
Abstract
Introduction:
The COVID-19 pandemic has substantially impacted the management of chronic conditions, particularly endometriosis. This study aims to analyze the effects of the pandemic on the quality of life among women with endometriosis under the care of an academic referral center in Italy.
Methods:
Conducted from June to October 2020, this observational study utilized an online survey to assess various health dimensions. The participants included women with a confirmed diagnosis of endometriosis whose clinic appointments were cancelled, and new ones were difficult to schedule due to COVID-19 pandemic restrictions. The online questionnaire comprised 117 questions designed to evaluate chronic pelvic pain, quality of life, and psychological impacts using validated scales such as SF-12, HADS, EHP-5, and PSQI.
Results:
A total of 105 participants completed the online questionnaire. It was found that pandemic-related disruptions in healthcare services exacerbated symptoms of endometriosis, increased pain levels, and heightened psychological distress among participants. Specifically, 23.8% of patients reported increased pain due to delays in medical consultations and treatments caused by the pandemic. Results indicated significant correlations between higher levels of anxiety, depression, and deteriorated physical and mental health. The analysis revealed that pandemic-related stress and disruptions in routine care were significant predictors of worsened symptoms and overall health status in patients with endometriosis.
Conclusion:
The study underscores the need for integrated care approaches that address both the physical and psychosocial aspects of endometriosis, especially during healthcare crises. Enhanced support and resources are essential to mitigate the impact of such disruptions on chronic disease management and improve the quality of life for those affected.
Introduction
Endometriosis is a chronic gynecological condition characterized by endometrial-like tissue outside the uterine cavity, necessitating ongoing medical management to prevent the exacerbation of clinical manifestations.1–3 This disease affects an estimated 10% of women worldwide, exerting a substantial burden on individual health and healthcare systems. 4 In Italy, it is estimated that endometriosis affects approximately 3 million women, presenting commonly with pelvic pain—a complex symptom often associated with dysmenorrhea, dyspareunia, and dyschezia. 5 The chronic nature of endometriosis profoundly impacts the quality of life (QoL), adversely affecting various facets of life including work, social interactions, and physical and psychological health.6,7 The onset of the coronavirus disease 2019 (COVID-19) pandemic, instigated by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that emerged in China in late 2019, has rapidly become a pivotal health emergency. Recognized as a global pandemic by the WHO on 11th March 2020, it has led to dramatic changes in healthcare delivery. 8
The Italian government’s strict distancing measures, aimed at reducing virus transmission, inadvertently disrupted medical services, particularly those concerning the management of non-urgent, benign conditions such as endometriosis. The healthcare sector’s pivot toward COVID-19 has resulted in the deferral of elective surgeries, the suspension of fertility services, and the postponement of routine consultations, thus disrupting the continuity of care for those with chronic illnesses.9–11 Moreover, the pandemic and its associated restrictions have been a source of increased anxiety and stress, which may exacerbate symptoms of endometriosis, leading to further deterioration in QoL.12,13
This study aims to analyze the impact of the COVID-19 pandemic on the QoL among a cohort of women affected by endometriosis under the care of our academic referral center. It examines how disruptions in healthcare access, such as delayed consultations and postponed surgeries, affected symptom severity and disease progression. Additionally, the study explores the psychological impact, including increased anxiety, depression, and feelings of medical abandonment, alongside the broader social consequences, such as challenges in work, daily routines, and interpersonal relationships.
Materials and methods
This study was conducted from 1st June to 30th October 2020 at the Center for Endometriosis and Pelvic Pain of the Duilio Casula University Hospital (Monserrato, Cagliari, Italy), in accordance with the Declaration of Helsinki, adhered to the Committee on Publication Ethics guidelines and complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines. 14 The study’s protocol received approval from the local Ethics Committee (Ref. No. PG/2020/14096), ensuring adherence to ethical research standards.
Recruitment
Participants were women aged 18–48 years who had previously been evaluated at our institution and whose clinic appointments had been cancelled due to the COVID-19 pandemic-related restrictions. Eligibility for inclusion in the study was predicated upon a confirmed diagnosis of endometriosis, which had been established surgically or via ultrasound. We excluded potential participants if they had been diagnosed with psychiatric disorders or cancer diseases.
The selected patients were invited to complete an anonymous online survey via e-mail. This survey aimed to provide insight into the impact of the COVID-19 pandemic on their condition and QoL while ensuring the confidentiality of their responses.
All the participants provided their informed consent for the collection and use of their data in this study.
Data collection and assessment
The online questionnaire, consisting of 117 questions, was meticulously constructed using measurement scales designed explicitly to assess endometriosis chronic pelvic pain and evaluate quality of life in various contexts7,15,16:
- SF12 (Short Form Health Survey) 17 : This abbreviated version of the SF-36 questionnaire consists of eight items focusing on two domains: the physical component summary (PCS) and the mental component summary (MCS). Higher scores indicate a better QoL.
- HAD SCALE (Hospital Anxiety and Depression Scale) 18 : Comprising 14 questions, this scale assesses the influence of mood disorders, particularly anxiety and depression, on the distress experienced by patients. Responses are scored from 0 to 3, with 3 indicating the highest frequency of symptoms. Subscale scores (anxiety and depression) range from 0 to 21, with scores categorized as follows: normal (0–7), mild (8–10), moderate (11–14), and severe (15–21). The total score (emotional distress) ranges from 0 to 42, with higher scores indicating more significant distress.
- EHP-5 (Endometriosis Health Profile) 19 : This shortened version of the EHP-30 questionnaire, the only validated tool for assessing Health-Related Quality of Life (HRQoL) in endometriosis, consists of 11 questions evaluating the QoL of women affected by endometriosis.
- PSQI (Pittsburgh Sleep Quality Index) 20 : Comprising 19 items, this scale measures sleep quality and any sleep disturbances experienced over the past month. Component scores are summed to calculate the global PSQI score, ranging from 0 to 21, with higher scores indicating greater sleep impairment. A global PSQI score above 5 is considered indicative of sleep disturbances.
Additionally, the questionnaire included 37 questions related to symptoms and experiences during the Covid-19 pandemic, evaluated on a VAS (Visual Analog Scale) from 1 to 10 by the patients, and 28 questions for gathering demographic and anamnestic data, such as age, Body Mass Index (BMI), parity, comorbidities, marital status, level of education, history of previous pelvic surgeries, current hormone therapies, and the localization of endometriosis.
Data analysis
In our analysis, we aligned the collected data from the online survey with existing literature, contrasting our findings with control groups and clinical samples of women with endometriosis from the pre-pandemic era, where available. For the SF12, HADS, and PSQI values, comparisons were explicitly drawn from studies with Italian women to ensure cultural relevance. Due to the absence of normative values in Italy for the EHP-5, we utilized data from a Spanish sample as a comparative benchmark. This comparison with both control groups and clinical samples of women with endometriosis before the pandemic provided a comprehensive understanding of the impact of COVID-19 on our cohort.
Statistical analysis
In this study, non-parametric descriptive and inferential statistical methods were employed, utilizing open-source software Jamovi (version 2.2.5) and Jasp (release 0.16.2.0), with a significance level set at <0.05. The online survey data analysis involved calculating aggregate scale scores, with Spearman’s Rho coefficient assessing inter-scale correlations. We compared these scores to pre-pandemic literature benchmarks via the Student’s t-test.
Results
A total of 119 participants were initially contacted to complete the online questionnaire. However, 14 participants were excluded due to various reasons: seven participants had incomplete responses, four did not meet the inclusion criteria, and three were excluded because they did not provide consent for data usage, resulting in 105 completed questionnaires. The detailed patient characteristics, symptoms assessment, treatment, healthcare access, and concerns are synthesized in Table 1. The mean age of this subgroup was 37.36 years. Employment status was high, with 58.7% working. Education levels showed that 44.2% had obtained a high school diploma, while 27.9% had a university degree. Smoking habits were predominantly absent, with 81.9% identifying as non-smokers. The mean age at first menstruation was recorded at 12.02 years.
Data collected from online survey.
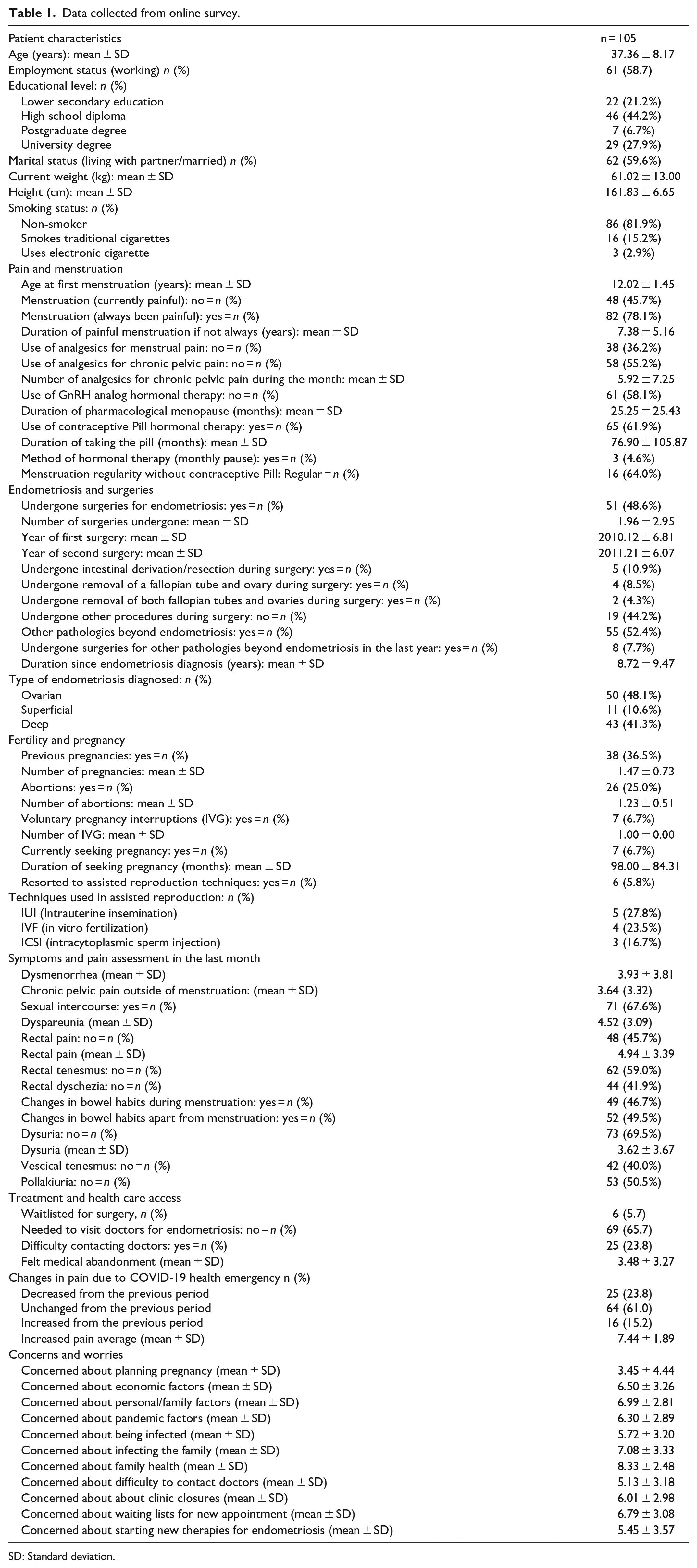
SD: Standard deviation.
Regarding menstrual pain, 45.7% reported no current pain, whereas 78.1% had always experienced painful menstruation. For those whose menstruation was not always painful, the duration of the painful experience averaged 7.38 years. In terms of pain management, 36.2% did not use analgesics for menstrual pain, and 55.2% did not use them for chronic pelvic pain, with an average of 5.92 analgesics used per month by those who did. Hormonal treatments varied, with 58.1% not using GnRH analogs and 61.9% using contraceptive pills. The mean duration of pharmacological menopause was 25.25 months, and the average time on the pill was 76.90 months. Surgical intervention for endometriosis was reported by 48.6% of participants, with an average of 1.96 surgeries undergone. A small proportion had undergone significant surgical procedures, including intestinal derivation/resection (10.9%), removal of a fallopian tube and ovary (8.5%), or both tubes and ovaries (4.3%). Additional pathologies beyond endometriosis were reported by 52.4% of participants, with 7.7% having undergone surgery for such pathologies within the last year. The diagnosis of endometriosis had been established for an average of 8.72 years, with various types documented, including ovarian (48.1%), superficial (10.6%), and deep (41.3%) endometriosis. Reproductive history showed that 36.5% had previous pregnancies, averaging 1.47 per person. The rate of abortions stood at 25.0%. A small number were actively attempting to conceive a child (6.7%), and 5.8% had resorted to assisted reproduction techniques. In the last month, the mean score for dysmenorrhea was 3.93, chronic pelvic pain outside menstruation was 3.64, and dyspareunia was 4.52. A considerable proportion of the sample experienced rectal pain (54.3%), tenesmus (41.0%), and dyschezia (58.1%). Almost half reported changes in bowel habits during (46.7%) and outside of menstruation (49.5%). Dysuria was absent in 69.5% of the cohort, with an average pain intensity of 3.62 for those affected.
Concerns about economic, personal, familial, and pandemic factors yielded scores ranging from 5.13 to 8.33. The impact of the COVID-19 pandemic on healthcare access and management of endometriosis was reflected in various aspects. While a small percentage was waitlisted for surgery (5.7%), a considerable number did not need to visit doctors for endometriosis (65.7%), and some experienced difficulty in contacting doctors (23.8%). The mean score for felt medical abandonment was 3.48. The changes in pain due to the health emergency showed that 23.8% reported an increase, 61.0% no change, and 15.2% a decrease from the previous period.
The results from Table 2 provide an in-depth overview of the health-related QoL, psychological distress, and sleep quality among the 105 participants who completed the online questionnaire assessing the impact of endometriosis.
Questionnaire scales results.
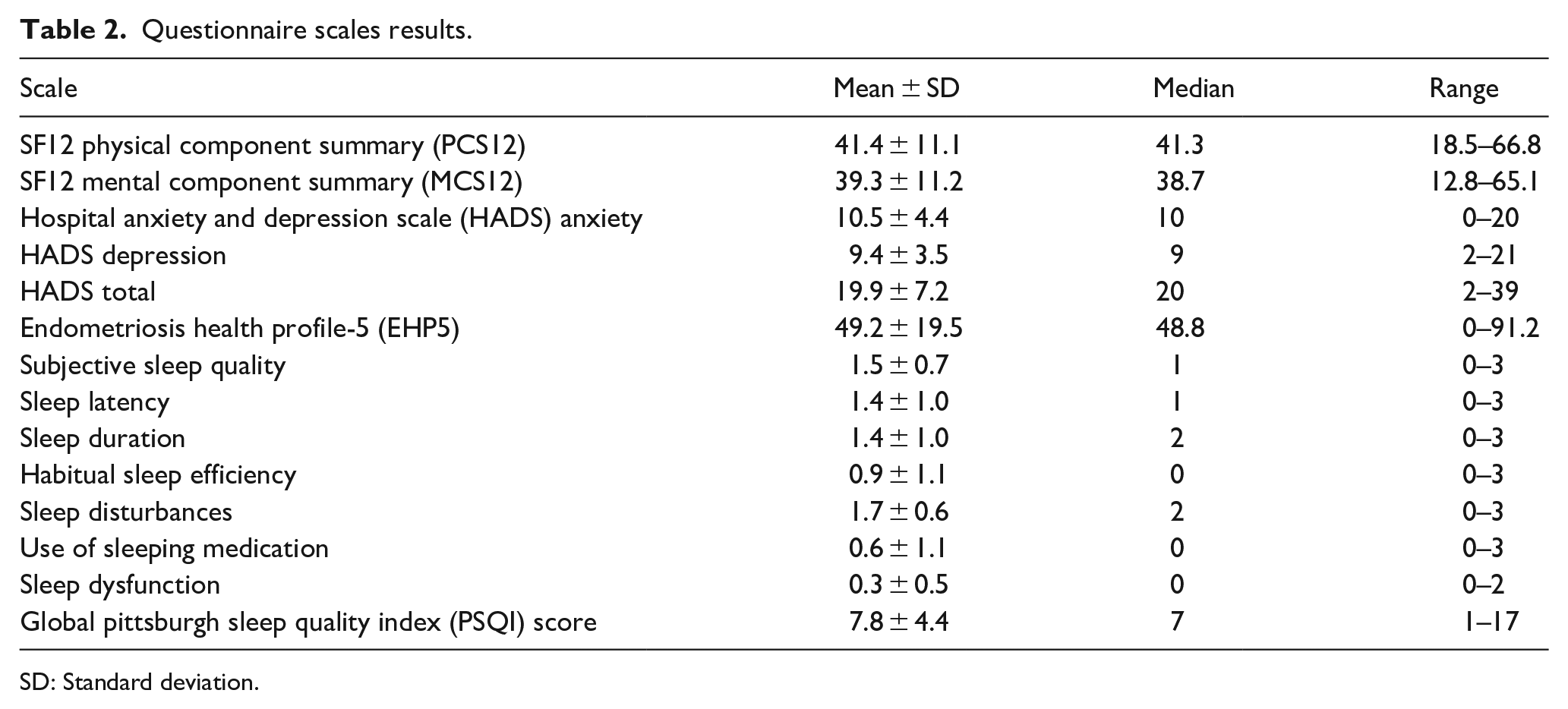
SD: Standard deviation.
The SF12 Physical Component Summary (PCS12) revealed an average score of 41.4 (SD = 11.1), ranging from 18.5 to 66.8. The Mental Component Summary (MCS12) showed a similar diversity in mental health, with an average score of 39.3 (SD = 11.2) and a range from 12.8 to 65.1.
Psychological distress, as measured by the Hospital Anxiety and Depression Scale (HADS), was notably high. The mean anxiety score stood at 10.5 (SD = 4.4), with scores ranging from 0 to 20, while the depression score averaged 9.4 (SD = 3.5), with a range from 2 to 21. The combined HADS total score further emphasized the psychological burden, averaging 19.9 (SD = 7.2) and spanning from 2 to 39.
The Endometriosis Health Profile-5 (EHP5) provided insights into the disease's impact on participant’s QoL. With an average score of 49.2 (SD = 19.5) and a range from 0 to 91.2, the EHP5 highlighted the significant variability in experiences among women with endometriosis.
Sleep quality, evaluated through various PSQI components, showed that participants experienced diverse sleep-related issues. The Global PSQI Score averaged 7.8 (SD = 4.4), suggesting a general trend toward poor sleep quality among respondents. Specific aspects of sleep, such as Subjective Sleep Quality, Sleep Latency, Sleep Duration, Habitual Sleep Efficiency, Sleep Disturbances, Use of Sleeping Medication, and Sleep Dysfunction, revealed scores that further detailed the nature of sleep difficulties faced by the participants, with mean scores ranging from 0.3 to 1.7, reflecting varied extents of sleep disturbances and the impact of endometriosis on sleep patterns.
Spearman's Rho coefficient analysis of the interrelationships among various health and psychosocial measures revealed significant findings, as illustrated in Table 3. For instance, the SF12 Physical Component Summary (SF12 PCS) and Mental Component Summary (SF12 MCS) scores showed a negative correlation with anxiety and depression scores from the HADS, underscoring the inverse relationship between QoL dimensions and psychological distress. More specifically, a strong negative correlation was found between SF12 MCS12 and HADS Depression (−0.673, p < 0.001), indicating that as mental health component scores decrease, depression scores tend to increase significantly.
Spearman’s rho correlations among health and psychosocial scales.
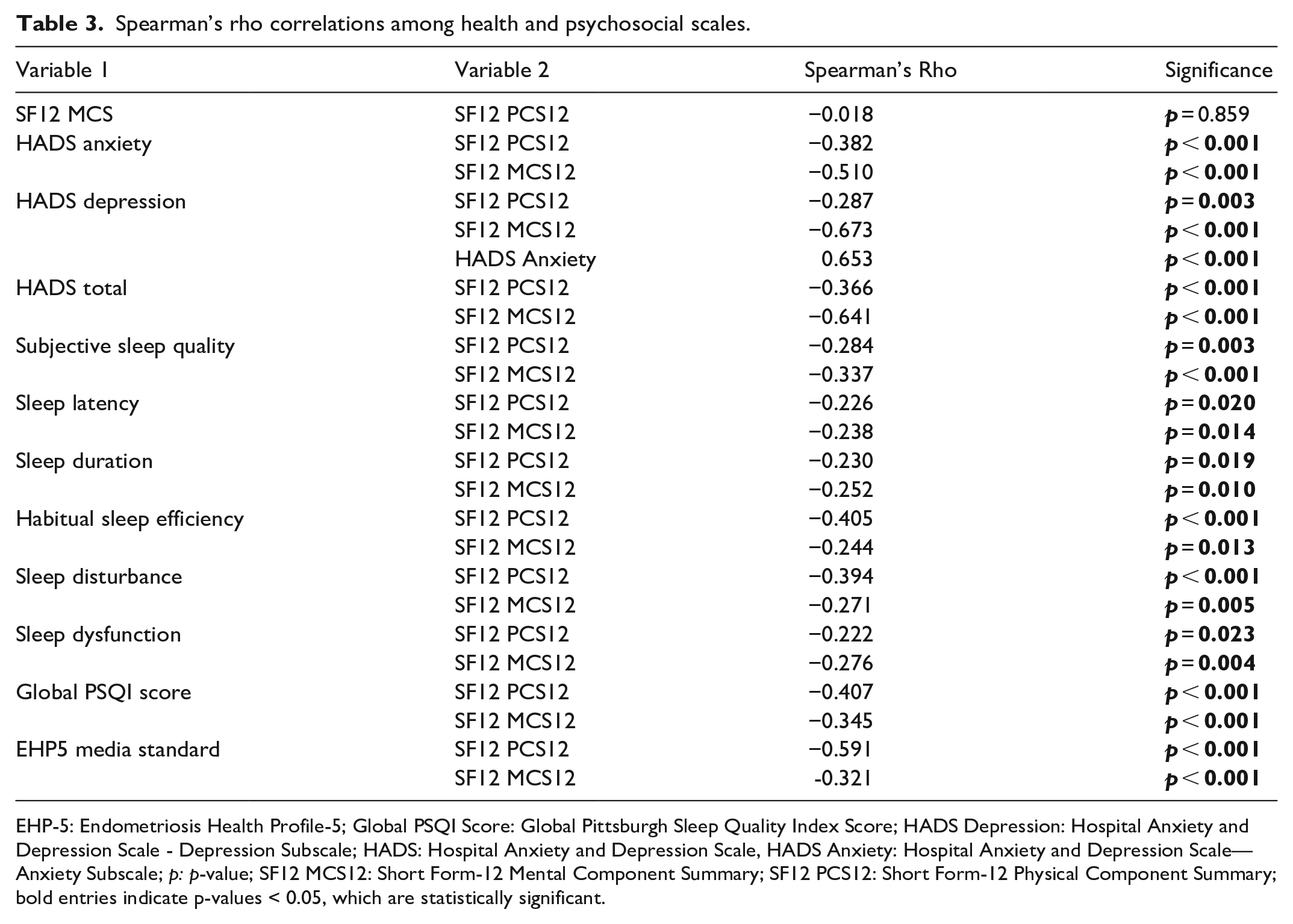
EHP-5: Endometriosis Health Profile-5; Global PSQI Score: Global Pittsburgh Sleep Quality Index Score; HADS Depression: Hospital Anxiety and Depression Scale - Depression Subscale; HADS: Hospital Anxiety and Depression Scale, HADS Anxiety: Hospital Anxiety and Depression Scale—Anxiety Subscale; p: p-value; SF12 MCS12: Short Form-12 Mental Component Summary; SF12 PCS12: Short Form-12 Physical Component Summary; bold entries indicate p-values < 0.05, which are statistically significant.
Moreover, the Global PSQI Score showed a positive correlation with both HADS anxiety (0.541, p < 0.001) and depression scores (0.516, p < 0.001), suggesting that higher anxiety and depression are associated with worse sleep quality. Notably, the Global PSQI Score exhibited significant positive correlations with subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, and sleep dysfunction, reflecting the multifaceted impact of poor sleep on overall health and well-being.
The correlations extend to the media EHP5 standard, which is positively correlated with HADS total (0.448, p < 0.001), indicating that worse endometriosis-related QoL is related to higher anxiety and depression scores.
Utilizing the K-means clustering method, our analysis delineated two primary patient clusters regarding their adaptation to endometriosis and the COVID-19 pandemic: Cluster 1 comprises well-adapted individuals, and Cluster 2 includes those less adapted. As illustrated in Figure 1, Cluster 1 patients scored more favorably on the SF12 PCS and MCS health surveys, suggesting a better health status, whereas Cluster 2 patients indicated a more adverse health impact, as reflected by their lower scores in these areas. Additionally, concerns regarding economic, personal, and health system factors were more acute among Cluster 2 patients.
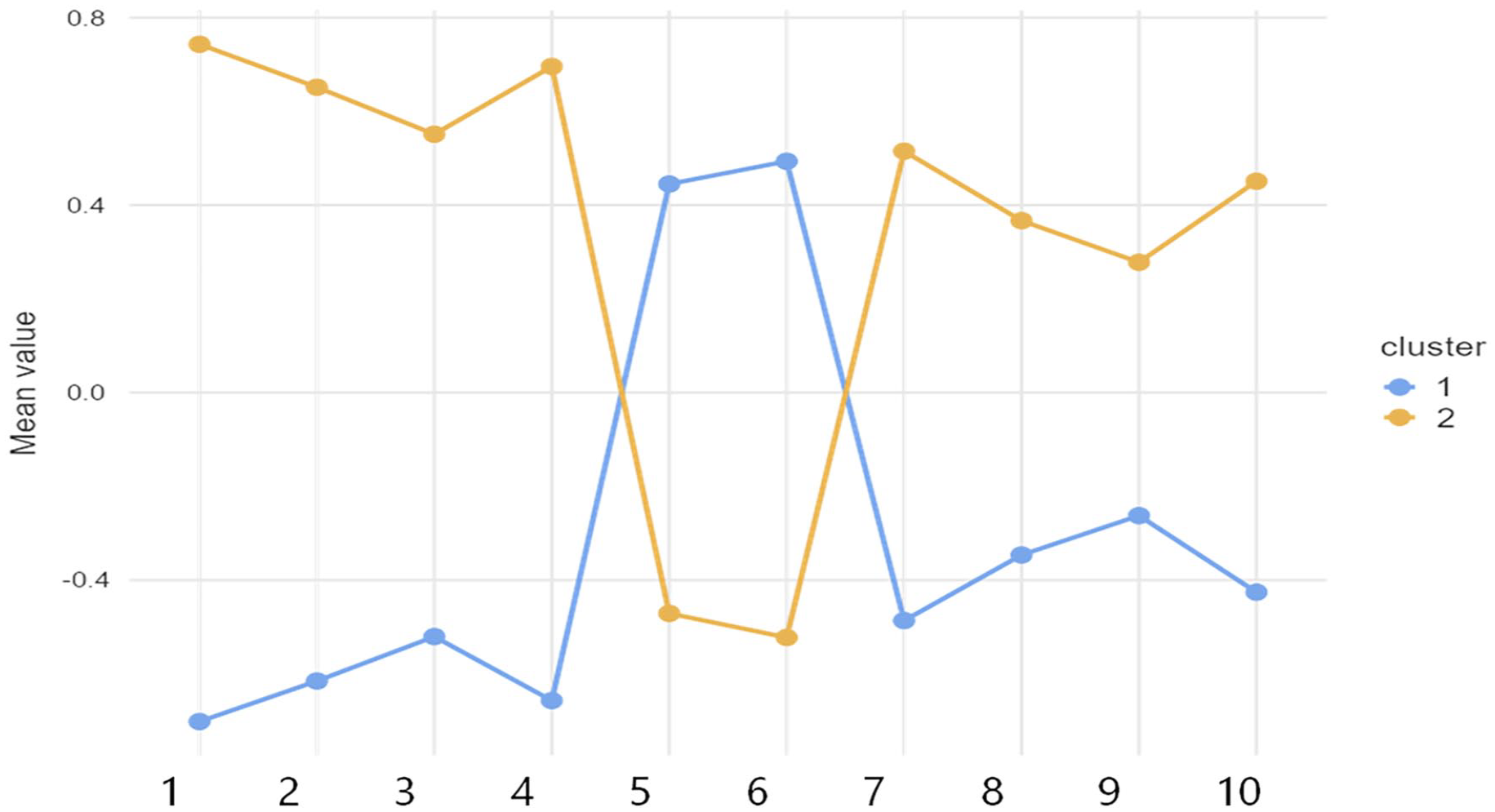
Plot of means across clusters.
The contrast between the clusters is particularly evident in their reported experiences of pain during the pandemic. As indicated in Table 4, 39.2% of Cluster 2 patients experienced increased pain, a significant difference compared to the 9.3% in Cluster 1. This discrepancy underscores the heightened pain challenges the less adapted group faced during the pandemic.
Contingency tables cluster.
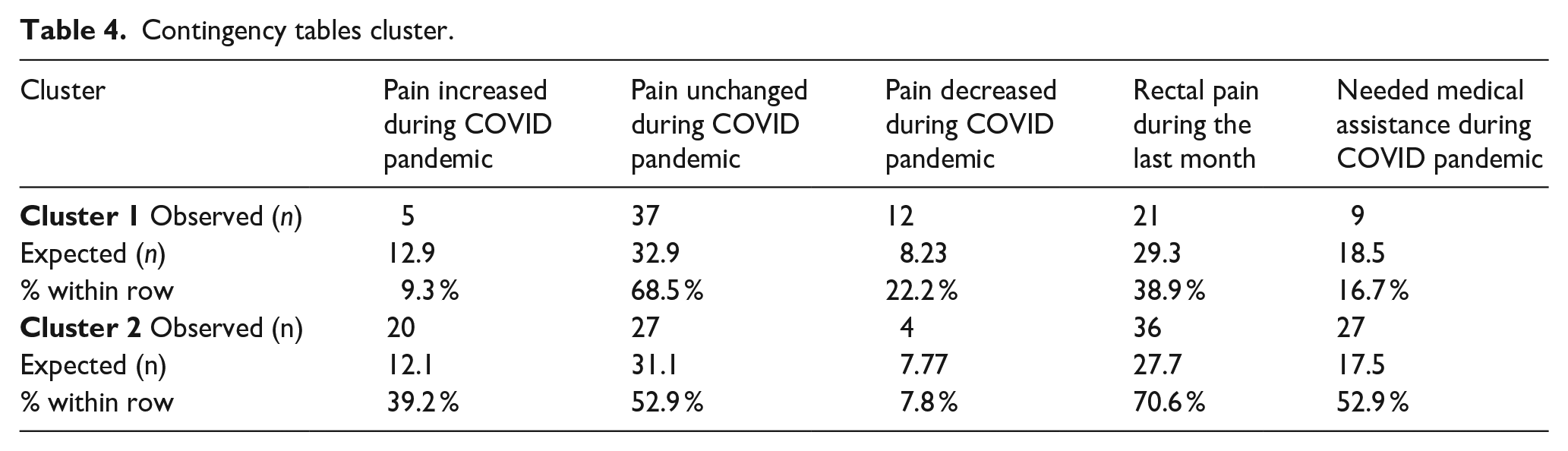
Furthermore, the prevalence of rectal pain was notably higher within Cluster 2, with 70.6% of these patients reporting such pain in the previous month, compared to 38.9% in Cluster 1. This finding emphasizes the variation in clinical symptoms between the clusters.
The need for medical assistance also differed markedly between the clusters. Cluster 2 patients more frequently required medical attention during the pandemic, with 52.9% seeking assistance versus 16.7% in Cluster 1, a substantial discrepancy highlighted in Table 4. This difference points to a greater demand for healthcare resources among patients less adapted to managing their condition during the pandemic.
Additionally, a thorough analysis was conducted by carefully comparing the data collected from the online survey with the existing literature presented in Table 5. We focused on highlighting the differences between our observations and the observations from both control groups and clinical samples of women with endometriosis collected before the pandemic, where such data were available.
Health scales and comparison with literature data.
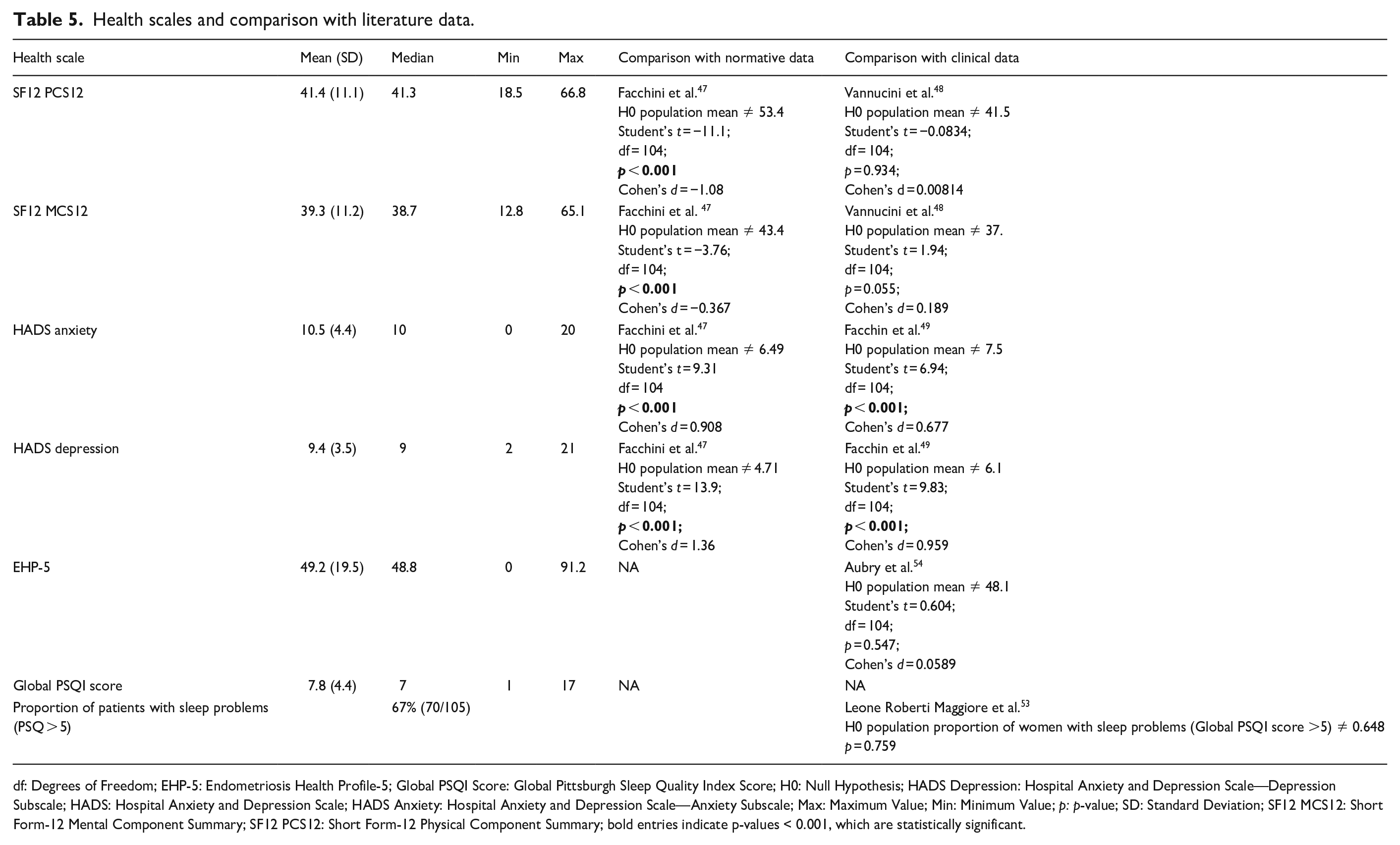
df: Degrees of Freedom; EHP-5: Endometriosis Health Profile-5; Global PSQI Score: Global Pittsburgh Sleep Quality Index Score; H0: Null Hypothesis; HADS Depression: Hospital Anxiety and Depression Scale—Depression Subscale; HADS: Hospital Anxiety and Depression Scale; HADS Anxiety: Hospital Anxiety and Depression Scale—Anxiety Subscale; Max: Maximum Value; Min: Minimum Value; p: p-value; SD: Standard Deviation; SF12 MCS12: Short Form-12 Mental Component Summary; SF12 PCS12: Short Form-12 Physical Component Summary; bold entries indicate p-values < 0.001, which are statistically significant.
Discussion
Characterized by an average age of 37.36 years, the demographic profile of our participants is representative of the primary age demographic impacted by endometriosis, as shown by Parasar et al. 21 These individuals are often active in the workforce, highlighting the socioeconomic burden of the disease. 22 The high incidence of surgical interventions within the cohort confirms the invasiveness usually required in endometriosis management.23–25 Hormonal treatments, widely adopted by our study group, emphasize the continuous struggle against the symptomatology of this chronic ailment.7,26,27 The clinical manifestation of endometriosis remained severe throughout the pandemic, with dysmenorrhea, chronic pelvic pain, and dyspareunia remaining prevalently unabated, corroborating the disease’s characteristically intense pain profile.5,28,29 Remarkably, the data revealed significant gastrointestinal disruptions, as a high percentage of participants reported changes in bowel habits. This finding aligns with the literature, suggesting that lifestyle alterations during the pandemic can potentially disrupt the brain-gut axis, compounding the gastrointestinal symptoms associated with endometriosis.30,31
Notably, a quarter of our participants reported an escalation in pain severity, highlighting the worsening of symptoms due to pandemic-related stress and healthcare disruptions. Women reporting increased pain during the pandemic were more likely to rate their general health as poor, highlighting the need for healthcare providers to prioritize pain management as part of a comprehensive care strategy.
This increase in pain severity aligns with contemporary studies that highlight the difficulty in accessing hormonal treatments during the lockdowns.32,33 Patients, already burdened by high-stress levels, faced worsening pain when faced with barriers to securing necessary therapies. For instance, Demetriou et al.’s study across a European cohort of 6,729 individuals with endometriosis found that 20.3% reported difficulties in obtaining repeat prescriptions, 10.5% had to change their hormone and painkiller regimes due to availability issues, and a significant 9.5% were compelled to discontinue their medications entirely. 34 Such disruptions likely contributed to the deteriorating pain management and increased stress levels reported by our study participants.
Similarly, a study conducted by Arena et al. within the same period on a sample of 468 Italian women with endometriosis corroborated these findings, revealing significant obstacles in accessing hormonal therapies during lockdowns. The study participants reported heightened levels of stress and a worsening of pain, particularly for those who faced challenges in obtaining their usual treatments. 35 Furthermore, the difficulty in accessing medical support, as reported by a substantial number of participants, alongside feelings of medical abandonment, likely contributed to the intensification of symptoms, including increased pain. These observations are consistent with findings from various international studies, which have collectively pointed to widespread challenges in medical service accessibility during the pandemic.10,32–36
Our K-means clustering analysis adds a deeper understanding of this variability, revealing two distinct patient subgroups that experienced the pandemic differently. The first cluster comprised individuals who reported better overall outcomes, including fewer increases in pain severity, lower psychological distress, and a more stable quality of life. This group demonstrated greater resilience and adaptability during the pandemic, potentially benefiting from less disrupted access to healthcare or greater use of available resources such as telemedicine. Conversely, the second cluster consisted of patients who experienced significantly poorer outcomes. This subgroup reported markedly higher pain severity, greater difficulty accessing hormonal therapies, and elevated anxiety and depression. Feelings of medical abandonment were particularly prevalent in this group, reflecting how systemic healthcare disruptions disproportionately impacted their ability to manage their condition.
The clustering analysis highlights a clear pattern: while some patients were able to maintain continuity of care and mitigate the worst impacts of the pandemic, others faced a compounding burden of physical, psychological, and systemic challenges. For individuals in the second cluster, the lack of access to timely hormonal treatments and difficulties navigating disrupted healthcare pathways likely created a feedback loop, intensifying both physical symptoms and mental health struggles. The clustering insights emphasize the variability within the patient population, underscoring the importance of targeted approaches to address these inequities.
Telehealth emerged as a crucial intermediary for many patients, especially for straightforward needs such as prescriptions. However, it was not without its deficiencies—reported shortcomings include the absence of thorough physical examinations. 33 Notably, while telehealth has generally met with patient approval during the pandemic, healthcare professionals have voiced more substantial criticisms.33,37 This dichotomy between patient satisfaction and professional concern suggests that while telehealth has brought some gaps during healthcare crises, it cannot wholly substitute for in-person care, particularly for conditions like endometriosis that often require comprehensive physical assessments.
The reported data indicates that 6.7% of our study's participants were engaged in pursuing conception, which, during the pandemic, was particularly significant given the added difficulties in accessing reproductive healthcare services. 10 The pandemic has likely exacerbated the already lengthy process of attempting to conceive a child.38,39 This prolonged duration, combined with the stress and healthcare strain of the pandemic, may significantly impact mental health and the sense of well-being in these individuals.
The use of assisted reproduction techniques by 5.8% of the participants might have encountered additional difficulties throughout the pandemic. Procedures such as IUI, IVF, and ICSI require regular visits to healthcare facilities, monitoring, and sometimes complicated regimens that could have been disrupted or delayed due to healthcare prioritization and restrictions.10,40–42 Furthermore, the concern levels about planning pregnancy, with a mean score of 3.45 on a scale of 10, suggest that while the desire for pregnancy remains, the uncertainty and stress related to the pandemic have had a considerable psychological impact. These concerns are likely amplified in the context of endometriosis, where the chances of conception are already affected. 43
The multifaceted concerns encapsulated by our data—encompassing family health, economic implications of the pandemic, and individual health—portray a community struggling with fears extending beyond their immediate health challenges.
Economic and personal worries were notable predictors of anxiety related to endometriosis, signaling the far-reaching impact of the pandemic's socio-economic consequences on patient health perceptions and management of the disease.44,45 This reality mandates a healthcare response that transcends clinical treatments to consider the broader socio-economic adversities faced by patients.
The pervasiveness of endometriosis extends beyond the physical, permeating the psychological realm and impacting the QoL profoundly. It affects various aspects of daily living, including work, intimate relationships, and overall family dynamics. This multi-dimensional impact of endometriosis on health-related QoL is well-documented, with a substantial body of literature linking the condition to heightened risks of depression and anxiety.6,46
For the SF12 PCS, the average score within our cohort was 41.4 (SD = 11.1), significantly lower compared to the normative Italian average of 53.4 reported by Facchin et al. 47 However, this did not differ substantially from the pre-pandemic clinical sample average of 41.5 by Vannuccini et al. [48]. The SF12 MCS revealed an average score of 39.3 (SD = 11.2), which was below the normative average of 43.4 by Facchin et al. 47 , aligning with the pre-pandemic clinical sample's average of 37.2 by Vannuccini et al. 48 This congruence with pre-pandemic data underscores the persistent challenges faced by those with endometriosis, suggesting that the core impact of the condition on QoL remains stable, even amid the additional pressures introduced by the COVID-19 pandemic.
However, a notable increase in psychological distress, as measured by the HADS, which surpassed both the normative means and the clinical averages observed before the pandemic, signals a potential intensification of mental health challenges within this already at-risk group due to pandemic-related stressors.
The HADS mean score of 10.5, were significantly above the normative mean of 6.49 by Facchin et al. 47 , and also showed a significant increase from the pre-pandemic clinical sample of 7.5. 49 Depression levels followed a similar pattern, with an average score of 9.4 (SD = 3.5) exceeding the normative mean of 4.71 47 and the pre-pandemic clinical sample of 6.1. 49
This observation is further supported by the rise in mental health concerns across the general population during the pandemic,50,51 with our findings indicating a more pronounced effect among individuals with pre-existing conditions such as endometriosis.
In exploring sleep quality through the PSQI, our findings parallel those in the broader literature, which links poor sleep with chronic pain conditions, 52 In our study Global PSQI Score stood at 7.8 (SD = 4.4), reflecting the cohort's overall sleep quality concerns. However, a more targeted analysis disclosed that two-thirds of the women (66.7%) had PSQI scores exceeding the threshold of 5, which denotes substantial sleep difficulties. This specific proportion of affected individuals aligns with the prevalence rates reported by Leone Roberti Maggiore et al. confirming that the substantial sleep disturbances observed are consistent with those experienced by patients with endometriosis before the pandemic. 53
The elevated Global PSQI Score within our cohort is a mirror to this relationship, suggesting that the interplay of pain and psychological distress likely contributes to a detrimental cycle that undermines the quality of sleep and, by extension, the overall QoL.
The EHP-5 score yielded a mean of 49.2 (SD = 19.5), aligning closely with the results from a Spanish clinical sample pre-pandemic by Aubry et al. of 48.1, indicating no significant statistical variance. 54 This suggests that the impact of endometriosis on quality of life is sustained, crossing geographic and temporal divides.
Correlational analyses via Spearman's Rho coefficient further articulate the interconnectedness of physical and mental health with QoL and sleep. Notably, a strong negative correlation between MCS12 and HADS depression scores suggests that as mental health deteriorates, depressive symptoms intensify.
Moreover, the identified negative correlations between QoL metrics and psychological distress suggest a bidirectional relationship, where enhancements in mental health could lead to improvements in life quality and vice versa. This finding illuminates a significant oversight in the comprehensive treatment of endometriosis—psychological care is crucial yet frequently sidelined. Addressing this gap could not only improve mental health outcomes but also enhance the overall QoL for those affected by endometriosis, as previously demonstrated in the literature.45,55
Our study, while robust in its findings, is not without limitations. The reliance on self-reported measures might introduce a bias toward subjective interpretations of symptoms and experiences.
The severity of endometriosis was not assessed in this study. Nevertheless, it is well established that the severity of endometriosis does not always correlate with the severity of symptoms experienced. In our survey, patients did not prioritize providing an elaborate medical description and assessment of their condition but rather describing their subjective feelings and experiences associated with endometriosis. This approach enabled us to concentrate on their perceived well-being, which was the primary focus of our study. Moreover, the study's methodology, which involved comparing current patient experiences against pre-pandemic groups and control groups from previous studies, might not fully capture the direct effects of the pandemic, potentially affecting the generalizability of the findings. Although this study provides valuable insights into the immediate effects of healthcare disruptions during the COVID-19 pandemic, the longer-term impact on endometriosis outcomes remains unclear. Longitudinal studies are needed to explore how delays in treatment affect disease progression, quality of life, and mental health over time.
On the other hand, this research’s strengths include the comprehensive dataset reflecting a wide array of experiences and the use of K-means clustering to elucidate the varying impacts of the pandemic on our cohort. This approach has provided a nuanced understanding of patient experiences and identified a subgroup requiring more intensive support.
Conclusion
The COVID-19 pandemic has laid bare the vulnerabilities in chronic disease management, particularly for those with endometriosis, amplifying existing symptoms and inflicting additional psychosocial and healthcare access challenges. Our findings underscore the intricate interplay between endometriosis's physical and psychosocial dimensions, exacerbated under the unique strains of a global health crisis. The persistence of these challenges, despite the pandemic, indicates the chronicity of endometriosis-related distress and highlights the disease's enduring impact on patients' lives. These findings support a more integrated care approach that addresses both the psychosocial and physical aspects of endometriosis. Healthcare systems must recognize and bridge the gaps in service provision, especially in times of crisis, to prevent symptoms from worsening and improve the overall QoL for those living with this challenging condition.
Supplemental Material
sj-pdf-1-pev-10.1177_22840265251314992 – Supplemental material for Impact of the COVID-19 pandemic on patients affected by endometriosis: A questionnaire-based cross-sectional online survey
Supplemental material, sj-pdf-1-pev-10.1177_22840265251314992 for Impact of the COVID-19 pandemic on patients affected by endometriosis: A questionnaire-based cross-sectional online survey by Stefania Saponara, Michal Ciebiera, Salvatore Giovanni Vitale, Mirian Agus, Andrea Piselli, Maurizio Nicola D’Alterio, Stepan Feduniw and Stefano Angioni in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Data availability statement
Research data is available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.