
Abstract
Endometriosis is a chronic gynecological condition with profound consequences. Despite increasing research, studies on health-related quality of life (HRQoL) in endometriosis remain fragmented, often neglecting the interplay between medical and psychosocial aspects. This narrative review aims to provide an integrated perspective on the medical and psychosocial factors influencing HRQoL in individuals with endometriosis. A comprehensive literature search identified peer-reviewed studies examining both qualitative and quantitative research. Medical aspects such as chronic pain, dysmenorrhea, infertility, dyspareunia, fatigue, and treatment side effects were strongly associated with reduced HRQoL. Psychosocial aspects included depression, anxiety, self-esteem, body-image, coping strategies, illness perceptions, and social and work-related challenges. Treatment-related aspects, including diagnostic delay and patient-centered care, emerged as important factors associated with HRQoL. The findings highlight the necessity of a holistic approach to improve patients’ HRQoL. However, research on the implementation and effectiveness of such approaches remains scarce. Future research should prioritize adolescents, longitudinal designs, and integrative analytic frameworks to better capture both short and long-term effects of the complex interactions between medical and psychosocial factors relevant to HRQoL in those affected.
Keywords
Introduction
Endometriosis is a prevalent gynecological condition in women of reproductive age, 1 marked by ectopic endometrial lesions, 2 causing chronic inflammation, 3 scarring, and adhesions that may distort pelvic anatomy. 4 Symptoms include chronic pelvic pain, dysmenorrhea, infertility, back pain, dyspareunia, cyclical micturition or defecation problems, and fatigue.5,6 Chronic pain is the leading symptom, 7 initially cycle-dependent, but eventually persistent. 8 Up to 50% of patients face fertility issues.9,10 The cause-and-effect relationship remains controversial, 9 but endocrine abnormalities and altered pelvic anatomy may impact fertility. 11
Despite a prevalence of 10%–15% among women of reproductive age, 12 awareness of its clinical presentation remains low, 6 with many cases unreported. 1 Research is scarce, and consensus on definition, classification, and treatment is lacking. 2 The multifactorial etiology involves genetic, immunological, hormonal and environmental interactions. 13 This uncertainty hinders causal therapy development, shifting focus to symptom management11,12 through pain medications, hormonal treatments, and surgery. 13 Recurrence and symptom exacerbation remain major concerns. 7 Diagnostic delay averages 10 years 12 due to factors such as reliance on laparoscopy for diagnosis.1,6
Beyond physical burden, endometriosis affects psychological health and social participation, though underexplored. Research indicates psychological distress, 14 impaired mental health, and reduced health-related quality of life (HRQoL 15 ). HRQoL, a multidimensional construct, encompasses physical, psychological, social, and environmental domains. 16 In chronic illnesses like endometriosis, these domains are commonly assessed through subdomains such as physical functioning, emotional well-being, control or powerlessness, self-image, and social aspects. 17 Overall HRQoL in endometriosis is reduced across all domains. 18 Patients are at risk of developing depression and anxiety, 19 and disruption in academic, professional, and economic potential. 12 We want to acknowledge that in this review, the term “patients” refers to all individuals affected by endometriosis, including those with diverse gender identities.
Given the complexity of endometriosis, both psychosocial and medical factors affect HRQoL, with psychosocial factors influencing symptom severity and coping. 20 Understanding and managing endometriosis must include both medical and psychosocial dimensions to improve overall HRQoL for those affected. However, previous reviews have neglected this issue and a holistic approach is needed.
This narrative review addresses these gaps by asking: What medical and psychosocial factors influence HRQoL of women with endometriosis? How do they affect HRQoL? What are methodological limitations in existing research? To answer these questions, it synthesizes existing findings, critically evaluates methodological limitations, and identifies research gaps. Both qualitative and quantitative research are included to capture the complexity of patient experiences and clinical outcomes. By advocating for a holistic framework, it contributes to a comprehensive understanding of the disease’s multidimensional impact. In this review, the term “holistic approach” refers to an interdisciplinary and biopsychosocial perspective that considers medical, psychological, and social factors in conceptualization and clinical management. The insights gained may support the development of practical interventions that address both medical and psychosocial needs and thereby enhance HRQoL of those affected.
Methods
To ensure scientific rigor, the Scale for the Assessment of Narrative Review Articles 21 was used to select high-quality studies, following Baumeister and Leary’s 22 criteria for a structured and comprehensive synthesis. Each eligible study was critically evaluated to ensure methodological rigor and relevance before inclusion. The search terms were intentionally kept broad to allow psychosocial constructs (e.g., self-perception, self-concept) to emerge from the literature rather than being predefined. Figure 1 provides a visual overview of the review process, outlining the steps of literature search, screening, and eligibility assessment.
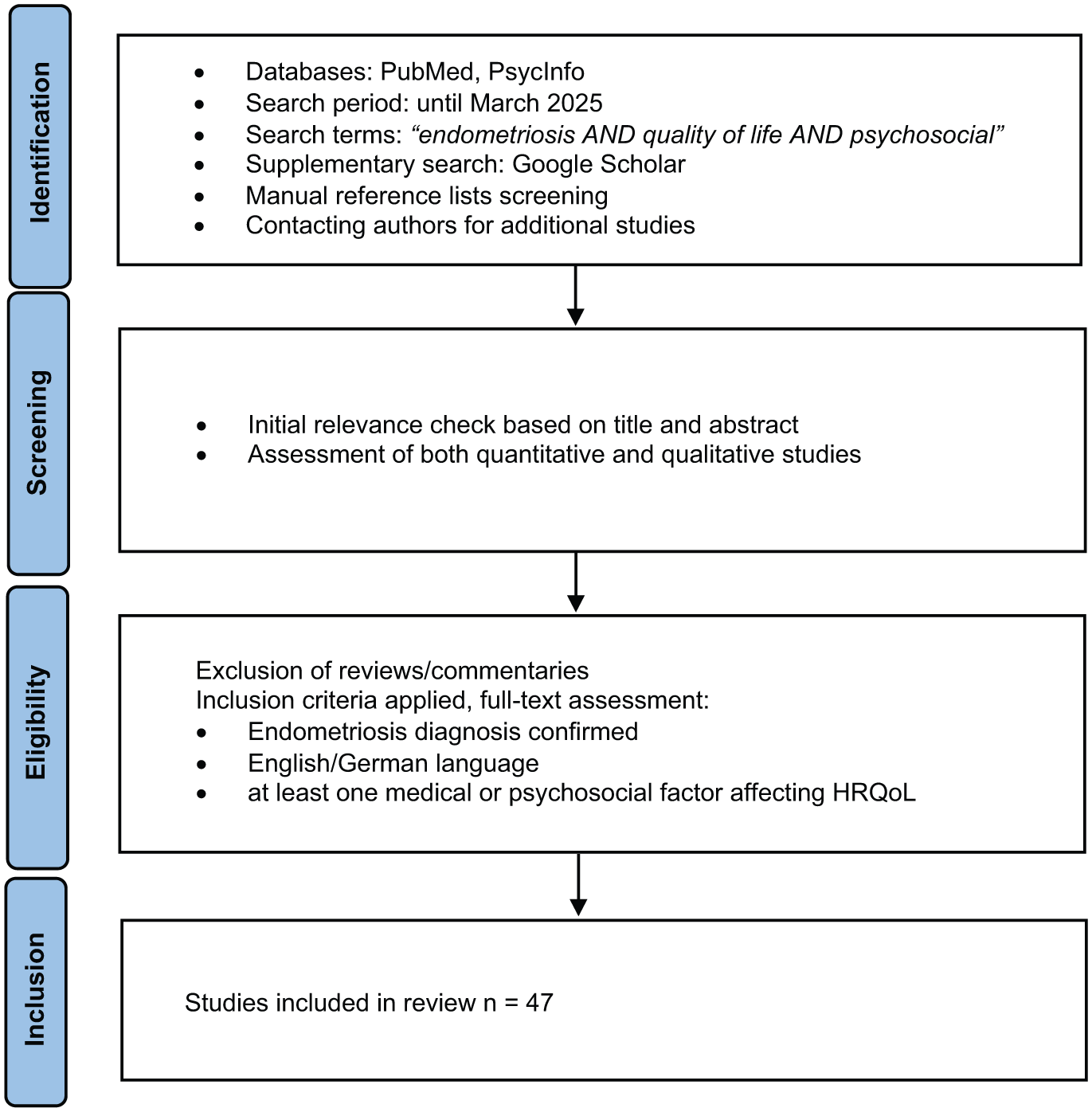
Flowchart of the narrative review process.
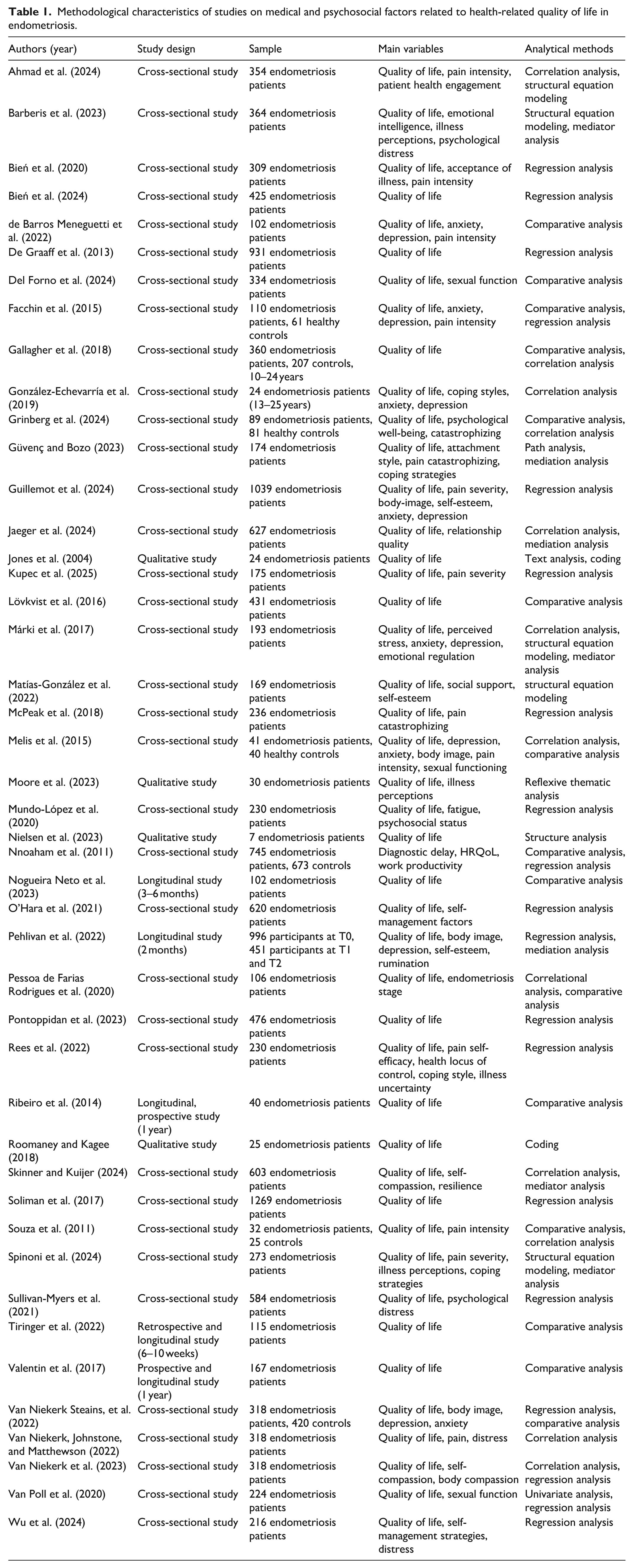
Table 1 outlines the methodological characteristics of selected studies.
Methodological characteristics of studies on medical and psychosocial factors related to health-related quality of life in endometriosis.
Results
Medical factors
HRQoL in endometriosis patients is associated with various medical factors, encompassing somatic features and menstrual cycle characteristics. Chronic pain negatively correlates with HRQoL.23,24 However, the pain-HRQoL association varies across dimensions. Some studies show stronger correlations with the psychological domain, 25 while others find stronger ones with the physical domain. 26 De Graaff et al. 27 found negative effects of pain on both physical and psychological components. Specifically, pelvic pain severity correlates negatively with HRQoL,28–31 particularly within the psychological (emotional well-being, control 32 ) and physical domains (pain experience;32,33 physical functioning 34 ). In adolescents, intensity significantly affects both psychological and physical HRQoL. 35 The negative impact is likely due to reduced physical functioning, including mobility and daily activities, and its recurrent nature. 24
Menstrual irregularities, such as dysmenorrhea, irregular cycles, and heavy bleeding, also reduce HRQoL.24,29,36,37 Dysmenorrhea correlates with lower physical33,38 and psychological HRQoL domains, 24 while heavy bleeding affects the physical (pain), psychological (control, emotional well-being, self-image) and social domain (social support 39 ). The relative impact of dysmenorrhea versus heavy bleeding on HRQoL remains unclear, as comparative studies are limited.
Dyspareunia also affects HRQoL,28,40 impacting psychological, social, 24 and physical domains. 27 Using the same scales, Facchin et al. 38 found no significant effects of dyspareunia on HRQoL in another sample, suggesting moderating factors. Moreover, fatigue reduces HRQoL,36,41 not only predicting HRQoL impairment, 24 but also mediating the pain-HRQoL association. 41 Additional symptoms such as nausea, bloating, anemia, 36 skin problems, 24 and dysuria further diminish HRQoL.24,32 Physical changes such as surgical scarring, abdominal bloating, or weight-gain negatively impact the subdomains within the psychological domain self-image and body-related perceptions,24,34,42 yet research on these factors remains limited. The impact of any endometriosis symptom on HRQoL is profound, particularly in terms of the psychological subdomain powerlessness. 36 Severity and number of symptoms impair the physical subdomains physical functioning and self-care, including standing and walking. 29 Comorbidities independently affect physical and psychological HRQoL. 27 Infertility further negatively impacts HRQoL, 43 despite its emotional burdens manifesting as anxiety, depression, and feelings of inadequacy. 24
Van Niekerk et al. 44 report negative associations between disease severity and psychological HRQoL, while Pessoa de Farias Rodrigues et al. 28 found no significant effects. Symptom duration negatively correlates with HRQoL, 40 particularly in the physical (pain), psychological (control, powerlessness), and social domains (social support 32 ).
Patient age also influences HRQoL, with younger women reporting more severe symptoms and lower overall HRQoL.45,46 Age predicts impairments in the social domain of HRQoL. 34 Adolescents with an early menarche report poorer physical HRQoL. 35 However, physical HRQoL declines with age, while psychological HRQoL tends to improve, 26 suggesting adaptation and changes in expectations.
In summary, while chronic pain and menstrual irregularities have well-established impact on HRQoL, dyspareunia, fatigue, physical changes, and infertility require further exploration. Long-term effects of symptom duration and age require more investigation to improve understanding of the medical factors affecting HRQoL in endometriosis.
Treatment-related aspects
A significant treatment-related factor negatively associated with HRQoL in endometriosis is the delay in diagnosis and treatment.35,46 Impairments on psychological HRQoL (frustration, disillusionment, and psychological distress) often result from unclear explanations or dismissal by healthcare providers. 24 Contributing factors include misdiagnosis, multiple consultations before specialist referral, and inadequate knowledge among healthcare professionals. 24 More visits to general practitioners before referral are negatively associated with the psychological subdomain self-image. 46 The effect of early diagnosis on HRQoL remains unclear, as studies mainly focus on negative consequences of delays.
Pharmacological treatments play a central role in endometriosis but have a complex and sometimes contradictory impact on HRQoL. Prescription medications are negatively associated with physical HRQoL, 26 and opioid use reduces pain (physical domain) but also affects psychological (control), and social subdomains (social support 46 ), raising question on long-term well-being. Hormonal treatments reduce pain and improve HRQoL 46 but may cause side effects side like mood disturbances and weight gain. Despite its widespread use, comparative research on hormonal treatments’ HRQoL outcomes remains limited.
The relationship between surgery and HRQoL also is complex, with both positive and negative effects. Some studies show surgery reduces physical (pain) and psychological domains (control 39 ), while others report improvements in HRQoL,47–49 for example, physical (pain), and psychological (control, emotional well-being, and self-image 32 ). However, improvement may depend on the stage of endometriosis, with minimal cases showing low success rates, 50 highlighting the need for careful patient selection and alternative treatment considerations.
Beyond medical treatments, care delivery significantly impacts HRQoL. Patient-centered care improves all HRQoL domains, 46 with effective communication, education, and emotional support being key. 51 Providing detailed information about disease mechanisms, treatment options, and self-management strategies improves HRQoL. 29 Conversely, feeling neglected or not taken seriously reduces HRQoL. 52 Barriers such as limited access to specialists, inconsistent medical advice, and incorrect diagnoses lower HRQoL and trust in healthcare. 29 Despite growing recognition of patient-centered care’s importance, research evaluating its long-term effects on HRQoL remains limited.
In summary, diagnosis delays are consistently associated with lower HRQoL, yet long-term benefits of early detection remain unclear. Medical and surgical treatments affect HRQoL differently, but interpersonal aspects of healthcare are crucial for endometriosis patients.
Mental-health aspects
Psychological distress symptoms reduce HRQoL in endometriosis patients.44,46 Psychological distress correlates with psychological subdomains such as self-image 53 and predicts lower scores in the psychological subdomains emotional well-being and self-image as well as in the social subdomain social support. 46 Specifically, higher levels of depressive and anxiety symptoms impair HRQoL.18,24,53,54
Beyond symptoms of depression and anxiety, stress, 36 isolation and hopelessness further impair HRQoL, particularly within the psychological domain. 29 Patients describe constant somatic concerns, fear, and unpredictability, particularly regarding pain—factors affecting both the psychological and physical domains of HRQoL.40,52 Emotional distress may manifest as irritability and mood swings, exacerbating overall psychological burden. 24 However, conceptual overlap between stress, uncertainty, and emotional distress complicates measurement.
Body-image is an important, yet understudied aspect in psychological subdomain of HRQoL in endometriosis.18,44 Some women report a sense of incompleteness due to infertility, impacting the psychological subdomain self-perception and overall HRQoL. 24 Evidence further suggests that body-image concerns are not only associated with psychological but also physical HRQoL. 55 Despite its importance, existing research on body image in endometriosis primarily examines the concept in relation to psychological distress, such as depression or anxiety. Broader aspects of self-perception, such as identity, embodiment, and self-concept, are less frequently explored.
Endometriosis symptoms contribute to reduced self-esteem, negatively impacting HRQoL. 29 Recent findings further suggest that higher self-esteem is associated with better psychological and physical HRQoL, indicating that self-esteem may serve as a protective factor across multiple domains. 55 Self-esteem also mediates the relationship between body-image and depression, with negative body-image leading to reduced self-worth and greater depressive symptoms. 42 However, its role in resilience and coping is understudied.
In summary, mental health aspects of endometriosis are complex and impact HRQoL. Research on body-image and self-esteem remains scarce, highlighting the need for further investigation. Additionally, it should be noted that most studies assessed symptoms of psychological distress rather than clinically diagnosed mental health disorders. Therefore, the findings refer to reported symptoms rather than diagnostic prevalence.
Aspects of coping
Coping strategies significantly shape HRQoL in endometriosis patients. 29 Adaptive strategies improving HRQoL include problem-focused coping (self-management, knowledge-seeking, symptom-focused living, social support) and emotion-focused coping (acceptance, positive attitude, self-talk, spirituality 29 ). Problem-focused coping mediates the relationship between attachment anxiety and HRQoL, with lower use leading to poorer outcomes. 56 Engagement in health management also mitigates negative impacts of chronic pain on HRQoL. 22 However, coping preferences vary; some gain control through information-seeking, while others rely on supportive communities. 52
In young patients, self-criticism correlates with work impairment (social domain), mood disturbances (psychological domain), and physical distress (physical domain), while social withdrawal exacerbates the psychological domain and the social subdomain academic career. 57 Conversely, emotional expression, social support, and cognitive restructuring reduce the psychological subdomain mood stability. 57 Maladaptive coping strategies, particularly catastrophizing, are associated with lower HRQoL.33,56,58 and mediate the negative link between pelvic pain and HRQoL. 41
Self-compassion buffers against HRQoL impairment, with resilience mediating its effects on the psychological subdomains emotional well-being and control. 59 Body compassion predicts improvements in the physical and social domains, and overall HRQoL. 60 Self-management behaviors (medication adherence, rest, dietary modifications) improve HRQoL, 37 and self-efficacy predicts HRQoL.26,61 However, causal pathways between self-compassion, self-efficacy, and HRQoL remain underexplored.
Illness perceptions profoundly influence HRQoL. Illness uncertainty impairs physical, psychological, social, and environmental HRQoL. 61 Negative illness perceptions (endometriosis limiting career, relationships, or fertility) further impair HRQoL.62–64 Patients feeling controlled by the disease report fear and identity loss, and reduced levels on the psychological domain. 63 Maladaptive coping mediates these effects, leading to greater HRQoL impairment. 64 Conversely, adaptive coping fosters control and resilience, improving HRQoL. 63 These findings highlight the need for interventions targeting illness perceptions and promoting adaptive coping strategies.
Acceptance of illness is associated with higher physical, psychological, and social HRQoL. 34 Conversely, pain unpredictability induces helplessness and frustration, further reducing HRQoL. 24 Emotional regulation difficulties negatively impact psychological HRQoL, 54 while higher emotional intelligence improves it. 62 Interventions targeting emotional regulation may improve HRQoL outcomes.
In summary, coping strategies, self-compassion, self-management, emotional intelligence, and illness acceptance influence HRQoL. However, research on individual differences remains limited.
Social life and work-related aspects
Endometriosis significantly impacts the social domain of HRQoL, causing isolation, misunderstanding, and loneliness. 24 Unpredictable pain and fatigue lead to missed social gatherings, exacerbating social withdrawal and reducing overall HRQoL. 24 Additionally, endo-stigma stress, defined as social labeling and rejection of differences, negatively correlates with HRQoL. 65 However, social support buffers these effects, highlighting the role of strong interpersonal networks. 65 Yet, research on long-term effects of stigma stress and social support remains limited.
Dyspareunia and infertility frequently impair romantic relationships and sexual well-being, reducing HRQoL.24,29,34 Specifically, reduced sexual functioning is directly associated with poorer overall HRQoL, 66 and the strength of this relationship varies according to severity and type of dyspareunia. 67 Reduced libido and lower relationship quality correlate with poorer outcomes in the social and psychological domains.18,68 Interestingly, being in a relationship is associated with higher psychological HRQoL, 26 suggesting that emotional support mitigates distress. However, most studies rely on cross-sectional data, limiting causal conclusions.
Endometriosis profoundly affects the social subdomain professional life. Many women experience guilt when taking leave from professional responsibilities due to symptoms.24,29 In male-dominated workplaces, shame and the need to justify absences further impair HRQoL. 24 Chronic pain and fatigue interfere with career progression and workplace engagement, 39 yet research on workplace adaptations and employer support remains scarce. Additionally, many patients struggle with childcare 29 and worry about transmitting endometriosis to their daughters, increasing psychological distress. 24
In summary, endometriosis reduces HRQoL by affecting social life, relationships, work, and parenting, with social isolation, stigma, and relationship strain adding to its psychological burden.
Based on the findings of this review, Figure 2 illustrates a holistic model of HRQoL in endometriosis.
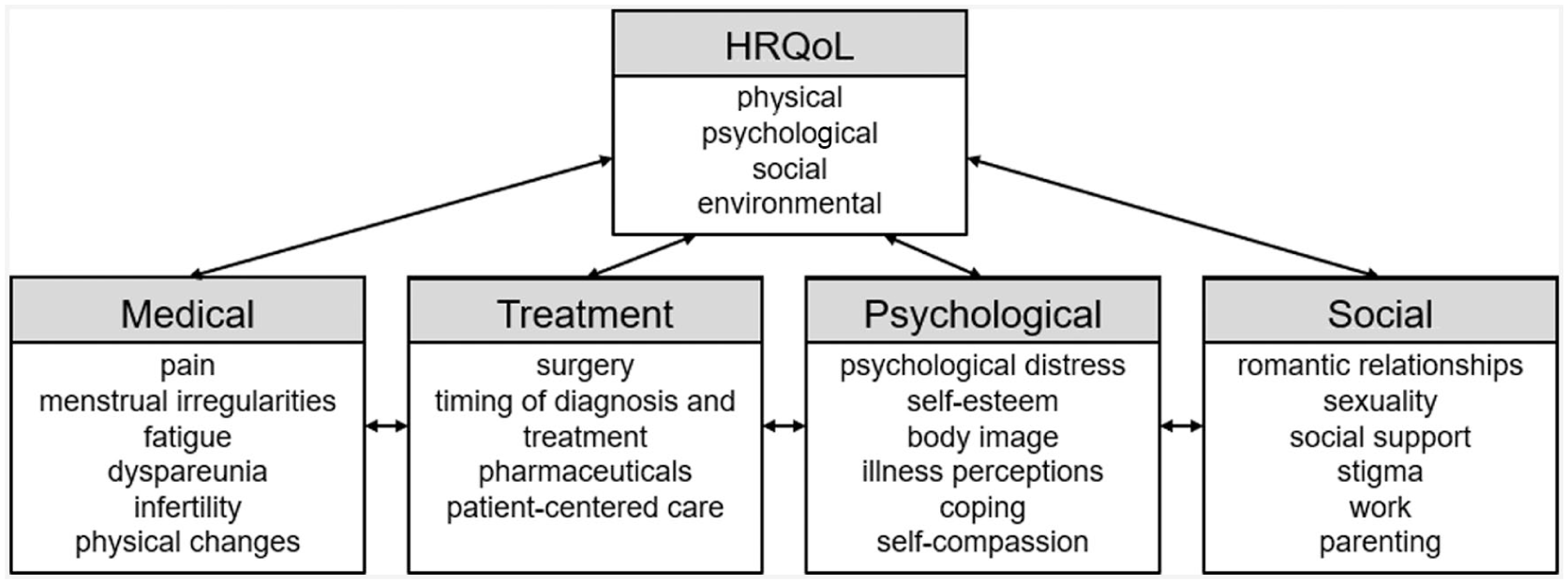
Holistic model of HRQoL in endometriosis.
Discussion
This review underscores the substantial impact of endometriosis on HRQoL, spanning physical, psychological, social, and, although less frequently examined, environmental domains. Chronic pain, menstrual irregularities, fatigue, and infertility significantly impair HRQoL, with pain as the primary factor. Diagnostic delays and inconsistent healthcare further diminish HRQoL. Mental health issues, self-esteem, coping strategies, self-compassion, and patient engagement emerged as crucial factors. Social support and interpersonal relationships also influence HRQoL, as patients frequently experience social isolation, stigma, and challenges in relationships and professional settings. The review demonstrates the fundamental influence of medical and psychosocial factors on HRQoL in endometriosis.
However, the predominance of cross-sectional studies limits causal interpretations, as these designs capture only a single time point and cannot determine the temporal direction of associations between psychosocial factors and disease outcomes. Consequently, it is not clear whether factors such as depression, anxiety, and social support contribute to changes in disease progression and quality of life or are a consequence of disease burden. Longitudinal research is necessary to evaluate these dynamics over time, especially across significant life stages such as adolescence, pregnancy, and menopause. Such research would provide a more comprehensive understanding of the relationship between psychological and medical factors. Additionally, this review only included English- and German-language studies, which limits the generalizability of the findings to other cultures. Recognizing these limitations is important because both the reliance on cross-sectional designs and the language restrictions constrain the conclusions. This fact highlights the need for future studies with different cultures and longitudinal designs. A common methodological feature across reviewed studies is the use of standardized self-report instruments, which may introduce bias. 69 However, self-report remains the most appropriate method for assessing psychosocial constructs in endometriosis. Many of these experiences, such as pain and HRQoL, are inherently subjective and cannot be meaningfully captured through objective indicators alone. Although self-report measures can introduce biases, this fact is mitigated if well-validated instruments are used and if self-report data is supplemented with other methods such as objective data where possible. Further, psychosocial variables (e.g., social support and coping strategies) are frequently examined separately rather than within an integrative analytical framework. In this review, “integrative models” refers to multi-layered statistical approaches that can examine medical, psychological, and social determinants of HRQoL simultaneously. Advanced techniques, such as mediation and moderation analyses, multivariate path models, and structural equation modeling, remain underutilized. These techniques would enable researchers to map indirect effects, reciprocal pathways, and the joint contribution of biological and psychosocial stressors. These models could clarify how factors interact over time, moving the field beyond simple bivariate associations. Additionally, further research on psychosocial experiences of adolescents is warranted, as symptoms often emerge at puberty, a period associated with educational disruptions and body-image concerns. Also, patient-centered approaches remain underutilized despite evidence that shared decision-making, disease education, and psychological support enhance well-being. Many healthcare systems fail to implement these practices, leaving patients feeling disregarded. Greater mental health service integration is essential to optimize patient care.
A comparison with previous reviews reveals both converging and diverging findings regarding medical and psychosocial aspects of HRQoL in endometriosis. Prior research underscores the impact of chronic pain, dysmenorrhea, dyspareunia,70–72 infertility, 73 and mental health disorders on HRQoL.70,74–76 Social and occupational consequences on HRQoL are equally well-documented.70,72,75,77 Consistent with prior literature, delayed diagnosis and inadequate healthcare interactions reduce HRQoL. 75
Unlike reviews that focus solely on medical or psychosocial factors (e.g., Della Corte et al., 70 Heng and Shorey 73 ), this review integrates both dimensions within a holistic framework, addressing underexplored areas such as self-perception, body dissatisfaction, and identity-related concerns. It broadens perspectives on coping, considering maladaptive (e.g., catastrophizing) and adaptive strategies (e.g., self-compassion, cognitive restructuring, social engagement). Moreover, it extends the literature by highlighting the psychological impact of infertility on identity, relationships, and HRQoL, aspects rarely addressed in past reviews. While prior reviews acknowledge diagnostic delays, this review also explores how patient-provider interactions, shared decision-making, and emotional support influence HRQoL. Unlike most reviews relying solely on quantitative HRQoL scales, this review incorporates qualitative and quantitative research, offering a comprehensive exploration of subjective experiences. Still, this review, like all of the previous ones, is limited by language restrictions, potentially introducing language bias by excluding relevant non-English studies, and by publication-bias, as non-significant findings are less frequently published.
The findings of this review have several practical implications for improving the HRQoL of individuals with endometriosis. Due to the multidimensional nature of the condition, clinical management should take a biopsychosocial and patient-centered approach. First, integrating mental health professionals into endometriosis care through embedded psychotherapy, psychoeducation, or depression and anxiety screening pathways could reduce the psychological burden on patients and improve their emotional and social functioning. Interventions that target maladaptive illness perceptions and enhance adaptive coping strategies, such as cognitive restructuring, self-compassion, and resilience training, may further mitigate the negative effects of chronic pain and uncertainty. Routine assessment of psychosocial factors, such as psychological distress, illness perceptions, coping strategies, and social support, could complement medical evaluations. These psychosocial factors substantially shape HRQoL outcomes and often interact with symptom severity. Second, multidisciplinary care models combining gynecology, pain medicine, psychology, and physiotherapy may be beneficial to endometriosis patients, especially those with complex symptom profiles. These models support individualized treatment planning, strengthen self-management skills, and reduce care fragmentation. Third, patient-centered communication has been shown to build trust in the therapeutic relationship, improve treatment adherence, and positively impact HRQoL. As diagnostic delays and negative healthcare experiences contribute to psychological distress and reduced HRQoL, integrating patient-centered communication with early symptom recognition in primary care and establishing standardized referral pathways and systematic provider training are essential strategies for mitigating distress and supporting patients. Finally, given the substantial impact of endometriosis on social participation, work functioning, and intimate relationships, supportive workplace policies, couple-based interventions, and peer support programs may reduce isolation and stigma while strengthening social HRQoL. Together, the findings of the present review underscore the importance of integrated, multidisciplinary, psychosocially informed care models that address the intricate interplay between medical and psychosocial factors which influence HRQoL in endometriosis.
Conclusion
In sum, significant advancements have been made in understanding the medical (e.g., pain, infertility) and psychosocial (e.g., depression, relationships) impact of endometriosis on HRQoL across its physical, psychological, social, and environmental domains, yet key gaps remain. Endometriosis is a complex condition that extends beyond physical symptoms.
This review contributes to the field by synthesizing existing research, highlighting methodological limitations (e.g., lack of longitudinal, integrative designs) and underexplored factors (e.g., illness perceptions, coping strategies). By incorporating qualitative and quantitative research, it provides a broad perspective on HRQoL impairments. This review emphasizes medical and psychosocial aspects of endometriosis, contributing to a holistic understanding of the multidimensional impact. Importantly, our findings highlight that the interplay between medical and psychosocial factors is crucial in shaping HRQoL outcomes and developing effective support strategies. Future research should prioritize longitudinal designs, adopt holistic frameworks, and expand beyond adult populations to fully capture patients’ experiences.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.