
Abstract
Introduction
Intravenous drug use and other forms of substance abuse fall under the umbrella of addiction. The American Psychiatry Association (APA) characterizes addiction as “a brain disease that is manifested by compulsive substance use despite harmful consequences”. 1 Mental health disorders are a leading cause of disease burden, costing the American health care system a notable $89 billion in 2013. 2 As the most common sites for infection are the antecubital fossa and hand, plastic surgeons, the experts of hand, wrist, and soft tissue, are often consulted to perform surgical debridement and incision and drainage. 3 Over the past ten years, hospitalization secondary to intravenous drug use (IVDU)-related complications has increased, from 4 to 9 per 100 000 people between 1993 and 2010. 4 The upper extremities are the most common site for injection, making people who inject drugs more susceptible to soft tissue abscesses, osteomyelitis, and septic arthritis, all of which may lead to pain and disability.5,6 Mortality rates among intravenous drug users are also a cause for concern. Canadian epidemiological data suggested that people who inject drugs were at 13 and 54 times greater risk of premature mortality than the general population. 7 Individuals are highly likely to relapse, with relapse rates ranging from 40% to 60%, primarily driven by compulsive cravings for the substance. 8
A potentially important tool for plastic surgeons to use when addressing this specific patient population is the practice of motivational interviewing. Motivational interviewing (MI) is an evidence-based practice that has proven effective for supporting various behavioral changes, including those with substance use disorders. 9 Using traditional methods, physicians may encourage patients to stop injecting, but their advice may be met by resistance or noncompliance. 9 There is a large body of literature to suggest that MI may be useful in overcoming this resistance. Although a surgeon may be “time poor”, evidence suggests that brief interventions utilizing MI techniques are clinically and cost-effective in fostering behavior change in individuals with substance use disorders.10-12 This article explores the concept and process of MI and its potential role in facilitating behavior change by plastic surgeons in patients using intravenous drugs.
Definition of Motivational Interviewing
Motivational interviewing was defined by founders William Miller and Stephen Rollnick as “a person-centered counseing method for addressing the common problem of ambivalence about change”. 13 MI is an alternative to the traditional, paternalistic conversation model between the physician and patient. The goal of MI is to strengthen the patient's motivation toward achieving a change in behavior, leading to better health outcomes.
MI utilizes a conversational interviewing style to address ambivalence and perceived barriers that patients face when tasked with the need to change their behavior. 13 Rather than asserting a need for change and confronting the patient, a physician applying MI will seek to develop a collaborative partnership with their patients and co-develop achievable goals for change.
Evidence
Motivational interviewing has demonstrated effectiveness in facilitating behavior change when used by formally trained therapists. 14 A two-arm parallel randomized control trial comparing MI to a brief educational intervention among people who inject drugs demonstrated that at six months follow-up, participants in the MI group were at 50% fewer odds of reporting any risky injection behavior (odds ratio [OR] = .50; 95% CI = .13–.87). 15 A review of four meta-analyses suggested that MI may have a small to moderate effect in the context of substance use and dependence compared to no treatment (Cohen's d = .19 to .43). 16 Another systematic review with a median 12-month follow-up (range two months to 4 years) demonstrated that MI could be effective in brief encounters of only 15 min. 17 Short motivational interviews have also proven to be cost-effective compared to standard care.11,12 Additionally, there is a growing body of evidence suggesting health care professionals do not have to be formally trained therapists to practice MI effectively. Previous studies have supported the use of MI by obstetricians, 18 pediatricians, 19 general practice physicians, 20 dental professionals, 21 nurses, and dietitians. 22 However, there is no evidence evaluating the use of motivational interviewing by plastic surgeons to our knowledge.
What Is Motivational Interviewing? Principles and Practice
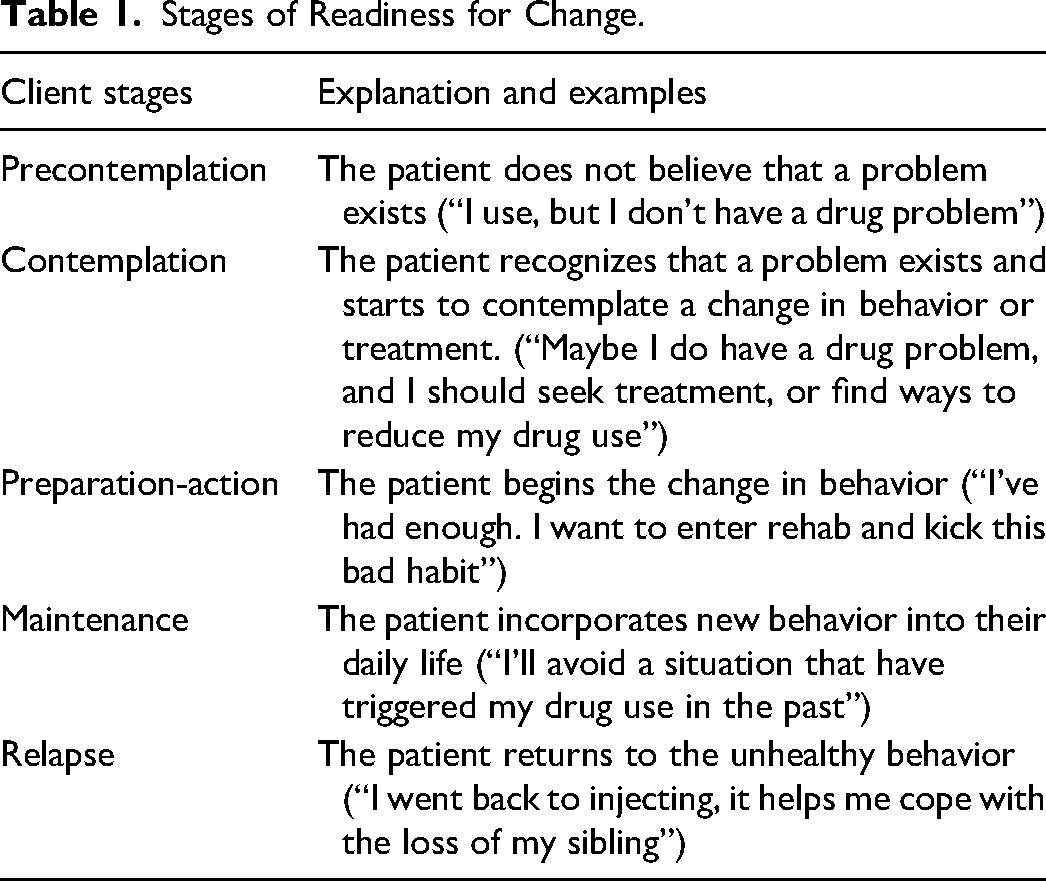
The objective of using motivational interviewing is to guide the patient as they move through the stages of readiness for change (concerning the targeted behavior)23,24 (Table 1). The objective is to enable the patient to move from the precontemplation stage to the maintenance or relapse stage.14,15
Stages of Readiness for Change.
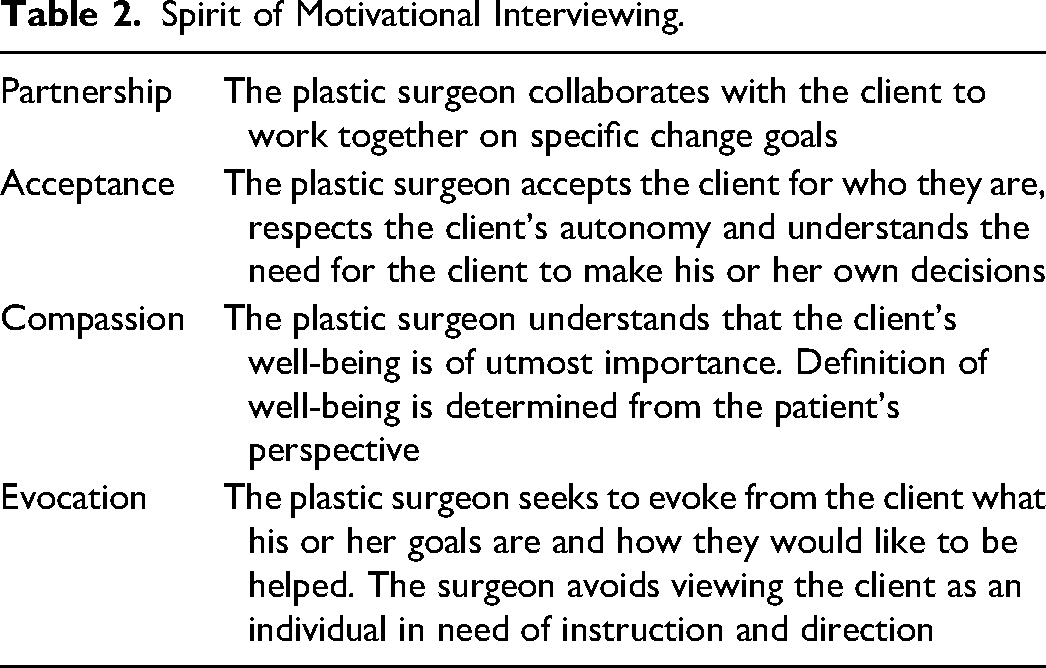
The overall spirit of MI is centered on empathy. 25 Empathy manifests in the relationship between the physician and patient in four ways: partnership, acceptance, compassion, and evocation (Table 2). 26 The founders of MI have commented that implementing MI strategies in the absence of the spirit of MI is ineffective. 23
Spirit of Motivational Interviewing.
Motivational Interviewing in Practice
The skills required for MI may appear simple, but the process takes practice, feedback, and commitment.
26
The plastic surgeon has three critical tasks:
reflective listening, eliciting “change talk,” offering information, feedback, and advice using MI principles.
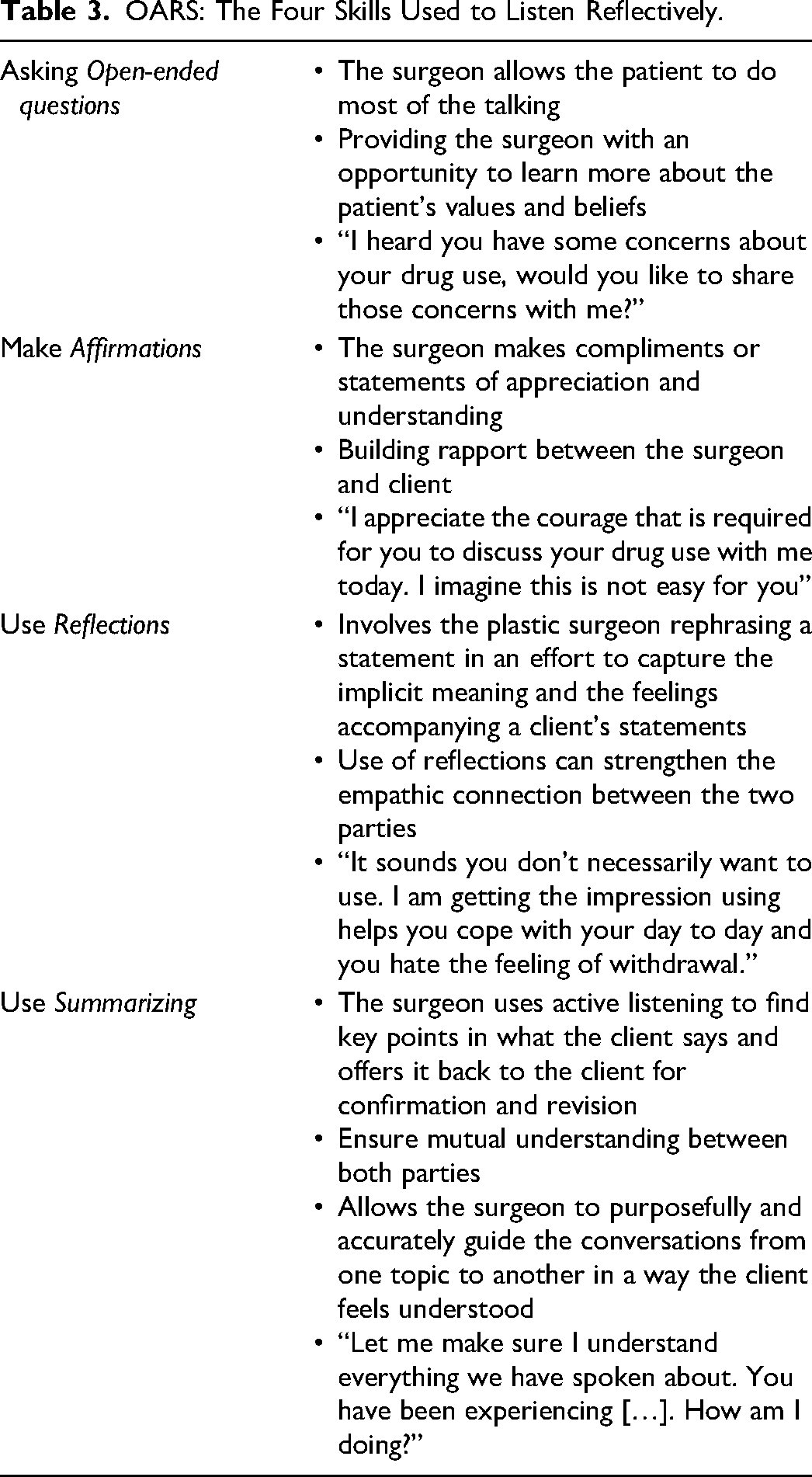
Reflective listening assists in building rapport and establishes the therapeutic relationship consistent with the spirit of MI. Reflective listening utilizes four skills represented by the acronym OARS (Open ended questions; Affirmations; Reflections; Summarizing) (Table 3).
25
OARS: The Four Skills Used to Listen Reflectively.
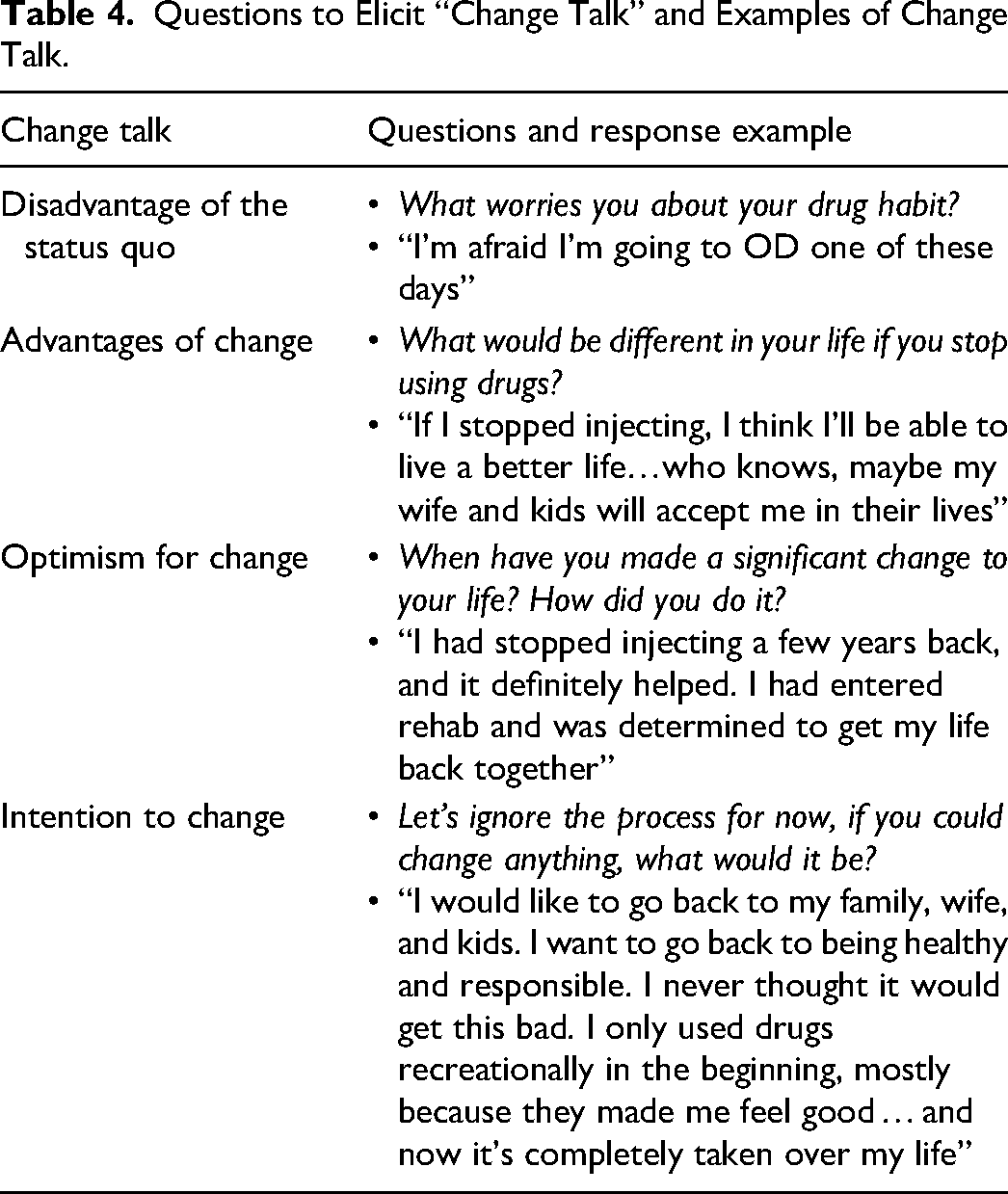
Change talk is a conversation with the patient that favors healthy behavior change.
26
Multiple strategies are available for eliciting change talk, but the simplest way is by asking a series of questions based on four categories
23
(see Table 4):
disadvantages of the status quo; advantages of change; optimism for change; and intention to change.
Questions to Elicit “Change Talk” and Examples of Change Talk.
Application of Motivational Interviewing in Brief Interactions
The time required for the implementation of a comprehensive MI intervention can be a challenge. A solution is to simplify the practice of MI for healthcare settings through four guiding principles.
23
The acronym RULE represents the following principles:
resisting the righting reflex; understanding your patient's motivations; listening with empathy; and empowering your patient.
Hall et al
27
described the “importance ruler,” “confidence ruler” and change plan as quick employable strategies to elicit change talk in brief interactions. The following script has been adapted from their commentary.
The “importance ruler” highlights discrepancies between a patient's current and ideal situations. For example:
Plastic surgeon: Think of a scale from zero to 10 of how important it is for you to stop injecting. On this scale, zero is not important at all, and 10 is extremely important. Where would you be on this scale?
Patient: 4
Plastic surgeon: Why are you at four and not zero? What would it take for you to go from a 4 to a 7? 27
The “confidence ruler” focuses on the patient's strengths, thereby building their confidence in their ability to change. 27 For example:
Plastic surgeon: “On a scale from zero to 10—where zero is not confident at all and 10 is extremely confident in your ability to stay away from Fentanyl—where would you be on this scale?”
Patient: 6
Plastic surgeon: Why are you at 6 and not zero? What would it take to take you to go from 6 to a higher number?
Lastly, it is crucial to work collaboratively on a change plan. Utilizing the principles of MI, surgeons should not immediately advise their patients, as is characteristic of the paternalistic approach.
27
They should remind patients that they are their own experts. Using empowering language such as, “You are the expert on you, so I’m not sure I am the best person to judge what will work for you. But I can give you an idea of what the evidence shows us and what other people have done in your situation”
27
may prove helpful in facilitating behavior change. Other useful phrases include the following:
27
“It sounds like things can't stay the same as they are. What do you think you might do?” “What changes were you thinking about making?” “Where do we go from here?” “What do you want to do at this point?” “After reviewing all of this, what's the next step for you?”
Discussion
Considerable barriers prohibit the implementation of MI, which may include time pressures, patient complexity, lack of training, and the culture of the “medical expert”. 27 Medical education at both the undergraduate and postgraduate levels has not traditionally included the principles of motivational interviewing in their curriculum. A training course in MI can be as brief as three days and still improve interactions between patients and healthcare professionals. 28 Moving away from the “specialty silo” approach in medical education and inviting experts from different fields for grand rounds and other interdisciplinary medical education activities are suitable approaches to facilitating the use of MI by plastic surgeons. 24
While it may not be feasible to implement MI in all patient interactions, using motivational interviewing where possible will serve plastic surgeons and their patients more effectively. During the minor procedure of evacuating a forearm abscess, there is an approximately 20–30 minute window where the patient is awake and may consider a lifestyle change under current circumstances. This opportunity to engage in productive conversations is often underutilized. Unfortunately, these vulnerable patients who receive medical attention are often met with stigmatizing attitudes, leading to an avoidance of the health care system. 29
The field of plastic surgery would benefit from the formal investigation of the effectiveness of motivational interviewing in facilitating behavioral change in patients who inject drugs. The study methodology could emulate previous randomized controlled trials. Such research would be useful in encouraging the utilization of MI by plastic surgeons. Although patients who inject drugs are the subject of this paper, MI can help other plastic surgery patients. A recent pilot randomized controlled trial on bariatric surgery patients demonstrated that MI was a feasible and effective intervention to improve dietary adherence, binge eating symptoms, and confidence for change. 30 Similarly, a 2016 systematic review 31 demonstrated improved outcomes related to smoking cessation, pain management, fatigue, and healthy eating habits following MI in cancer patients and survivors. Considering the many potential applications of MI by plastic surgeons, MI should be researched further in the context of plastic surgery. Programs with trained and dedicated MI counselors could be cost-effective and lead to better patient outcomes. There is also evidence to suggest that MI may also be especially beneficial for those who have experienced substance use relapse. 32 These findings strengthen the argument that MI can lower health system costs and better health outcomes for patients.
Conclusion
The complexity of a patient's medical and social comorbidities is highlighted when their addiction brings them into the tertiary care setting for a plastic surgeon's treatment. Using the principles of motivational interviewing ensures patients have positive encounters with the healthcare system when they are most vulnerable. Enhancing rapport may make patients more receptive to multidisciplinary care, involving addiction medicine and social workers who can offer continuing treatment. Importantly, research has demonstrated that early intervention is the most effective way to prevent someone with a substance use problem from becoming worse. 33
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.