
Abstract
Umbilical endometriosis, although relatively rare, has been described with plenty of case reports and case series available in the literature. Surgical excision has been the preferred mode of treatment, with or without excision of the umbilicus. Few cases described laparoscopically assisted excision but lacked descriptions of a safe alternative non-umbilical laparoscopy entry portal, management of possible concomitant intraperitoneal lesions, and aesthetic umbilicus repair. The aim of this work is to describe a modified technique of laparoscopically assisted excision of umbilical endometriosis and treat concomitant intraperitoneal lesions via a new laparoscopic entry portal with aesthetic preservation of the umbilicus. Successful complete excision of the mass with aesthetic preservation of the umbilicus followed by 3 months of Dienogest therapy resulted in complete resolution of the mass. It is concluded that utilizing “Darwish point” for abdominal access to excise umbilical endometriosis and treat concomitant intraabdominal lesions, offers smart abdominal access with aesthetic umbilicus repair. Moreover, postoperative hormonal treatment (Dienogest) is helpful to ensure a better cure.
Introduction
Endometriosis is an enigmatic disease in all aspects. Extra genital endometriosis is rare if compared with genital endometriosis. Umbilical endometriosis (UE) is a rare subtype of extra genital endometriosis comprising 0.5–1% of all extra pelvic disease. 1 UE, although relatively rare, has been described with plenty of case reports and case series available in the literature. 2 Surgical excision has been the preferred mode of treatment, with or without excision of the umbilicus. Few cases described laparoscopically assisted excision3,4 but lacked descriptions of a safe alternative non-umbilical laparoscopy entry portal, management of possible concomitant intraperitoneal lesions, and aesthetic umbilicus repair. The aim of this work is to describe a modified technique of laparoscopically assisted excision of umbilical endometriosis and treat concomitant intraperitoneal lesions via a new laparoscopic entry portal (Darwish point) with aesthetic preservation of the umbilicus.
Case presentation
A 39-year-old patient delivered by caesarean section twice and currently is not using contraception presented to the out-patient department (OPD) with a complaint of severe, progressive, and crescendo central abdominal pain exacerbated on a touch of the umbilicus and exaggerated before and during menstruation. Characteristically, some blood-tinged discharge came out from her umbilicus during pain attacks. In between pain attacks, she felt a hard mass in the umbilicus which dated for years before starting to have pain. She gave no history of dysmenorrhea, menstrual abnormalities, or dyspareunia. She gave a history of laparoscopic insertion of a gastric band that causes continuous upper abdominal pain and repeated vomiting for some time which obliged bariatric surgeons to remove it due to infection. Thereafter, another gastric band was inserted for her with a smooth postoperative course. After that, she was subjected to laparoscopic cholecystectomy and some orthopedic operations. On inspection of the abdomen, there were many abdominal scars in the upper abdomen (epigastric, supra-umbilical, and left lumbar regions). On palpation, there was a definite fleshy mass underneath the umbilicus about 5 × 5 cm with restricted mobility and mild tenderness. Vaginally the uterus was bulky without evidence of adnexal masses or tenderness. There was no nodularity in the posterior fornix. On trans-abdominal ultrasonography, this mass appeared echogenic with hazy borders (Figure 1). Transvaginal ultrasonography revealed no significant gynecologic findings. MRI with contrast was ordered that revealed an anterior abdominal wall mass lesion at the region of umbilicus, measuring 5 × 2.5 cm in dimensions, appearing hypointense on Tl and T2 sequences, mild heterogeneous enhancement on post-contrast sequence, signal intensities suggesting blood in chronic phase, radiological picture suggesting endometrioma (Figure 2(a) and (b)). The patient was counseled on the surgical approach. She signed a consent to perform surgical intervention but persistently asked to preserve her umbilicus whenever possible. After preoperative preparation, anesthesia consultation, and approval by the insurance company the patient was prepared for the laparoscopic approach. Since the mass was umbilical, an alternative entry point was chosen excluding umbilical, left lumbar and epigastric regions. The right and left hypochondriac regions were also excluded due to many scars on the upper abdomen. The challenge was to select the safest entry site. The selection of the left lumbar region was the best choice “Darwish point.” 5 Veress needle was inserted at the level of the umbilicus (transverse line) meeting a vertical line 2.5 cm medial to anterior superior iliac spine (Figure 3(a)). After the performance of saline test for safety, induction of the pneumoperitoneum was done. Thereafter insertion of a 5 mm trocar and a wide-angle telescope was made. Adhesiolysis of some omental adhesions was followed by cutting the peritoneum and fascia underneath the mass using Ligasure (Figure 3(b)). Laparoscopy excluded any associated pelvic endometriosis. Dissection of the mass continued until it became loosely adherent to the umbilicus (Figure 3(c)). A semilunar infra-umbilical skin incision was made to access the mass that was completely excised using alternating blunt and sharp dissections (Figure 3(d)). Umbilical remodeling comprised closure of the fascia using Proline 0 interrupted sutures, closure of the subcutaneous defect using Vicryl sutures, and skin closure using SC 4/0 Monocryl sutures. The final step was to check hemostasis by laparoscopy. Histopathologic diagnosis revealed endometrial glands and stroma surrounded by fibrofatty tissue with areas showing thick-walled blood vessels with scattered inflammatory cells suggestive of an endometrioma (Figure 4). Postoperative course passed smoothly, and the patient came for a follow-up for wound check and dressing. Clinical and sonographic follow-up revealed complete resolution of the mass. Adjuvant postoperative Dienogest (Visanne®) was prescribed for 3 months. The patient reported no more pain or mass recurrence during the follow-up period of 9 months. She signed another consent to publish her case with complete anonymity.
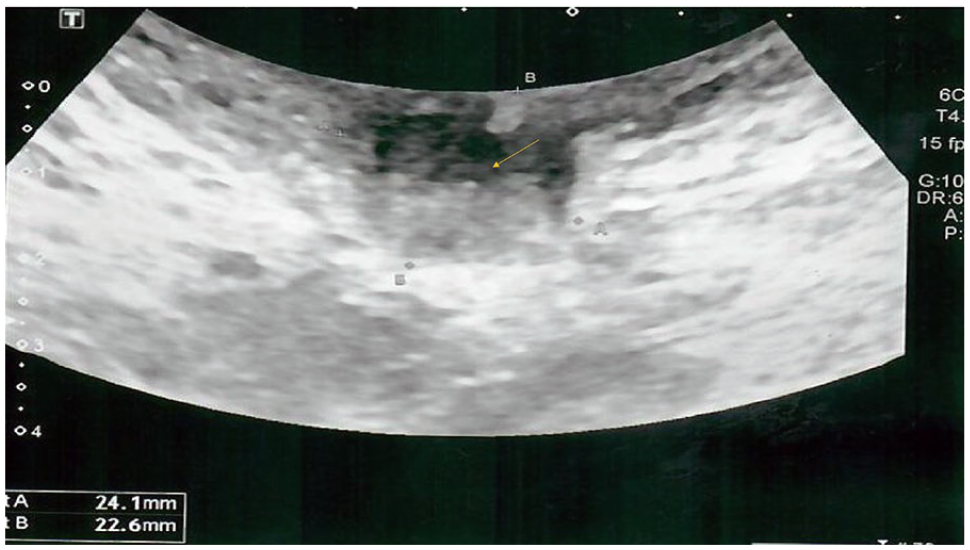
Ultrasonographic appearance of the mass.
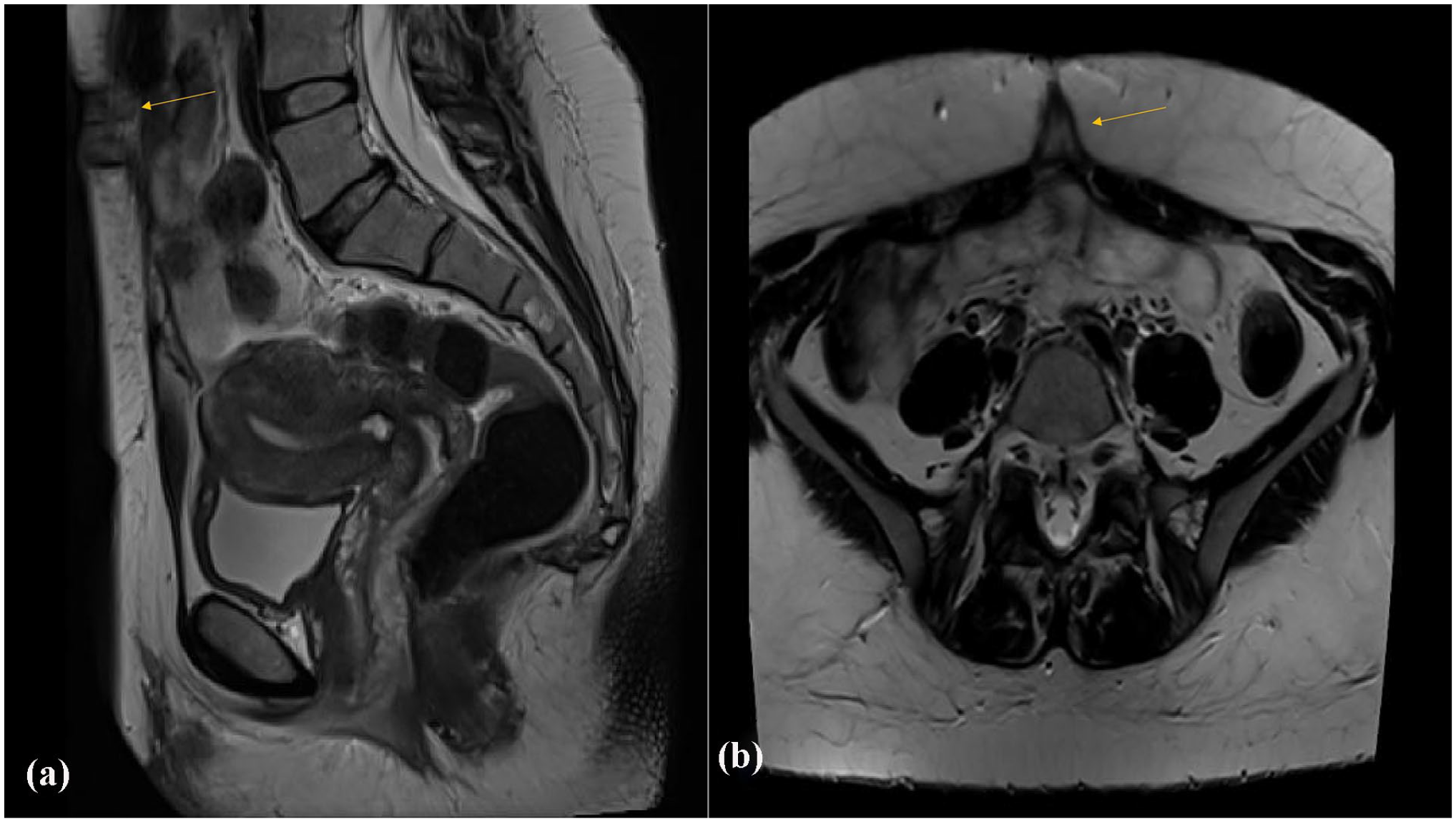
MRI appearance of the mass: (a) longitudinal scan and (b) transverse scan.
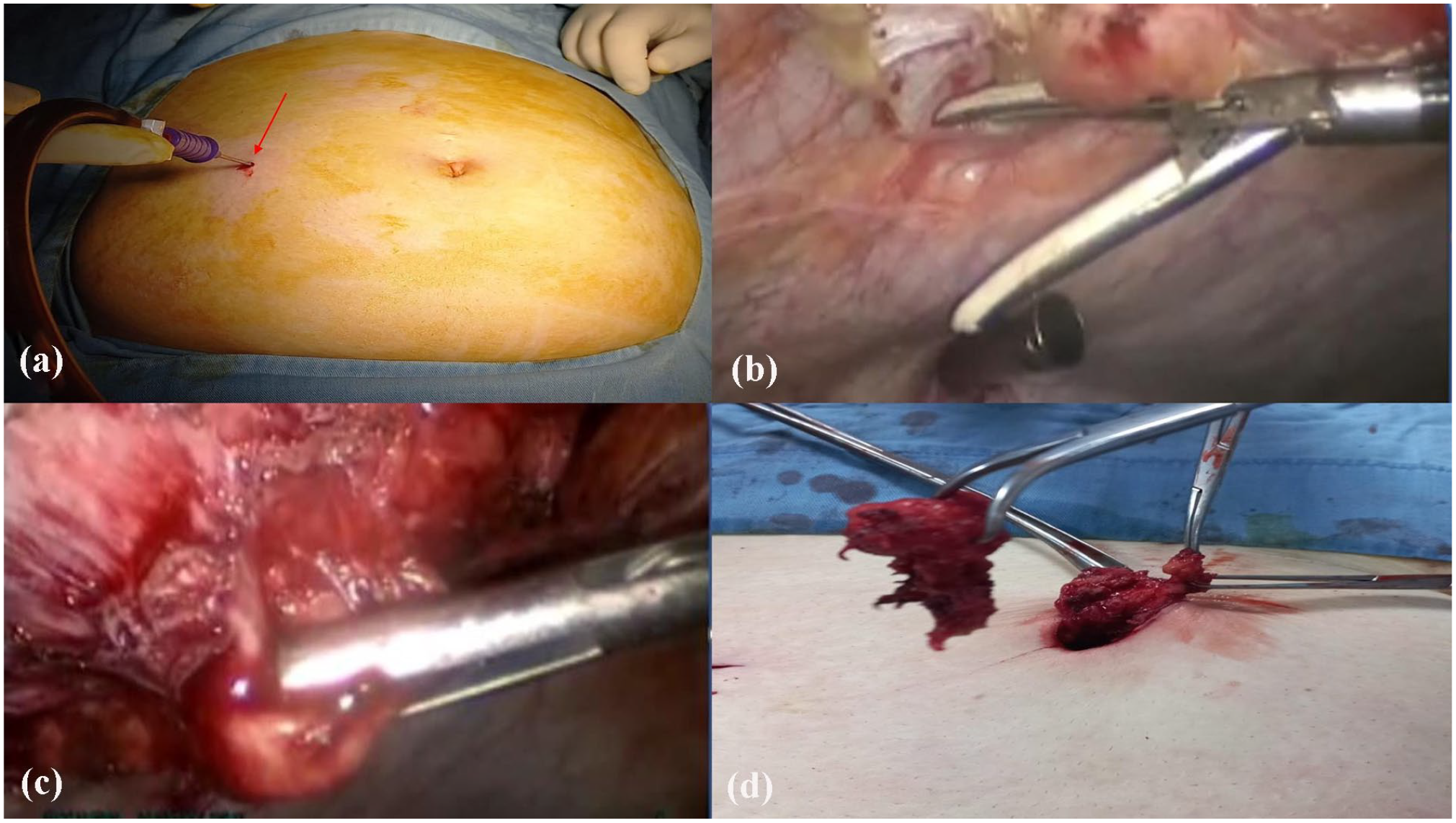
(a) Insertion of Veress needle at the level of the umbilicus, (b) LigaSure dissection of the peritoneum underneath the mass, (c) freeing of the mass after fascial incision, and (d) extraction of the mass via a small periumbilical semilunar incision.
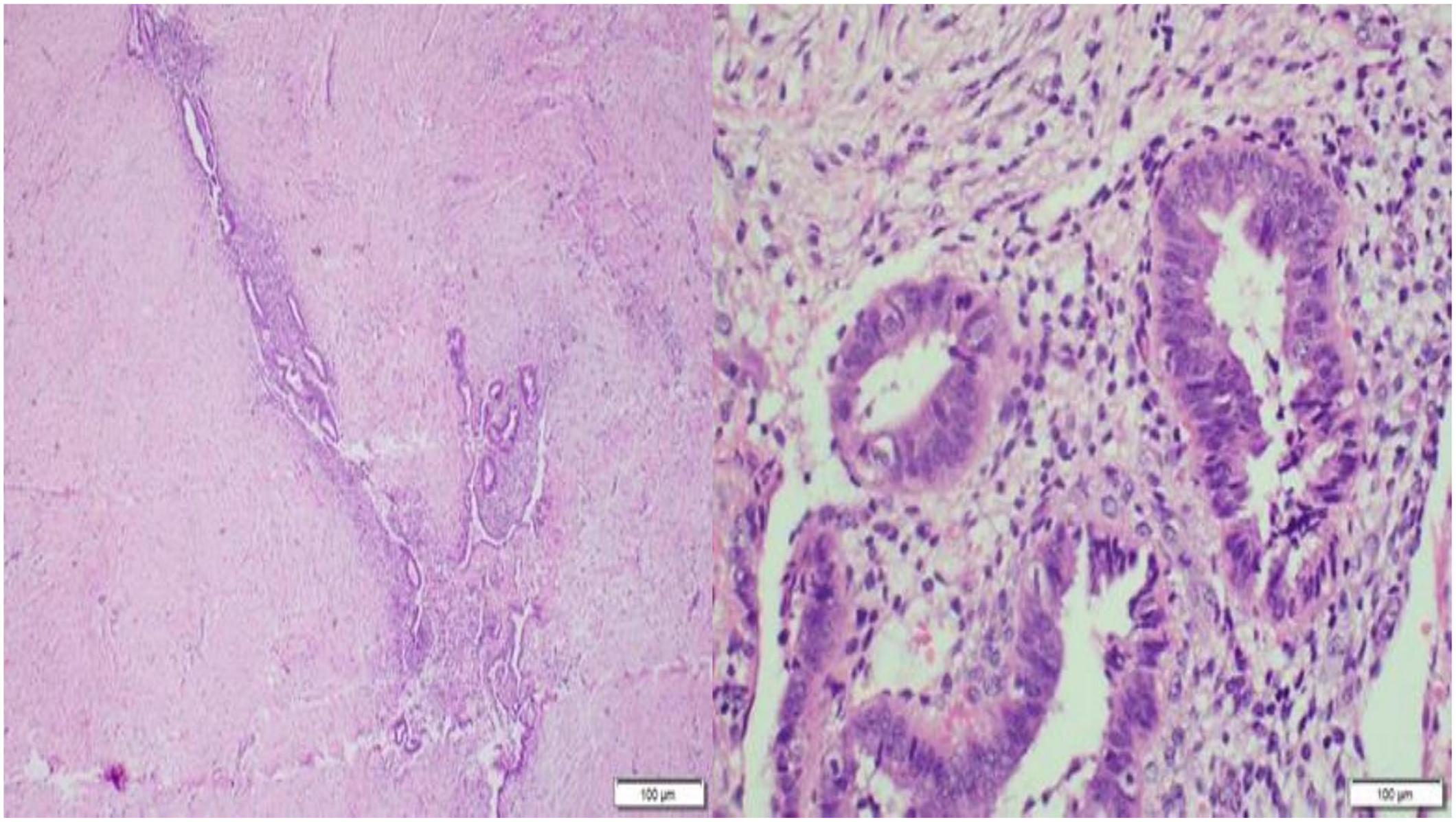
Section revealed endometrial glands and stroma surrounded by fibrous tissue (H&E stain ×20).
Discussion
Skin endometriosis is usually reported at lower abdominal scars following pelvic surgeries. 6 This case report of UE had a history of caesarean section without evidence of pelvic scar endometriosis suggesting a transcoelomic spread of some endometrial tissues as previously postulated. 7 Many of publications on UE described classic open surgery to excise the mass and the umbilicus causing great disfigurement of the female abdomen. 8 If a minimally invasive surgical approach is chosen, the first challenge is how to access peritoneal cavity in a safe way particularly in women with previous operations like this case. In this case report, a new access point “Darwish point” 5 was chosen due to previous operations and the umbilical mass. Selection of right lumbar region access was successful and safe if compared with left sided access points like Palmar 9 or Jain 10 points. Moreover, it was advantageous over risky upper abdominal access points like Latif 11 or Lee-Huang 12 points. Under-vision laparoscopic dissection of the mass using the advantage of vessel sealing character of the bipolar tool of Ligasure was a clear valuable surgical step that released the mass from the peritoneum and the fascia to be easily excision trancutaneously. An additional advantage was conservation of the umbilicus by performing a small semilunar incision around the umbilicus aiming at its preservation. The umbilicus is an important aesthetic item of the abdomen particularly for females. 13 Finally, adjuvant Dienogest (Visanne®) was given for 3 months to ensure complete relief of symptom as we used to prescribe adjuvant therapy for extra genital endometriosis as recently published by our team. 14
Conclusions
It is concluded that utilizing “Darwish point” for abdominal access to excise umbilical endometriosis and treat concomitant intraabdominal lesions, offers smart abdominal access with aesthetic umbilicus repair. Moreover, postoperative hormonal treatment (Dienogest) is helpful to ensure better cure. Despite being a rare disease, UE deserves more research on minimally invasive aesthetic umbilicus-sparing approaches particularly laparoscopically assisted.
Footnotes
Acknowledgements
We thank our patient for agreement to publish her case.
List of abbreviations
UE: umbilical endometriosis.
Authors’ contribution
AD conceptualized the idea, performed the operation, wrote, and reviewed the manuscript. DD reviewed the paper and shared the idea. MF assisted in the operation. HA made histopathologic diagnosis and wrote the section on it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
An additional consent signed by the patient to publish these findings.
Ethical approval
Ethics approval by the medical director and consent to participate by the patient were taken.
Attestation statement
• The subjects in this trial have not concomitantly been involved in other randomized trials (If applicable).
• Data regarding the subject in the study has not been previously published unless specified.
• Data will be made available to the editors of the journal for review or query upon request.
Availability of data and material
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.