
Abstract
Objective:
To assess the effect of Dienogest versus surgical management of endometriomas on ovarian reserve.
Methods:
This randomized clinical trial was conducted at Suez Canal university hospital from November 1st, 2020, to July 31st, 2022. We recruited patients with endometriomas according to particular inclusion and exclusion criteria. The study population was allocated into two groups: group one received Dienogest, and group two had laparoscopic cystectomy. Eligible patients were subjected to history and examination to evaluate pelvic pain using the Biberoglu and Behrman score and the visual analogue scale. Ultrasound examination was done to diagnose ovarian endometrioma and its diameter. Ovarian reserve was evaluated by the antral follicle count and serum anti-mullerian hormone. After 3 months, patients were reevaluated regarding cyst diameter, antral follicle count, pain scores, and the anti-mullerian hormone. The primary outcome measure was to evaluate the ovarian reserve before and after intervention in both groups.
Results:
The antral follicle count and anti-mullerian hormone increased significantly after Dienogest therapy and decreased significantly after surgical excision (p < 0.001). Only induration was significantly decreased in the medical treatment group (p < 0.001). Both management options resulted in a noticeable reduction in the visual analogue scale scores in each group individually.
Conclusion:
Dienogest rescued ovarian reserve in women with endometriomas.
Introduction
Endometriosis, a multifactorial disorder 1 affecting women of reproductive age, causes female infertility and pelvic pain. Involvement of the ovary results in the development of endometriomas in 17%–44% of patients. 2 Endometriomas, a chronic inflammatory condition, warrant treatment according to patients’ complaints. This might be surgical intervention, medical treatment, in-vitro fertilization (IVF) in infertile women, and even conservative management when asymptomatic.3,4 Although proved effective, these modalities do not result in a long-term cure rate, with a recurrence rate of 36%–57% in 5 years.5,6 Surgery has been advocated for pain, large-size endometriomas, or failed medical treatment. However, its effect on the ovarian reserve is questioned. 7 Surgical removal resulted in removal of the healthy ovarian tissue with subsequent decreased follicular growth and decreased response to gonadotropins.8,9
Additionally, the presence of endometriomas affects the ovarian reserve, which is a challenge when deciding conservative management. 10 This is due to the growing endometrioma compresses the normal ovarian tissue. 11 However, the effect of medical treatment was not appropriately investigated. 12 The medical treatment provides lower remission rates, especially after surgery, but its effect on pregnancy is not evaluated. 6 The desired medication should be effective in reducing pain, avoiding hypoestrogenism, and with few side effects, as it would be administered for a long time. 13 Dienogest, a fourth-generation progestogen, has many properties, such as having a high affinity to progesterone receptors and a lack of androgenic effects, making it a drug of choice for patients with endometriosis. 14 This study aimed to evaluate the effect of Dienogest treatment versus cystectomy of endometriomas on ovarian reserve.
Materials and methods
This open label randomized clinical trial was conducted at the obstetrics and gynecology department at Suez Canal university hospital. The trial commenced from November 1st, 2020, to July 31st, 2022, after approval of the research ethics committee. We recruited patients according to specific inclusion and exclusion criteria. Inclusion criteria: (a) unilateral endometrioma, (b) size of 3–8 cm, (c) age 18–45 years, (d) regular cycles, and (e) no previous ovarian operations in the last 3 months. Exclusion criteria: (a) suspected or confirmed malignancy, (b) women within 2 years of menarche, (c) women on progesterone or combined hormonal contraception, (d) menopause, (e) suspected pregnancy, and (f) incidental finding of endometrioma in the contralateral ovary during laparoscopy.
After a detailed explanation of the study procedure, informed consent was obtained from all eligible patients accepting participation in the study. The study population was randomly allocated into two groups using random generation of numbers through computer software in a 1:1 manner. Group one received Dienogest, and group two had laparoscopic cystectomy. Randomization was done after evaluating the participants for eligibility.
Eligible patients were subjected to the following:
1- Complete personal and medical history.
2- Complete physical examination and local examination to evaluate pelvic pain. The pain was assessed using the Visual Analog Scale (VAS) and the Biberoglu and Behrman Score (B&B). The VAS is a unidirectional measure of the intensity of pain. It is composed of a horizontal scale, 10 cm in length. It is anchored by two verbal pain extremes. An extreme was represented by “no pain” (scored as 0), and the other extreme was represented by “the worst pain ever” (scored as 10). The patients were told to place a mark on the scale that represents the extent of pain they suffered. The score was determined by measuring the distance between the “no pain” extreme and the mark determined by the patient. This gave a range of scores from 0 to 100. A higher score indicated severe pain. 15 The B&B score is divided into two parts: pelvic symptoms score (includes dysmenorrhea, pelvic pain, and dyspareunia) and physical symptoms score (includes tenderness and induration). Each symptom is marked as absent, mild, moderate, or severe and scored from 0 to 3, respectively. The final score combines the scores of both parts, giving a total score of 0–15. A score of 0 indicates the absence of symptoms, 1–2 indicates mild symptoms, 3–5 indicates moderate symptoms, 6–10 indicates severe symptoms, and 11–15 indicates very severe symptoms. 16
3- Ultrasound examination, either transabdominal for virgins or transvaginal for sexually active women, to diagnose ovarian endometrioma. This was done after demonstrating a unilocular cystic lesion with a ground glass echogenicity of the fluid and a regular thick wall. 17 The antral follicle count (AFC) was evaluated on days 2–3 of the cycle by determining the number of follicles measuring 2–10 mm. 18 For the study, the AFC was measured separately for the two ovaries, and that of the affected ovary was considered in pre- and post-evaluation.
4- Laboratory evaluation was done. The complete blood count, coagulation profile, and liver function test were withdrawn for group 2 patients. Anti-mullerian hormone (AMH) was withdrawn for the whole study population.
5- Group one patients received medical treatment with Dienogest (Visanne VR, Bayer AG, Soficopharm; 2 mg/day) starting on the first day of the first menstrual cycle for 3 months.
6- Group two patients had laparoscopic ovarian cystectomy.
7- After 3 months, patients were subjected to clinical evaluation, including cyst diameter and AFC using ultrasound and measurement of AMH.
The primary outcome measure was to evaluate the ovarian reserve before and after intervention in both groups. The secondary outcome measure was the degree of pain in both groups before and after intervention and the side effects of Dienogest therapy.
The sample size was calculated at a significance level of 95%and an error level of 20% using a difference in mean change of AMH in the Dienogest group (10.1 ± 3.1; 12) and the mean change in AMH after laparoscopic cystectomy (11 ± 6; 19). 19 The estimate of pooled standard deviation was 2.5. A drop out of 12% was added. So, the sample was 60 patients per group.
Statistical analysis
Data were statistically described as mean and standard deviation, frequencies (number of cases), and percentages when appropriate. p Values of less than 0.05 were considered statistically significant. All statistical calculations were done using the computer program SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA), release 23 for Microsoft Windows. The Chi-square test was used for categorical variables, and the (t) test for continuous variables with normally distributed data. Non-normally distributed data were tested using Fisher's exact for categorical variables and Mann-Whitney U tests for continuous variables.
Results
About 125 women were eligible for the study, 3 declined to participate, and 2 refused medical treatment, leaving 120 women divided into two groups for the final analysis (Figure 1).
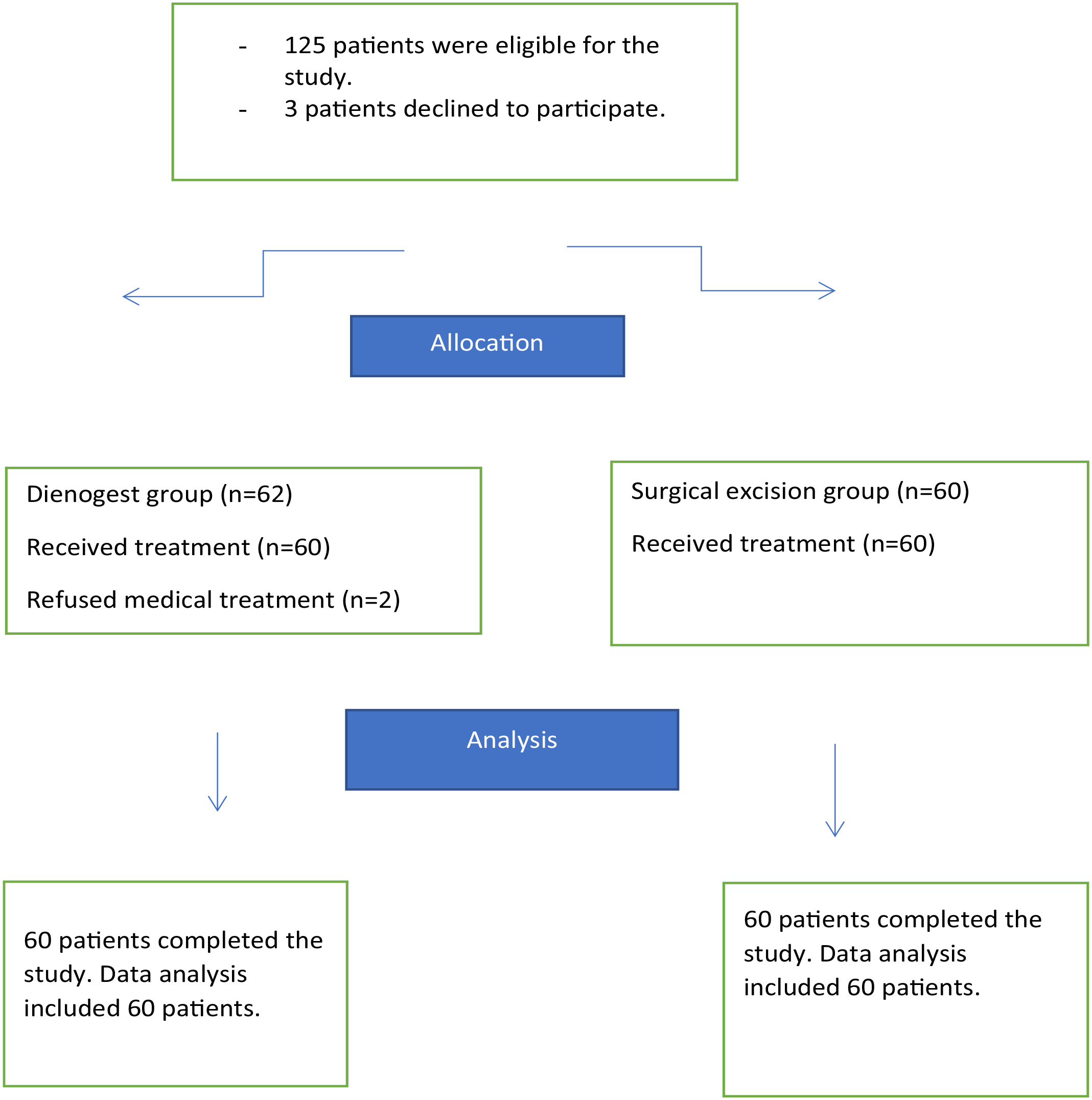
Patients’ flow chart.
There was no difference in the primary demographic data of the studied population, as demonstrated in Table 1.
Basic demographic data of the studied population.
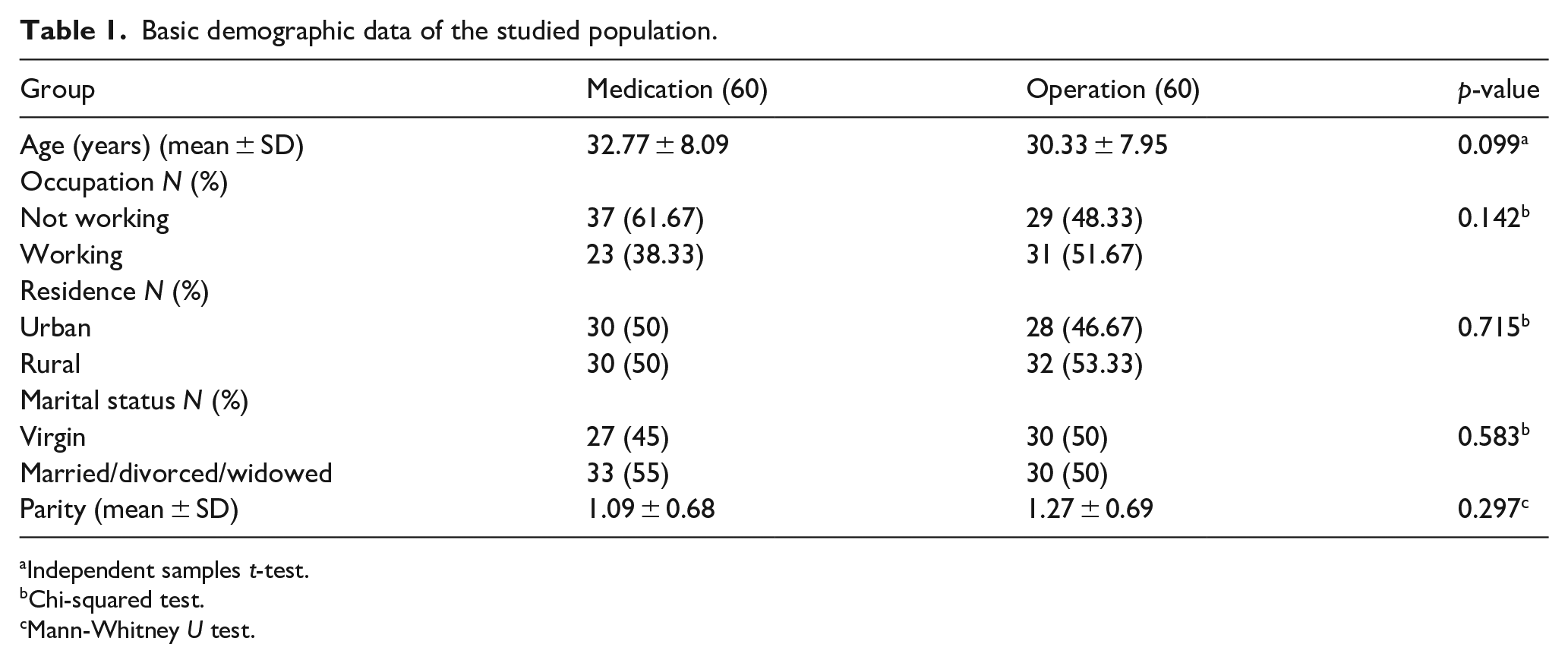
Independent samples t-test.
Chi-squared test.
Mann-Whitney U test.
There was a significant decrease in cyst diameter with both modalities of treatment. There was no difference in the AMH level before allocation. After the intervention, a significant difference was noted (p < 0.001). Additionally, a significant increase and decrease in the AMH were noted in the Dienogest group and after laparoscopic cystectomy, respectively (p < 0.001). Also, the same difference was noted regarding the AFC in both groups (Table 2).
Comparison of the ovarian reserve before and after intervention.
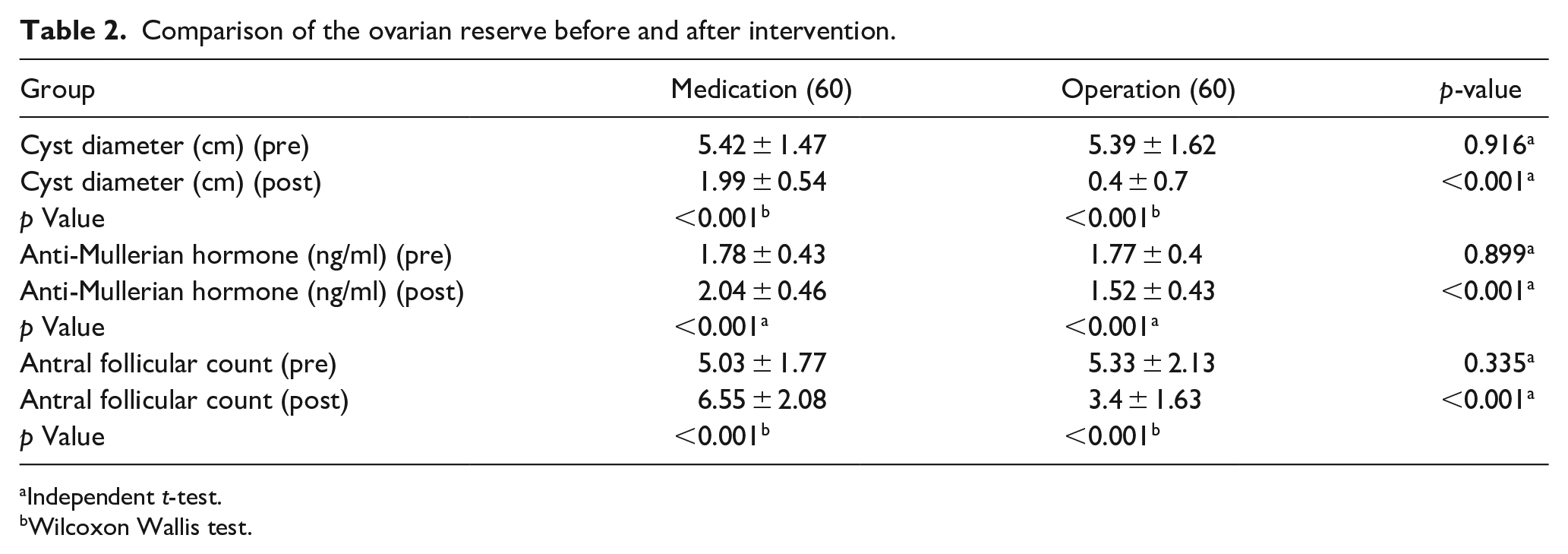
Independent t-test.
Wilcoxon Wallis test.
There was no difference in the pain scores used on the B&B scale before and after intervention in both groups but for induration which was significantly decreased in the medical treatment group (p < 0.001). However, both treatment modalities significantly reduced the VAS scores in each group individually (Table 3).
Comparison of pain scores before and after intervention.
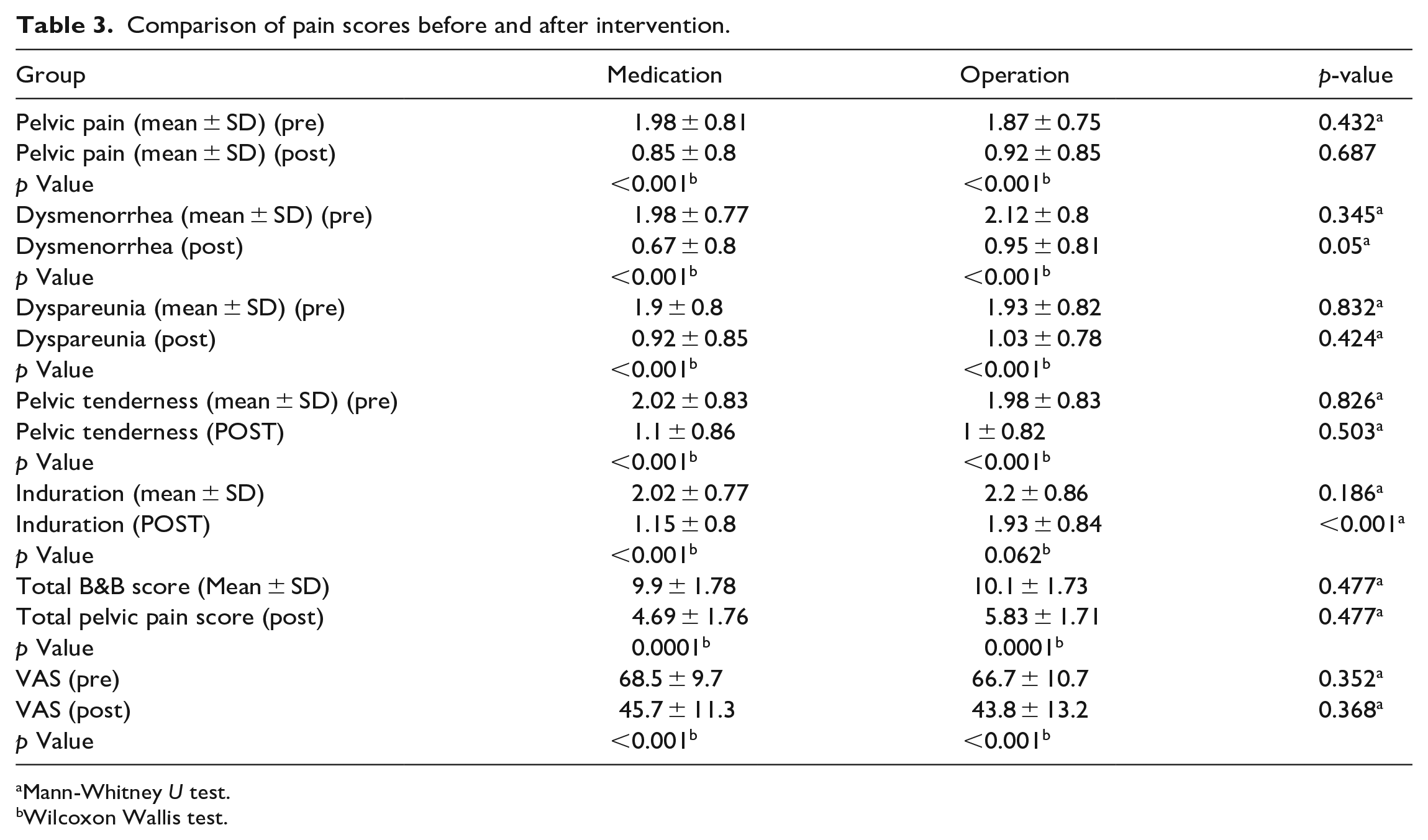
Mann-Whitney U test.
Wilcoxon Wallis test.
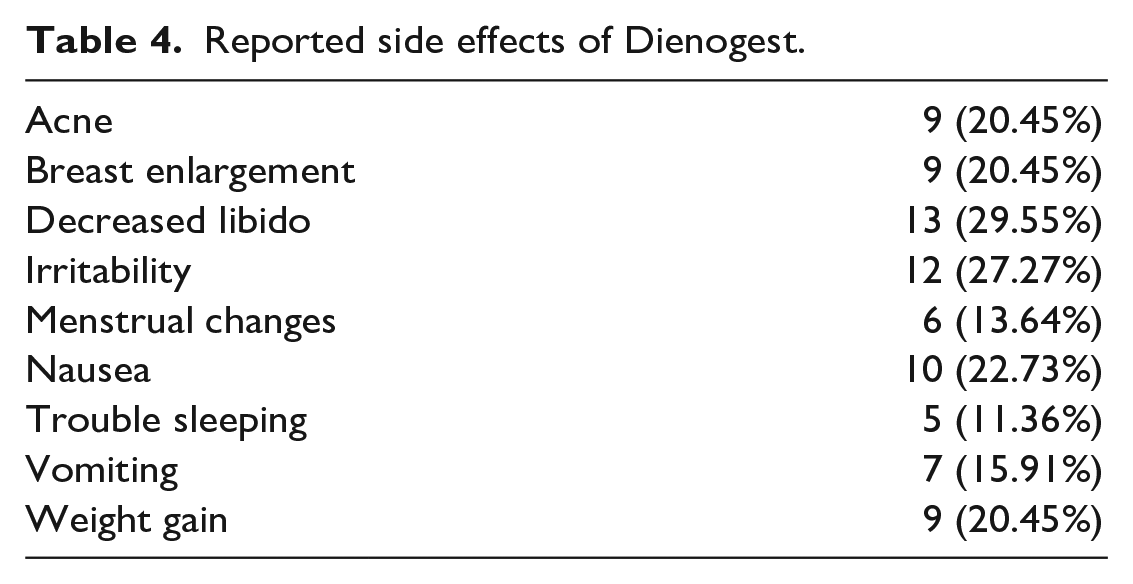
Dienogest was associated with some side effects as reported by the users; however, it was tolerable, and treatment was not interrupted. These included decreased libido, irritability, and nausea at the highest frequencies (29.55%, 27.27%, and 22.73%, respectively; Table 4).
Reported side effects of Dienogest.
Discussion
This study recruited women with unilateral endometriomas. The effect of medical treatment (Dienogest) and laparoscopic cystectomy on the ovarian reserve and pain scores was assessed. The studied population was in the childbearing age (mean age 32.77 ± 8.09 and 30.33 ± 7.95 for the medication and operation groups, respectively). This was noted in the recruited population in an earlier study. 12 It has been reported that endometriosis affected women of reproductive age with a mean age ranging from 25 to 29 years. It also may affect adolescents especially in those with mullerian anomalies. 20
There was a significant decrease in the cyst diameter with Dienogest treatment. Another study reported similar results where the diameter declined from 4.0 ± 1.3 to 2.4 ± 1.2 cm after 6 months, 12 while we continued the follow-up for 3 months only. Another one reported a reduction of 70% in cyst diameter after 3 months. 21 An additional one reported a 27% decline in size after 6 months of treatment. 22 Decreased diameter would be explained by the effects of Dienogest on endometriosis. It has a suppressive effect on proliferating stromal cells and live epithelial cells. 23 Another study reported increased autophagy and apoptosis with Dienogest therapy. 24
The AFC and AMH increased significantly after Dienogest and decreased significantly after laparoscopic cystectomy. This agreed with previous results where the AFC increased significantly in the affected ovary from 4.2 ± 2.8 at recruitment to 8.6 ± 4.2 after 6 months; however, they reported no change in AMH levels. 12 Another study reported no change in AMH levels after medical treatment, however they recruited patients using Dienogest and leuprorelin without proper discrimination of individual treatment effect. 25 Increased AMH levels after medical treatment might be explained by the decrease in inflammatory markers and toxic substances as the size of endometrioma decreases. 26 There is no proper information about the effect of medical treatment of endometrioma on ovarian reserve markers. 12
Another study reported contradicting results, as the AFC did not differ before and after surgery. 27 Additionally, the AFC could be underestimated in patients with endometriomas, as evidenced by the retrieval of increased numbers of oocytes during ART cycles than expected. 28 Underestimation of the AFC would be rendered to the impaired resolution of the transvaginal probe due to the long length to reach the cyst capsule. Also, waves with higher frequency lead to more significant attenuation and failure to detect small follicles. 29 After endometrioma removal, pelvic anatomy is restored with improved imaging quality allowing accurate detection of AFC. 28
Surgical management has been reported to result in a 34% decrease in AMH levels. 7 An earlier study reported on ovarian reserve after ovarian cystectomy, regardless of the nature of the cyst, confirmed a significant reduction in the AMH levels, with a significant reduction in endometriomas and follicular cysts. However, measurement of AMH was done before surgery and 2 weeks after. 30 This would be attributed to the removal of ovarian tissue during surgical excision, which increases as the cyst diameter increase. 31 Even with smaller cysts, follicles were lost. 32 Antral follicle count represents the large antral follicle pool, while the AMH is produced by preantral follicles, emphasizing the beneficial effect of medical treatment on the ovarian reserve. 33
Only induration differed significantly between both groups, with a significant reduction noted after Dienogest therapy. This confirmed previous results where Dienogest effectively reduced endometrial nodules.34,35 The VAS score decreased significantly after medical treatment and after the operation as well. This was reported previously after Dienogest treatment.12,21,22 Even when combined with Ethinyl estradiol, a significant reduction in pain score was noted. 36 The decline in the inflammatory markers -interleukin-1 beta (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), tumor necrosis factor-alpha (TNF-α), and monocyte chemotactic protein-1 (MCP-1)—in the peritoneal fluid after Dienogest therapy, would explain this improvement. 37
The most common reported unwanted effects of Dienogest included decreased libido, irritability, and nausea. Menstrual changes occurred in 13.6% of patients. These effects were tolerable, and treatment was not interrupted. This agreed with previous results as Dienogest resulted in continuous bleeding without discontinuation of treatment. 37 Another reported menstrual change in 16.6% of cases besides weight gain, decreased libido, weight gain, headaches, and depression urged 10% of users to discontinue treatment. 38
Strength and limitations
The sample size is a limitation. Follow-up was conducted for 3 months only. A prolonged follow-up would be more informative. The comparison was performed between medical and surgical interventions. An expert gynecologist performed all surgeries to avoid damage to ovarian tissue by inexpert surgeons. We used AFC to estimate the ovarian reserve, which the endometrioma might compress. This would result in inadequate evaluation. However, we used AMH levels in addition to getting accurate results.
Conclusion
Surgical removal of the endometriomas resulted in a significant reduction in ovarian reserve markers. Dienogest represented a safe and effective management option for women with endometriomas.
Footnotes
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Trial registration number
PACTR202010622528145.
Date of registration
15/10/2020.