
Abstract
Endometriosis is a chronic condition affecting 1 in 10 women of reproductive age. This review examines how endometriosis impacts women’s professional experiences, highlighting workplace challenges and identifying interventions to support their employment and well-being. A metasynthesis of qualitative studies was conducted, analysing data from 20 studies and 1241 women, using Thomas and Harden’s thematic synthesis to identify recurring themes and patterns. Several key challenges emerged including discriminatory behaviour from colleagues and employers, stigmatisation and a global lack of understanding. The psychological impact of these challenges included feelings of invalidation, shame and isolation among many women. Professional obstacles such as frequent absenteeism, diminished productivity and financial insecurity were also common. Flexible working arrangements and supportive workplace policies were found to be beneficial but were rarely implemented. To address these workplace challenges, comprehensive interventions are needed, including flexible work options, targeted employer training and public health campaigns to reduce stigma. Legal recognition of endometriosis as a disability could further ensure necessary protections and accommodations. Future research should prioritise the development and evaluation of these interventions to create more inclusive and supportive work environments for women with endometriosis.
Keywords
Introduction
Endometriosis is a chronic and debilitating condition affecting 1 in 10 women of reproductive age. 1 It is characterised by the growth of endometrial-like tissue outside of the uterus, which typically implants around the pelvic region on structures such as the ovaries, bowel, bladder and Pouch of Douglas. 2 For many, this can cause severe symptoms including cyclical and non-cyclical pelvic pain, lower back pain, digestive disturbances, bladder dysfunction, fatigue and comorbidities such as anxiety, depression and infertility. Endometriosis, also referred to as ‘the missed disease’, takes between 7 and 12 years to diagnose.3,4 Subsequently, this prolonged diagnostic period means women are less likely to receive adequate treatment and may experience disease progression and further impacts to quality of life that extend far beyond physical health alone. 5
Extensive studies have quantified the significant negative impacts of endometriosis on women’s professional lives, including substantial declines in work productivity and capability as well as limitations to career progression and salary growth.6–12
Nnoaham et al. 6 conducted a multi-national study including 1418 women and found an average loss of 10.8 h of work weekly, primarily attributed to reduced work effectiveness. Work-related impacts have profound societal economic ramifications, with a Canadian study estimating the average annual cost of endometriosis per patient to be $5200, 78% of which was attributed to lost work productivity and leisure time. 13
Despite advances in medical understanding and quantitative research, the social and professional impacts of endometriosis remain underexplored. This study aims to investigate these impacts, focussing on the lived experiences of women in the workplace and provide a comprehensive understanding into their perspectives using qualitative methodology. Specifically, the research objectives are a. To synthesise and understand the experiences of women with endometriosis in the context of their work environment and professional life and b. To understand the current workplace interventions that are in place to support women in managing their endometriosis.
Addressing these objectives may support the development of interventions and policies to improve the quality of life and professional outcomes for women with endometriosis.
Methods
This study is a qualitative systematic review and metasynthesis, conducted using thematic synthesis as described by Thomas and Harden. 38 This review followed the PRISMA 2020 guidelines for systematic reviews to ensure transparency and reproducibility of reporting. A completed PRISMA checklist 14 is provided as Supplemental Material File 1. Each stage of study identification, screening, eligibility and inclusion was documented and summarised in a PRISMA flow diagram (Figure 1). This review is registered in PROSPERO: CRD42024558835.
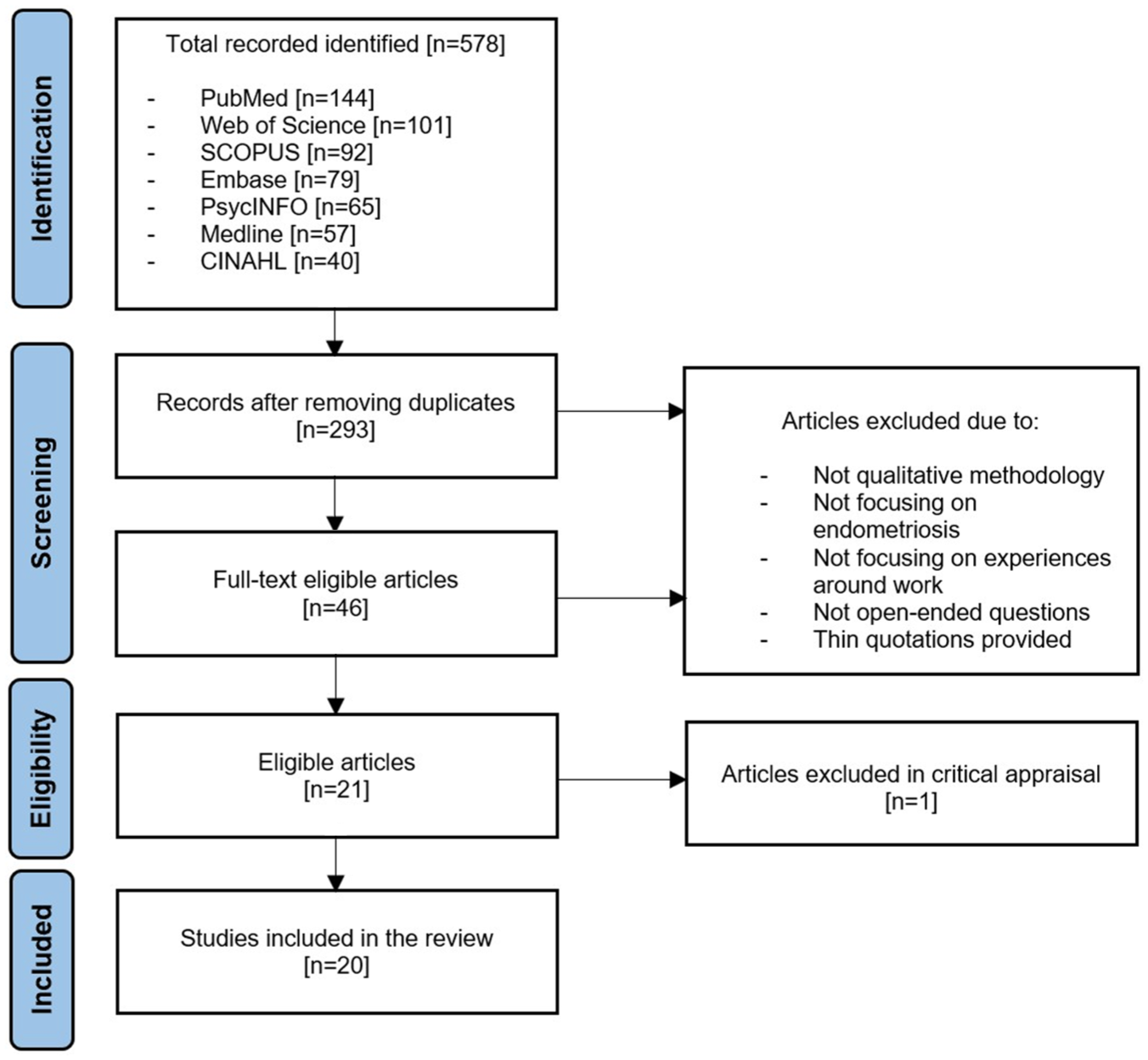
PRISMA 2020 flow diagram of study selection.
Search strategy
A systematic, critical review of qualitative research exploring the lived experiences of women with endometriosis in the workplace was conducted. Seven databases, which include a range of publications in social, behavioural and life sciences, were chosen to ensure a comprehensive search of the literature. These included PubMed, Web of Science, SCOPUS, Embase, PsycINFO, Medline and CINAHL. The search terms were free-text synonyms to ‘endometriosis’, ‘workplace’, ‘experiences’ and ‘qualitative research’, joined by Boolean operators (AND/OR). Cross-reference was also used to identify further papers missed during the original search. The keywords and search terms were modified, depending on the database, to increase the search results. The literature search was conducted between January 2024 and March 2024 by the first author, and an independent researcher cross-checked a single database to ensure the process was comprehensive and systematically applied.
Inclusion and exclusion criteria
The inclusion criteria were adult women (16+ years old) diagnosed with endometriosis using recognised diagnostic criteria. Adolescents, elderly women, partners and healthcare professionals were excluded. The primary inclusion criterion was the use of only qualitative methodologies, including interviews, focus groups, qualitative phases of mixed-methods research or online surveys with open-ended questions. Furthermore, studies were eligible for inclusion if they had been published in English after 2004, as there have been significant advancements in the understanding and treatment of endometriosis over the past two decades.
Screening
The identified articles (n = 578) were reviewed through examination of their title, abstract and full-text review based on the inclusion/exclusion criteria (Figure 1). Hand searches of the selected journals were also undertaken to identify further articles. No new articles were found to meet the inclusion criteria after reviewing the titles and abstracts. After removing duplicates, the methodological quality of the studies was independently assessed using the Critical Appraisal Skills Programme checklist for qualitative research (CASP) and one question from the Joanna Briggs Institute Critical Appraisal tool (JBI-QAR).15,16 Overall, 20 articles met the inclusion criteria and were included in this review (Figure 1).
Results
Characteristics of the included studies
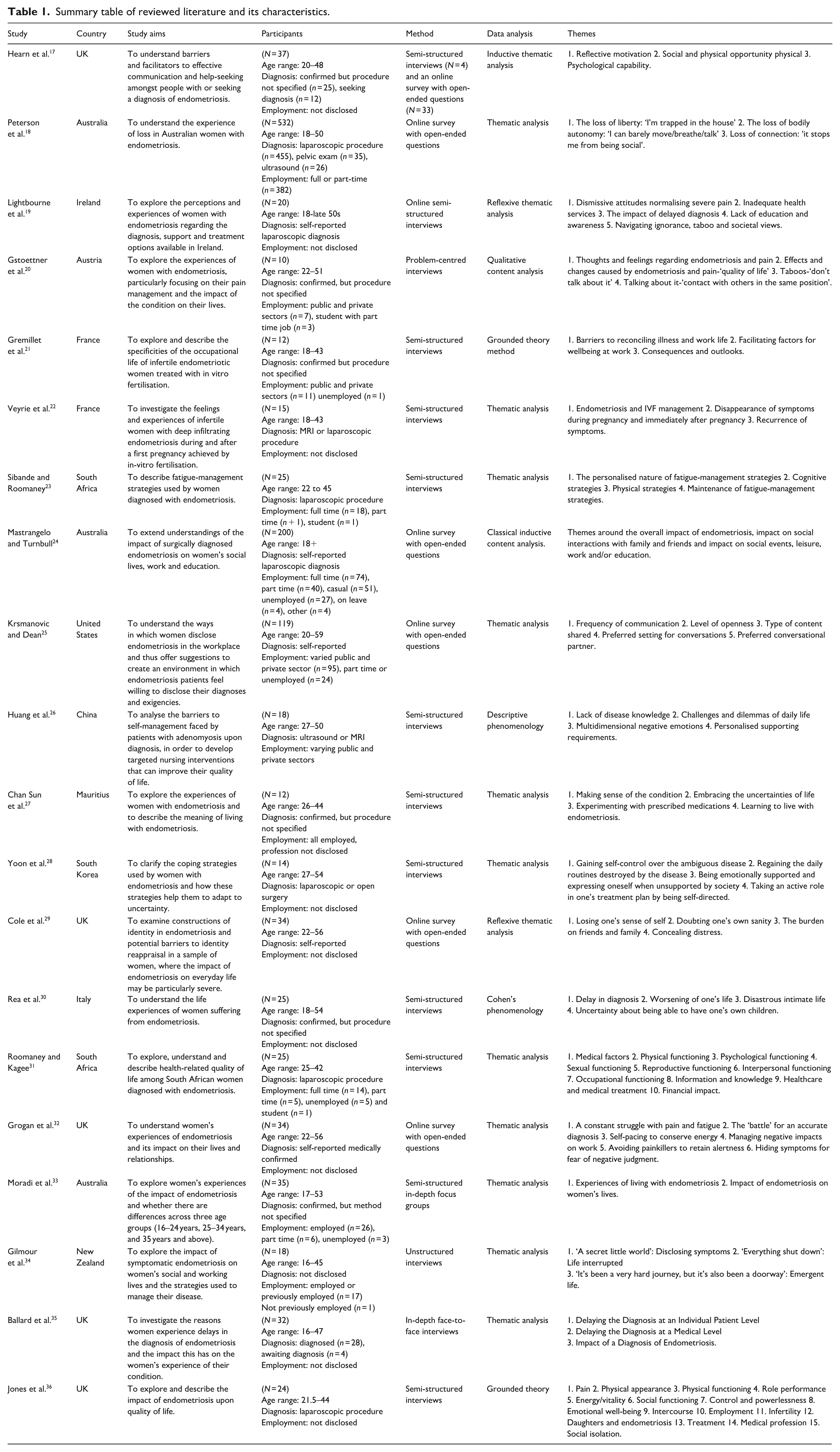
The key characteristics of the included studies are outlined in Table 1. The sample size of the included qualitative studies ranged from 10 to 532 participants, encompassing a total of 1241 women diagnosed with endometriosis across 20 studies. The participants’ ages ranged from 16 to 59 years old. Employment status varied, with several studies not disclosing this information. The majority of studies utilised semi-structured interviews or online surveys with open-ended questions, ensuring a comprehensive understanding of the participants’ experiences. The primary focus of these studies included barriers to effective communication and help-seeking, the experience of loss, perceptions of diagnosis and treatment, pain management and the impact on occupational life and social relationships. Data analysis methods included thematic analysis, reflexive thematic analysis, qualitative content analysis, grounded theory, descriptive phenomenology and classical inductive content analysis. Key themes identified across the studies encompassed psychological, social and physical impacts, coping strategies and the role of societal and healthcare system responses.
Summary table of reviewed literature and its characteristics.
Assessment of quality
Risk of bias and methodological quality were systematically assessed for all included studies. The Critical Appraisal Skills Programme (CASP) tool was used to evaluate credibility, transferability, dependability and confirmability, while the JBI-QARI checklist was used to assess congruence between philosophical underpinnings and methodology.15,16 These tools collectively addressed key domains of bias, including researcher influence, participant selection and analytical transparency. The overall risk of bias across studies was moderate, primarily due to incomplete reflexivity reporting. A summary of the critical appraisal is presented in Table 2, and full CASP and JBI-QARI checklists are available in Supplemental Material Files 2 and 3 respectively.
Critical appraisal of included studies using the CASP tool (Q1–Q10) and JBI-QARI tool (Q11).
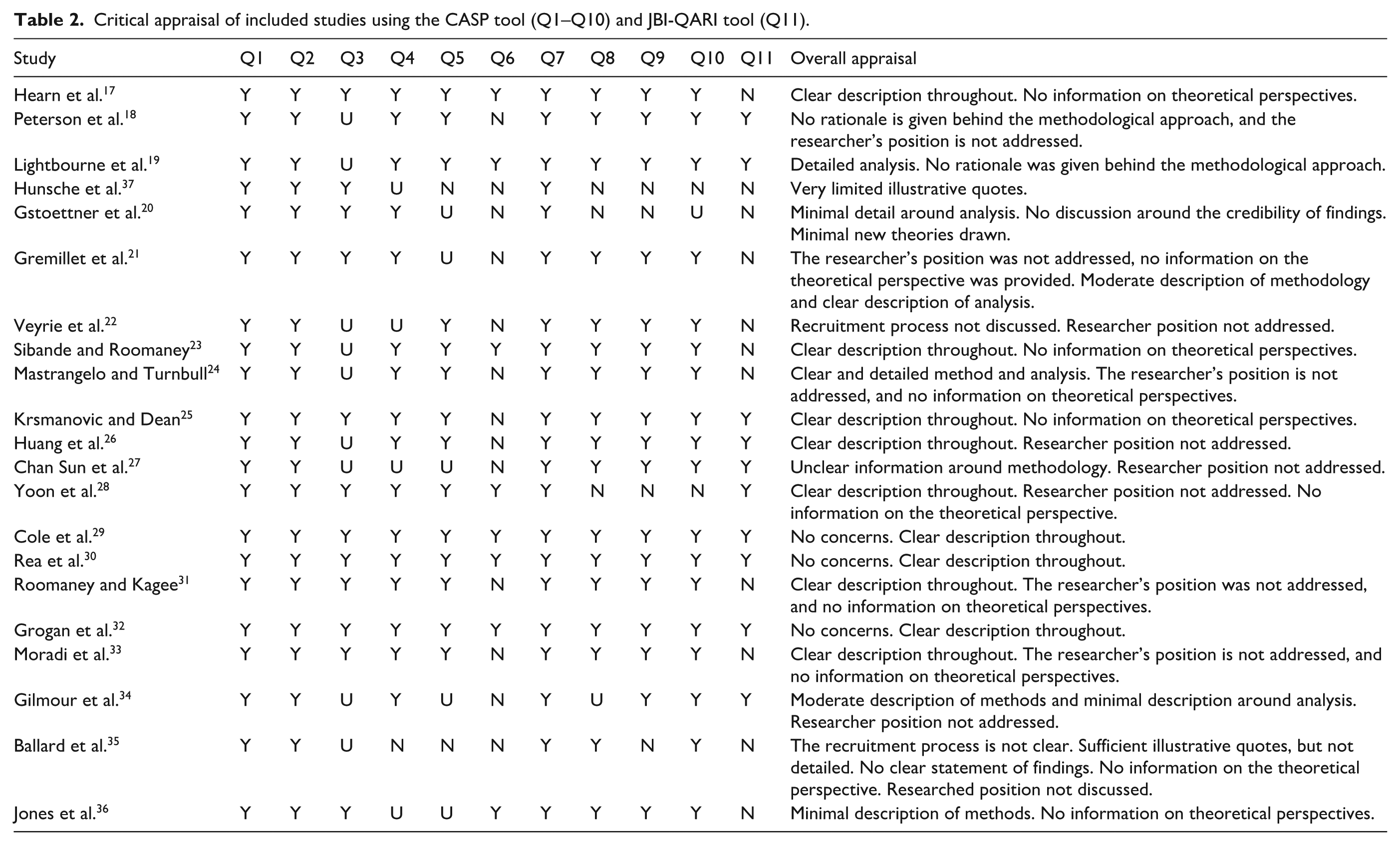
Overall, most studies included in the review were assessed to be of moderate to high quality. Those of poorer quality were still included to preserve valuable participant insights. This is with the exception of one study, which did not provide a sufficient number of quotations, making it challenging to trust that the author’s interpretations accurately reflected the participants’ accounts. 37
For the remaining studies, few critically examined the researcher’s own biases or potential influences during the research process, nor did they discuss their philosophical standpoints, thus reducing the trustworthiness of their findings. Whilst most studies clearly described their data analysis process and used investigator triangulation to promote credibility, few reported using respondent validation to ensure that their findings accurately reflected participants’ perspectives and experiences. Furthermore, not all studies justified their choice of data collection methods, making it difficult to assess the appropriateness of their chosen methods.
Data synthesis
Thomas and Harden’s thematic synthesis method was employed to analyse the results of the included studies. 38 Each study was meticulously reviewed by the primary author, with a secondary review conducted by the co-author to ensure reliability. Information that represented diverse viewpoints and patterns pertinent to the research objectives was extracted and placed in a table, without the use of computer software. 39
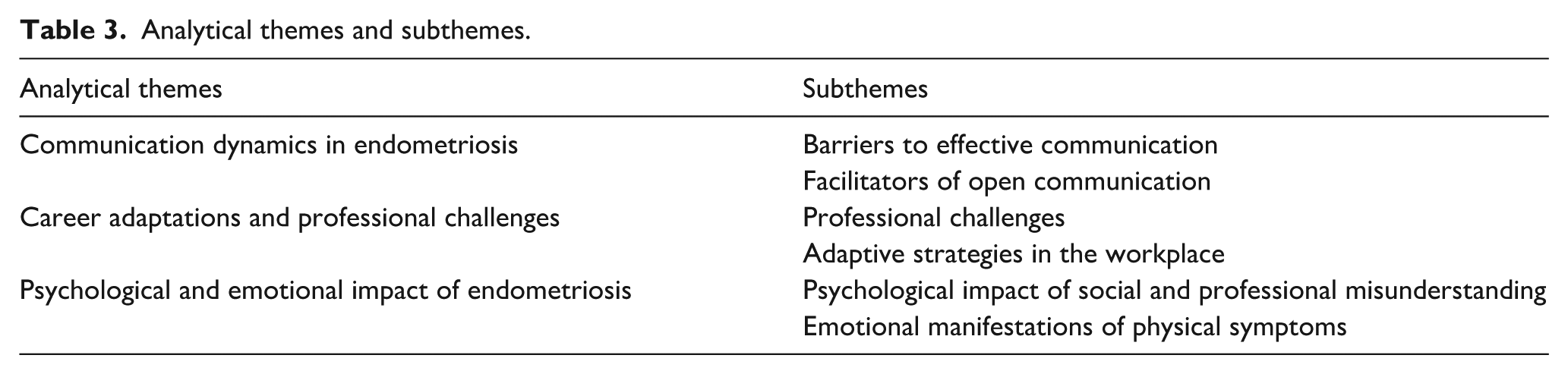
Immersion in the findings allowed for the development of initial codes that captured the core messages of the extracted quotes. Hierarchical tree structures were created to highlight similarities between codes which were then used to form descriptive themes. To synthesise the findings and form analytical themes, conceptual maps were created. These maps enabled the authors to transcend the original contents of the studies and develop more abstract thematic categories. This iterative process of coding and mapping ensured a robust synthesis that accurately reflected the complexity of the data. The final themes and subthemes are presented in Table 3.
Analytical themes and subthemes.
Thematic synthesis
Communication dynamics in endometriosis
Barriers to effective communication
The stigma surrounding menstruation and endometriosis created significant barriers to open communication and hindered help-seeking behaviours. Women felt ‘embarrassed’ about disclosing their symptoms in the workplace, often resorting to fabricating the origin of their discomfort, such as claiming a migraine, or using vague depersonalised language such as ‘chronic illness’, and providing no further details around their condition. This sense of embarrassment was intensified when interacting with male colleagues or managers, whom women perceived as unlikely to understand or respond sympathetically. For instance, one participant shared that:
It was very difficult to talk about, especially since I only work with men. They don’t really understand and are completely disconnected from that reality.
21
When women did disclose their symptoms to male colleagues and managers, they were often met with dismissal and discomfort, pushing them to conceal their symptoms. One participant suggested that:
It’s hard to explain absence from work or a need to take breaks when these things are due to heavy bleeding and extreme pain. My managers have all been male, and all told me I was exaggerating.
17
Although less common, female colleagues were also described as dismissive in instances of disclosure. Specifically, female colleagues exhibited a survivorship bias, questioning the severity of endometriosis symptoms due to their own less severe experiences around menstruation. Hierarchical disparities are presented as a significant barrier to communication for many women, often disclosing their condition to seniors only out of necessity. This concealment stemmed from both fear of being perceived as malingering and fear of professional repercussions, as one woman described that disclosing her symptoms would be:
basically giving them ammunition to use against me in the future. It’s better to silently brave through it and let my strong work ethic cover my deficiencies.
25
Facilitators to open communication
Several factors facilitated open communication around endometriosis in the workplace. The presence of compassionate and understanding colleagues and managers who listened attentively and responded proactively significantly eased the disclosure process. For instance, one participant described how her manager acted as an advocate and intermediary, explaining her absences to fellow colleagues, ensuring they were informed and accommodating upon her return. Personal advocacy was also demonstrated to enhance communication, as some women took it upon themselves to educate their colleagues about endometriosis so that they would understand their experiences. For women who were not comfortable doing this, having managers with a prior awareness and understanding of endometriosis was extremely beneficial. One participant noted:
When I asked for time off for my first surgery, I said I have a disease called endometriosis. My supervisor said her sister has it, so she already understood everything.
25
For women who felt delegitimised by coworkers in the face of an invisible disease, having more concrete proof in the form of a medical diagnosis, upcoming surgery or IVF treatment confirmed the genuineness of their symptoms and facilitated workplace communication. One participant shared:
I have been in the IVF program for three years now, and it is easier for me to justify my absences. [. . .] I feel more legitimate in the context of my pregnancy project than in the context of simple stomach aches. I feel like my boss and colleagues understand my situation better.
21
Additionally, women who were aware of their workplace rights and organisational policies were able to utilise these in discussions with employers to communicate their needs and requests with confidence. One woman was able to refer directly to French law to justify her absences in support of her reproductive treatments.
Career adaptations and professional challenges
Professional challenges
Women with endometriosis faced discriminatory behaviour on a regular basis as managers frequently misunderstood and dismissed their concerns. One participant recounted:
[. . .] and he [boss] just asked if I couldn’t do it [laparoscopy] later, and I said No, because there’s really something going on for me, and I’m also in insane pain and I can’t stand it any longer. And then he actually fired me while I was on sick leave.
20
Regular absences or sick leave for surgery often provoked threatening remarks from employers. Some women were compelled to work through severe pain or return from recovery ‘a week early’ to keep their jobs. For others, this lack of compassion created an unworkable environment, forcing them to leave their positions.
The physically debilitating symptoms of endometriosis dictated the career paths for many women, preventing them from advancing in their chosen fields or forcing them to change sectors entirely. One woman with aspirations to become a police officer found herself unable to cope with the physical demands of the role and was forced to make a ‘professional change with regrets’.
21
Work performance and productivity was significantly impacted by both endometriosis-related symptoms and treatment side effects. One woman described struggling to concentrate at work after taking pain medication, which, as a nurse, impacted her ability to ‘focus on patients’ needs’.
32
Symptoms, side effects, medical appointments and surgeries all contributed towards absenteeism, and as a result, women found that their employability was impacted. One participant shared:
left my part-time job because I was not able to work due to severe symptoms and undergoing two surgeries. . . Having two surgeries within a year, it’s kind of hard to find a job if you think that that’s going to be ongoing, not many people are going to employ you to have time off.
33
Financial insecurity and loss of financial independence were common among women, as they often exhausted their sick leave and annual leave, resulting in unpaid leave. In countries with privatised healthcare, some women disclosed their financial vulnerability and reported being unable to afford medical appointments for their endometriosis.
Adaptive strategies in the workplace
To navigate workplace challenges arising from endometriosis symptoms, women employed various proactive coping strategies. For example, anticipating flare-ups and planning time off in advance were common practices. Women also reported overcompensating in times that they were feeling well and stressed the importance of pacing themselves, with evenings and weekends being spent resting to restore depleted energy levels. However, this poor work-life balance often negatively impacted their social lives, leading to frequent cancellations of events and feelings of isolation. One participant noted:
by the end of the week I am in bits and have to rest the whole weekend to even feel partly prepared for the next week.
32
Flexibility emerged as a critical workplace accommodation. Workplaces that fostered a culture of flexibility, allowing for adjustments in schedules and accommodations for periods of leave, were regarded as ‘safe’ and ‘positive’.
25
One lady described how, by playing on the flexible parameters of her workplace, she was able to keep working through her endometriosis and had ‘hardly ever’ taken time off.
21
In contrast, for those in less supportive employment adopted an attitude of ‘just getting on with things’ and demonstrated acquired resilience. One woman shared that:
I rarely take time off work as I refuse to let the endometriosis take over, so I put on my TENS machine or take pain killers or just cope with it.
32
Psychological and Emotional Impact of Endometriosis
Emotional manifestations of physical symptoms
Women described the profound emotional impacts of living with endometriosis and how the persistent pain and unpredictable symptoms caused significant stress and anxiety. This anxiety was exacerbated by concerns about symptom flare-ups at work and the inaccessibility of essential resources, such as bathrooms and medications, necessary for managing their condition.
Their pain was described as both physically and mentally exhausting and subsequently led to emotional outbursts in women’s professional and personal lives. One woman reported having a fight in the workplace, stating:
Just because, yeah, it’s stressful and you’re angry, and I guess that’s the point where it can affect your relationships with people more seriously.
33
Emotional instability was further exacerbated by the side effects of hormone therapy treatments. Women also experienced feelings of guilt and burden due to their inability to meet demands in both their personal and work lives, resulting in diminished self-worth. One woman described experiencing profound despair and hopelessness, as well as a loss of professional drive and ambition, directly attributed to her monthly symptoms:
Every month (during menstruation) I feel like I’ve lost my mind. I don’t want anything, not money, not a high position. . . The pain is so intense that I wish I didn’t have to live like this, and sometimes I feel like banging my head against the wall.
26
Psychological impact of social and professional misunderstandings
Women experienced significant psychological distress due to the widespread misunderstanding of endometriosis by others. This lack of understanding and frequent dismissal led to feelings of invalidation, shame and self-doubt, as women often questioned the legitimacy of their condition and their sanity. One woman stated, ‘I sometimes think I am being a hypochondriac and get very worried and anxious’. 32
Consequently, many women found it challenging to discuss their symptoms, which severely impacted their quality of life, leading to feelings of isolation and loneliness. One participant described endometriosis as ‘a secret little world’ to live in. 34
The misconception of endometriosis as merely ‘bad period pains’ by colleagues and managers led women who experienced more regular or non-cyclical pain to fear judgment or mislabelling as dramatic, lazy or unreliable. This fear was exacerbated in male-dominated industries, where stigma was more pronounced and empathy notably lower.
Discussion
This systematic review extends the existing knowledge and provides an in-depth examination of the professional experiences of women with endometriosis.
This review found that the difficulties faced by women with endometriosis are not solely attributable to the condition itself but frequently arise from the reactions and responses of others. Women are experiencing dismissal, discomfort and discrimination upon disclosing their condition to colleagues and managers. These reactions were notably more prevalent in male-dominated industries and occurred for a multitude of reasons, most commonly a lack of understanding, stigmatisation and disinterest. In the absence of emotional support, women were often left with feelings of invalidation, shame, self-doubt and isolation. The impact of an unsupportive work environment has been documented extensively in previous research. For instance, Rasool et al. 40 highlighted that toxic workplace environments significantly mediate the relationship between organisational support and employee well-being, leading to decreased employee engagement and productivity, as well as increased stress and burnout.
These findings are consistent with the broader literature on workplace discrimination and chronic illness. For example, a recent study found that employees with chronic illnesses often face substantial workplace barriers, including a lack of accommodations and understanding from colleagues and supervisors. 41 This lack of support not only affects their work performance but also their overall mental health and quality of life. The evidence underscores the need for organisations to foster a more supportive and inclusive work environment, particularly in male-dominated industries where empathy and understanding towards conditions like endometriosis are critically lacking.
Previous research has also revealed that this lack of emotional support extends far beyond the workplace, as women discuss being dismissed by family members, friends and healthcare professionals (HCPs).42–44 This was made apparent in a recent metasynthesis exploring how women with endometriosis experience healthcare encounters. 45 This review revealed patients with endometriosis to be treated with ignorance in non-specialised healthcare centres, and felt HCPs did not take their concerns seriously. Thus, with an average diagnostic journey of 7–12 years in which women are likely to experience repeated dismissal, it is highly plausible that this long-term delegitimisation is contributing towards the wider psychosocial issues evident in the workplace. 4
Studies have shown that negative encounters with HCPs can be improved by equipping physicians with the necessary knowledge to recognise endometriosis and by treating patients with empathy, valuing them as partners in their health. 46 It was emphasised that training healthcare providers to recognise and empathise with endometriosis symptoms can significantly improve patient satisfaction and health outcomes. 46 Wygant et al. 47 highlighted that empathetic treatment and proper communication are crucial for patient satisfaction among those suffering from chronic pelvic pain. These recommendations are equally applicable to the workplace as our review demonstrates that empathetic responses upon disclosure are regarded as highly positive experiences by women with endometriosis. However, this review also revealed that familiarity with the condition often leads to greater empathy, suggesting that those with prior knowledge of endometriosis are more likely to respond supportively. Therefore, increasing awareness in workplace settings is crucial to foster more empathetic responses and create safer environments where women feel comfortable disclosing their condition. To effectively disseminate information, initiatives should particularly target individuals in leadership roles, as they bear the greatest responsibility for sharing this information and preventing discriminatory behaviour. Although the optimal method for disseminating information is not specified in this review, it is recommended that training programmes, awareness campaigns and policy changes be implemented to educate managers and colleagues about endometriosis.
Thus far, this review has focused on enacted stigma; the unfair, unjustifiable and discriminatory treatment by others in response to a socially unacceptable difference. 48 Scambler discusses how enacted stigma manifests in health-related scenarios, where individuals are marginalised due to their conditions. 48 However, self-stigmatisation was also highly prevalent and arguably more disruptive. Women would demonstrate self-silencing behaviour motivated by fear of judgement and internalised shame around their endometriosis, the implications of which are two-fold.
Firstly, this has significant psychological consequences, including increased levels of depression and social isolation. 49 Stoppard highlights that self-silencing and internalised stigma are closely linked to higher rates of depression among women, reinforcing the findings of this review. 49 Women with endometriosis often internalise societal stigma, which exacerbates feelings of shame and inadequacy. This internalised stigma not only affects their mental health but also hampers their ability to seek support and advocate for their needs in the workplace. The fear of judgment and misunderstanding leads many women to conceal their condition, resulting in isolation and a lack of necessary accommodations. Secondly, endometriosis is a highly individualised condition; without effective communication with employers, personalised management plans cannot be implemented. The lack of open communication due to fear of stigmatisation means that many women do not receive the workplace accommodations they need. This can lead to decreased productivity, increased absenteeism and overall lower job satisfaction, whereas effective communication and tailored management plans are crucial for managing chronic conditions in the workplace. 50 To mitigate against the harmful effects of stigma and promote open communication, previous reviews have recommended the implementation of public health awareness campaigns, highlighting the effectiveness of these on other stigmatised conditions such as HIV and mental illness.51,52 Reinhardt and Eitze 51 emphasise the importance of addressing menstrual stigma through social norm approaches, which can be highly effective in reducing stigma and promoting acceptance. This review is in full support of wider campaigning and emphasises the importance of targeting male audiences while including both educational material and social norm messages to promote acceptance of endometriosis. Such campaigns can educate the public, including employers and colleagues, about endometriosis, thereby fostering a more supportive environment for women with the condition. As understanding and acceptance of endometriosis increase, women may feel more comfortable disclosing their condition and advocating for their needs. This can lead to better workplace accommodations, improved mental health and overall better quality of life for women with endometriosis.
Our metasynthesis identified minimal evidence to suggest that workplaces are implementing strategies to support employees with endometriosis. These findings are reinforced by a recent scoping review, which summarised global evidence on interventions designed to support women in managing menstruation, menstrual disorders and menopause in the workplace. 53 This review found only two articles aimed at supporting those with endometriosis, neither of which focused on the design and implementation of evidence-based interventions.54,55 Despite the increasing awareness of endometriosis and its implications, practical strategies and interventions remain underdeveloped. This gap is critical as endometriosis not only affects physical health but also has profound psychosocial consequences, which can be exacerbated by unsupportive work environments.
To promote well-being and support women with endometriosis to stay in employment, future research must prioritise exploring the efficacy of such interventions. For instance, flexible working hours, remote work options and more frequent breaks could all be beneficial adaptations. Additionally, developing comprehensive workplace policies that include education for all employees about endometriosis could foster a more supportive environment. Previous qualitative studies conducted during the COVID-19 pandemic explained how these measures allowed women with endometriosis to more effectively manage their symptoms, decrease flares and increase productivity.56,57 However, the current evidence base demonstrates wide variability in the impacts of work-from-home (WFH) opportunities for the general population. 58 Therefore, future research should use quantitative measures to determine the effects of WFH opportunities specifically on work productivity in women with endometriosis.
This review found that women who were aware of their workplace rights were able to confidently communicate their needs to employers. However, whilst it is an employer’s responsibility to ensure the well-being of their employees and inform them of their rights, the review demonstrated that employers are often neither accommodating nor responsive and thus may fail to provide this essential information. 59 This finding aligns with existing literature that highlights the gap in employer knowledge and responsiveness regarding chronic conditions like endometriosis. Research indicates that many employers lack adequate understanding and resources to support employees with chronic health conditions, leading to insufficient accommodations and support. 60 Advice around this matter may be sought from human resources or occupational health departments, evidence has shown these departments often have limited knowledge of the condition. 21 Therefore, it is critical for additional support to be provided by other professionals involved in their care. For instance, gynaecologists, physiotherapists working in women’s health, and general practitioners should all aid in disseminating this knowledge to women with endometriosis, helping to facilitate their well-being in the workplace.
Despite the need for better support, workplace rights and policies may not always accommodate the needs of individuals with endometriosis. Standard sick leave policies often fall short, and in some cases, may inadvertently discriminate against those with the condition. For example, the Bradford Formula is a tool utilised by employers to quantify the impact of employee absences. 61 This metric penalises frequent and unplanned absences, which are a common characteristic of endometriosis. Additionally, in the UK, endometriosis is not classified as a disability under the Equality Act. 62 Consequently, women with endometriosis are not automatically entitled to the same legal protections as those with other substantial and long-term conditions. While women can independently advocate for their condition to be recognised as a disability to obtain workplace reasonable adjustment plans, current laws do not explicitly mandate employers to disregard disability-related absences. Thus, women continue to exhaust their sick and annual leave and face absence-related repercussions. By redefining workplace policies to include flexible working arrangements, comprehensive sick leave policies and targeted training for managers and HR professionals, organisations can better support employees with endometriosis.
Limitations
While this review provides valuable insights into the experiences of women with endometriosis in the workplace, several limitations must be acknowledged. First, the reliance on qualitative studies means that the findings are based on subjective experiences and may not be generalisable to all women with endometriosis. Additionally, the included studies varied in their methodologies, sample sizes and geographic locations, which could influence the consistency and applicability of the findings.
Secondly, whilst this review included a significant number of studies, only two were specifically targeted at examining the influence of endometriosis on the professional lives of participants. The majority of studies adopted a generalised approach, emphasising the overall experiences of endometriosis, with work-related experiences representing only a minor aspect of the findings. Thus, to ensure a fully comprehensive overview of this area, further primary studies into this topic would be beneficial. Additionally, future research should examine the impact of endometriosis on more physically demanding job roles, such as those in the armed forces, where endometriosis-related job loss is reportedly more frequent. 54
Third, the heterogeneity in the diagnostic criteria and definitions of endometriosis used across studies could impact the comparability of the findings. Some studies relied on self-reported diagnoses, while others required medical confirmation, leading to potential differences in the severity and management of the condition among participants.
Despite these limitations, this review underscores the urgent need for workplace policies and interventions that address the unique challenges faced by women with endometriosis, ultimately fostering more supportive and equitable professional environments.
Clinical Relevance and Implications for Practice
The findings of this review have important implications for clinical and occupational health practice. Clinicians, including gynaecologists, physiotherapists, occupational health professionals and general practitioners, are in key positions to support women with endometriosis in maintaining employment. By proactively discussing workplace adaptations and providing medical evidence to support flexible arrangements, clinicians can help mitigate absenteeism and improve overall quality of life. Moreover, interdisciplinary collaboration between healthcare providers and employers can facilitate early identification of work-related challenges, allowing for tailored interventions such as graded return-to-work plans, ergonomic assessments and pain management support. Embedding these practices within clinical pathways may promote holistic care that addresses both the physical and psychosocial dimensions of endometriosis.
Conclusion
This review highlights the multifaceted challenges faced by women with endometriosis in their professional lives, including inadequate workplace interventions and active dismissal by coworkers and employers. These issues are compounded by similar experiences in personal and healthcare interactions, driven largely by a lack of awareness and understanding.
The review emphasises the urgent need for comprehensive support mechanisms, including flexible working arrangements, targeted training for employers and public health campaigns to reduce stigma. Legal reforms to recognise endometriosis under disability laws are also recommended to ensure necessary protections and accommodations.
Future research should focus on developing and evaluating evidence-based interventions to support women with endometriosis in the workplace. By increasing awareness, implementing policy changes and providing dedicated support systems, we can create more inclusive and supportive professional environments.
Supplemental Material
sj-docx-1-pev-10.1177_22840265261427636 – Supplemental material for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis
Supplemental material, sj-docx-1-pev-10.1177_22840265261427636 for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis by Alice Hodgins and Glykeria Skamagki in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-docx-2-pev-10.1177_22840265261427636 – Supplemental material for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis
Supplemental material, sj-docx-2-pev-10.1177_22840265261427636 for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis by Alice Hodgins and Glykeria Skamagki in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-docx-3-pev-10.1177_22840265261427636 – Supplemental material for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis
Supplemental material, sj-docx-3-pev-10.1177_22840265261427636 for The experiences of women with endometriosis in the workplace: A qualitative metasynthesis by Alice Hodgins and Glykeria Skamagki in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Author contributions
AH: Substantial contributions to the conception, acquisition, analysis and interpretation of the work. Substantial contributions to reviewing and final approval for publication. Is accountable for ensuring all questions related to the accuracy and integrity of the work are resolved. GS: Substantial contributions to analysis and interpretation of the work. Substantial contributions to reviewing and final approval for publication. Is accountable for ensuring all questions related to the accuracy and integrity of the work are resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval was not sought for this systematic review as it exclusively utilises secondary data from previously published studies, which have already received ethical approval by their respective ethics committees. No new data was collected or analysed.
Consent for publication
Both authors have consented for publication. No other consent applicable.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.