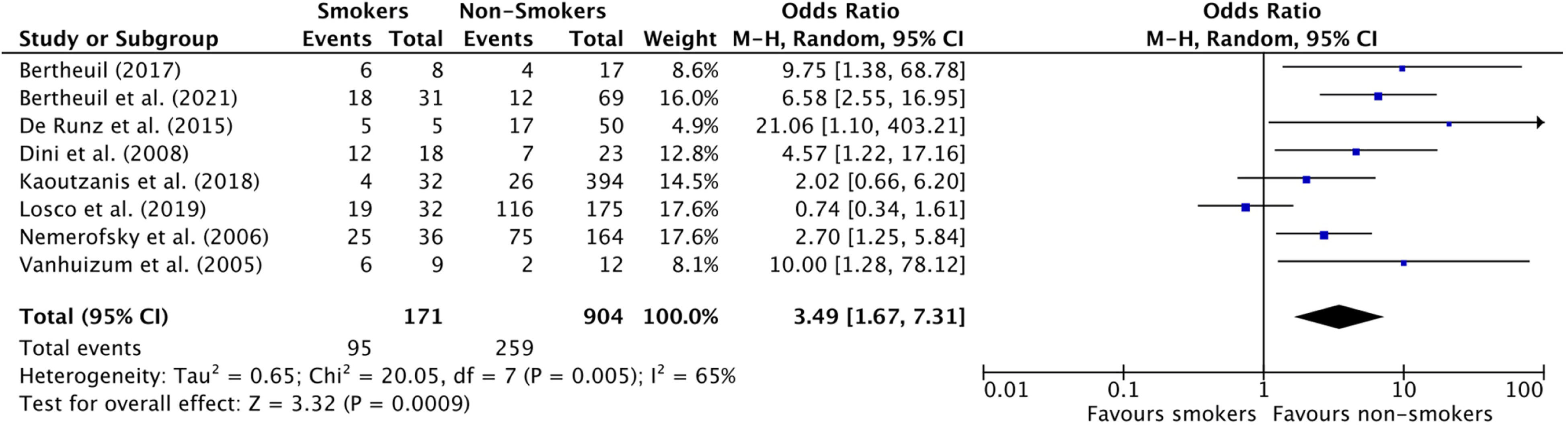
Among patients undergoing a rhytidectomy, smoking was associated with an increased risk of total complications (OR: 2.99 [1.59, 5.60] [p = 0.0007] (
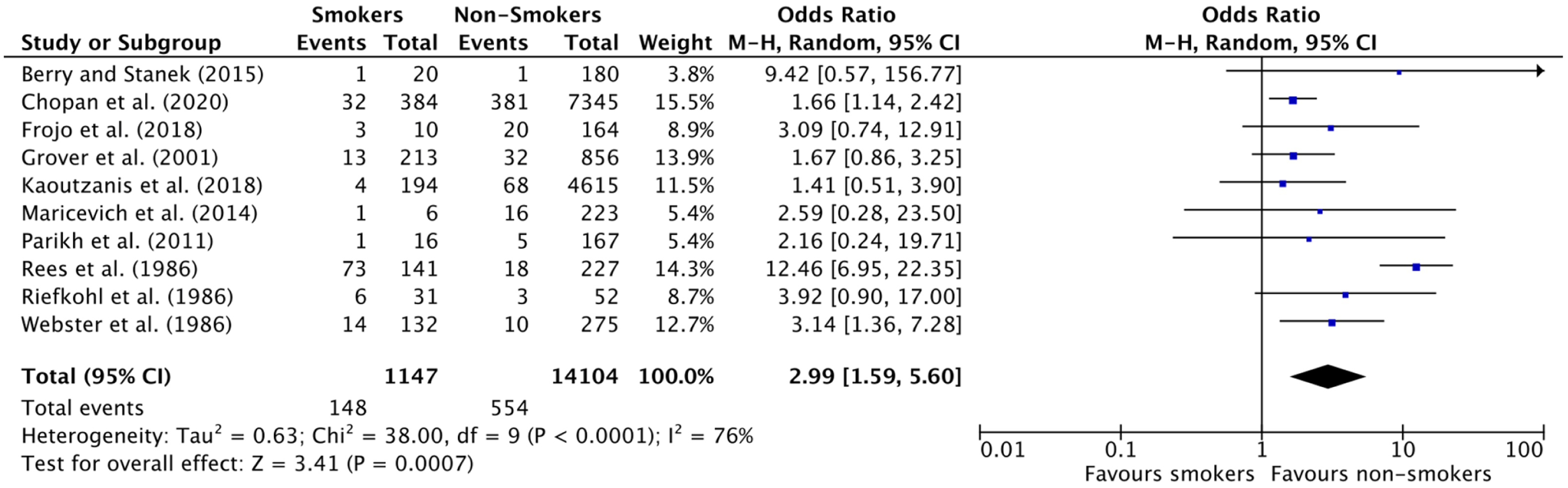
Forest Plot for Overall Complicate Rate in Rhytidectomy studies.
Forest Plot for Overall Complicate Rate in Rhinoplasty studies.
Discussion
The results of this meta-analysis demonstrate that smoking is associated with higher odds of incurring overall surgical complications across most of the aesthetic surgical procedures studied (abdominoplasty, lower body lift, breast reductions, breast augmentation, and rhytidectomy). However, among patients undergoing mastopexy or rhinoplasty, our review demonstrated no association between smoking and an increased risk of complications.
The underlying pathophysiology of smoking in surgical patients relies on the reduction in tissue perfusion, the impairment of inflammatory cell functions, and the attenuation of reparative cell functions. 97 Mainly through catecholamine release and activation of the Thromboxane A2 pathway, nicotine and nitric oxide promote vasoconstriction and thus decrease tissue perfusion.98,99 Simultaneously, tobacco smoke toxins cause an impairment in neutrophil and monocyte-macrophage activity, and promote the release of reactive oxygen species, which are detrimental to the wound healing pathway.97,100,101 However, previous studies have shown that reversal of cellular damage can be observed after three weeks of abstention. 100 Therefore, aesthetic surgeons should strive to provide adequate smoking cessation support and education to all of their pre-operative patients, mainly through behavioral support and nicotine replacement therapy, especially since Van Slyke et. al. 102 have shown that enforcing smoking cessation before cosmetic surgery may promote long lasting smoking cessation. 103
Not only was smoking associated with a higher rate of complications in the majority of aesthetic surgeries studied, but it was also associated with a significantly higher rate of reoperation in abdominoplasty/panniculectomy, as well as following breast reduction surgery. This is in line with previous literature where smoking was found to be associated with higher rates of reoperation in other surgical domains.104,105 Although this may be true for other cosmetic procedures included in the present study, the authors could not investigate re-operation risk for the other procedures due to the paucity of data.
Interestingly, the two types of surgeries that did not show a significant association between smoking and increased rate of complications were mastopexy and rhinoplasty. A closer analysis of our rhinoplasty cohort demonstrates that most complications reported by Irvine et al. 92 (OR = 0.59 [0.08, 4.53]) occurred in former smokers, and these were pooled with the non-smoker group as per our protocol, which could have contributed to the lack of statistical significance between our two studied groups. As per our meta-analysis, mastopexy does not seem to confer an added risk among smokers. However, theoretically this is counterintuitive as the added incisional wounds from a mastopexy result in a decreased dermal blood supply, a phenomenon which is exacerbated by the known vasoconstrictive effects of tobacco smoking.98,106 Therefore, this led the authors to suspect a source of bias in this cohort. A closer look of the primary studies revealed that only two primary studies11,27 comprised the majority of patients (79.8%) in this cohort, and thus weighed heavily on the meta-analysis. Both studies explained the lack of association between smoking and complications through a pre-selection bias, suggesting that surgeons may have refused surgery for the heavier smokers pre-operatively. Therefore, “light” smokers were compared to non-smokers, which may have contributed to the lack of difference in complications between both groups.
Limitations and Future Directions
This review is not without limitations, mainly due to the inherent heterogeneity of the included studies. Considering only a few studies reported numbers for previous smokers, for the statistical purposes, the authors pooled previous smokers with the non-smoker categories, as most other studies relied on self-reported smoking status at the time of their respective data collection. To add to this, most studies did not report their definition of non-smokers, or had varying timelines for what they considered a “non-smoker”. The authors also could not account for the heterogeneity in techniques utilized for different cosmetic procedures (eg different breast reduction pedicles, different planes for face lifts etc), which may have introduced another source of bias into the results. This heterogeneity is reflected in the high I2 values seen in our results, despite being mitigated by using random effects modelling in our analysis. Considering the time and dose-dependent nature of the effect of smoking, and that certain studies demonstrated differing risks among former and non-smokers, the authors believe future studies should report numbers of former smokers and indicate their amount/time of consumption. Moreover, future studies should better characterize the effects of smoking on mastopexy and rhinoplasty. Finally, other than scarring and capsular contracture, there is a lack of reporting on aesthetic outcomes between smokers and non-smokers, which would be interesting to compare in future studies.
Conclusion
Despite the overall reduction in smoking habits in the last few decades, smoking remains a major risk factor across the board for cosmetic surgery patients. This is especially true for reoperation rates in abdominoplasty, infection and dehiscence in breast reduction, and skin necrosis and hematoma in rhytidectomy. Conversely, more research is needed to accurately quantify the risk of smoking on complications in rhinoplasty and mastopexy. The authors hope that due to the paucity of large, prospective trials, the results demonstrated in this meta-analysis can be used to better counsel patients pre-operatively, better stratify post-operative risk for developing specific complications, and ultimately improve the process of informed consent between aesthetic surgeons and their patients.
Supplemental Material
sj-docx-1-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-3-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-4-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-5-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-6-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-6-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-7-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-7-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-8-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-8-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-docx-9-psg-10.1177_22925503221085083 - Supplemental material for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-9-psg-10.1177_22925503221085083 for A Procedure and Complication-Specific Assessment of Smoking in Aesthetic Surgery: A Systematic Review and Meta-Analysis by Gabriel Bouhadana, Hassan ElHawary, Peter Alam and Mirko S. Gilardino in Plastic Surgery
Footnotes
Author Contributions
G.B. and H.E. contributed to the design of the research, analysis of the results and writing of the manuscript. M.G. contributed to the editing of the manuscript and supervision of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.