
Abstract
Introduction
The prevalence of obesity has increased from 30.5% to 42.4% between 2000 and 2018. 1 Obesity continues to pervade the fabric of our society, having multisystem consequences that differ by sex, ethnicity, and socioeconomic background. As the idea of undergoing surgery to achieve weight loss has become a more socially acceptable notion, the number of body contouring procedures have increased in parallel. The presence of a pannus can lead to issues with mobility, problems with hygiene, and skin breakdown. One of the most commonly performed procedures to remove this lower abdominal tissue is a panniculectomy.
Throughout medical literature, it has been made clear that obesity often occurs hand in hand with diabetes; in other words, diabetes is frequently associated with this now common panniculectomy procedure.2–4 As the rate of obesity continues to surge, diabetes has evolved as a global health issue, having more than doubled in the last 20 years with a rate of 400 million worldwide. 5 Furthermore, it is clear that diabetes has a negative impact on wound healing.6–9
Despite the weight loss that some patients undergo in preparation for a panniculectomy, many of these patients have refractory diabetes. In spite of all of this, few articles specifically delve into the relationship between panniculectomy and diabetes, and those that do often look at smaller populations or often address diabetes broadly through the lens of metabolic syndrome. Furthermore, obesity is one of the only established risk factors for adverse panniculectomy outcomes, whereas data on diabetes, smoking, and hypertension (HTN) are inconsistent. 10 The purpose of the article was to evaluate the effect of diabetes on post-operative complications following a panniculectomy in the setting of a large cohort and to determine the risk factors associated with adverse post-operative events.
Materials and Methods
A commercially available, proprietary, national insurance claims-based database, PearlDiver Patients Records Database (www.pearldiverinc.com; PearlDiver Inc.) was utilized in this study. The records used for analysis are de-identified, anonymous, and compliant with the privacy rules of the Health Information Portability and Accountability Act and were therefore exempted from review by the institutional review board at our institution. Accordingly, queries resulting in less than 11 patients are not indicated to protect patient privacy. The database contains patient demographics, comorbidities, diagnoses, procedures, and medications among numerous other data available for patients which may be queried via International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) and procedures or Current Procedural Terminology (CPT) codes. The database information spans all US patients insured from 2010 to 2018, and patients can be tracked across all locations (inpatient, outpatient, etc) throughout the database years, and contains approximately 20 million patients.
The CPT code 15380 was used to identify patients who had undergone a panniculectomy. Patients were filtered for the presence of valid age, gender, regional information, as well as the presence of claims data available for one year following the operation. General comorbidity information, patient factors, and post-operative complications were collected and described in Supplemental Table 1. Demographic data on age and sex were reported by the database and of course included in our tables. Diabetes mellitus was identified as the risk factor of interest within this patient population and thus the 2 groups of panniculectomy patients were divided into those without diabetes (Group 1) and those with diabetes (Group 2). Patients were matched by Charlson Comorbidity Index (CCI) index, age range, cardiac complications, and gender. Because of the sheer volume of codes assigned to cardiac complications, we chose to control for this comorbidity separately. Patients with diabetes were further divided into 2 cohorts—those that were insulin-dependent (Group 2A) and those that were not (2B).
Univariate Analysis of Demographics and Comorbidities in Panniculectomy Patients.
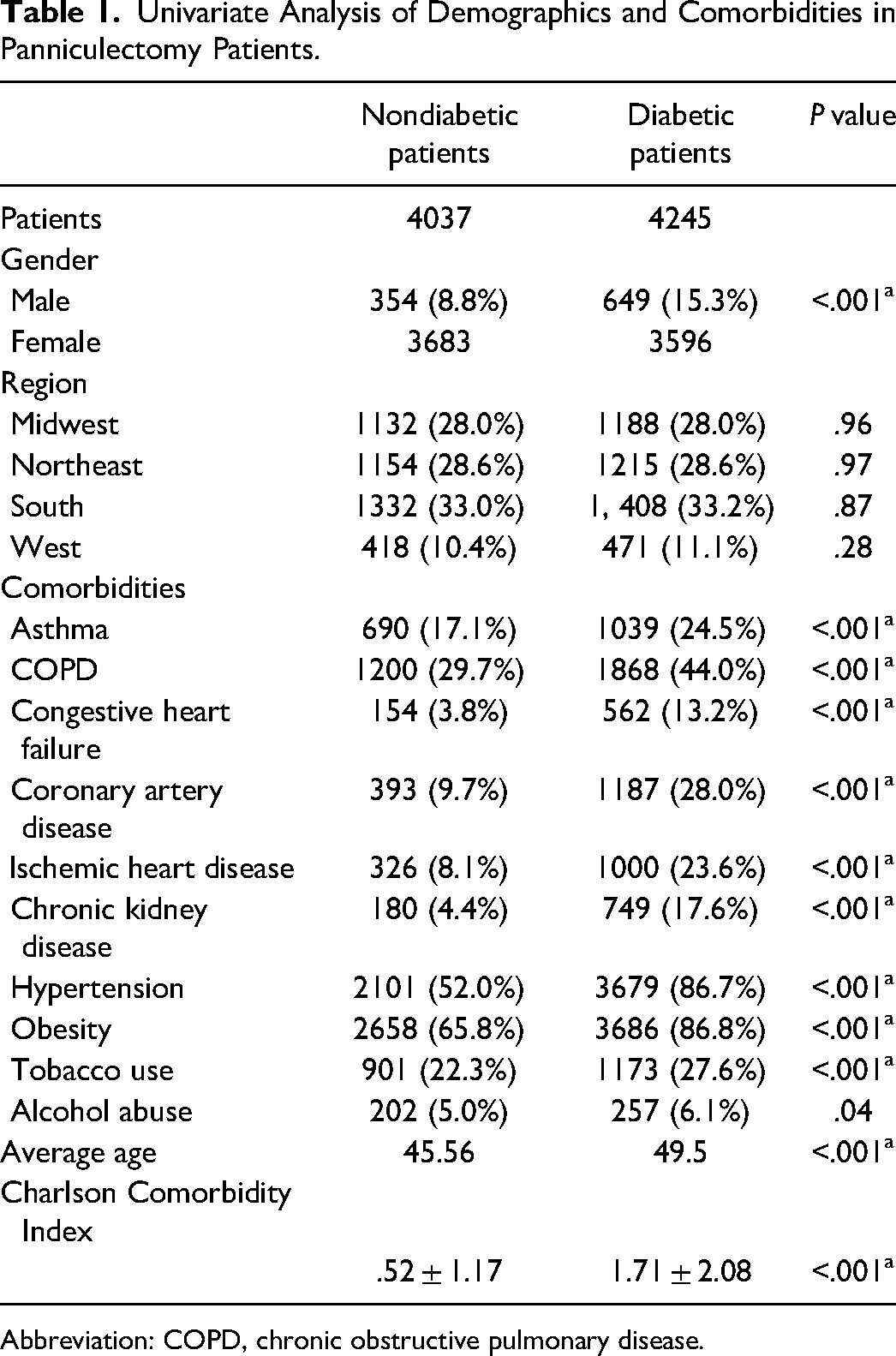
Abbreviation: COPD, chronic obstructive pulmonary disease.
Matched b —Analysis of Demographics and Comorbidities.
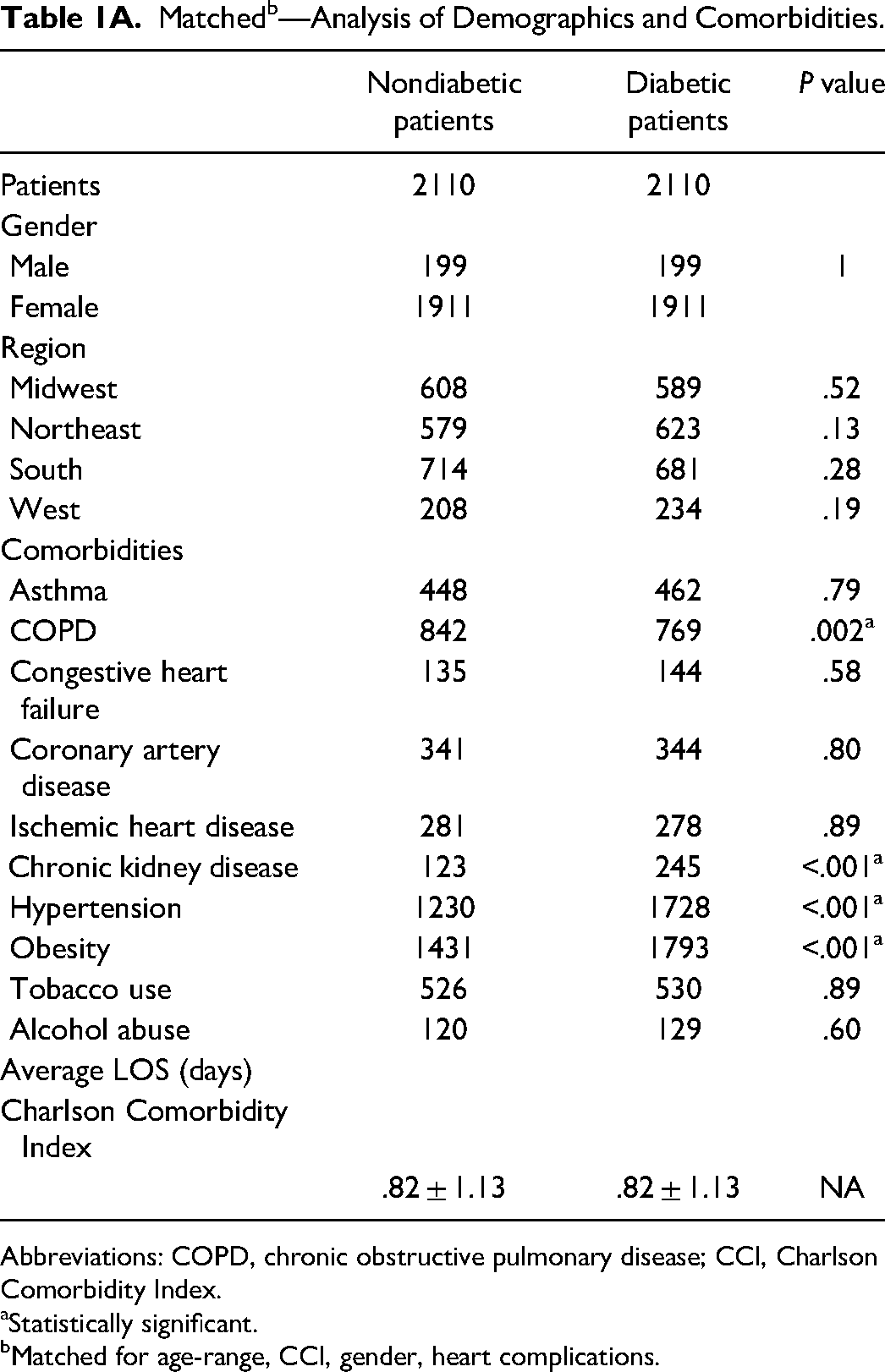
Abbreviations: COPD, chronic obstructive pulmonary disease; CCI, Charlson Comorbidity Index.
Statistically significant.
Matched for age-range, CCI, gender, heart complications.
R Project for Statistical Computing software (https://www.r-project.org/), available through the PearlDiver database was used for all statistical analyses. Epidemiologic data were then analyzed to report descriptive statistics including number, percentage, mean, median, and ranges as appropriate. Logistic regression analysis was utilized to evaluate the association of patient-related risk factors including demographic variables and comorbidities with the reporting of perioperative and prolonged opioid prescriptions. Secondary endpoints included all-cause 30-day emergency department visits or hospital admissions. Odds ratios (ORs) were calculated from the regression analysis, and a corresponding 95% confidence interval (CI) and P value were also calculated for each patient-related risk factor. For all statistical calculations, P < .05 was considered statistically significant.
Results
A total of 8282 patients that underwent a panniculectomy were identified within the database—4245 (51.3%) with diabetes and 4037 (48.7%) without. The average age of patients in the diabetic group was higher at 49.5, compared to 45.56 in the nondiabetic group (P < .001). Although the majority of patients that underwent this procedure were female for both nondiabetic and diabetic patients, the percentage of women was significantly higher (84.7% vs 91.2%, P < .001). Although there were a number of comorbidities identified in both groups, there were higher rates of comorbidities across in the board in diabetics. Notably, in diabetic patients, there were significantly higher rates of HTN, chronic obstructive pulmonary disease (COPD), obesity, and chronic kidney disease (CKD) when patients were matched. There was an overall higher incidence of comorbidities in the diabetic population, which coincided with the higher CCI (0.52 vs 1.71, P < .001).
Univariate analysis showed that diabetic patients had a higher rate of surgical complications, including hematomas (11.4% vs 5.7%), wound disruption (12.1% vs 4.6%), and surgical site infection (11.3% vs 4.3%). There was also a higher rate of readmissions (9.5% vs 5.0%) as well as reoperations (6.0% vs 15.6%). Overall, patients with diabetes sustained higher rates of complications; importantly, this was true once patients were matched, as evidenced by Table 2A. In other words, in a controlled population comparing diabetic patients to nondiabetic patients, the rates of adverse post-operative outcomes remain higher for patients with diabetes.
Univariate Analysis of Surgical Outcomes and Medical Complications in Panniculectomy Patients.
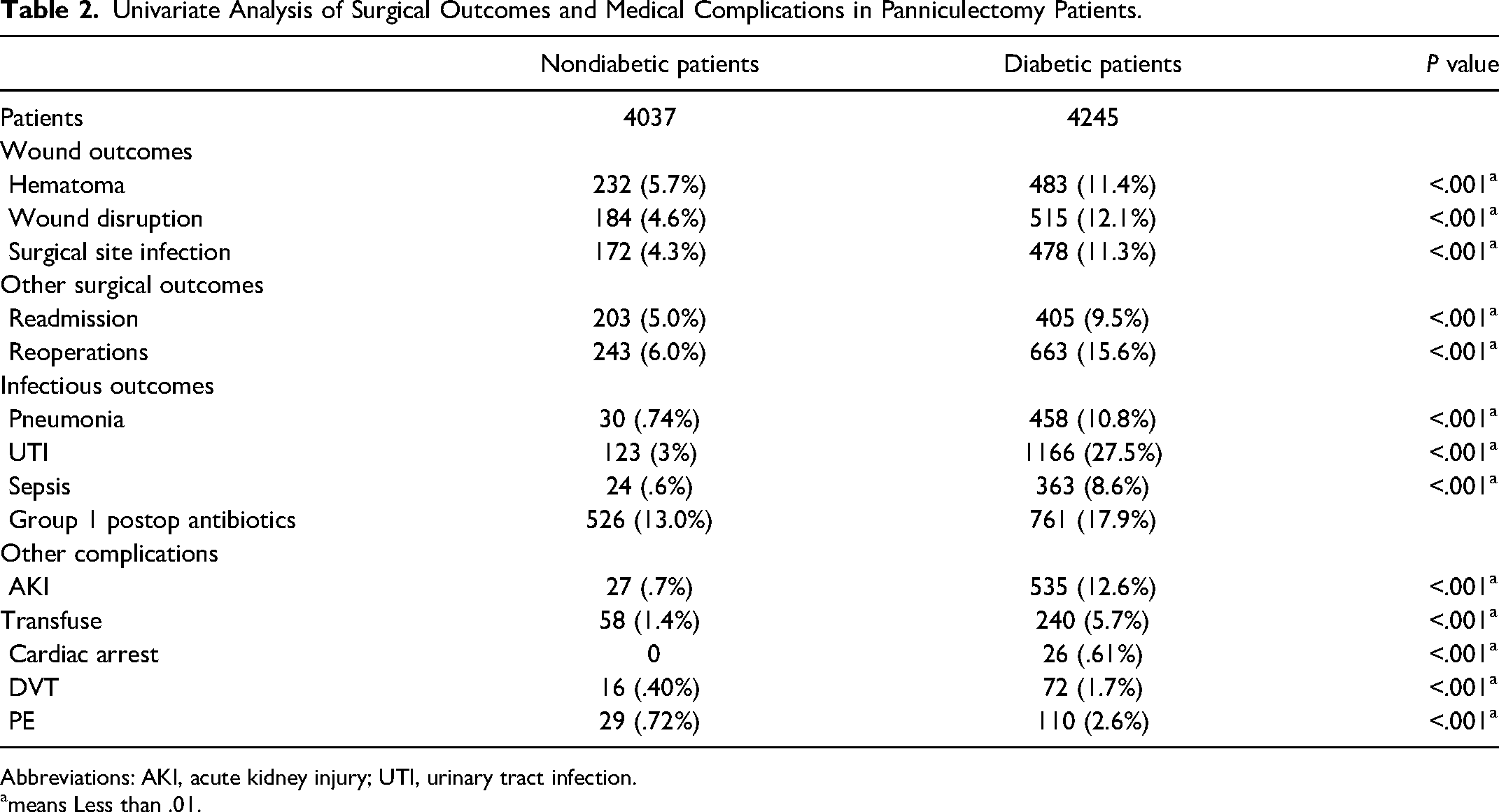
Abbreviations: AKI, acute kidney injury; UTI, urinary tract infection.
means Less than .01.
Matched—Surgical Outcomes and Medical Complications in Nondiabetic Versus Diabetic Panniculectomy Patients.
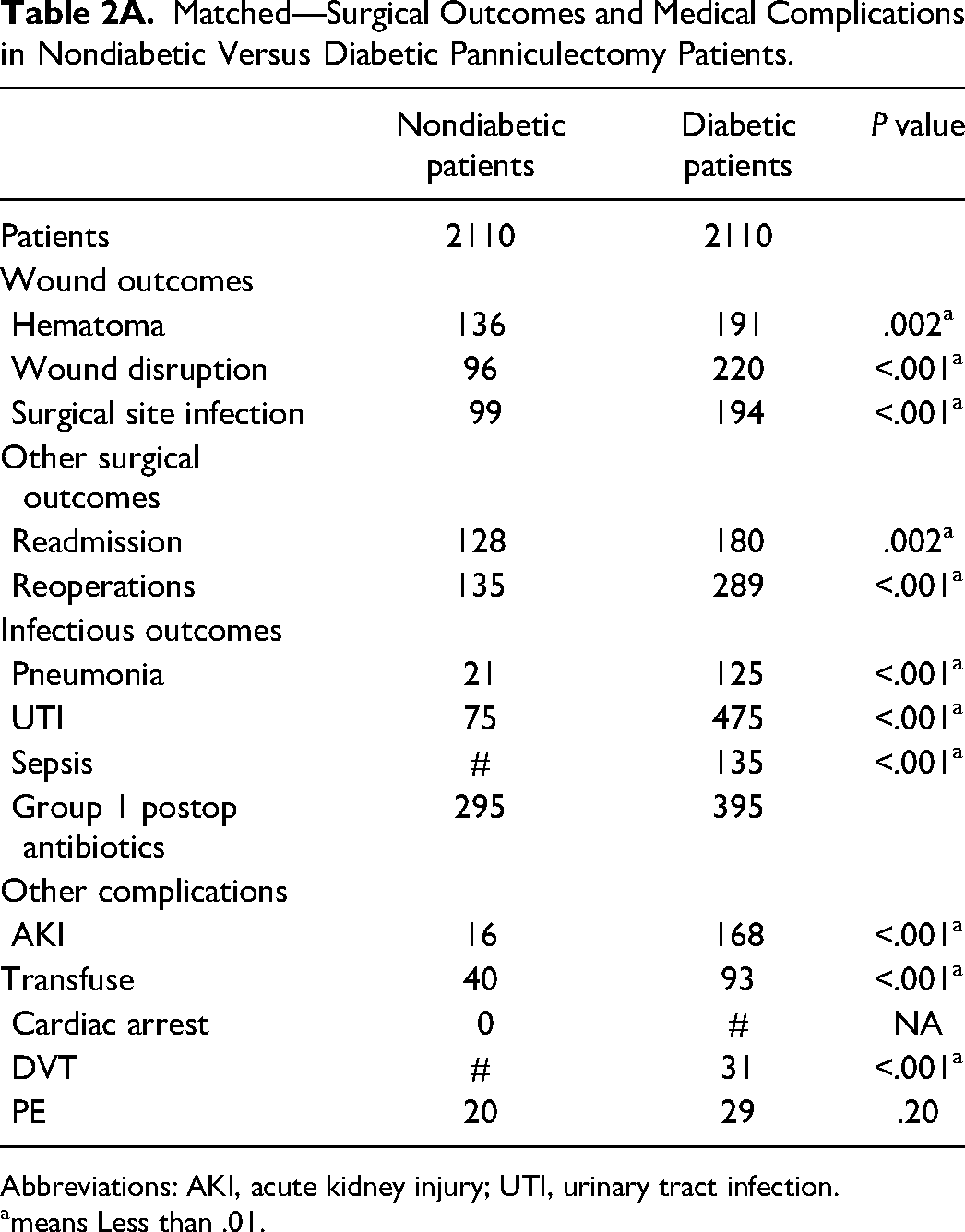
Abbreviations: AKI, acute kidney injury; UTI, urinary tract infection.
means Less than .01.
Diabetic patients were then stratified into insulin-dependent and noninsulin-dependent as evidenced by Table 3. Although there was no significant difference in surgical wound complications between either group, there was a notable increase in rates of readmission (12.4% vs 8.8%, P < .001), urinary tract infections (UTIs; 28.5% vs 22%, P < .001), sepsis (10.9% vs 5.7%, P < .001), and the incidence of acute kidney injury (AKI; 17.4% vs 8%, P < .001) in insulin-dependent diabetics. Furthermore, tobacco was identified as a clear risk factor with regard to all wound-related complications in both diabetics and nondiabetics (P < .001).
Complete Cohort-Insulin Versus No Insulin Use in Diabetic Panniculectomy Patients.
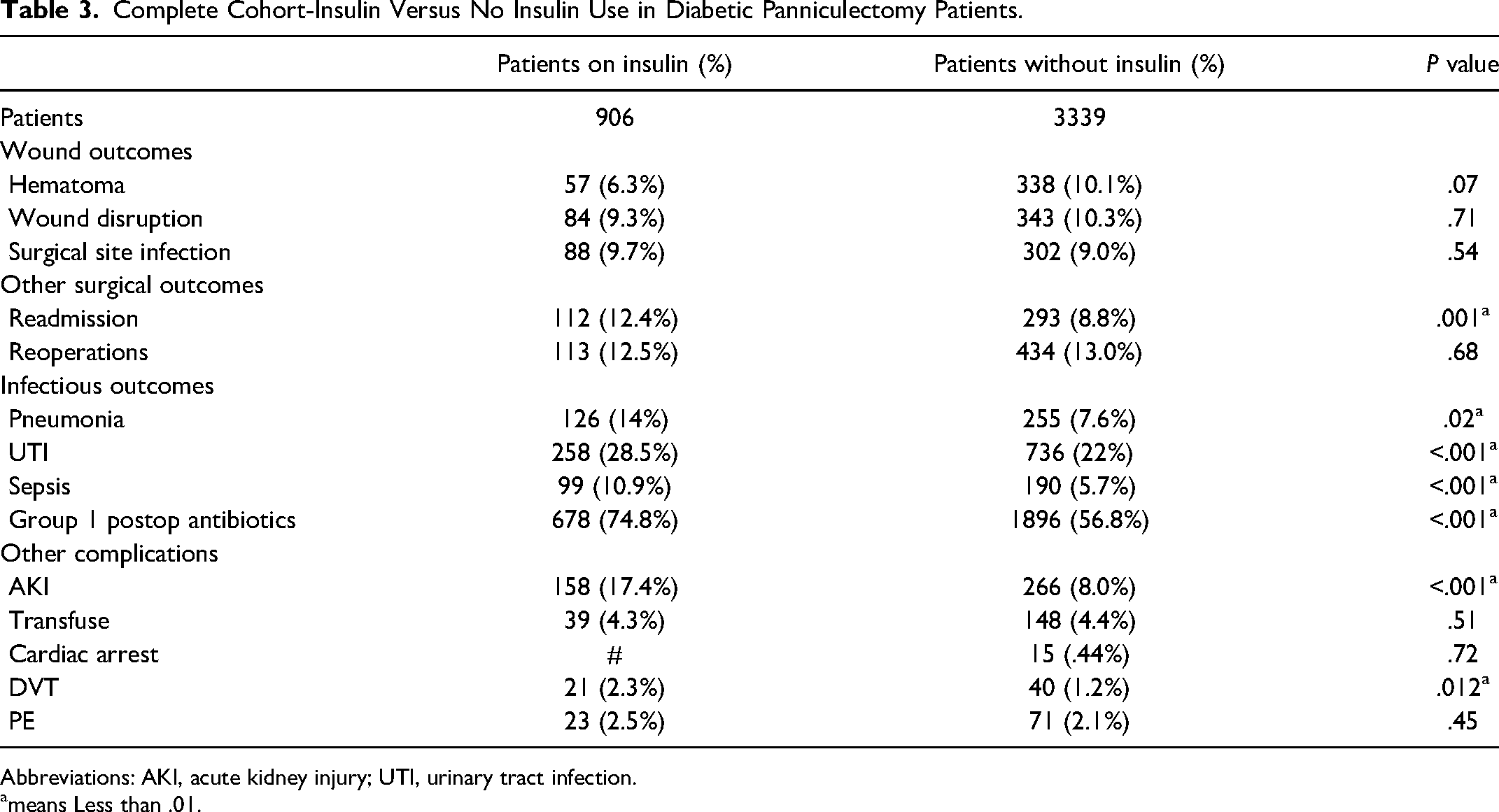
Abbreviations: AKI, acute kidney injury; UTI, urinary tract infection.
means Less than .01.
Discussion
Our study assessed early post-operative outcomes in panniculectomy patients and specifically evaluated these outcomes in diabetic populations. Although there are a number of articles in the current literature that establish obesity as a risk factor in developing complications following a panniculectomy, there are surprisingly few articles that address the relationship between diabetes and panniculectomy itself. The articles that do address diabetes remain controversial, and many of the existing studies do not separate abdominoplasties from panniculectomies.
Cammarata et al found that diabetes was in fact a statistically significant independent risk factor for post-operative wound complications and overall complications following an abdominal panniculectomy. 11 The notable study by Kantar et al found that although there seemed to be an association between diabetes and wound complications overall, diabetes was only a statistically significant, independent risk factor for the development of wound dehiscence alone. 12 Conversely, Zavlin et al demonstrated that patients with metabolic syndrome were overall at a significantly higher risk of post-operative complications in general, but diabetes alone was not a statistically significant risk factor. 13 In a retrospective study that involved 25 478 abdominoplasties, Winocour et al determined that diabetes mellitus itself was not a significant risk factor in the development of major complications. 10 However, this study addressed abdominoplasties instead of panniculectomies. Furthermore, the frequency of diabetes in this particular study was only 2.8% and the authors did suggest that the low prevalence of diabetes is likely due to the fact that the patients that chose to undergo this cosmetic procedure were in good health overall.
In our study, our univariate analysis comparing complications in patients with and without diabetes demonstrated that patients with diabetes had a higher incidence of statistically significant associated medical problems (Table 1). When matched for cardiac complications, CCI, age range, and gender, however, COPD, HTN, obesity, and CKD stood out as comorbidities that occurred in greater frequency within the diabetic population.
Our second univariate analysis comparing complications in diabetics versus nondiabetics demonstrated that patients with diabetes had a higher incidence of statistically significant associated medical problems (Table 2). This was true for almost all surgical and medical complications, once patients were matched by heart complications, CCI, age range, and gender (Table 2A). We chose to match for these variables to try to eliminate other comorbidities as a confounding factor. Interestingly, the number of patients with COPD was proportionally increased in patients with diabetes along with diabetic patients who contracted pneumonia. Although it might seem like there's a clear connection between the increase in COPD and the increase in pneumonia, it is prudent to consider the potential association of COPD and diabetes. 14 Thus, it is all the more important to investigate the role that diabetes may play in a panniculectomy patient.
The only article in the literature that addresses insulin-dependent diabetics and panniculectomy patients is the article by Sereti et al which suggests that insulin resistance is not improved following a panniculectomy. 15 Our study found that patients on insulin had worsened outcomes; specifically, patients that were on insulin had increased incidences of UTIs, AKI, had increased episodes of sepsis, and also had an overall increased need for antibiotics.
The existing literature looks at all patients that undergo panniculectomies and identified tobacco use and diabetes as risk factors but does not evaluate the risk factors of the diabetic panniculectomy patient individually.10–13 Our multivariate analysis demonstrated that diabetic patients in general had worsened outcomes, in that they had increased surgical site infections, wound dehiscence, hematomas, and had an increased need for reoperation (Table 4). Furthermore, in diabetic patients, tobacco abuse, COPD, and CKD were found to be a statistically independent risk factor for all wound-related complications (Table 5). This is a new finding, as prior literature has looked broadly at panniculectomy patients, regardless of diabetic status.
Multivariate Regression Analysis of the Effect of Diabetes on All Wound-Related Complications in the Total Panniculectomy Population.
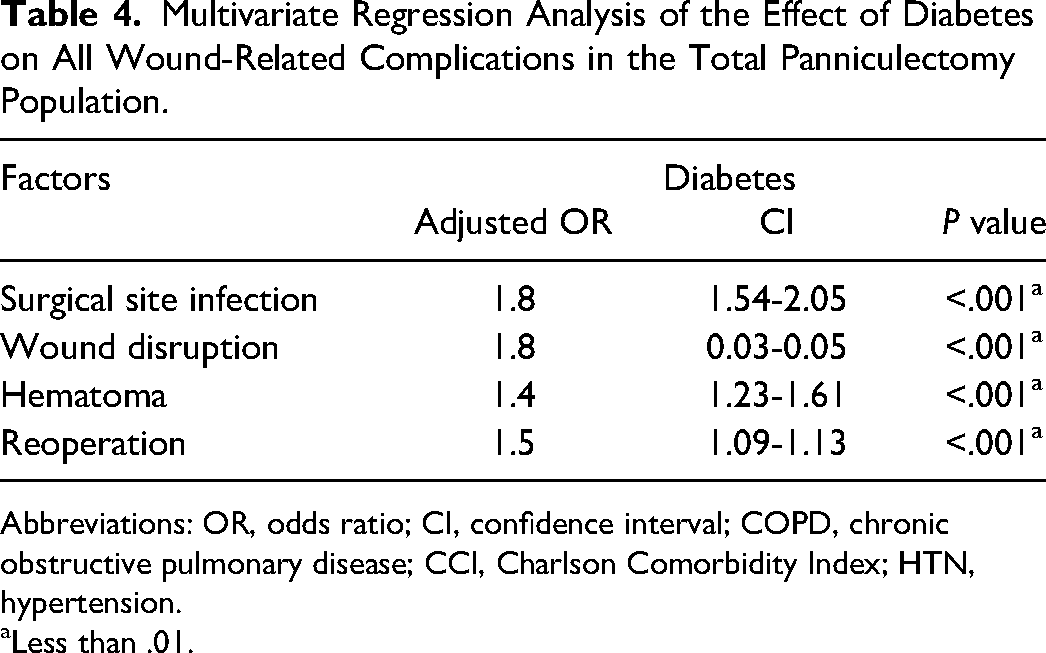
Abbreviations: OR, odds ratio; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CCI, Charlson Comorbidity Index; HTN, hypertension.
Less than .01.
Multivariate Regression Analysis of Wound-Related Complications in Diabetics.
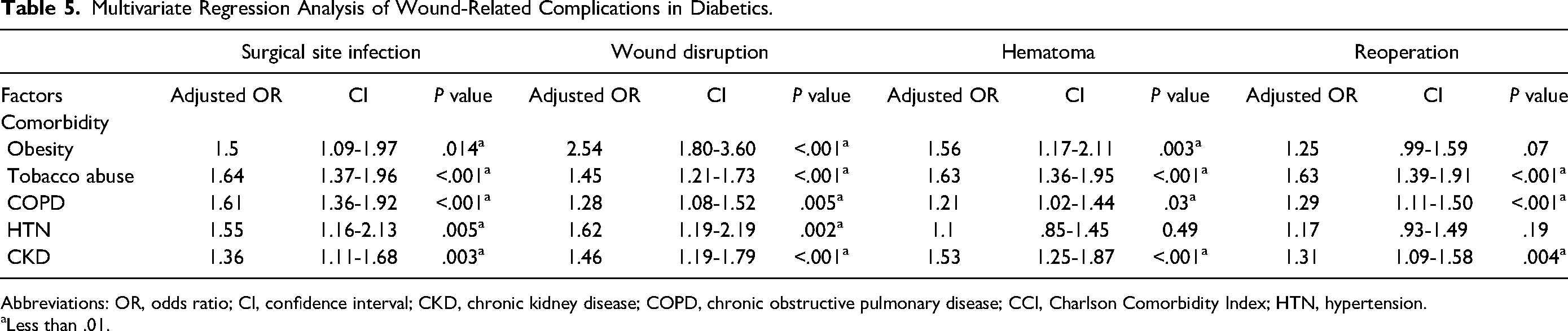
Abbreviations: OR, odds ratio; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CCI, Charlson Comorbidity Index; HTN, hypertension.
Less than .01.
Obesity has been well-established as an independent risk factor following a panniculectomy, but its impact on specific post-operative complications is less clear.3,10 Our study found that obesity was statistically significant in the diabetic panniculectomy patient for developing wound disruption, surgical site infection, as well as for developing a hematoma, but not for needing reoperation.
Data regarding HTN and potential complications in the panniculectomy patient is inconsistent.10,13,16 However, the article by Kantar et al shows that diabetic panniculectomy patients did have a higher rate of HTN compared to those who were nondiabetic, which was reflective of our data. 12 Although the study by Kantar et al did not specifically evaluate whether or not HTN could be a risk factor, our multivariate regression analysis did demonstrate that HTN was a statistically significant independent risk factor in developing a surgical site infection as well as wound dehiscence within the diabetic panniculectomy population.
In spite of the risk of morbidity, most patients have a high desire to undergo this operation and also maintain a high level of post-operative satisfaction.17–20 The benefits from undergoing this procedure span from everything from improved psychological status to better hygiene. Having said this, it is the responsibility of the surgeon to ensure maximum preoperative optimization by means of smoking cessation and blood sugar control. The findings from this study can assist as a guide for preoperative planning and preparation, and patients must have a clear understanding of the potential risks in undergoing this procedure.
Limitations
Limitations of the database prevented us from obtaining individual numbers such as body mass index, perioperative blood glucose levels, or hemoglobin A1c, and thereby stratifying our patients by such numbers; such limitations exist because of the nature of obtaining information from a large-volume national insurance database. Although we controlled for end-organ damage in our population, no conclusion can be drawn between the degree of diabetes mellitus and the severity of outcomes; in other words, the increased level of complications may be secondary to the severity of their individual disease process, rather than those with well-controlled diabetes. Furthermore, details regarding operative technique, size of specimen, or complications during surgery were unavailable to us. It also should be noted that we were unable to distinguish inpatient from outpatient use of insulin so we were unable to determine whether the patients that were on insulin were truly insulin-dependent outside of an acute setting.
Conclusion
Diabetes is often tied closely to obesity, which presents as a 2-fold problem in the panniculectomy patient. The evaluation of diabetes within the panniculectomy patient demonstrates that diabetic patients are at higher risk of developing post-operative complications, including readmission, reoperation, and other surgical complications. Not only does this study closely examine this aforementioned relationship but it also demonstrates worse outcomes, particularly in those who are insulin-dependent, in patients with diabetes. Our analysis highlights the importance of optimizing modifiable preoperative risk factors in patients that wish to undergo an abdominal panniculectomy in order to ensure safe and ideal outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.