
Abstract
In the setting of a global pandemic, it is vastly important now more than ever that patients have agency and control over pain management when living with a debilitating chronic pain disease such as endometriosis. We present a review of the available literature on the most popular and easily accessible complementary pain management therapies for endometriosis including Transcutaneous Electrical Nerve stimulator (TENS) units, diets, Cannabidiol (CBD), turmeric, meditation, yoga, and acupuncture. These are worthwhile recommendations; however, the data for each is limited and more research is needed to further support each of its use.
Introduction
Endometriosis is a disease defined by the presence of endometrial stroma or glands outside of the endometrium of the uterus that manifests as chronic pelvic pain, dysmenorrhea, dyspareunia and infertility. It has been estimated to effect 10% of the female population and accounts for a large number of women with chronic pelvic pain.1,2 The main pathogenesis theory for endometriosis is Sampson’s Theory of retrograde menstruation whereby the endometrial lining that sheds during menstruation refluxes backwards through the fallopian tubes into the abdominal cavity. Cells of the endometrium then depot and implant onto dependent areas of the pelvis where they are most commonly found such as the ovary, rectovaginal space, bladder surface, and pelvic side walls. However, endometriosis has been found in extra-pelvic and extra-abdominal locations and in women with Mullerian agenesis that gives credence to alternative theories such as coelomic metaplasia and stem cell dysfunction. 1
Endometriosis is challenging to diagnose and treat as it is poorly visualized on imaging and there is no known diagnostic laboratory marker. It is a surgical and pathological diagnosis involving biopsy of tissue. Due to its invasiveness it is not uncommon for a woman to experience a delay in diagnosis of 7–11 years.1,2 There is no cure for endometriosis. The standard of care treatment of endometriosis involves a combination of lifestyle modification, hormonal and non-hormonal medications as well as surgical interventions depending on a woman’s fertility desires. Many women will also incorporate opioid pain medications and women with endometriosis have a higher probability of prolonged use compared to the general population. 3
The mechanism of pain in endometriosis is multifactorial and poorly understood. It can be divided into three types of pain (1) nociceptive, (2) inflammatory, and (3) neuropathic. 4 The first occurs in the peripheral nervous system as a transfer of painful stimuli via superficial or visceral thin Aδ and C pain fibers; endometriosis lesions may cause mechanical pain via compression and infiltration of these nerves.4,5 Secondly, endometriosis is regarded as a chronic inflammatory state with elevated levels of inflammatory cytokines and markers in the peritoneal fluid. 4 Lastly, neuropathic pain results from damage to neurons in the periphery as well as processes such as the central sensitization of pain in the central nervous system. Endometriosis also manifests with episodes of waxing pain and accompanying symptoms with variable duration, or “flares” that may be debilitating and require increasing pain medications.
Self-management is an active participation in the management of one’s own chronic condition and has been associated with improved knowledge and self-efficacy in the setting of endometriosis.6,7 Research thus far have shown positive results on endometriosis pain from dietary changes, yoga, and other exercises, heat application and self-reported cannabis use.8,9 Care during a global pandemic is challenging. Patients with endometriosis flares seeking pain relief and improvement in their quality of life may face new obstacles in obtaining healthcare appointments during times of isolation and distancing. 10 It is more important now than ever to provide patients with various modalities of pain control that are easily accessible and safe with the potential of extending its use in the aftermath of the COVID-19 pandemic.
Here, we provide a narrative review of the existing evidence on complementary therapies for patients with endometriosis and pelvic pain. The literature search was conducted on PubMed with search terms of each intervention AND endometriosis; however due to limited results, this was broadened to include pelvic pain for TENS, cannabidiol, and meditation sections. These search terms were “Transcutaneous Electrical Nerve Stimulator AND Endometriosis OR Pelvic Pain,” “Diet AND Endometriosis,” “Cannabidiol AND Endometriosis OR Pelvic Pain,” “Turmeric OR supplements OR curcumin AND Endometriosis,” “Meditation OR Mindfulness OR Yoga AND Endometriosis OR pelvic pain,” and “Acupuncture AND Endometriosis.” We then focused the narrative description on those pertinent to endometriosis specifically. Each author was responsible for a singular topic and the primary author reviewed each article, eliminated duplicate articles, and composed the tables of findings. The tables of result summary will highlight those directly related to endometriosis in bold. A total of 60 unique articles resulted from these search terms and each summarized in the tables of respective sections. Articles were not included if not published in English. There was a total of 14 articles for TENS, 7 for diet, 7 CBD, 5 turmeric, 11 meditation, 6 yoga, and 10 on acupuncture. 30/60 (50%) articles addressed endometriosis specifically with the breakdown as follows: 1/14 TENS, 7/7 diet, 2/7 CBD, 3/5 turmeric, 2/11 meditation, 5/6 yoga, 10/10 acupuncture.
Transcutaneous electrical nerve stimulator (TENS)
TENS units have a wide application from treatment of chronic back pain, chronic abdominal pain, cancer pain, perioperative pain, and labor pain.11–16 They are FDA approved for primary dysmenorrhea. TENS units work by the Gate Control theory whereby stimulation of large diameter, cutaneous, proprioceptic Aβ nerve fibers by the TENS unit inhibits the transmission of pain and other noxious stimuli through the smaller Aδ and C pain fibers.17,18
Advantages of TENS units are that they are controlled by the patient and do not involve a medication or prescription. They are easily accessible, inexpensive, and have minimal risk and contraindications. TENS units are small adhesive devices generally applied to the lower abdominal dermatome distributions. Higher frequency (50–120 Hz) is more effective at reducing pelvic pain, which is where most TENS units marketed for dysmenorrhea and pelvic pain are set. 17 The amplitude is self-adjustable to be noticeable yet comfortable. Personal timing of use varies but is usually used in 30-min intervals up to 8 h of application daily. These units are discrete and can be used in any setting whether at home or work.
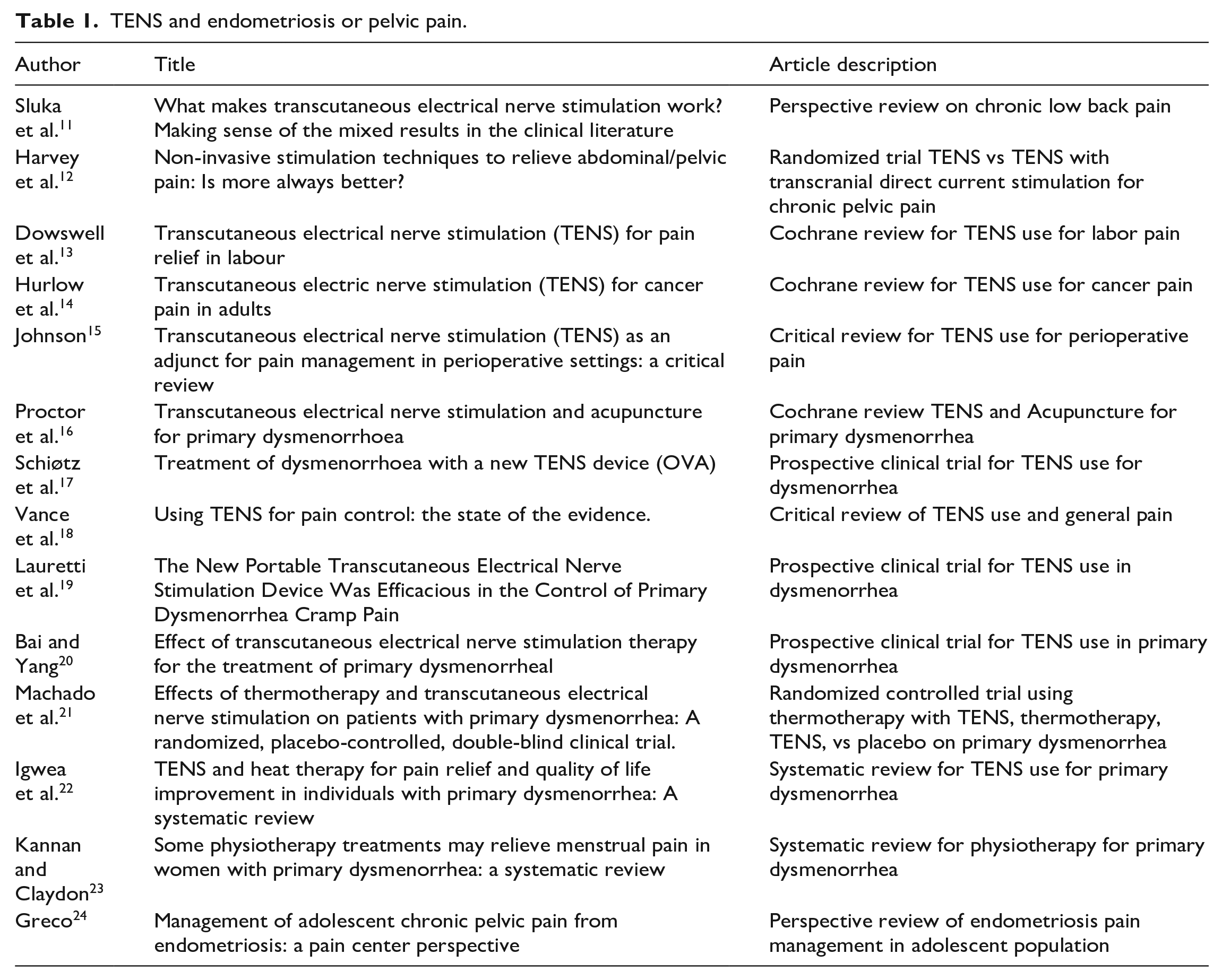
TENS units have been shown to be well-tolerated with minimal side effects and have been successful in reducing pain as quickly as within minutes of application.11–15,17–24 Studies have not only shown a 2–4 point decrease on a 0–10 pain scale with TENS unit use, but also a decreased need for pain medication consumption for the indication of primary amenorrhea.17,19–21 A prospective cross-over trial out of Norway examined the efficacy of TENS on dysmenorrhea in 21 women over 4 menstrual cycles with a month on and month off use of TENS whereby the participants acted as their own controls in the off use months. 17 The investigators found a statistically significant drop in average pain score from 6.73 to 5.18 (p = 0.0009) as well as statistically significant decrease in pain medication use (p = 0.03) whereby 33% of women stopped needing to take pain medication altogether (p = 0.02). 17 No adverse events were found. On long-term follow up 6–8 months after the study, 14/21 (67%) of the participants were still using the TENS unit for pain management. A randomized controlled trial included 40 Brazilian women evaluated the effectiveness of TENS units on pain control of primary dysmenorrhea found a prompt onset of pain relief and a significant drop in mean pain score from 8 to 2 on a 10-point scale (p < 0.001). 19 Diclofenac use was also significantly reduced (p < 0.01). 19 Quality of life significantly improved on standardized quality of life surveys pre and post TENS use (p < 0.05). 19 3 months post study termination, 14/20 (70%) of the participants randomized to the TENS arm continued its use. A similar randomized trial comprising of 134 Chinese women also studied the effect of TENS use on treatment of primary dysmenorrhea and found similar results of significant reduction in pain (p < 0.01), duration of pain (p < 0.01), and pain medication usage (p < 0.01). 20 The common thread among these trials is the indication for TENS use being primary dysmenorrhea and the exclusion of endometriosis pathology. Are these positive findings applicable to a specific patient population with a specific disease process known to have pain as a presenting symptom? Additionally, are these findings in international studies generalizable to the American population? There is ample room to fill in the knowledge gap. Literature search results summarized in Table 1.
TENS and endometriosis or pelvic pain.
Diet
Diet can play an important role as a modifiable risk factor effecting severity and progression of endometriosis. Unfortunately, there is limited literature evaluating this relationship. Generally, maintaining a balanced diet rich in nutrients and low in processed and refined foods can be beneficial. Specifically, certain nutritional deficiencies may be involved in metabolic changes that can increase one’s risk of disease development due to oxidative stress and epigenetic abnormalities. Incorporating vegetables, legumes, and whole grains rich in nutrients such as folic acid, methionine, zinc, vitamin B12, vitamin B6, and vitamins A, C, and E can potentially prevent these negative impacts. 25
Additionally, there are some foods that are associated with development of endometriosis and increased pain symptoms. Some literature suggests that excess estrogen can stimulate production of prostaglandins, increasing inflammation and contributing to worsened pain. Consumption of red meat, which contain relatively higher amounts of estradiol, can increase circulating steroid levels. Trans fat intake with hydrogenated vegetable fat often found in processed foods has also been associated with increased inflammation and development of endometriosis25,28,29 Coffee may be similarly associated. 29
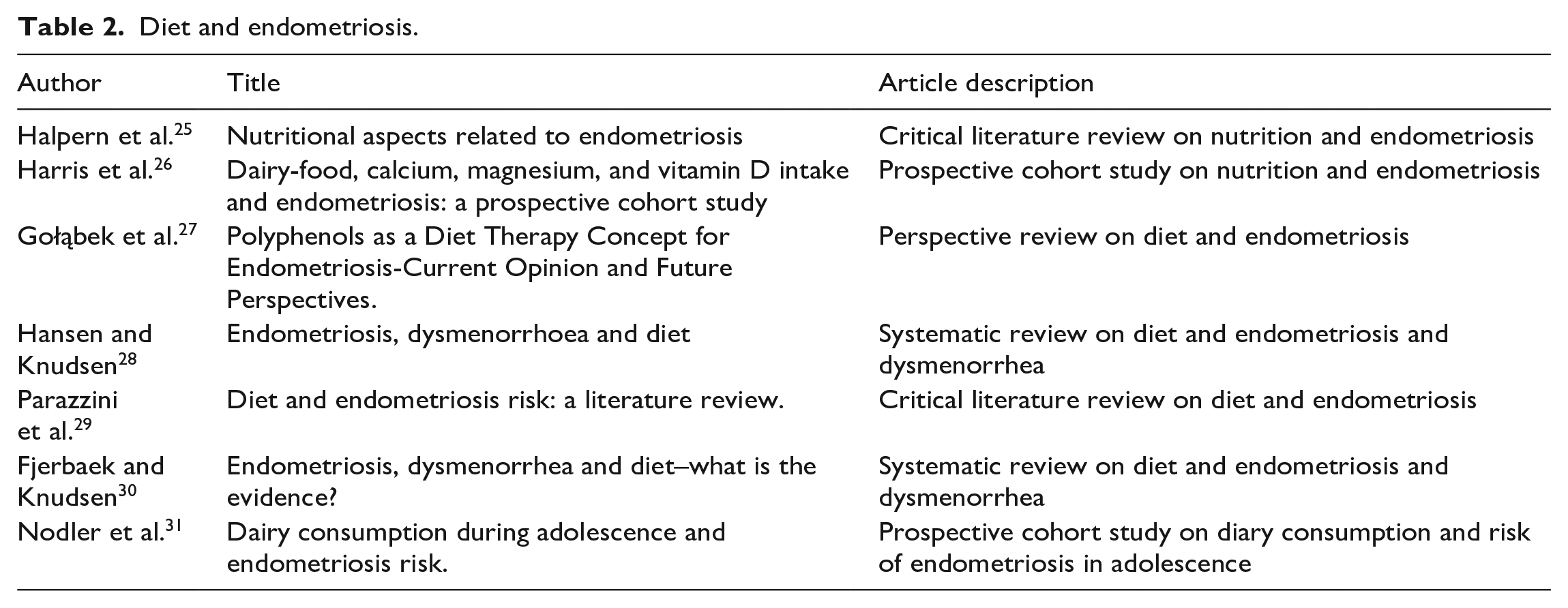
Conversely, introduction of some foods can aid in prevention and improvement of disease. Foods rich in omega-3 fatty acids are thought have anti-inflammatory effects; intake of fish oil may be associated with improved symptoms.25,28–30 Foods containing polyphenols are thought to have anti-endometriotic properties; these foods include citrus fruits, apples, green tea, olive oil, and chocolate. 27 In addition, some studies suggest that increased plasma levels of 25-hydroxyvitamin D and higher intake of dairy products may be associated with a decreased risk of endometriosis, especially with consumption in adolescence.26,31 Results of literature search found in Table 2.
Diet and endometriosis.
Cannabidiol (CBD)
Cannabis is a well-known plant that contains over 100 cannabinoids. The most widely studied is Δ9-tetrahydrocannabinol (THC), but cannabidiol (CBD) has been increasingly favored for its reduced psychotropic profile, potential health benefits and widespread availability. Both CBD and THC have profound effects on human physiology, mainly through the endocannabinoid system (ECS). 32 The ECS is a group of endogenous receptors, ligands, enzymes and proteins that are located in the central and peripheral nervous system. The ECS has been shown to have direct effects on motor function, eating habits, mood, immunocompetency, cell proliferation, pain perception and inflammation.33–35 It is mainly through these last several qualities that CBD is thought to have a beneficial effect on pain conditions, such as endometriosis. Here, we focus primarily on CBD as the policies for other Cannabis strains for medical or recreational use vary greatly from state to state.
CBD is available in many routes of administration including sublingual and oral. Other less common routes of administration included topical, inhalation, vaginal suppository and buccal spray. CBD is generally well tolerated. Common side effects include decreased appetite, fatigue, sleep disturbances, gastrointestinal upset, hypersensitivity reactions (rash) and dose dependent liver dysfunction. Mild transaminitis was mostly seen with concomitant use of valproate and to a lesser degree, clobazam.36,37
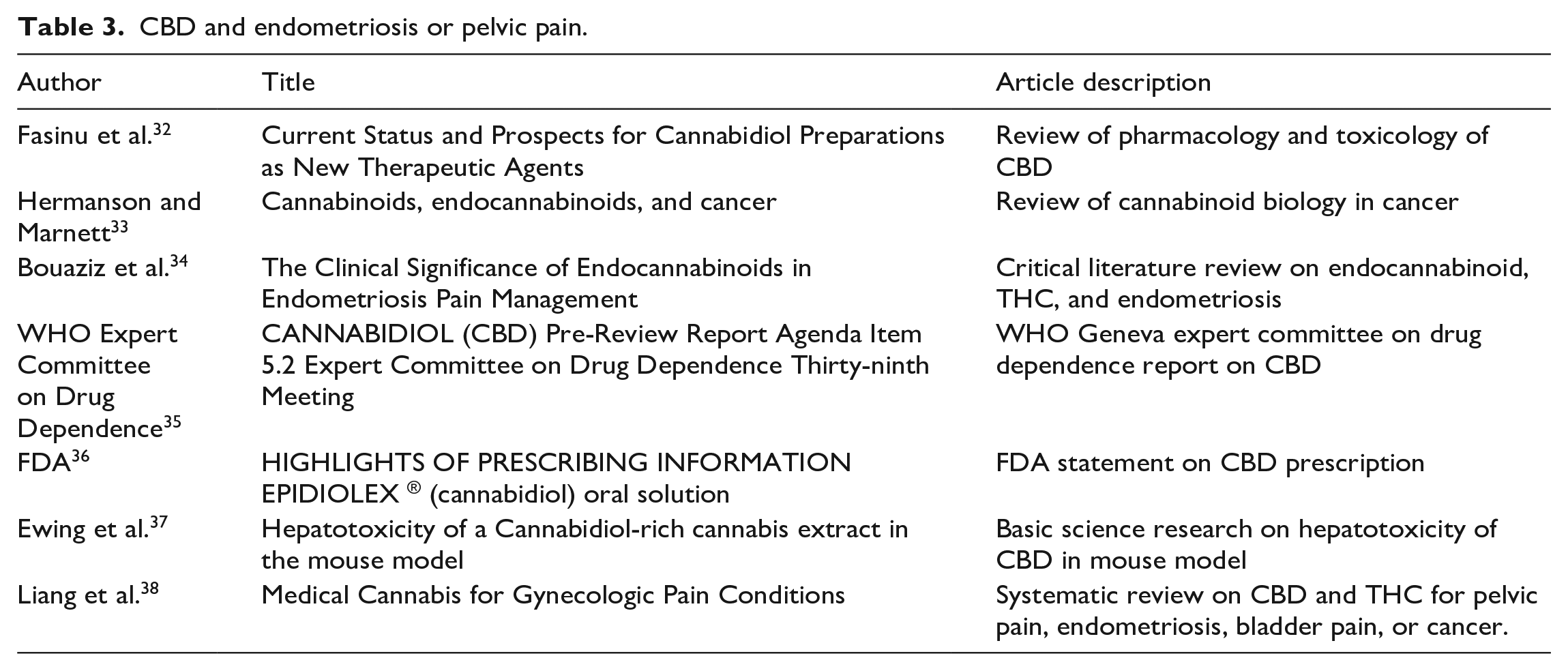
While there are currently over 70 clinical trials studying the role of cannabidiol with or without THC in the acute or chronic pain setting, no randomized prospective studies have been published for CBD in the setting of endometriosis related pain. A wide variety of data exist regarding CBD use and its effect on pain, compounded by multiple delivery methods and varying combinations of THC. Surveys demonstrate that CBD has been used in self-management strategies for endometriosis with significant pain reduction. 7 The authors of this paper agree with a recent systematic review that Cannabis derivatives have potential to be relatively safe and effective treatment for pelvic pain conditions. 38 With appropriate counseling, CBD or CBD dominant products can be used as an adjunctive measure, but not as a replacement for standard surgery or medical management for endometriosis. Details of literature search results in Table 3.
CBD and endometriosis or pelvic pain.
Turmeric
Turmeric use has become more popular in modern times; however, it has been used for centuries for a multitude of purposes, including medicinal, cosmetic, and dietary. Turmeric is primarily derived from the cucuma longa plant. 39 The primary chemical typically studied is curcumin which has been linked to decreasing inflammation. 40 Curcumin has also been seen to have positive effects on endometriosis as well. Animal studies have shown how cucurmin can have a therapeutic potential against endometriosis by decreasing certain cytokines and having anti-angiogenic effects.40,41
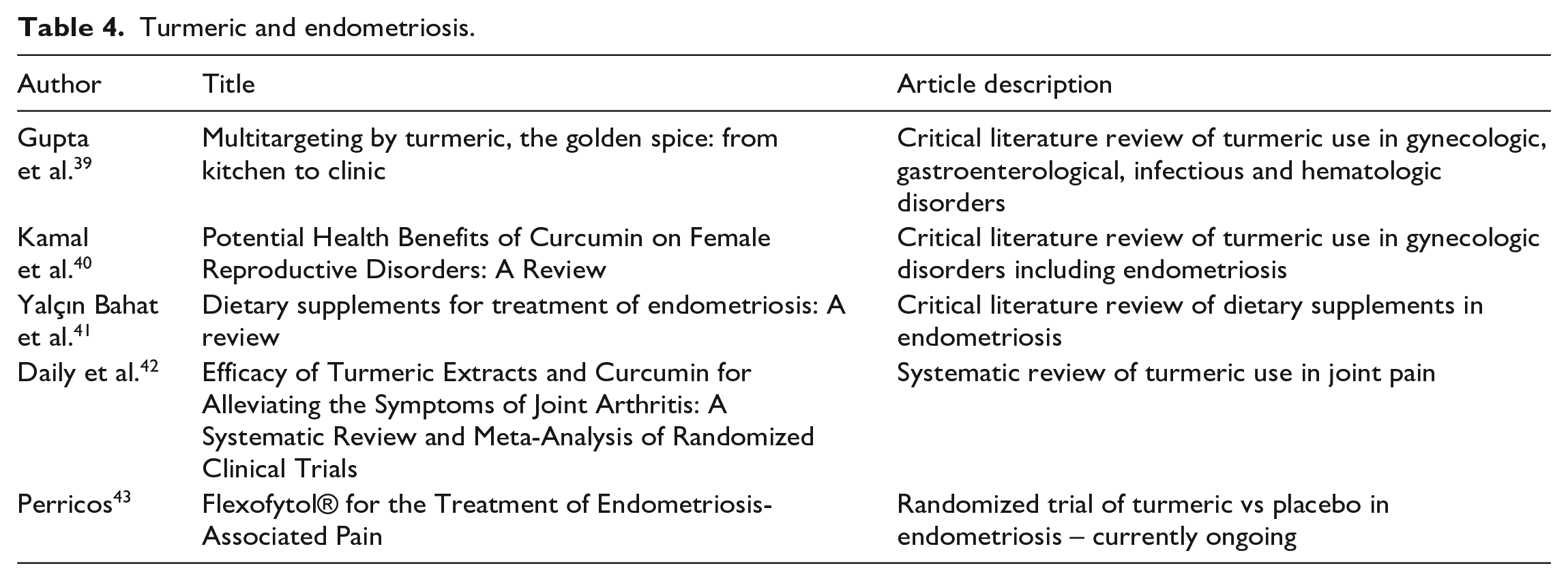
The benefits of turmeric that patients with endometriosis see are not well described in the literature. While effects have not been well studied there are no harmful side effects seen with turmeric supplementation. There is no current guidance on how much turmeric a patient could take to see results. There are a variety of supplements on the market which range from 350 to 1000 mg of turmeric. There are studies evaluating turmeric and arthritis pain which show benefits similar to NSAIDS when taking 1000 mg per day. 42 There is currently a randomized controlled trial out of Vienna, patients will have received either 42 mg of curcumin versus placebo. The primary outcome is pain compared to baseline after 4 months. 43 Results for the study are not yet published. Hopefully future studies will continue to show the benefits of turmeric for patients with endometriosis. Table 4 summarizes the results of the literature search.
Turmeric and endometriosis.
Meditation
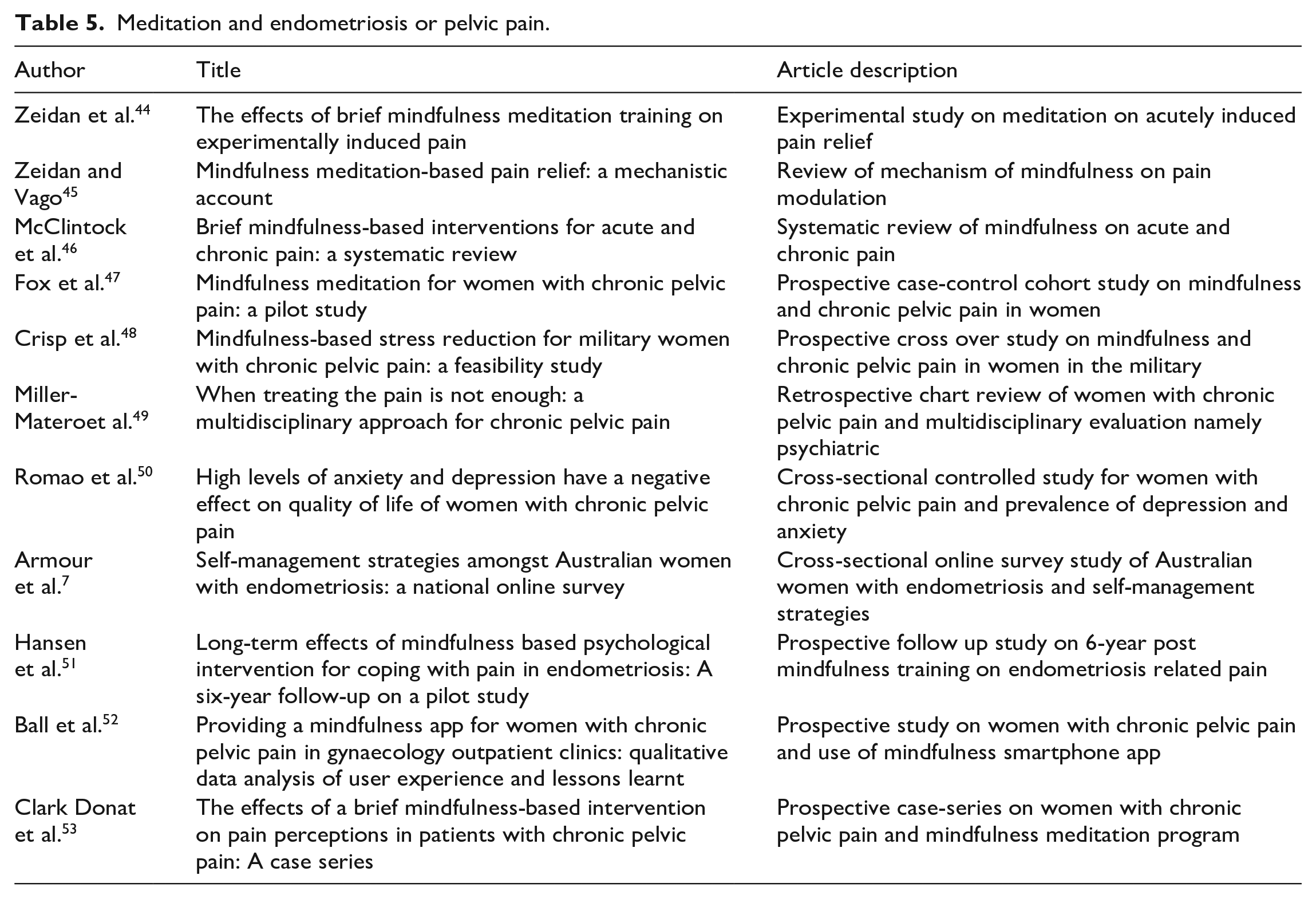
Although there are many types of mindfulness meditation practices, the main goal of meditation is to learn how to work toward a state of non-judgment, acceptance and deliberate focus on the present. Mindfulness-based interventions have been effective in improving outcomes in chronic pain syndromes.44–48 These techniques include deep-breathing exercises, guided imagery, hypnotherapy, progressive relaxation among others.
Patients with chronic pelvic pain have been reported to have a high rate of mental health issues with a prevalence rate of anxiety of 38.6%–73% and rates of depression of 25.7%–40% in women with chronic pelvic pain.49,50 Given the high association of psychological comorbidities with endometriosis and chronic pelvic pain and the stress of dealing with a chronic pain syndrome, treatments which focus on promoting mental health hold significant promise. Mindfulness meditation is a strategy that can be utilized by a patient having a mental health crisis or a pain flare. Mindfulness meditation programs vary in length and intensity. Having multiple strategies to manage and cope with pain can ultimately empower patients with a chronic pain condition.
Mindfulness meditation is favored by patients as a method of self-treatment. In one study that surveyed 484 Australian women with endometriosis, meditation was one of the most common forms of self-management with 47% of respondents using meditation or breathing exercises. 7 Many of the formal programs are time intensive which can be a barrier for patients. However, once patients learn simple mindfulness strategies, they can implement these into their own lives and treatment plans.
In a group of 10 patients with chronic pelvic pain and endometriosis, Hansen et al showed sustained long-term effects of a 10-session mindfulness intervention with improved quality of life at 6-year follow-up. 51 A study in the UK which aimed to implement the use of a mindfulness meditation smartphone app, found disappointing results with only 36% of the meditation group using the app once during the study. 52 One consideration would be tailoring apps specifically to the patient population.
Another study aimed to make mindfulness more accessible to patients by integrating this into already scheduled pelvic floor physical therapy sessions. Pre-taped meditation sessions were designed specifically for chronic pelvic pain patients, and they were also given written guidance on their practice. While only half of the participants finished the study, for those that completed the study, pain catastrophizing scores significantly improved. 53
Implementation of a mindfulness meditation practice into the multidisciplinary care of patients with chronic pelvic pain has the potential to improve mental health and overall quality of life. See Table 5 for details of articles referenced in this section.
Meditation and endometriosis or pelvic pain.
Yoga
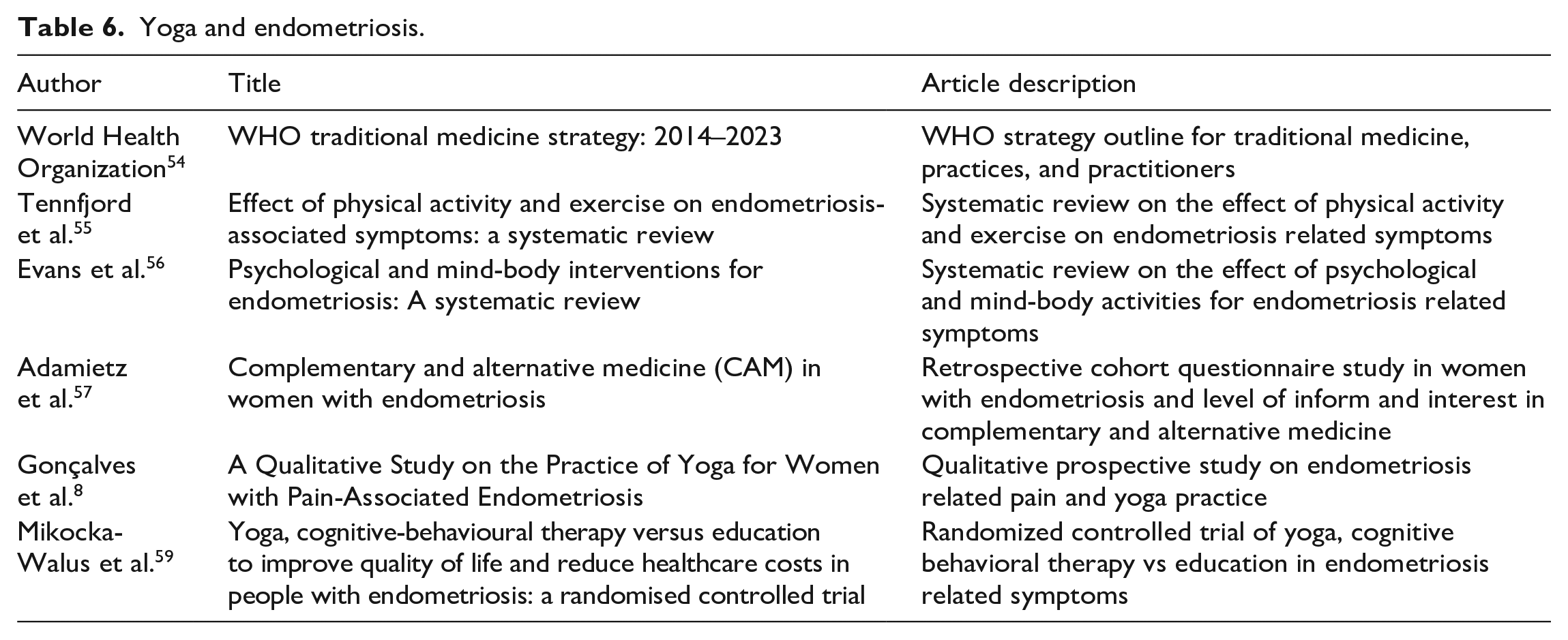
The World Health Organization classifies yoga as a mind-body intervention, while other literature considers yoga a psychological and/or physical activity.54–56 Due to the diversity of yoga methodologies where some focus more on the psychological aspect of the practice and others prioritize the physical practice, yoga has a wide range of uses and applications. A 2019 survey of 484 Australian women with endometriosis found that 35% (131) of patients used yoga as an aspect of their endometriosis care, with a mean level of symptomatic improvement recorded at 4.5 on a scale of 1–10, where 10 represented “symptoms most improved.” 7 More recently, a survey assessing knowledge and adoption of Complementary and Alternative Medicine (CAM) in endometriosis patients similarly determined that yoga is a popular management technique, with 33.3% (38) of patients indicating that they had used yoga for disease management (n = 114). 57
Multiple studies have tried to characterize the safety and efficacy of yoga in regards to endometriosis management, but varied styles of yoga, small sample sizes, and low-quality evidence create challenges for systematically reviewing literature. 54 Currently, the only existing randomized control trial regarding yoga as a therapeutic management technique for endometriosis was conducted on a small sample of Brazilian women diagnosed with endometriosis. 57 This study found that patients who completed twice weekly 90-min session yoga for 8 weeks experienced significantly lower daily pain when compared to the control group (p = 0.0007). Both the control group and the group assigned to yoga reported Quality of Life improvements on pre- and post-intervention surveys. 58 A systematic review examining the effects of physical activity on endometriosis analyzed this Brazilian study, but rated the overall quality as poor according to National Heart Lung and Blood Institute guidelines for “quality assessment of controlled intervention studies.” 54 Gonçalves also published a qualitative study on the practice of yoga in 15 women who suffered from pain associated with endometriosis. These patients underwent twice weekly yoga sessions for 8 weeks, followed by semi-structured interviews that revealed all participants found yoga was beneficial in controlling pelvic pain. 8 The authors postulated that this was likely due to a combination of mind-body integration, self-awareness, and psychosocial support developed between participants. 8
The protocol for a randomized control trial which aims to compare yoga, cognitive behavioral therapy and education as means of endometriosis management on quality of life measures was recently published; this study should further elucidate the efficacy of yoga on endometriosis. 59 Refer to Table 6 for articles referenced in this section.
Yoga and endometriosis.
Acupuncture
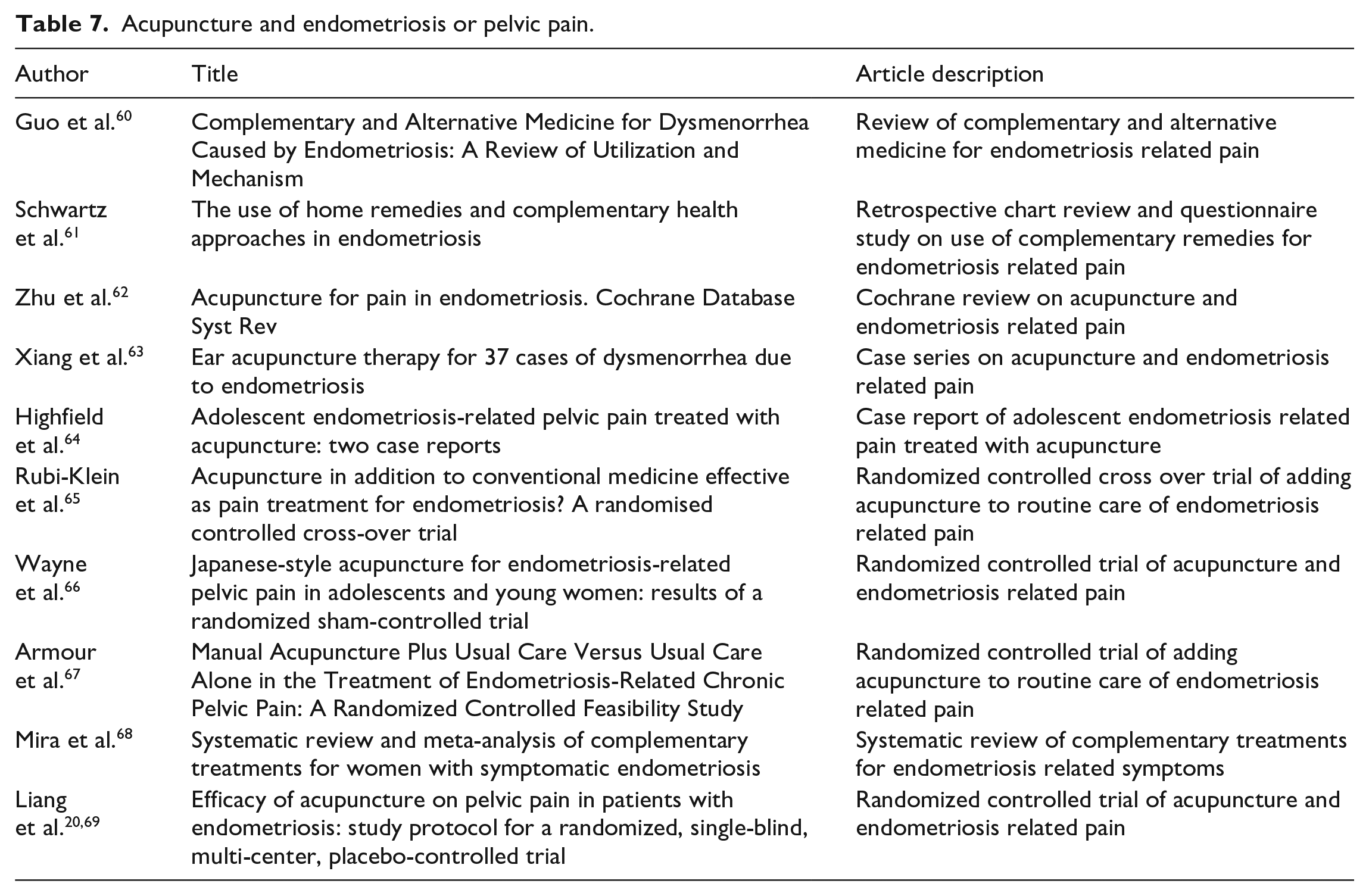
Once solely practiced as a component of Traditional Chinese Medicine (TCM), acupuncture has gradually developed into diverse practice with multiple methodologies documented in research literature. A recent review article described several different types of therapeutic acupuncture used in the treatment of endometriosis: acupuncture with or without moxibustion, acupuncture combined with TCM, warming acupuncture, acupoint catgut embedding, electroacupuncture, and auricular acupoint treatment. 60 Multiple surveys assessing patient attitudes toward and adoption of complementary or alternative therapies suggest that acupuncture is increasing in popularity. Studies published between 2019 and 2021 indicate that between 8% and 22.8% of endometriosis patients reported using acupuncture for disease management.7,57,61 One of these surveys additionally inquired about efficacy, and found that 44.3% (58 of 574) of patients felt acupuncture was effective. 61 Several randomized control trials as well as systematic reviews have reported a small, but overall positive effect of acupuncture when used for endometriosis management.62–66 Most recently, 19 participants with confirmed laparoscopic diagnosis of endometriosis completed a randomized controlled feasibility study where they were administered 16 acupuncture treatments over 8 weeks in addition to usual care. 67 The control group received usual care alone and experienced a disproportionate withdrawal rate (53%) compared to the treatment group (14%); treated patients experienced a significant decrease in reported pain and improved quality of life. 68 The authors concluded that acupuncture is safe and effective, but usual care is not an acceptable control group. 67 A systematic review and meta-analysis published in 2018 evaluated two different randomized control trials where traditional acupuncture methods were compared with “sham” acupuncture, meaning the placebo group had needles placed at cutaneous sites that are not traditional endometriosis acupoints. 68 This review determined that acupuncture was associated with improvement in endometriosis symptoms; meta-analysis of the two RCTs revealed that acupuncture according to traditional methods led to better outcomes when compared with participants who received sham or placebo acupuncture (RR: −1.93, 95% CI: −3.33 to −0.53; p = 0.007). 68 An additional protocol for a randomized, single-blind, placed-controlled trial was published in June 2018 and aims to further determine acupuncture effectivity with a treatment group receiving care that aligns with Traditional Chinese Medicine, while control group members will receive acupuncture at non-acupoints.20,69 Table 7 demonstrates the articles cited in this section.
Acupuncture and endometriosis or pelvic pain.
Conclusion
Being able to self-manage pain, whether chronic or flare ups, gives patients agency and control over a chronic pain condition that can be debilitating especially during a pandemic where access to care may be limited. We reviewed the available data on popular complementary therapies for endometriosis-related pain ranging from TENS, diets, CBD, turmeric, meditation, yoga, to acupuncture. The overarching theme across these multitude of therapies is that we need more research and data for each of the above to better counsel patients with endometriosis on complementary therapies. We have some basis to suggest these options of self-managed therapies however with limited data in support. We hope to have provided insight into what is available as complementary modalities of pain management for patients with endometriosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.