
Abstract
Introduction
Since Illouz's landmark presentation in 1982 during the American Society of Plastic Surgery meeting, liposuction has experienced a remarkable rise.1–4 Today, liposuction represents one of the most commonly performed aesthetic procedures with a 31.9% rise in frequency from 2014, and ∼1 billion dollars spent annually in the United States alone. 5 Throughout its evolution, suction-lipoplasty has undergone a variety of modifications and additions as newer technologies, knowledge of anatomy, fluid dynamics, instruments, and techniques continue to evolve. 6
Although generally seen as a relatively benign intervention, the procedure is not without its complications. Multiple publications, each with their respective focus, design, and limitations, have provided unique insight on adverse events associated with liposuction, including a host of minor and major complications, both local and systemic, and procedure-specific or anesthesia-related. 7 A database inquiry of 4534 patients undergoing liposuction reported a total complication rate of 1.5%. 8 In contrast, a survey study encompassing 1249 procedures reported an overall complication rate of 9.3%, 9 while a retrospective analysis of 655 patients reports an overall complication rate of 22.3%, 10 with no major complications when liposuction was performed alone. While such large-scale primary studies can shed valuable insight into the rate of major complications and adverse sequelae encountered in aesthetic liposuction, by nature of study design and publication bias, these efforts may fall short in providing accurate insight into the rate of common complications frequently encountered in aesthetic surgery practice.
The objective of this study is thus to quantify the reported rate of relatively common complications associated with aesthetic liposuction through a meta-analysis of published primary clinical studies, with an emphasis on local cosmetic-related adverse events, and to address any inherent limitations in the evaluated literature which may pose a challenge to this effort.
Methods
Search Strategy
A systematic review and subsequent meta-analysis were carried out in full accordance with the Cochrane Handbook for Systematic Reviews of Interventions, 11 as well as the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 12
The MEDLINE via Pubmed, Embase, and The Cochrane Central Register of Controlled Trials databases were queried. The following keywords were used: (“Liposuction” or “suction lipectomy” or “lipoplasty”) in combination with (“complications” or “adverse events”). A manual citation search followed through relevant retrieved articles and key journals to supplement the initial protocolized search.
Primary screening was conducted based on title and abstract review, and relevant articles subsequently underwent full-text review. Screening was performed by 2 independent reviewers. The authors resolved eligibility disagreements by means of consensus. Data extraction was carried out by 2 reviewers for analysis. Key data, such as study design, nature of intervention, sample size and patient factors, perioperative setting, anesthesia protocol, mean lipoaspirate volume, and proportion of patients with outcomes of interest were extracted (ie contour irregularities, seroma, hematoma, infection, tissue loss or necrosis, pigmentary changes, as well as other complications in addition to the total number of patients with complications), when available.
Eligibility Criteria
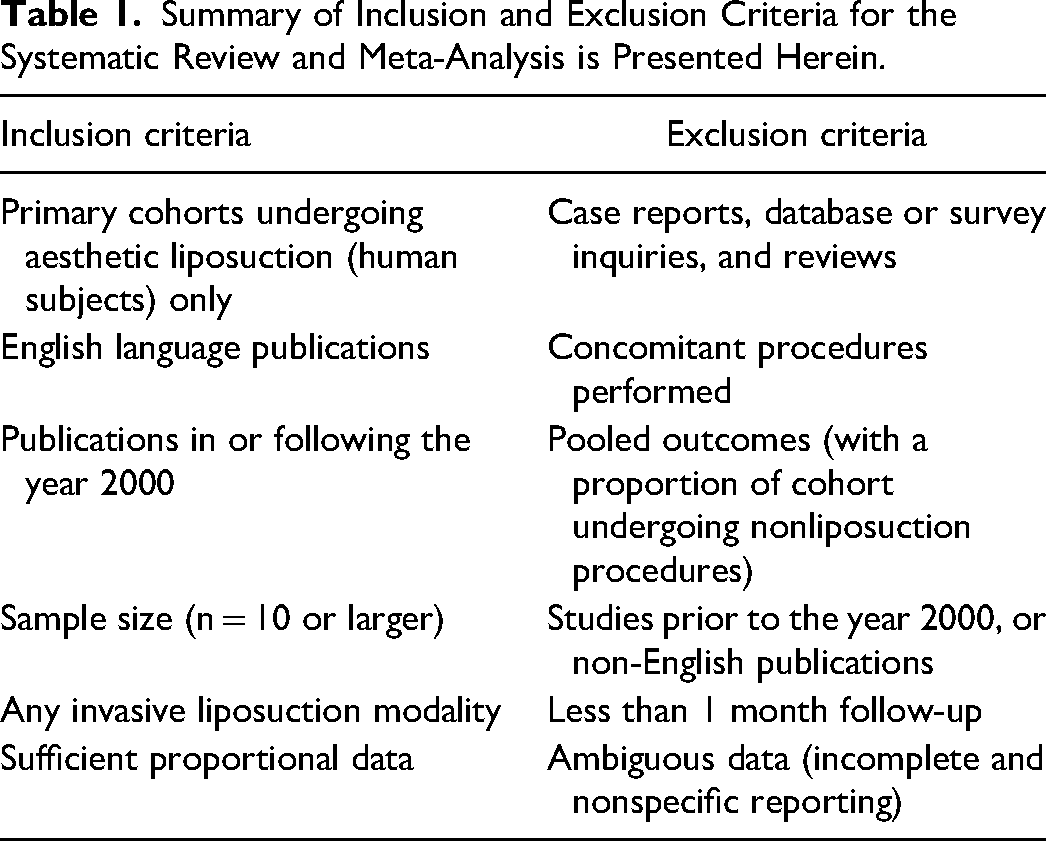
Original primary research articles, including experimental and observational designs, containing patient cohorts that underwent exclusive aesthetic liposuction of any body site (including liposuction-only breast interventions), utilizing any invasive modality, with sufficient, extractable, unambiguous reporting on complications, published in English after the year 2000 were included. Publications were excluded if substantial data was missing, or if the patient cohort underwent liposuction for nonaesthetic purposes, liposuction with cointerventions, or the pooling of outcomes with concomitant procedures was done. Case reports, reviews, surveys, background, and database articles were also excluded, as were publications with <1 month of follow-up. If a study contained multiple arms, data from only those that fit the inclusion criteria were extracted. Cohorts containing patients selected based on a specific outcome were excluded, as were cohorts with <10 patients to avoid publication bias and overreporting on complication rates, respectively (Table 1).
Summary of Inclusion and Exclusion Criteria for the Systematic Review and Meta-Analysis is Presented Herein.
Defining Complications
Major complications were aggregated and defined mainly as a systemic adverse event that may potentially be life-threatening, or require urgent pharmaceutical or surgical intervention. Included as well were “organ-threatening” complications, for example. direct visceral organ injury, optic neuropathy, or named major nerve-sectioning (Table 2).
Classification of Complications, as Either Major or Minor, is Presented. Major Complications Were Defined Mainly as a Systemic Adverse Event, Potentially Life-Threatening or Requiring Urgent Pharmaceutical or Surgical intervention.
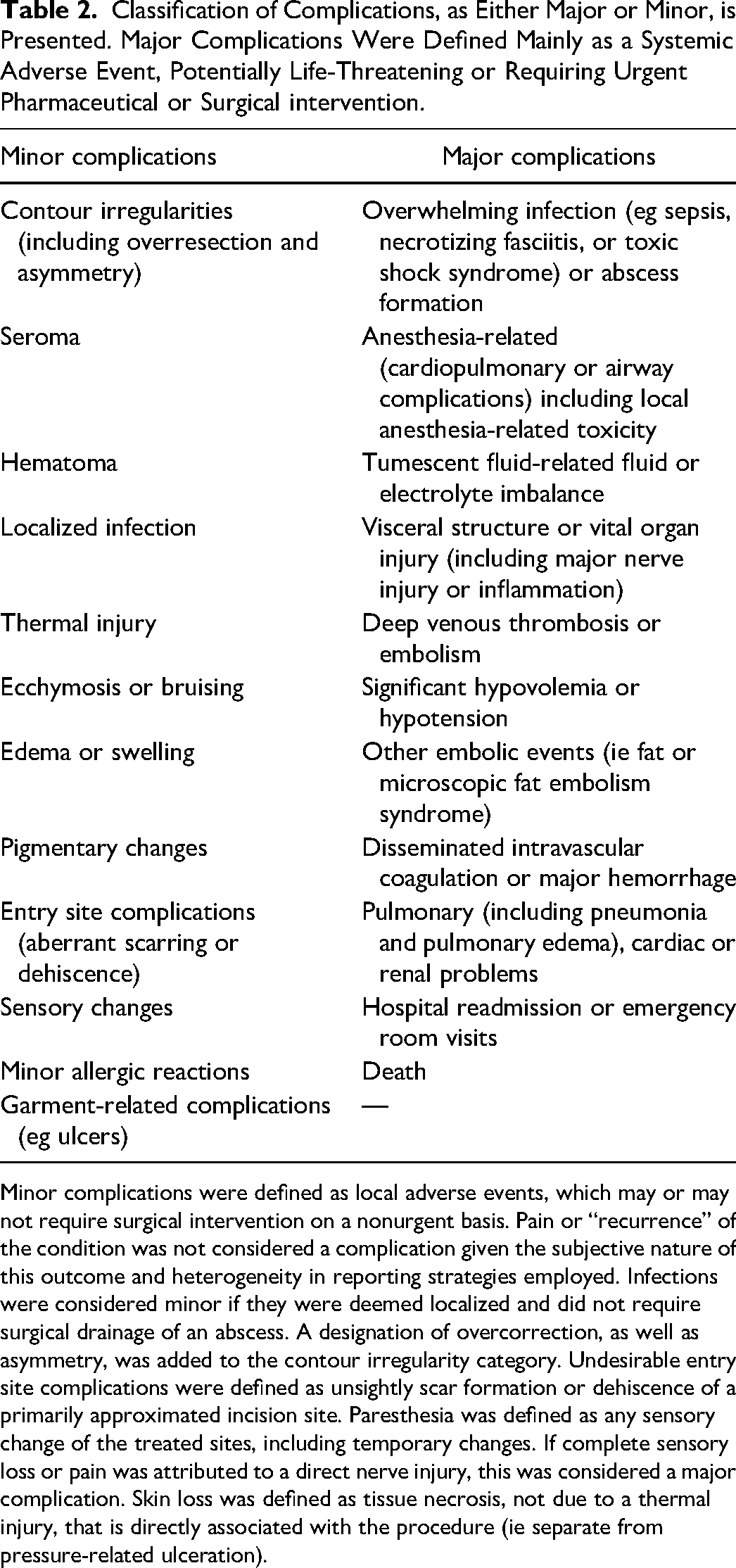
Minor complications were defined as local adverse events, which may or may not require surgical intervention on a nonurgent basis. Pain or “recurrence” of the condition was not considered a complication given the subjective nature of this outcome and heterogeneity in reporting strategies employed. Infections were considered minor if they were deemed localized and did not require surgical drainage of an abscess. A designation of overcorrection, as well as asymmetry, was added to the contour irregularity category. Undesirable entry site complications were defined as unsightly scar formation or dehiscence of a primarily approximated incision site. Paresthesia was defined as any sensory change of the treated sites, including temporary changes. If complete sensory loss or pain was attributed to a direct nerve injury, this was considered a major complication. Skin loss was defined as tissue necrosis, not due to a thermal injury, that is directly associated with the procedure (ie separate from pressure-related ulceration).
Minor complications were reported separately, when statistically feasible. These were defined as local adverse events that may or may not require surgical intervention on a nonurgent basis (Table 2). Pain or “recurrence” of the condition was not considered a complication given the subjective nature of this outcome and heterogeneity in reporting strategies employed. Infections were considered minor if they were deemed localized and did not require surgical drainage of an abscess.
Undesirable entry site complications were defined as unsightly scar formation (eg hypertrophic or widened scars) or dehiscence of a primarily approximated incision site. Paresthesia was defined as any sensory change (ie hypo or hyperalgesia, dysesthesia) of the treated sites, including temporary changes. If complete sensory loss or pain was attributed to a direct nerve injury, this was added to the major complication incidence. Skin loss was defined as tissue necrosis, not due to a thermal injury, that is directly associated with the procedure (ie separate from pressure-related ulceration). A designation of overcorrection, as well as asymmetry, was added to the contour irregularity category. Suction-assisted and power-assisted liposuction (PAL) cohorts were excluded from the analysis of thermal injury incidence to avoid underestimation of incidence, given that this complication is unique to laser- and ultrasound-assisted liposuction (UAL). Infrequent complications were not reported separately, however, were still included in the calculation of the overall complication rate. The overall complication rate was calculated as the total number of complications (as per the author’s criteria) as a weighted proportion of the total number of patients within each cohort.
Statistical Analysis
Meta-analyses were performed using the aggregated data. Proportions were calculated as the ratio of the number of affected patients to the total sample size. Proportions are provided with the corresponding 95% confidence intervals (CIs). For all studies, a meta-analysis was performed for each outcome. Combined with the inspection of forest plots, the I2 index, and the τ2 statistics were utilized to investigate statistical heterogeneity. Heterogeneity based on the I2 statistic was defined as low (25%), moderate (50%), and high (75%). Given the high degree of heterogeneity, the authors proceeded with a random-effects model for overall complications with a logit transformation. Studies from which a specific complication rate was not extractable with confidence were excluded from a subgroup analysis of that particular outcome. Publication bias was not statistically pursued given the substantial heterogeneity in addition to the design of a meta-analysis of proportions. Meta-analyses and sub-analyses were performed using the R software (The R Project for Statistical Computing, R version 3.2.1). 13
Results
A total of 3768 papers were retrieved after the removal of duplicates; 60 papers were included in the final synthesis following abstract and full-text review. An elaboration on the search strategy, as well as the inclusion and exclusion process, is presented in Figure 1. Table 3 provides a summary of all primary articles included in the meta-analysis.6,14–74 Most studies were of an observational design. Within included cohorts, the majority of procedures utilized either suction-assisted liposuction (SAL) or laser-assisted liposuction (LAL), followed by UAL, radiofrequency-assisted liposuction (RFAL), and PAL. Among studies that provided sufficient procedural and patient demographic data, the overwhelming majority performed low to moderate volume aspiration (<5 L) and female patients constituted the vast majority of included subjects. Twelve studies strictly used general anesthesia for all patients, while the majority used a combination tumescent anesthesia with or without sedation, and 7 cohorts were variable.
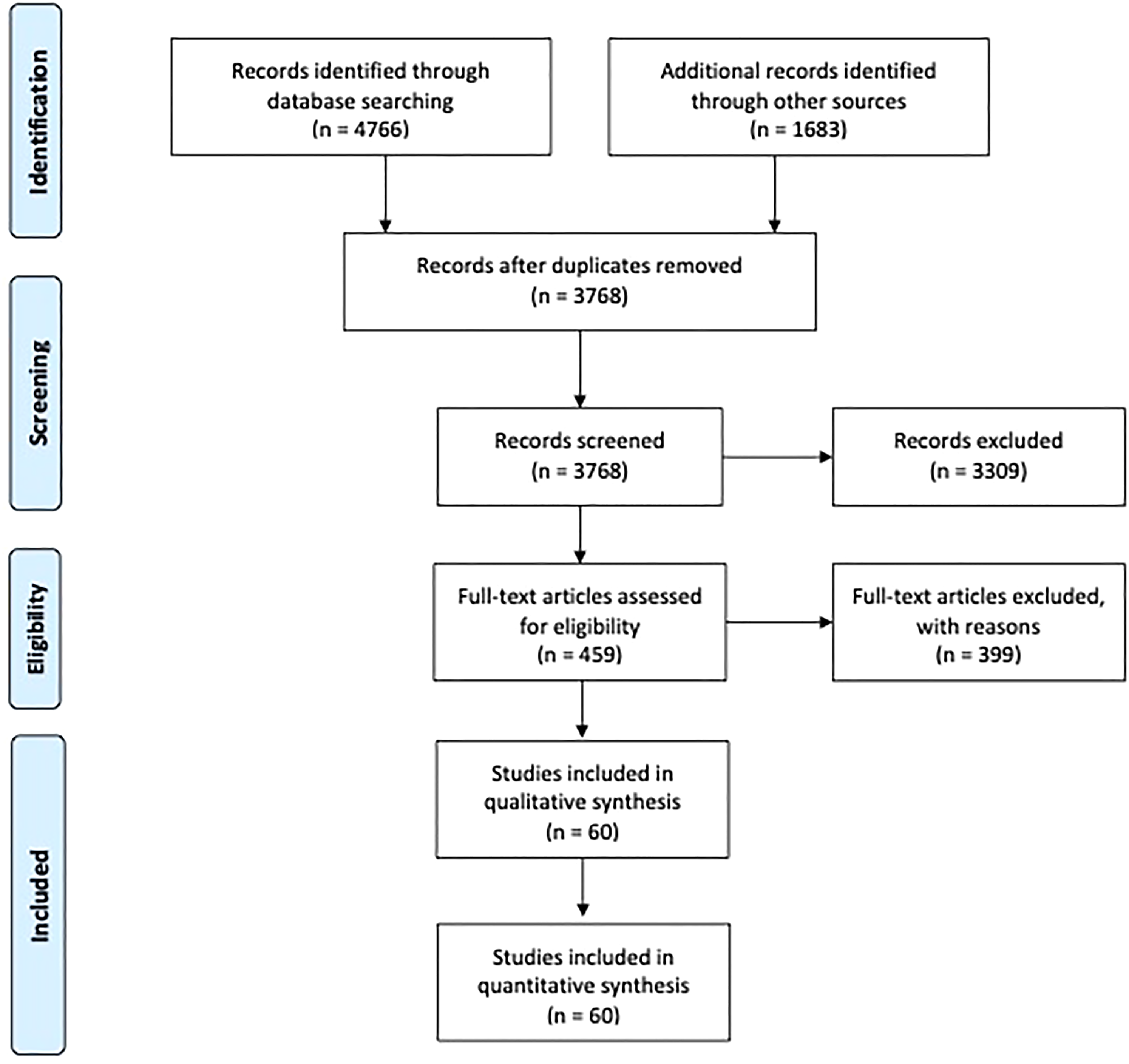
Flowchart of the search strategy, conducted in accordance with the Cochrane handbook for systematic reviews of interventions, as well as the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines
Synthesis of Studies and Outline of Study Characteristics That met the Inclusion Criteria for the Meta-Analysis.
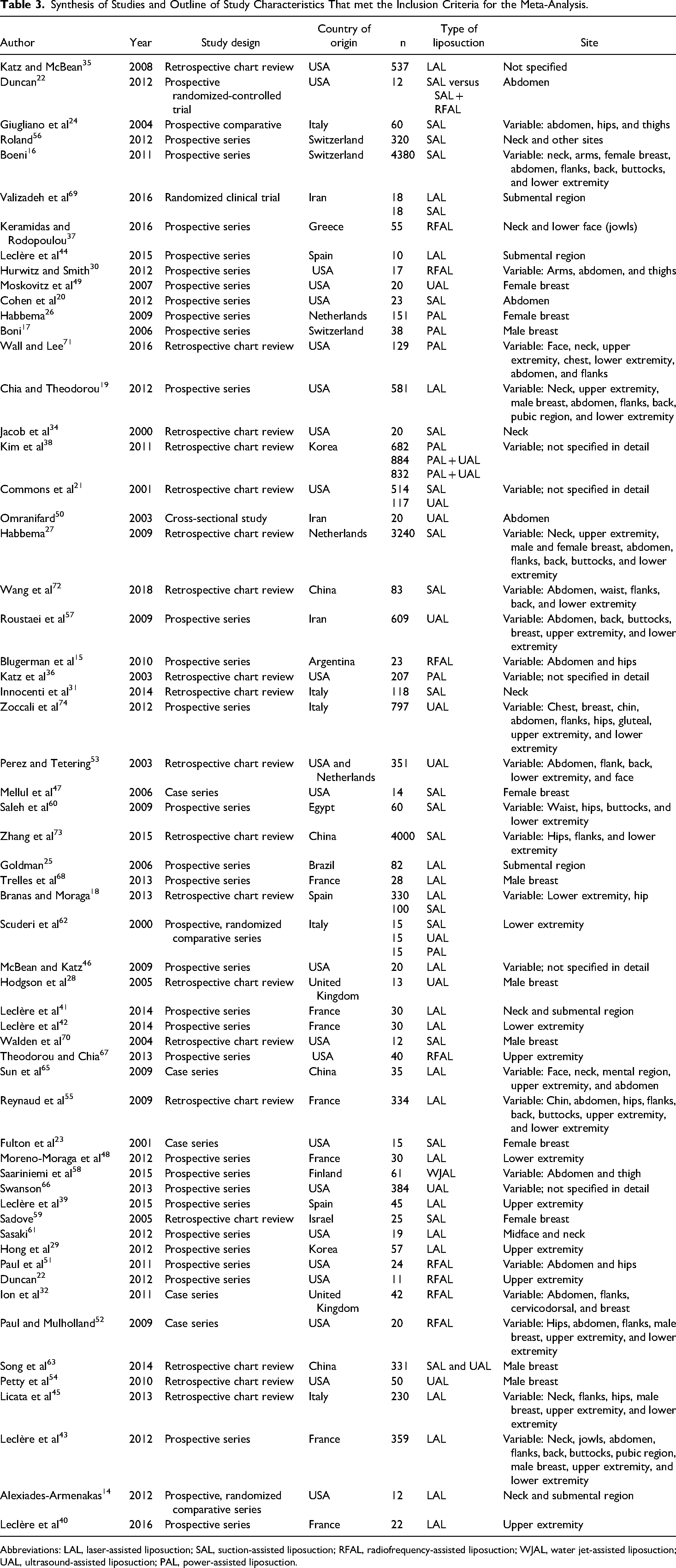
Abbreviations: LAL, laser-assisted liposuction; SAL, suction-assisted liposuction; RFAL, radiofrequency-assisted liposuction; WJAL, water jet-assisted liposuction; UAL, ultrasound-assisted liposuction; PAL, power-assisted liposuction.
Overall complications: The rate of total complications (including major and minor complications) was 12% (95% CI 8%, 16%). When the incidence of ecchymosis and edema were removed from the analysis, the total rate was reduced to 6% (95% CI 4%, 8%). In accordance with the definitions set for the present study, the total major complication rate was 1% (95% CI 0%, 1%) and the total minor complication rate was 5% (95% CI 4%, 8%) (Table 2). Forest plots are presented in Figures 2 to 4, and Supplementary Figure 1.
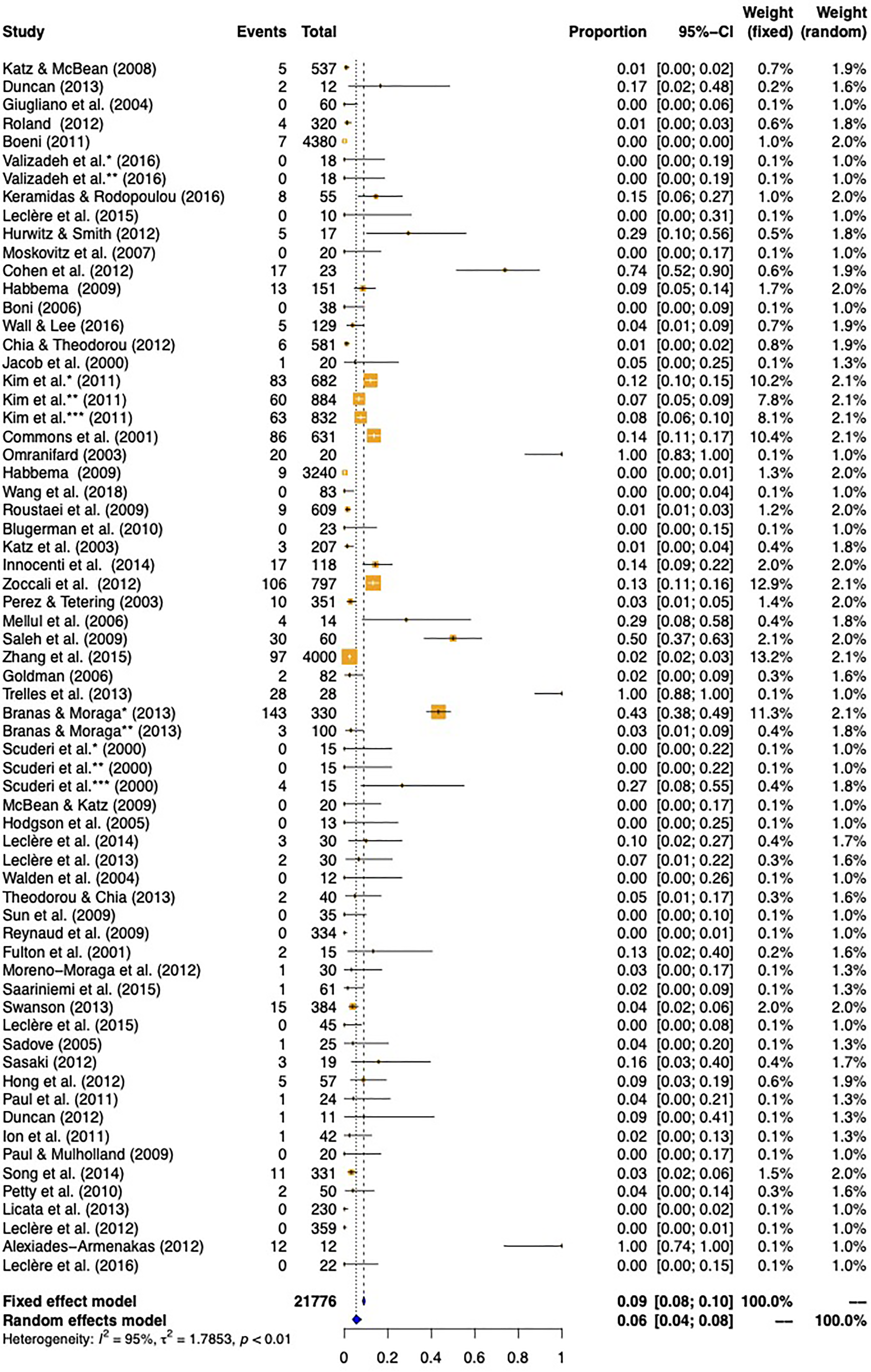
Total complication rate, excluding ecchymosis and edema.
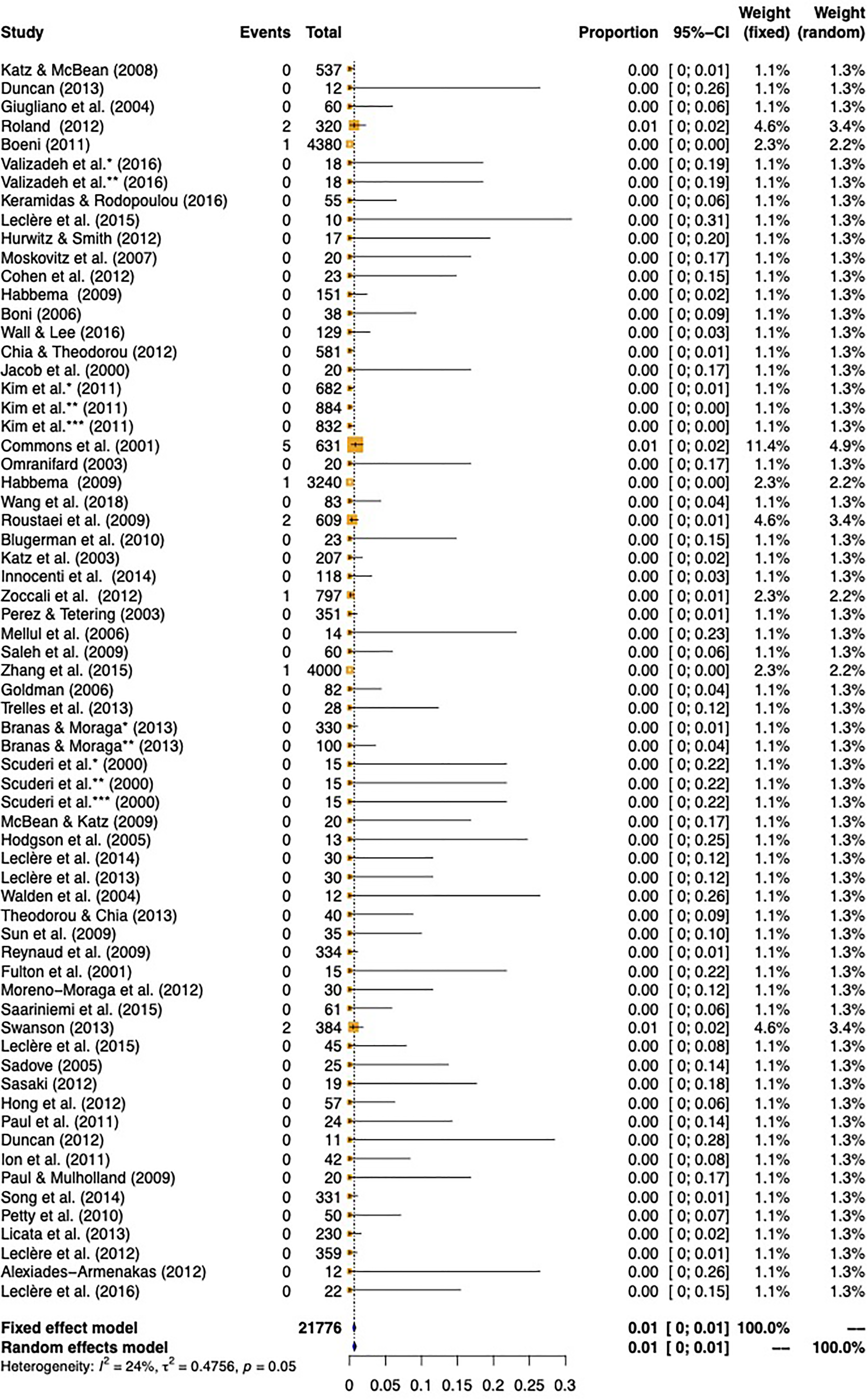
Total major complication rate as determined using both the fixed-effects and random-effects models for meta-analysis of articles meeting the inclusion criteria for review.
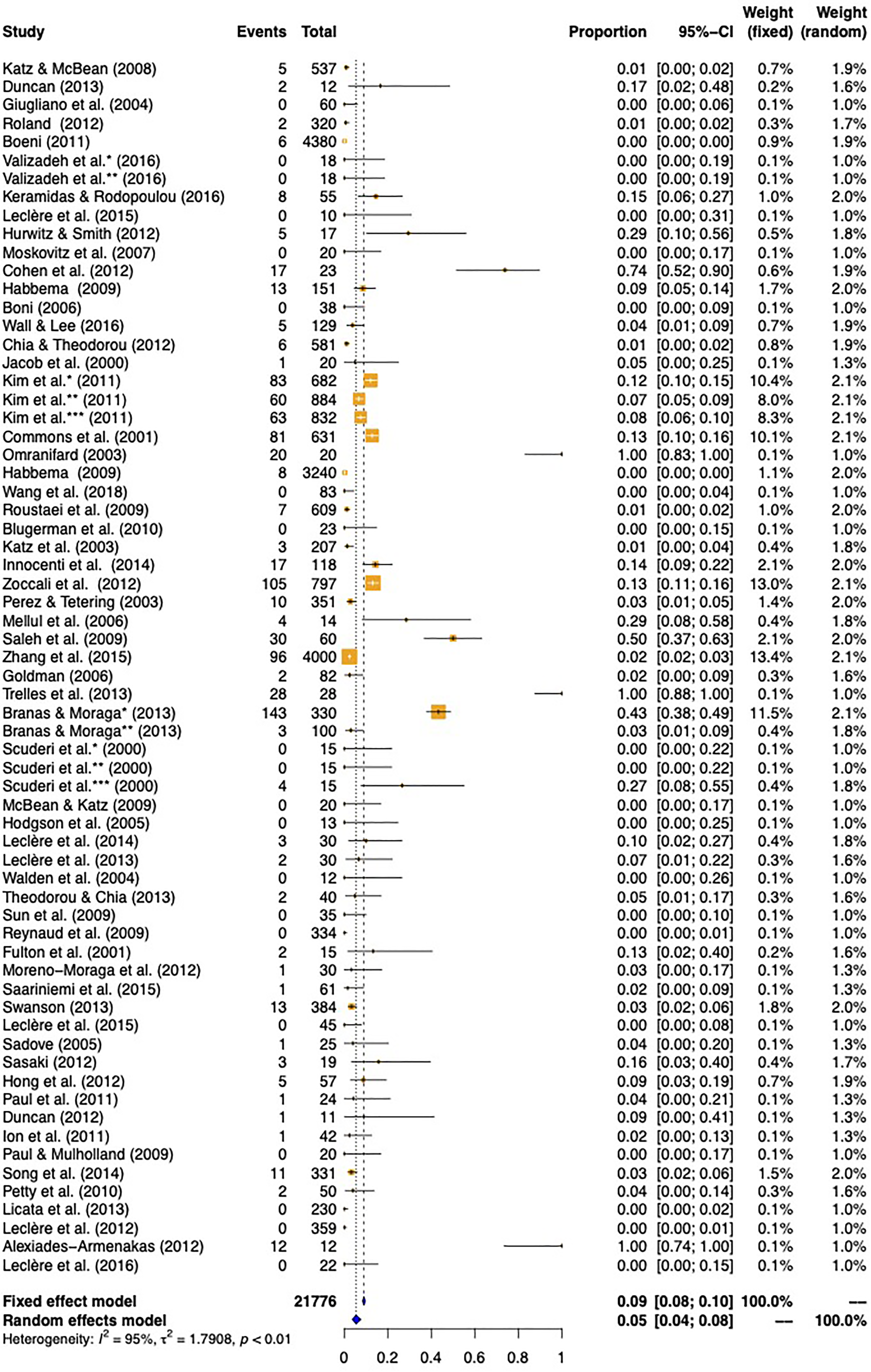
Total minor complication rate as determined using both the fixed-effects and random-effects models for meta-analysis of articles meeting the inclusion criteria for review.
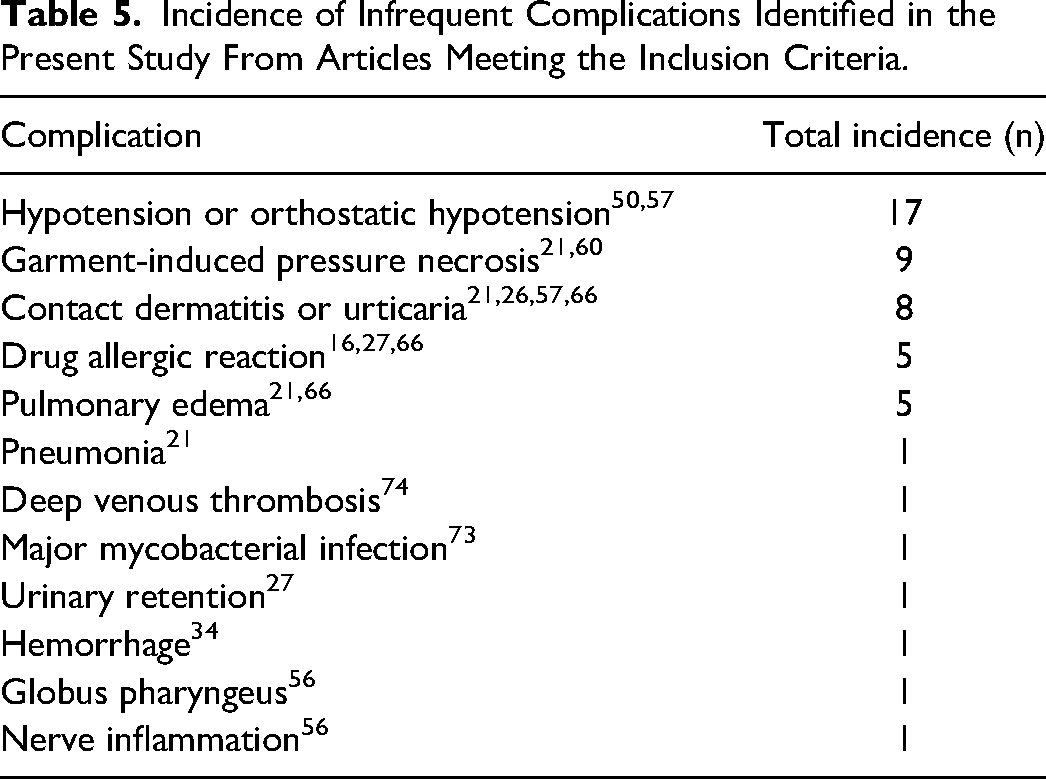
Specific complications: The reported rate of ecchymosis was established to be 3% [95% CI 1%, 7%); swelling as 2% (95% CI 1%, 3%), contour irregularity as 2% (95% CI 1%, 2%); seroma 1% (95% CI 1%, 2%); hematoma 1% (95% CI 0%, 1%); surgical site infection 1% (95% CI 1%, 2%); and thermal injury as 1% (95% CI 1%, 2%). Naturally, no patients in the SAL or PAL groups suffered any thermal injury, in contrast to 7 out of 2809 patients in the LAL group (0.25%), 22 out of 4092 in the UAL group (0.54%), 4 out of 250 patients in the RFAL (1.6%) affected. Pigmentary changes occurred at a rate of 1% (95% CI 1%, 1%), with no incidence in the RFAL treatment group. Paresthesia occurred at rate of 1% (95% CI 0%, 2%); fibrosis, nodularity, and induration at 1% (95% CI 1%, 2%); skin loss at 1% (95% CI 1%, 2%); and undesirable entry site complication at 1%, as per the definition established in the current study (95% CI 1%, 1%) (Supplementary Figures 2-13; Table 4). No deaths were reported; 1 case of thrombophlebitis was acknowledged with no embolic event. 74 Other infrequent complications not included in specific outcome analysis are summarized in Table 5.
Overall, Major, Minor, and Individual Complication Rates, as Identified and Synthesized in the Present Meta-Analysis Using a Random-Effects Model and Meta-Analysis of Proportions, are Presented Herein.
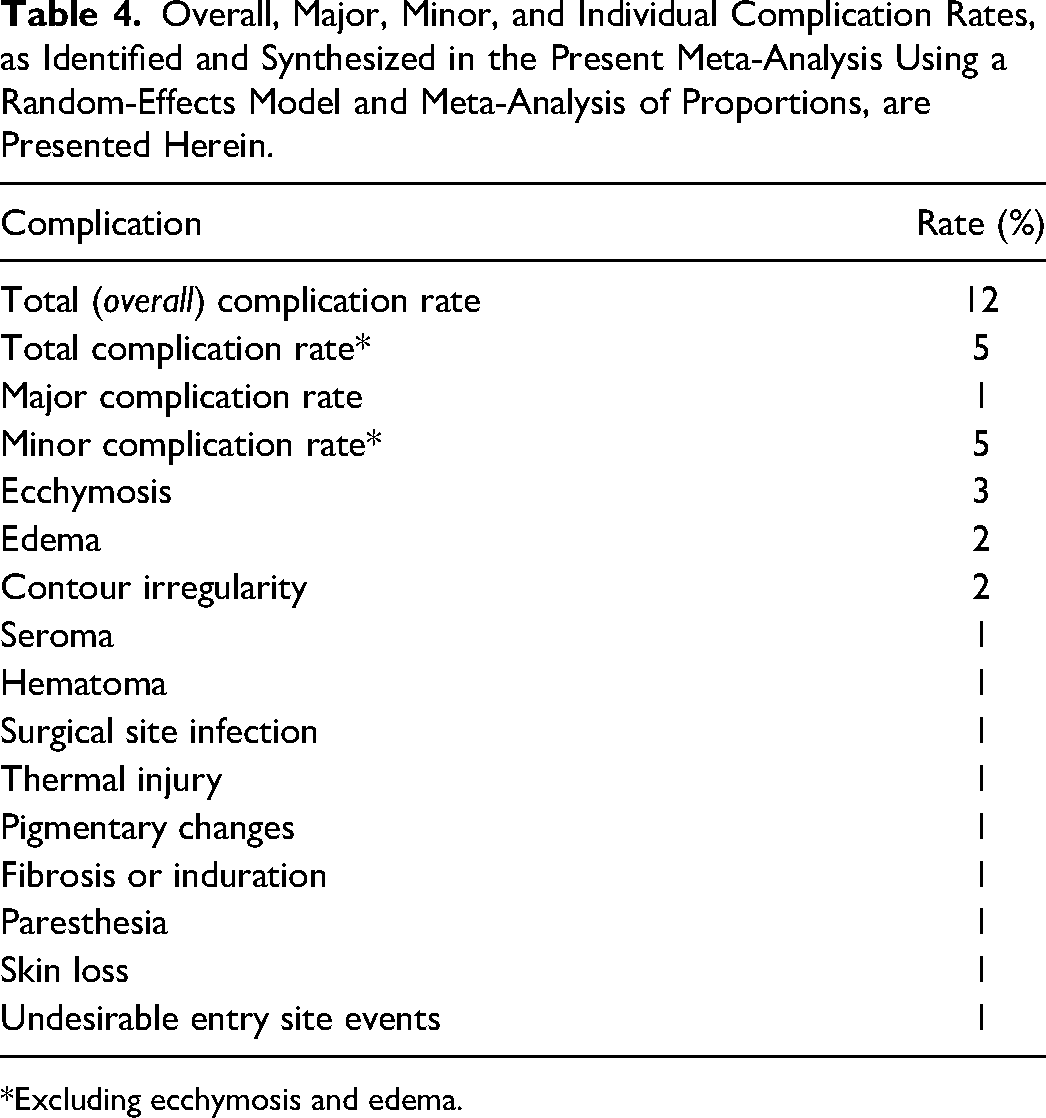
*Excluding ecchymosis and edema.
Incidence of Infrequent Complications Identified in the Present Study From Articles Meeting the Inclusion Criteria.
Discussion
This study seeks to provide further insight into the complication profile associated with aesthetic liposuction and aid clinicians in providing full disclosure within the spirit of informed consent, as well as explore the present state of the literature to identify procedure- and patient-specific factors associated with higher complications. Given the high degree of heterogeneity identified, the results of this meta-analysis should be interpreted in consideration of complication rates established in previous reports, all the while acknowledging the contrast between authors and centers, and potential subjectivity as to what constitutes a complication, as opposed to an undesirable aesthetic result, or an inevitable consequence of the operation (eg in the case of ecchymosis or edema).
As alluded to by Matarasso, 1 the lack of a central registry impairs exact reporting on complications associated with liposuction. Indeed, the published complication rate of certain adverse events may display a dramatic variability. 8 Nevertheless, the underlying factor common to many published cohorts is that liposuction tends to be a safe procedure when performed by trained hands.10,75 In a database inquiry of 4534 patients who underwent liposuction, Chow et al 8 reported a total complication rate of 1.5%. Contrasted to 9.3% in a survey encompassing 1249 procedures, 9 to 22.3% in a retrospective analysis 10 of 655 patients, with no major complications when liposuction was performed alone. The results of this study, including major, minor, and overall complications are within the range of reported rates in the literature.
As noted, the exclusion of edema and ecchymosis from aggregated analyses stems from the nature of included data; while some authors may mention that all patients experienced some degree of edema or bruising, culminating in 100% “complication rate,” others may disregard these as being an inevitable consequence of the operation, and not a complication per se (unless severe enough or persistent beyond a certain subjective limit). Thereby, the inclusion or exclusion of these complications may effectively inflate, or deflate the results, respectively, depending on the surgeon’s point of view. The rate of complications associated with the different liposuction modalities was not included given the notable difference in the number of studies and patients related to each group, precluding reliable interpretation.
Contour irregularities have been cited as the most common complication in suction lipectomy.76,77 In a large database study, Matarasso et al 77 demonstrated a 9.2% rate of irregularities, while another large survey study maintained a rate of 0.26%. 78 Cardenas-Camarena 10 reported a palpable irregularity rate of 7.36% and a visible irregularity rate of 3.25% (although some patients within the cohort underwent concomitant abdominoplasty).
In a commonly cited survey, Pitman and Teimourian 9 reported results of 612 plastic surgeons (1249 liposuction procedures) with the following rates: hypoesthesia (2.6%), seroma (1.6%), edema (1.4%), pigmentation (1%), hematoma (0.8%), infection (0.6%), and skin slough (0.2%). The previously mentioned rates are by no means an exhaustive coverage of all published figures. They do, however, serve to demonstrate the tangible discrepancy within the literature, as well as the fact that although subject to heterogeneity, the results of this study are not anomalous.
Finally, it remains pertinent to consider that while these complications are reported on in terms of prevalence, the severity of these complications, measures necessary for their rectification, and their financial burden, in addition to the patient-specific perception of these complications and their detriment on patient satisfaction and quality of life were all not taken into account. These factors remain essential aspects to consider alongside the incidence data presented to adequately assess the risk–benefit profile of this procedure on a patient-by-patient basis.
Limitations
To appreciate and adequately infer the results of this study, a thorough elaboration of its limitations should be noted. The inclusion and exclusion criteria chosen will undoubtedly introduce bias, such as limiting results to the English language, for example. Due to the set limitation on follow-up time (as the primary aim of the study was to look for aesthetic and local outcomes), some cohorts were excluded, effectively eliminating certain studies with shorter follow-up which may have provided more complete insight on intraoperative or immediate postoperative outcomes such as blood loss, need for transfusion, metabolic derangements, anesthetic-related events or immediate postoperative pain, for example.
The current state of the literature on this specific topic, with a relative lack of randomized-controlled trials (RCTs) and a general dominance of lower quality studies, dictates the quality of evidence and nature of pooled analysis characteristics. Given the type of desired outcome, namely complications, and the relative deficiency in experimental designs in this domain, it was not feasible to restrict study designs to RCTs alone, or even case-control designs. A substantial portion of our data set was retrieved from retrospective or prospective cohorts and case series, which, by design, are better equipped to capture the incidence of complications among a patient population. However, these studies tend to carry biases inherent to their designs (eg underreporting or information bias, publication bias), besides the frequent occurrence of incomplete data. In fact, multiple cohorts were excluded due to incomplete data, but could have been included should further (presumably readily available) data would have been provided. To that end, the authors recommend that future studies report on the incidence of each of the major and minor complications discussed in this manuscript, as presented in Table 2. Furthermore, should there exist an absence of certain complications, the authors recommend that the incidence is reported on and specified as zero, rather than omitting their mention as a whole. This serves to provide the readership with confidence in the authors’ reporting on complications and would permit the more detailed and inclusive synthesis and meta-analysis of data from future cohorts.
The decision to exclude case reports rests within the fact that these, albeit valuable in providing insight into rare, possibly catastrophic events, cannot be used to estimate proportional data. The detriment, however, is that rare adverse events: massive infections, visceral perforation, anesthetic complications, and fatalities, among others, will be invariably missed or understated. This accentuates the importance of interpreting the findings of the present study in consideration of data provided by previous reports using different strategies, such as database queries or large-scale surveys, which may better capture these complications. On the other hand, owing to the method of calculation of proportions with the available data, a certain amount of inflation will likely occur, considering that while some patients will have more than 1 complication, the total number of complications was still calculated out of a proportion of the total sample size. Surveys and database studies were excluded to limit duplication, and subsequent overstating, of complication rate, which again was detrimental to the major complication rate.
Studies conducted prior to the year 2000 were excluded; the rationale being an attempt to add a sense of homogeneity given the differences in techniques, instruments, technologies, and operative protocols that have evolved and changed over the years. Yet the authors recognize that although some studies were published after the year 2000, multiple included cohorts did, in fact, encompass patients that underwent surgery as far back as 1994.
The main challenge faced in the present study was the inconsistency pertaining to what constitutes a true complication according to the primary articles assessed. While some authors might mention a detailed summary of undesirable outcomes and proportions of which, others would acknowledge the presence of adverse events with broad, nonspecific descriptions. Data from the latter cases were avoided. Moreover, some may consider a complication exclusively as an undesirable outcome that requires a corrective intervention, operative or otherwise. Some publications did not provide numeric, prevalence data concerning specific complications, rather, provided measures of central tendency concerning visual analog or Likert scales. Data from these studies were not considered since no insight on incidence could be provided for the meta-analysis.
Finally, the authors acknowledge the heterogeneity pertaining to within-cohort and between-cohort differences in patient characteristics (eg age, body mass index, gender or race), perioperative protocols (eg anesthetic medications and techniques, warming, antibiotics, chemical or mechanical venous thromboembolism prophylaxis), intraoperative technique or site involved (eg breast vs abdomen) and amount of aspirate (low-volume vs high-volume), employed modality of ultrasound, settings of which (hospital or private practice), in addition to instruments as well as differences in the amount and constituents of wetting solutions. All of which coalesce, culminating in a state of heterogeneity that cannot be ignored when interpreting the results of this study; a variability that has been elaborated on by other authors as well. 79 Due to these limitations, the authors were unable to confidently proceed with a meta-regression to explore possible predictive factors of certain or overall complications such as the amount of aspirated fat, type of anesthesia, facility, modality of liposuction or specific patient demographics, among others.
Conclusion
In experienced hands, liposuction continues to be a safe aesthetic procedure; the overall complication rate was determined to be 12% in the present study by means of a meta-analysis of primary clinical studies. Special attention to full-disclosure in operative consent is paramount for maintaining a solid physician–patient relationship and appropriately managing patient expectations. Plastic surgeons should continue to probe the most recent evidence and employ appropriate judgment regarding patient selection, operative protocols, and technologies. Substantial heterogeneity in outcome reporting for liposuction exists which may impair reliable data synthesis. Although not always feasible, further large-scale, robust, and collaborative efforts are needed to clearly define and establish complication rates, as well as predisposing patient- and procedure-specific factors, which may require further attention to continue improving the safety profile of this procedure.
Supplemental Material
sj-jpg-1-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-1-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-2-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-2-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-3-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-3-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-4-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-4-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-5-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-5-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-6-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-6-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-7-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-7-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-8-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-8-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-9-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-9-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-10-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-10-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-11-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-11-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-12-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-12-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Supplemental Material
sj-jpg-13-psg-10.1177_22925503221078693 - Supplemental material for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-jpg-13-psg-10.1177_22925503221078693 for Complications of Aesthetic Liposuction Performed in Isolation: A Systematic Literature Review and Meta-Analysis by Albaraa Aljerian, Jad Abi-Rafeh, Thomas Hemmerling and Mirko S. Gilardino in Plastic Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.