
Abstract
Objective:
To systematically evaluate the epidemiology, diagnostic modalities, and treatment strategies for urinary tract endometriosis (UE), with the goal of informing evidence-based clinical practice.
Materials and methods:
A comprehensive search of PubMed, Ovid, Embase, MEDLINE, and the Cochrane Library was conducted from January 1976 to March 2023. The protocol was registered with INPLASY (INPLASY202420054). Original studies reporting clinical, diagnostic, or therapeutic aspects of urinary tract endometriosis (UE) involving the bladder, ureter, kidney, or urethra were included, while reviews, editorials, and duplicate publications were excluded. Three reviewers independently screened articles, extracted relevant data, and categorized findings by site of involvement and diagnostic or treatment modality. A narrative synthesis of the results was performed.
Results:
A total of 137 studies were included. Bladder endometriosis was the most common subtype (80%–85%), followed by ureteral involvement (9%–23%). MRI and transvaginal ultrasound showed the highest sensitivity and specificity for diagnosis. Minimally invasive surgery, particularly robotic-assisted laparoscopy, was associated with favorable outcomes and lower recurrence rates.
Conclusion:
UE is a rare and underdiagnosed manifestation of deep infiltrating endometriosis. Early recognition with appropriate imaging and multidisciplinary surgical planning improves outcomes. Larger prospective studies are needed to inform standard guidelines.
Introduction
Endometriosis is a chronic gynecologic condition that affects approximately 10%–15% of women of reproductive age and up to 3%–5% of postmenopausal women,1–5 often leading to debilitating pelvic pain, dysmenorrhea, dyspareunia, and infertility. 6 Although endometriosis most commonly involves the pelvic peritoneum and ovaries, it can also infiltrate other organ systems. One of the most underdiagnosed and potentially harmful manifestations is urinary tract endometriosis (UE), which involves the bladder, ureters, kidneys, or urethra.7,8
UE accounts for an estimated 0.3%–12% of all endometriosis cases and up to 19%–53% of cases involving deep infiltrating endometriosis (DIE).9,10 The bladder is the most frequently affected site, followed by the ureter, while renal and urethral involvement is rare.11–25 UE can present with nonspecific urinary symptoms, mimic other urological conditions, or remain entirely asymptomatic,26–41 placing patients at risk for delayed diagnosis and irreversible complications such as hydronephrosis or renal failure.35,37,38,41–51
Despite its clinical relevance, UE remains poorly characterized in the literature. Most available studies are limited to small case series or focus on a single organ system, which limits generalizability. Additionally, there is a lack of consensus regarding optimal diagnostic approaches, treatment strategies, and follow-up care.52,53 To date, no comprehensive guideline exists to aid clinicians in the identification and management of UE.
Given the complexity and rarity of this condition, a thorough synthesis of existing literature is essential to support early diagnosis, individualized treatment, and multidisciplinary care. 54 The objective of this review is to systematically evaluate the epidemiology, diagnostic modalities, and treatment strategies for UE, with the goal of informing evidence-based clinical practice.
Materials and methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 55 The protocol was registered with INPLASY (Registration No. INPLASY202420054). The PRISMA flow diagram is presented in Figure 1, and a completed PRISMA checklist is available in the Supplemental Material. Institutional Review Board approval was not required since this was a review of previously published literature.
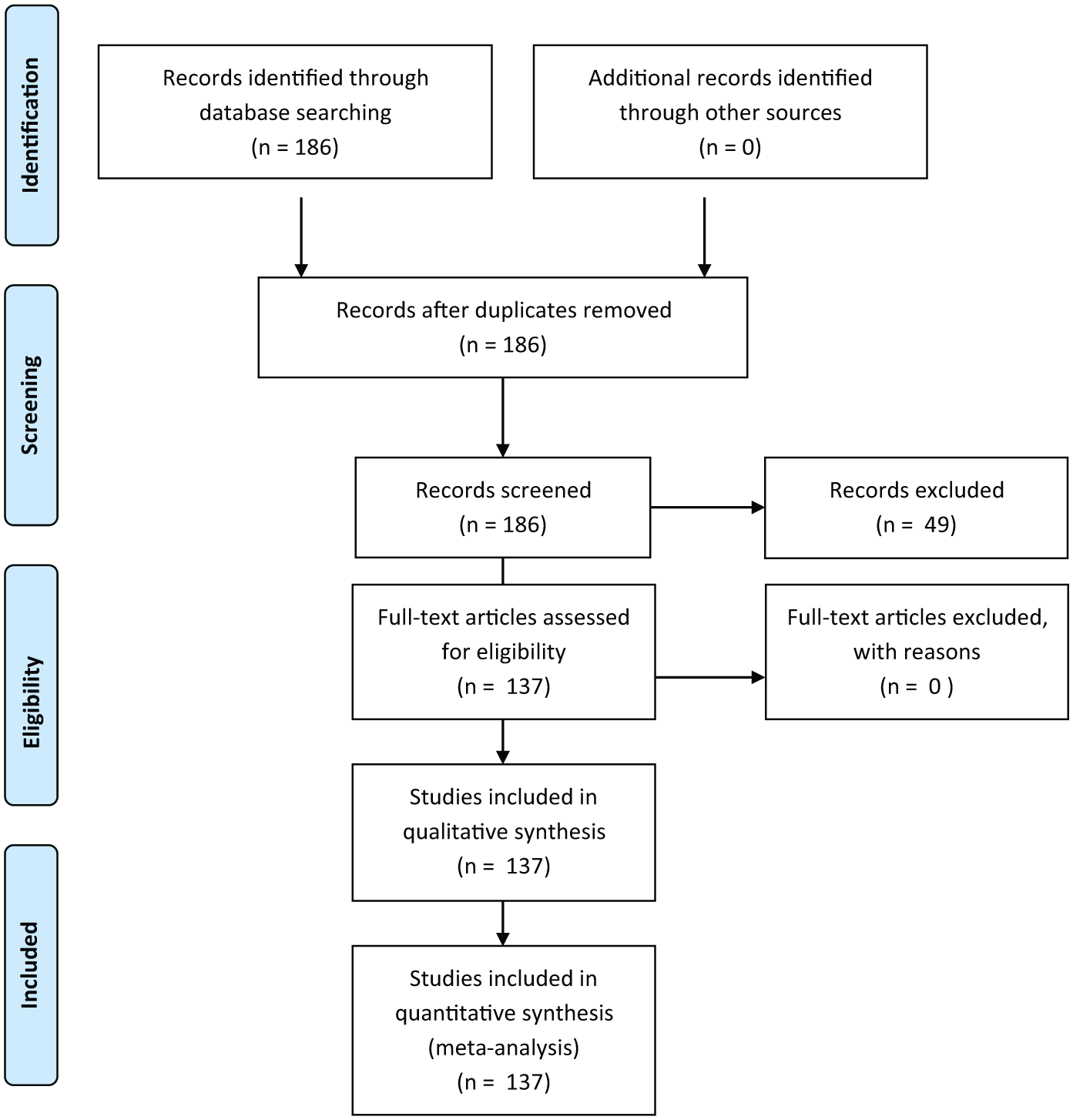
PRISMA flow diagram.
A comprehensive literature search was performed using PubMed, Ovid MEDLINE, Embase, and the Cochrane Library. The search period began in 1976, marking the publication of one of the earliest indexed reports specifically describing UE, and extended through March 2023. The search strategy included combinations of keywords related to urinary tract endometriosis, such as “bladder endometriosis,” “ureteral endometriosis,” “renal endometriosis,” and “deep infiltrating endometriosis involving the urinary tract.” Search terms were tailored to the indexing system of each database. Filters were applied to include only human studies published in English (Appendix 1).
Titles and abstracts were independently screened by three reviewers. Full-text articles of potentially relevant studies were reviewed in detail, and discrepancies were resolved through discussion and consensus. Each author contributed by independently screening studies from different decades. We did not attempt to identify unpublished studies or contact study authors.
Inclusion criteria were defined according to the PICO framework. The population of interest was women diagnosed with urinary tract endometriosis involving the bladder, ureter, kidney, or urethra. Interventions included any diagnostic or therapeutic approach, such as imaging studies, medical therapy, or surgical management. As this was a descriptive review, no formal comparison between interventions was required. Outcomes of interest included clinical presentation, diagnostic accuracy, treatment efficacy, recurrence rates, complications, and reproductive outcomes.
Studies were eligible for inclusion only if they were original research articles reporting primary clinical data on urinary tract endometriosis. These included case reports, case series, retrospective cohorts, and prospective observational studies. Review articles, meta-analyses, systematic reviews, editorials, and conference abstracts without full data were excluded from the data synthesis. However, select systematic reviews and meta-analyses were included in the reference list and cited in the Discussion section to provide contextual insight.
Initially, 186 studies published between January 1976 and May 2023 were identified. Of these, 49 were excluded because they did not specifically address urinary tract endometriosis or contained redundant findings. Therefore 137 studies were included in the final analysis. While we originally documented excluded articles and reasons during the screening process, the reference list of excluded studies was not preserved in a format suitable for inclusion.
Data extracted from the included studies included clinical manifestations, diagnostic modalities, laboratory and imaging findings, treatment strategies, and postoperative outcomes. Confidence intervals were not consistently reported and therefore could not be compared quantitatively. Study quality and potential sources of bias were qualitatively assessed based on study design, sample size, and completeness of reported data; however. a bias assessment tool was not applied due to heterogeneity in study design and reporting quality. These data were entered into a spreadsheet and reviewed collectively by the authors. Tables 1 to 4 summarize the findings. No heterogeneity analysis or sensitivity testing was performed. Cited references from the included articles were reviewed for background and discussion purposes. Based on the American College of Obstetricians and Gynecologists grading system, this review provides Level III evidence and a Grade B recommendation. 56
Common symptoms associated with UE.
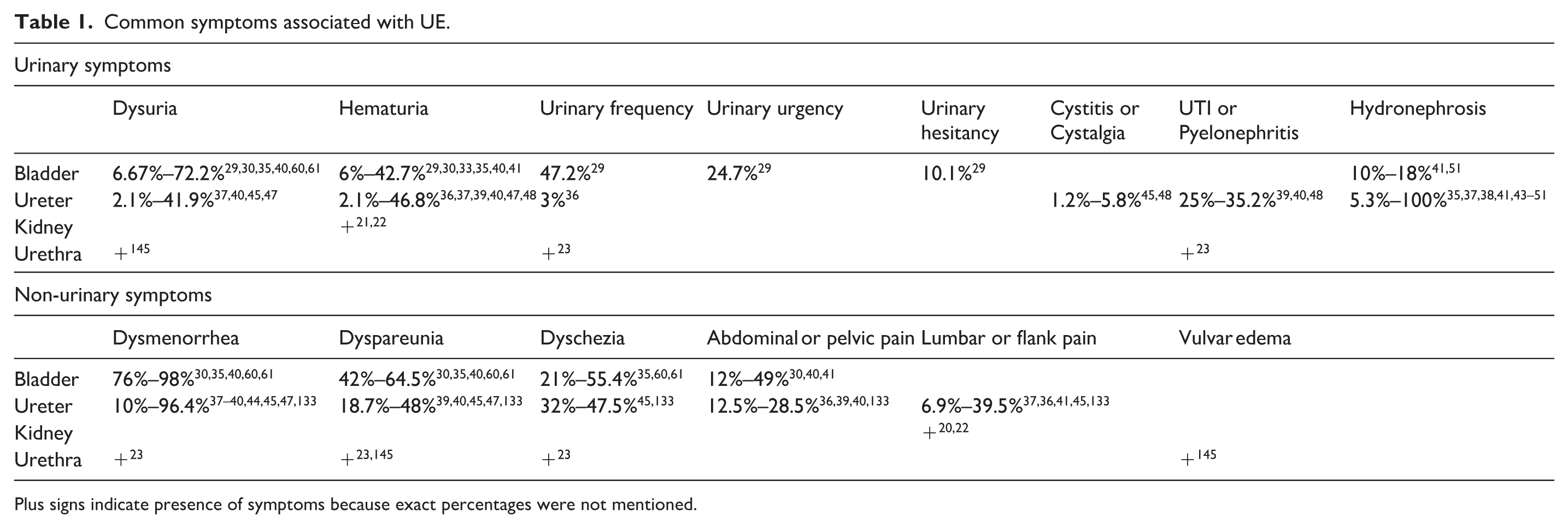
Plus signs indicate presence of symptoms because exact percentages were not mentioned.
Diagnostic modalities for urinary tract endometriosis.
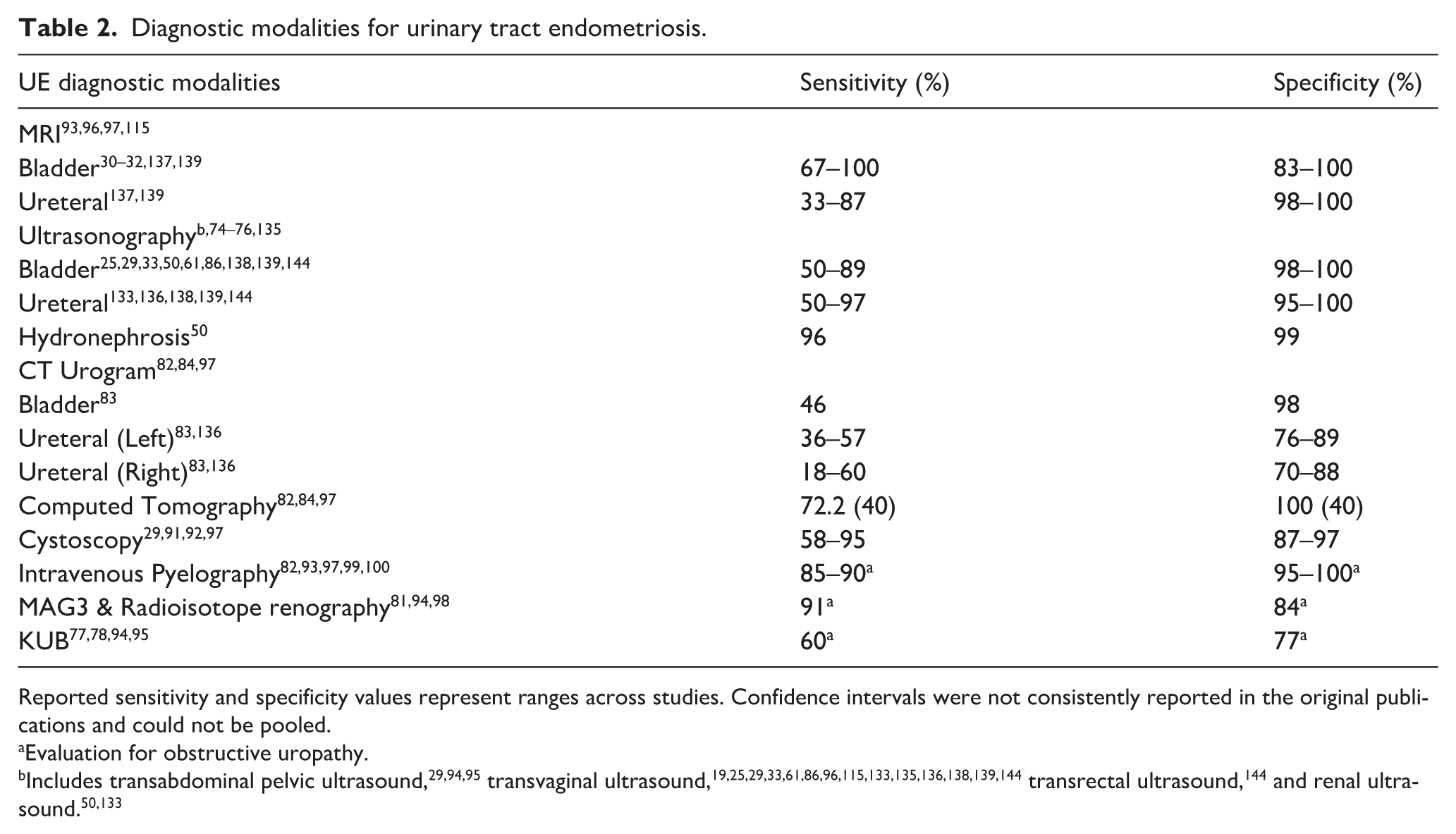
Reported sensitivity and specificity values represent ranges across studies. Confidence intervals were not consistently reported in the original publications and could not be pooled.
Evaluation for obstructive uropathy.
Characteristics of medical treatments for urinary tract endometriosis. 95
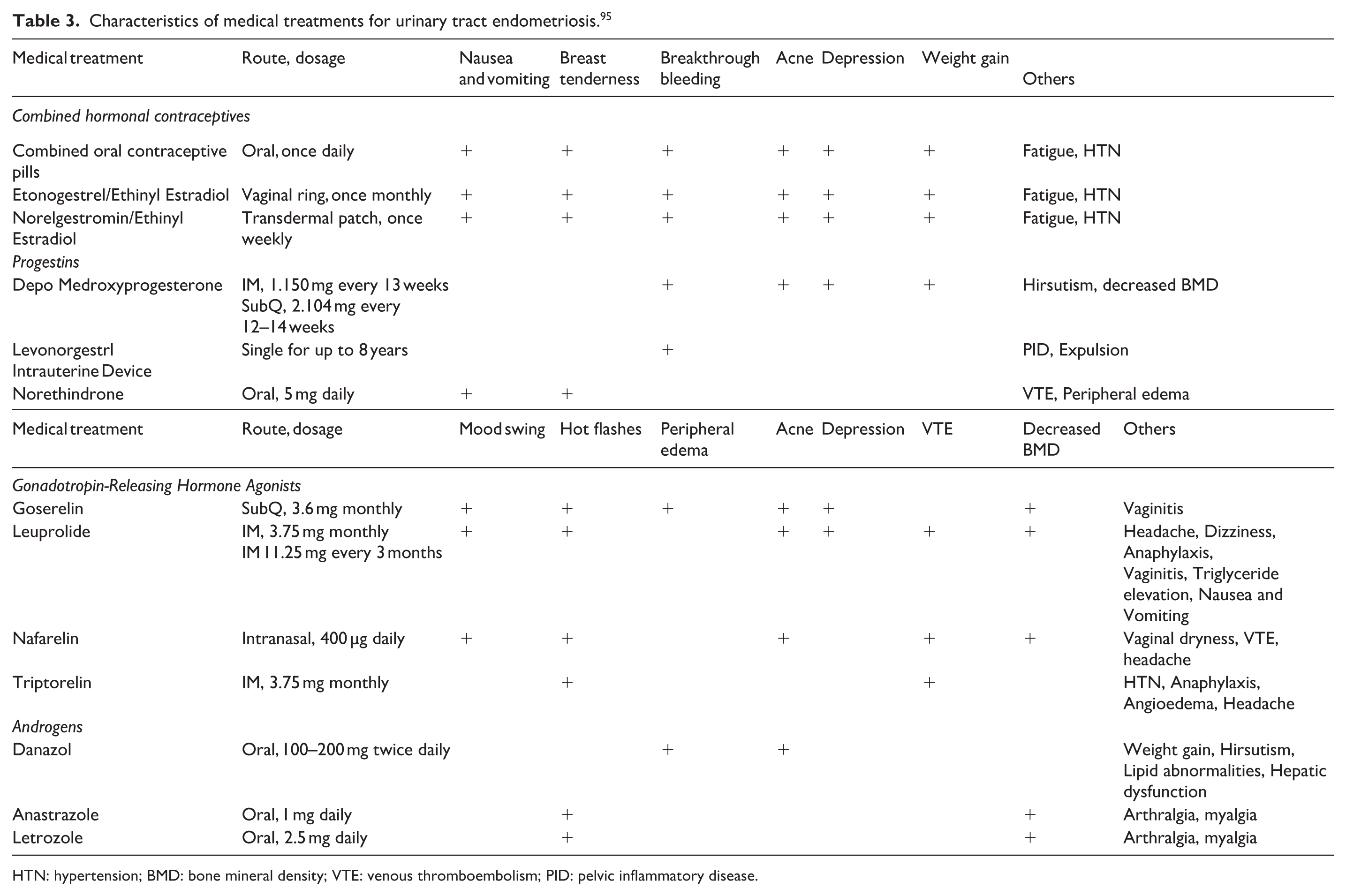
HTN: hypertension; BMD: bone mineral density; VTE: venous thromboembolism; PID: pelvic inflammatory disease.
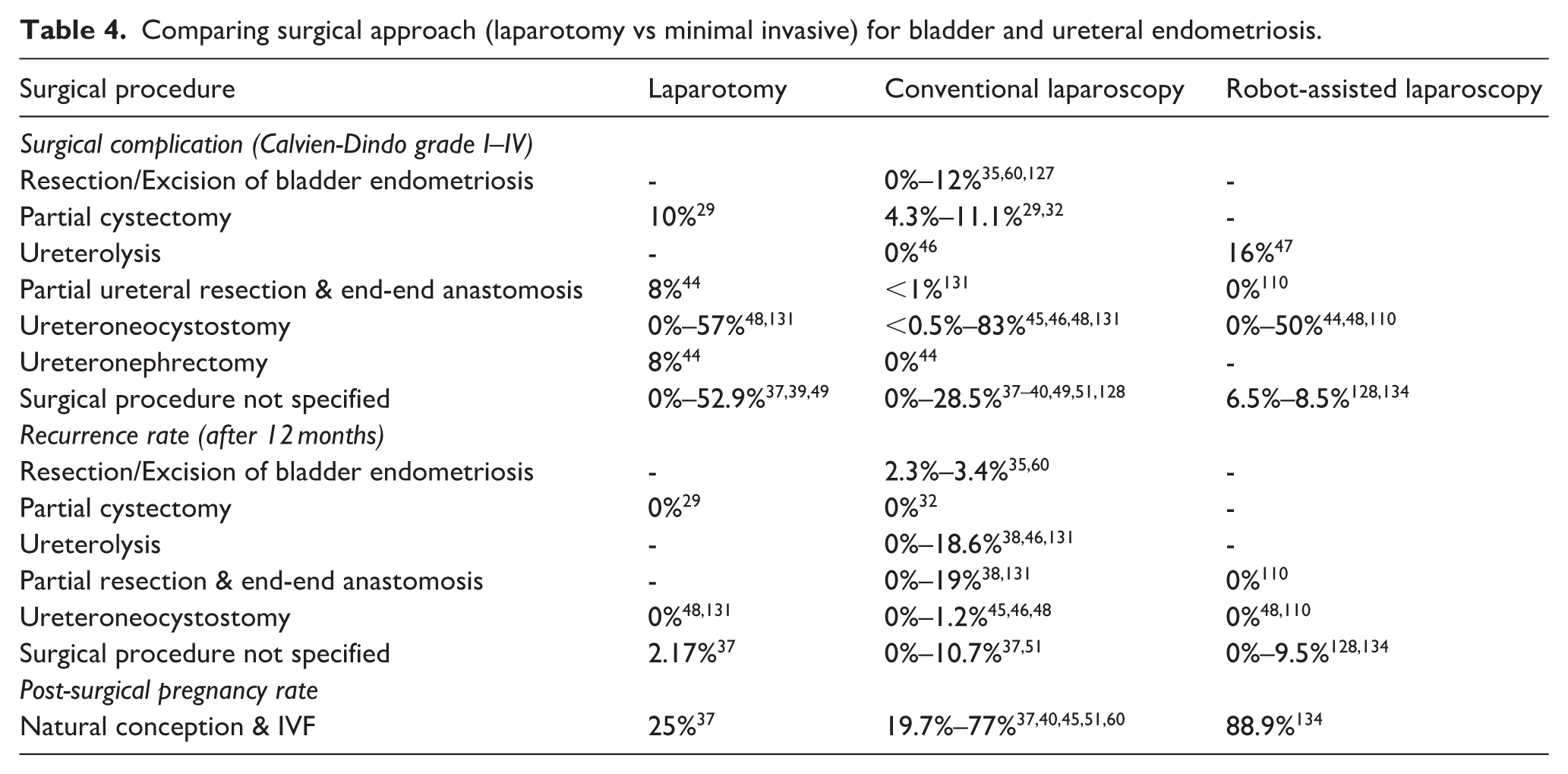
Comparing surgical approach (laparotomy vs minimal invasive) for bladder and ureteral endometriosis.
Results
Symptoms
UE has various clinical presentations depending on the size and location of the involvement. Most common symptoms include dysuria, hematuria, and urinary frequency. Other reported urinary symptoms are shown in Table 1.
Bladder endometriosis should be considered in patients with irritative urological symptoms such as dysuria, hematuria, frequency, urgency, hesitancy, urinary tract infection, bladder spasm, suprapubic discomfort, and pelvic mass, with aggravation of symptoms during menstruation.7,57,58 The most common symptoms in bladder endometriosis were dysuria, urinary frequency, and hematuria, with reported frequency up to 72%, 47%, and 43% respectively.29,30,32,35,40,41,59–61 Vercellini et al. reported perimenstrual urinary frequency, urgency, and dysuria in 95% of patients with bladder endometriosis. 62
Ureteral endometriosis can be clinically asymptomatic (50%) or present with pelvic pain, back pain, abdominal pain, 63 infertility, urinary frequency, dysuria, recurrent urinary tract infection, 64 hematuria, silent or progressive obstructive uropathy, and hypertension with advanced hydronephrosis. Hematuria and dysuria are the most common symptoms, with reported frequency up to 47% and 42%.36,37,39,40,45,47,48 Prevalence of UTI and pyelonephritis has been reported to be 25%–35%,39,40,48 and prevalence of hydronephrosis has been reported to be 5.3%–100%35,37,38,41,43–51 with up to 30% developing acute renal failure.2,7,65–67 Abdominal pain and flank pain were commonly seen in the studies reviewed in patients with ureteral endometriosis.
Diagnostic modalities
A number of imaging modalities may be utilized to confirm UE.68–70 However, UE diagnosis can be made based on the patient’s history, clinical signs, and symptoms, and it still needs to be proven by histopathology of the specimens collected during laparoscopy or another procedure. 71 Endoscopic visualization with biopsy is the best method to confirm the diagnosis. 72 It is also crucial to systematically evaluate the entire urinary tract before proceeding with any invasive diagnostic or therapeutic procedure.
Imaging
Table 2 summarizes the different imaging modalities used for diagnosis of UE. The imaging study of choice depends on clinical suspicion of location of UE involvement. MRI and ultrasound have been reported to have higher sensitivities and specificities compared to others. 73
Ultrasonography has sensitivity of 73%–83%29,30 and specificity of 86%–98%74–76 for diagnosis of UE. It is recognized as a non-invasive, practical, and cost-effective imaging method. It is superior to KUB X-ray with sensitivity and specificity of 60% and 77% respectively, in diagnosis of UE.77,78 Ultrasound, however, requires specifically trained personnel for detection and interpretation of endometriosis.79,80 MRI with and without contrast bypasses this challenge, and it is a non-invasive imaging modality that demonstrates sensitivity of 90% and specificity of 91%.11,81 CT-scan has a high specificity of 100% for UE,82,83 but sensitivity has been reported to be approximately 72.2%.84,85 It is essential to confirm renal patency before utilizing CT-Scan with contrast.
Cystoscopy is a diagnostic modality for bladder endometriosis,85–90 with sensitivity of 58%–95% and specificity reported to be 87%–97%.29,91,92 IVP, MAG3 & radioisotope renography, and KUB are used to evaluate obstructive uropathy. Their reported sensitivities are 85%–90%, 91%, and 60% respectively, and reported specificities are 95%–100%, 84%, and 77% respectively.77,78,81,82,93–100 IVP also requires confirmation of renal patency in advance.
Nevertheless, the sensitivity and specificity of retrograde pyelogram, intravenous urography, and ureteroscopy for ureteral endometriosis were not reported in the reviewed articles.97,101–106
Treatment
Medical management and surgical approaches for UE are demonstrated in Tables 3 and 4.
Medical management
Combined hormonal contraceptives, progestins, androgens, and gonadotropin-releasing hormone agonists in various dosages and routes have historically been used as medical management for endometriosis (Table 3). The advantage of medical treatment includes cost-effectiveness and ease of use; however, disadvantages include side effects (Table 3) and a limited degree of symptoms improvement, which necessitates patient’s awareness and counseling.1,107–109 Currently, there is no consensus on changes to medical management if the urinary tract is involved. However, the consensus regarding symptomatic treatment of genitourinary endometriosis remains based on age, severity of symptoms, extent of the disease, duration, and a desire to maintain reproductive ability.1,7,107
Medical management as a postsurgical approach may be used for some patients. In many studies, medical management was initiated after surgical treatment of UE as suppressive therapy.29,32,35,37,45,48,60,110 The decision for adjunct treatment must be individualized based on clinical judgment and the specific need for surgical management.
Surgical management
Surgical management may lead to symptom relief with preservation of renal function.111–114 Minimally invasive laparoscopy appears to be a safe and effective definitive treatment for UE, regardless of the depth or location of involvement.107,115–122 It may involve the laser ablation and excision of endometriosis lesions based on the depth and location of involvement, along with lysis of adhesions while taking care to preserve the blood supplies to the urinary tract.123–125
Reported recurrence rates for UE are low among different surgical approaches, as demonstrated in Table 4. Open surgical approaches for bladder or ureteral endometriosis excision were associated with a higher odds ratio for recurrence compared to robotic assisted laparoscopy (OR 1.16; p = 0.04). 126 Table 4 includes reported surgical complication rates (Calvien-Dindo grade I-IV) and robotic-assisted laparoscopy has lower complication rates and a higher postoperative pregnancy rate. Intra-operative conversion rates from laparoscopy (conventional and robotic combined) to laparotomy range from 0% to 30%.35,40,48,49,127,128
For renal endometriosis, nephrectomy7,64 or partial nephrectomy, with or without nephrostomy, 96 has been performed. Ureteral endometriosis procedures were based on the location and extent of ureteral involvement, as well as proximity to the bladder. Similarly, surgical interventions for endometriotic lesions on the bladder dome were based on the specifics of the involvement. Various surgical approaches are listed in Table 4.
Lastly, and rarely for urethral involvement, excision of the lesion with or without urethral reconstruction is recommended.
Postoperative follow-up
Regular postoperative follow-up is crucial to monitor for recurrence and to manage any ongoing symptoms or complications.6,29,32,35,37,45–48,51,60,110,117,127–134 Follow-up visits are typically scheduled every 3–6 months initially, then annually if stable. Symptom evaluation is performed during every visit for any new or recurring symptoms, such as pelvic pain, dysmenorrhea, or urinary symptoms. Regular serum creatinine and eGFR may be monitored to assess renal function, especially in patients who have undergone multiple surgeries. Mereu et al. reported that repeated ureteral surgeries for endometriosis were associated with higher risks of complications and adverse outcomes. 113
Imaging studies are useful to monitor for recurrence or progression of disease. Re-imaging is recommended based on symptoms or clinical suspicion of recurrence. However, for patients with severe disease or prior significant urinary involvement, periodic surveillance imaging may be considered even in the absence of symptoms. MRI and ultrasound are commonly used to detect recurrences, given their high sensitivity and specificity.31,33,133,135–140 Lastly, long-term hormonal suppression therapy may be considered to reduce the risk of recurrence and delay the need for repeat surgeries.
Discussion
Diagnosis of UE is very challenging 17 and due to its broad clinical presentation, it may be misdiagnosed or diagnosed late. UE can have long term and chronic consequences such as renal failure, pelvic pain, and infertility, which underscores its importance in regard to correct diagnosis and management planning.
Our review suggests that management should be delivered by a multidisciplinary team.17,29,32,35,37,39,40,44–49,51,110,126,128,134,141 The primary specialists include gynecologic endometriosis specialists to assess for multiorgan involvement of deep infiltrating endometriosis and coordinate the overall care, and urologists to evaluate and manage urinary tract involvement. Additional subspecialists may include radiologists to interpret imaging studies accurately and guide intervention, and colorectal surgeons in cases where endometriosis involves the rectum or bowel. In addition, pain management specialists and physiatrists may be helpful to improve quality of life for patients with chronic pelvic pain. Lastly, a referral to fertility specialists may provide counseling and treatment options for patients desiring to conceive.
An initial evaluation may be conducted by gynecologic endometriosis specialists, and urologists. A thorough history and physical examination should be performed in patients presenting with irritative perimenstrual urological symptoms. Imaging and diagnostic tests (e.g. pelvic ultrasound, MRI, and cystoscopy) are subsequently used to assess the extent of endometriosis and its involvement in the urinary tract. A recent systematic review and meta-analysis by Gerges et al. further supports these findings, highlighting the diagnostic accuracy of preoperative imaging in patients with deep infiltrating endometriosis, including urinary tract involvement. The study emphasized the superior performance of MRI and expert-guided transvaginal ultrasound for lesion detection and mapping, particularly in complex anatomical regions, underscoring their value in surgical planning and multidisciplinary management strategies.142–144
Surgical intervention with laparoscopy, or robotic excision of endometriosis, may be considered for definitive treatment. Hormonal therapy is often initiated after surgical treatment as suppressive therapy to improve the outcomes.
Another study by Roman et al. estimates the probability of requiring repeated surgery for endometriosis at 1, 3, 5, 7, and 10 years to be 3%, 11%, 18%, 23% and 28%. Postoperative pregnancy and hysterectomy were statistically significant independent predictors associated with a reduction in the probability of requiring repeated surgery. 145 The probability of repeated surgery for endometriosis increases over time due to several factors. In some cases, initial surgeries may not completely excise all endometriotic lesions, leading to persistent or recurrent symptoms that require additional surgeries. The natural progression of endometriosis can also lead to new lesions forming over time, especially if postsurgical hormonal suppression therapies are ineffective or discontinued. In addition, surgeries themselves can lead to the formation of adhesions, which may cause pain and functional impairment, prompting further surgical management. With this understanding, and our initial data suggesting robotic-assisted laparoscopy may lead to potential reduction in recurrence rates, minimization of surgical complications, and improvement in post-surgical pregnancy outcomes, robotic-assisted laparoscopy may be considered preferentially as the surgical approach when possible.
Robotic-assisted laparoscopy allows for superior visualization of the surgical field, and the dexterity of robotic instruments provides more precise dissection and excision of endometriotic lesions. This precision reduces the likelihood of leaving behind residual disease, which may explain the lower recurrence rates. Laparoscopic approaches also cause reduced tissue trauma, which leads to less blood loss and fewer adhesions, potentially resulting in lower complication rates. Patients typically experience faster recovery with minimally invasive surgeries, allowing for a quicker return to normal activities, including attempts to conceive, thereby potentially contributing to higher postoperative pregnancy rates.
Postoperative surveillance is essential to confirm functional and postoperative outcomes. Regular follow-up also allows monitoring and detection of recurrence.6,29,32,35,37,45–48,51,60,110,127,128,130–135,141 Collaboration between gynecologic endometriosis specialists, urologists, and other relevant specialists during follow-up period should continue for a more comprehensive care.
The current study has several strengths and limitations. We acknowledge the absence of a preserved exclusion log as a limitation that may impact transparency. A formal risk of bias assessment was not performed due to study heterogeneity, which represents another limitation of the review. A key strength of this review is its inclusion of literature spanning four decades, which provides valuable insight into the evolving diagnostic approaches and treatment strategies for UE. Our review is the largest and longest review of urinary tract endometriosis to the best of our knowledge.
One of the limitations remains the quality of the included studies. Clinical practice guidelines remain primarily based on poor to moderate overall quality of evidence. Due to the rarity of this clinical condition, most of the reviewed articles are case series. Medical and surgical management among included studies was not standardized, therefore it was not possible to comment on the comparative efficacy of treatment options. In addition, since the diagnostic technology has evolved, significantly in recent decades, it is possible that more UE cases were identified recently, affecting the reported rates and prevalence. Furthermore, long term follow-up and clinical outcomes were often not reported.
Another limitation involves physician preference in terms of treatment approach, given the non-standardized methods reported in the literature. It is also important to note that during our review we did not find any qualitative study addressing the psychosocial burdens of UE patients regarding the impact on their quality of life and clinical outcomes.
Currently, limited evidence is available to help with the diagnosis and management of UE. While this review provides an extensive summary of the existing literature on the management of urinary tract endometriosis and is likely one of the most comprehensive available, it does not offer a formal comprehensive strategy for clinical practice. Moving forward, it would be beneficial to develop a structured approach based on the findings to guide clinicians in managing these complex cases effectively. A proposed framework could involve comprehensive initial evaluation, multidisciplinary collaboration, personalized treatment plans, and detailed regular follow-up to address and manage recurrence and complications.
Conclusions
UE remains a rare but significant manifestation of deep infiltrating endometriosis. This systematic review synthesizes existing evidence on the epidemiology, diagnostic approaches, and treatment strategies for UE. Bladder and ureteral endometriosis are the most prevalent forms, while renal and urethral involvement is rare and often under-recognized. MRI and transvaginal ultrasound represent the most accurate imaging modalities, and cystoscopy remains essential for evaluating bladder lesions. Definitive treatment often requires minimally invasive surgical excision, with robotic-assisted laparoscopy showing promising outcomes in recurrence reduction and fertility preservation.
Given the lack of standardized guidelines, we emphasize the need for a multidisciplinary approach involving gynecologists, urologists, radiologists, and fertility specialists. Early identification and surveillance are key to minimizing renal compromise and optimizing treatment. Future prospective studies and registry-based research will be essential to develop more robust, evidence-based management algorithms for UE.
Supplemental Material
sj-docx-1-pev-10.1177_22840265261426911 – Supplemental material for Urinary tract endometriosis: Systematic review
Supplemental material, sj-docx-1-pev-10.1177_22840265261426911 for Urinary tract endometriosis: Systematic review by Soorena Fatehchehr, Maggie Jiang and Susan Nasab in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-docx-2-pev-10.1177_22840265261426911 – Supplemental material for Urinary tract endometriosis: Systematic review
Supplemental material, sj-docx-2-pev-10.1177_22840265261426911 for Urinary tract endometriosis: Systematic review by Soorena Fatehchehr, Maggie Jiang and Susan Nasab in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Appendix 1
Authorship
Soorena Fatehchehr, M.D.: Made a substantial contribution to the concept or design of the work, as well as acquisition, analysis and interpretation of data. Drafted the article or revised it critically for important intellectual content. Approved the version to be published. Maggie Jiang D.O.: Made a substantial contribution to the acquisition and analysis of data. Drafted the article critically for important intellectual content. Susan Nasab, M.D.: Made a substantial contribution to the acquisition and analysis of data. Revised the article critically for important intellectual content.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
IRB approval not required given the nature of this study being a retrospective review of current literature.
Trial registration
This review is registered with INPLASY. Registration number INPLASY202420054.
Prior presentation
This review was presented as an abstract at the 2023 AAGL 52nd Annual Global Congress on MIGS.
Data availability statement
Data is available from the authors upon reasonable request.*
Data registration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.