
Abstract
Aim:
To identify and review the success of non-pharmaceutical, non-surgical biopsychosocial interventions in individuals with endometriosis, in managing pain and improving body image.
Methods:
Cochrane, EBSCO, IBSS, NICE, Open Grey, OVID, Proquest, Scopus and Science Direct were searched in April 2021, using inclusion and exclusion criteria.
Data collection and analysis:
Five randomised control trials, and one controlled clinical trial resulted from the search. Study quality was assessed using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool. Studies were synthesised by intervention type, into physical only, and physical and psychological.
Results:
Across the six papers, 323 participants were recruited, through medical records or self-referral, and treatments largely administered by specialist practitioners. From the EPHPP quality assessment,2 weak quality papers, and four moderate quality papers found improvements to pain, with large effect sizes in four papers. No studies used established body image measures to examine intervention effects on body image, and all lacked health psychology theoretical basis. There were common issues in selection bias, confounders and blinding.
Conclusion:
Without gold-standard methodology, evidence of effectiveness cannot be concluded. However, there is promising rationale if these issues are addressed.
Introduction
Endometriosis is a chronic, painful condition affecting 10% of people born with female-assigned reproductive organs worldwide, and is the second most common gynaecological condition in the UK. 1 Due to the subjectivity of pain, many face challenges articulating their pain severity with healthcare professionals, often leading to dismissal and prolonged diagnosis. 2
Treatment
Endometriosis is usually treated with pharmaceutical (hormonal/medicinal) and surgical treatments. 3 However, cis-women report being dissatisfied with ‘conventional’ treatments received for their endometriosis, owing to persisting symptoms and lack of satisfaction with medical support. 4 61.5% of cis-women (n = 133) reported seeking naturopathic and/or complementary procedures instead. 5 However, the evidence base for non-pharmaceutical, non-surgical treatments is still limited, highlighting a need for further research on their effectiveness in endometriosis. Providing options for self-management are important, given the value these provide in increasing autonomy and self-esteem, 6 often damaged through dismissal or disbelief by health professionals. 7
Current challenges
The economic burden associated with endometriosis is estimated around £8.4 billion in the UK, with higher costs associated with increased pain presence, 8 similar to diabetes, 9 yet with no comparable financial or research investment. The lack of resource investment has meant despite 82% of physicians believing there is a need for those with endometriosis to receive psychosocial care, only 15% routinely refer patients for this, with 72% not feeling adequately trained to provide care for psychosocial aspects of endometriosis. 10 Therefore, understanding the impact of endometriosis on people born with female-assigned reproductive organs, and increasing the evidence base of treatments is needed.
A narrative review on the effects of complementary therapies on managing the condition, and associated sexological concerns, highlighted the need for a multidisciplinary team, to support the multifaceted outcomes from endometriosis. 11 There are important links between sexual functioning and body image, and greater body image perception has been found to have associated benefits related to sexual experience. 12 Greater body esteem also correlated with improved psychological outcomes in those with endometriosis. 13 However, interventions seeking to improve body image in endometriosis are scarce, suggesting a need to develop and understand intervention effects in this facet of the condition, for better psychological outcomes. 14
Body image
Body image is defined as a person’s perception, feelings and thoughts about their body, influenced by body size estimation, body attractiveness evaluation and associated emotions. 15 Those with endometriosis may have negative body image distortions and general body dissatisfaction, 16 due to scars following surgical interventions, or feeling overweight because of hormonal therapy. 17 Many describe feeling ‘less attractive’, with their body ‘not functioning as a woman’s body should’. 18 Dissatisfaction with one’s body has been linked with disruptions to sense of wellbeing and self-compassion. 19 Some see their relationship with their body as a constant struggle for control, with 34% (n = 40) feeling their general appearance had been affected by the condition, 20 negatively affecting self-esteem. 21 Those with endometriosis also report feelings of shame and inadequacy alongside the body image concerns, 22 creating a fractured sense of self in the body of the sufferer.
Pain
The relationship between the body and sense of self is further challenged in endometriosis, 18 as many struggle making meaning of undiagnosed, unexplainable pain for years. Pain becoming a core part of a person’s narrative identity, 23 can result in further pain, suggesting the altered sense of self, can make pain experience worse in those with endometriosis. 23 Pain associated with endometriosis significantly impacts psychological wellbeing, 24 with reports of confusion and self-guilt from those with the condition, as though they are responsible. 25 This negatively influences their beliefs that their health results from one’s own doing. 26 Those with endometriosis have reported their increased pain levels linked with an increased lack of familiarity with their body, possibly as a coping mechanism to distance themselves from the significant amount of pain their body faces. 16 Perceiving a ‘sick body’ with endometriosis and its associated chronic pain can cause negative body image and general body dissatisfaction. 16 Other research on chronic pain and body image suggests body appreciation can be more challenging when their body is a source of chronic pain, 27 highlighting a need for interventions to target both facets, and echoing the suggestion that a one-dimensional focus may not be sufficient for advancing optimal treatment. 28
Interventions to improve both pain and body image are currently limited, but have shown promise in chronic pain patients, where multisensory feedback interventions, such as virtual reality, resulted in improvements to both body image and pain-related symptoms. 29 Furthermore, increasing pain acceptance has been found to be effective at improving body image, 27 suggesting treating one facet can influence the other. Therefore, interventions to manage pain and improve body image, need to take into account the many individual, personal challenges that come with endometriosis, reiterating the importance of treating the condition in an individualised, biopsychosocial way. 22
Objectives
There have been limited systematic reviews on the effects of complementary therapies on pain in endometriosis,30,31 and none also seeking to understand the effect of these therapeutic interventions on body image. The objectives of this review are to identify and review the methodological quality, and effectiveness of non-pharmaceutical, non-surgical biopsychosocial interventions in managing pain and improving body image in those with endometriosis.
Materials and methods
Protocol and registration
This review was conducted in line with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) checklist and was registered with PROSPERO (ID: CRD42021245763). No information was amended after registration submission.
Information sources and search strategy
Electronic databases were searched by the primary reviewer (LF), using the search criteria below. These included nine databases, and grey literature, to counter publication bias; Cochrane, EBSCO, IBSS, NICE, Open Grey, OVID, Proquest, Scopus and Science Direct. Combinations of population (‘endometriosis’ and ‘wom?n’ OR ‘female’), intervention (‘diet*’ OR ‘exercis*’ OR ‘psychosocial’ OR ‘complementary therap*’) and outcome (‘pain’ OR ‘body image’) were used with Boolean Operators.
Eligibility criteria
To identify biopsychosocial interventions measuring pain and body image related outcomes in endometriosis, inclusion and exclusion criteria were created. Biopsychosocial is defined in this review as biological, physiological, psychological, social interventions influencing the outcome of interest, for example, to alter physical or psychological functioning. Participants had to be females, aged over 18, with laparoscopically confirmed endometriosis, due to the high validity this has compared to medical records alone, and wide variety of symptoms presenting with the condition. Cisgender females were included due to the complex body image and identity related concerns potentially arising from the condition presenting in someone with female organs but identifying as male. 32 Quantitative studies examining participants post intervention, against a comparator/control group were included. There were no date limitations. Theses, dissertations, articles, research reports and conference papers were included. Qualitative studies were excluded due to their difficulty in examining cause and effect. Studies not written in English were excluded, due to potential for misinterpretation with language translation. Studies using hormonal, medicinal, surgical interventions as the main treatment were excluded, to increase understanding of the effects of alternative treatments on symptoms and patient choice and autonomy. Studies without pain or body image as a primary outcome, for example, endometriosis-related risk or fertility, were excluded. Studies that were not interventions were excluded, for example, questionnaire-based studies of cis-women’s experiences. Studies without pain, body image or endometriosis related scales/measures were excluded. Articles on chronic pelvic pain and primary dysmenorrhoea in general were excluded due to the different way these conditions present.
Study selection
Two independent reviewers (LF and EH) screened studies for eligibility. Zotero was used for title and abstract screening, followed by Covidence for full-text screening.
Data extraction
The primary reviewer, LF developed and conducted a standardised data extraction protocol, reviewed by the secondary reviewer, EH. This included: reference; publication type/year; conflicts of interest; funding; study design; participant characteristics; intervention/recruitment methods; quality; outcomes/assessment tools; key findings. Missing data was obtained through request by LF, to the corresponding author of the relevant paper.
Quality assessments and risk of bias
Eligible full-text articles were assessed for selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs, intervention integrity and analyses, using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies. 33 Quality assessment was carried out by LF, and reviewed by EH. Effectiveness was evaluated in strong quality studies. Findings from weak/moderate studies cannot signify effectiveness due to higher risk of bias, so methodology was evaluated.
Data synthesis
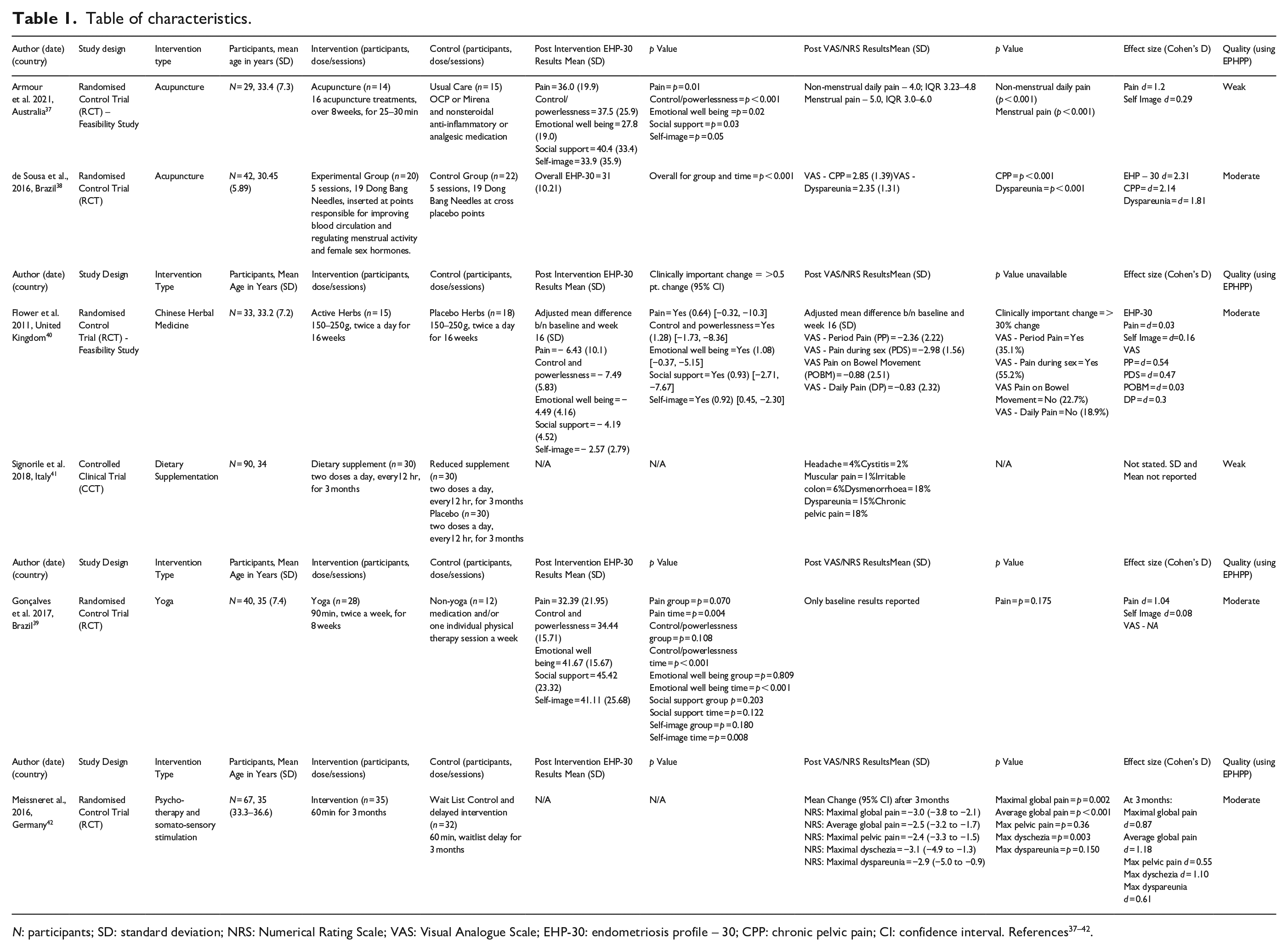
Due to clinical and methodological heterogeneity, a meta-analysis was not appropriate, a common problem faced in social sciences research. 34 Therefore, a narrative review was conducted, and table of characteristics (see Table 1) created to display homogeneity and heterogeneity in results. Data was synthesised through grouping the studies into two groups: ‘physical only’ interventions, defined as tangible interventions delivered to the physical body, or ‘combined physical and psychological’ interventions. Interventions were considered effective if they were rated strong using the EPHPP, and found statistically significant improvements (p value of <0.05), in pain or body image, against the control group. Where possible, effect sizes were calculated using Cohen’s d, using mean and standard deviation data. Effect sizes were interpreted as small d = 0.20, medium d = 0.50 and large d = 0.80. 35
Table of characteristics.
Results
Study selection
A total of six publications were identified from 9101 records (five Randomised Control Trials, and one Controlled Clinical study, displayed in detail in Figure 1).
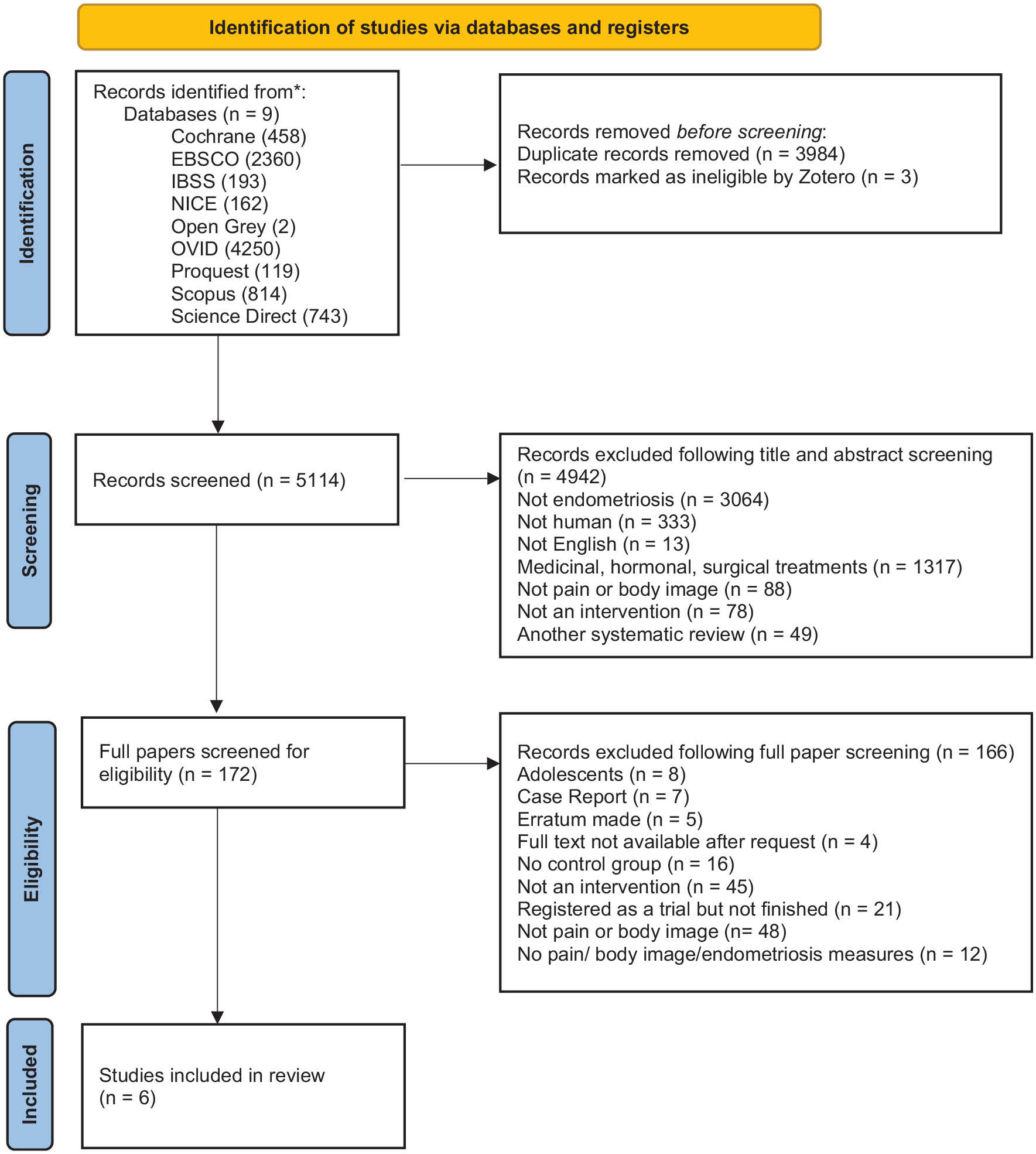
Flowchart of study screening – Adapted from Page et al. 36
Study characteristics
All studies included in this review were published between 2011 and 2021, and were conducted in Australia, 37 Brazil,38,39 United Kingdom, 40 Italy 41 and Germany. 42 Details on author, publication year, location, participants, intervention type, duration, outcome measures, p-values, effect sizes (where calculated), and study quality (see below for details of assessment) are presented in Table 1. All studies examined the results of the interventions on pain as a primary outcome, with none focusing specifically on body image. The only outcome measure recording variables relating to body image was the EHP-30, a valid, reliable disease specific endometriosis measure, 43 consisting of 30 questions, with five core subscales: pain, control/powerlessness, emotional well-being, social support and self-image. No outcomes from established body image scales were reported.
Sample characteristics
Three hundred twenty-three participants from the six studies included, had a mean age of 33.5 years. All were diagnosed with stage 1–4 endometriosis, and length of time since diagnosis varied from 4 to 12 years. Only two studies reported sociodemographic information,37,38 and in these two studies all the participants were white (n = 45), apart from four who were of black ethnicity. Most had studied to higher level education, and were married or in a relationship. Participants were recruited via university, 41 outpatient clinics38,39 or self-referred.37,40 One study 42 did not state how participants were recruited.
Quality assessment
The EPHPP tool identified two papers as weak37,41 and four as moderate38–40,42 (see Table 1). Selection bias was the domain with the lowest ratings, with all papers rated weak37,38,40 or moderate.39,41,42 Confounders were also an issue, with 3 weak37,39,41, one moderate rating. 42 Blinding had 1 weak, 42 and three moderate ratings.37,39,41 A strength across all papers was the use of valid, reliable tools to collect data.
Outcome measures
Four studies37–40 recorded EHP-30 results. An overall EHP-30 score was reported for papers without subscale scores. No standardised body image scales were used in any of these studies. This was instead measured with the self-image scale of the EHP-30. In addition to the EHP-30, Three studies38–40 also recorded Visual Analogue Scale (VAS) results, an 11 point line measuring a continuum of symptom severity. 44 One study used VAS 41 only. Another 42 used Numeric Pain Rating Scale (NRS) only, an 11 point numeric scale from ‘0’ (no pain) to ‘10’ (worst pain imaginable). 45 Both the VAS and NRS are widely used to measure pain and its related intensity, and best adapted for endometriosis pain measurement. 46
Intervention characteristics – Synthesis of results
The six studies included in this review were grouped by intervention focus; examining overall effects of physical interventions, and combined physical and psychological interventions. No effect sizes were reported, but were calculated where possible37–40,42 (see Table 1).
Physical only
Intervention
Four studies (total n = 216), investigated the effects of physical interventions in endometriosis; acupuncture,37,38 Chinese Herbal Medicine (CHM) 40 and Dietary Supplementation. 41 Two were feasibility studies37,40, three were randomised control trials,37,38,40 and one was a controlled clinical trial. 41 Interventions were conducted in hospital 38 and private clinic settings,37,40 delivered by specialist practitioners (e.g. physiotherapists, 38 Chinese Medicine Practitioners,37,40 or the patient. 40 Location and intervention delivery method were not stated in one study, 41 and unattainable upon request. Interventions ranged from 5 38 to 16 40 weeks, with treatment frequency ranging from 5 38 to 16 treatments. 37 Session duration ranged from 25 37 to 40 min. 38 Supplements were provided for consumption twice a day.40,41 Control group participants were offered placebo treatments38,40 or asked to continue their usual care.37,41 In one study, 37 participants were permitted to use other therapies, for example physiotherapy/massage/nutrition, at the same time as receiving the intervention, potentially influencing results. One study conducted an intention to treat analysis. 37
Outcomes
None of the four physical intervention studies were assessed as strong quality, therefore the results, whilst promising, must be interpreted with caution. One study 41 did not report statistics, so there was not enough detail to report effect size. One weak study 37 found significant large effect sizes in pain outcomes (d = 1.2, p = 0.01), with smaller effect sizes in self-image (d = 0.29, p = 0.05). One moderate study 38 found significant large effect sizes in overall EHP-30 (d = 2.3, p < 0.001) and VAS (d = 1.81–2.14, p < 0.001) outcomes. Another moderate study found small effect sizes for EHP-30 (d = 0.03–0.16), but larger effect sizes for VAS outcomes (d = 0.3–0.54). 40
EHP-30
Three studies recorded EHP-30 results,37,38,40 with improvements in the intervention groups in all EHP-30 domains. Significant, yet weak evidence resulted from one acupuncture study for improvements in pain (p = 0.01) and self-image (p = 0.05). 37 Despite initial improvements in the control group, these were not maintained. The moderate quality studies resulted in significant evidence for overall EHP-30 improvements (p < 0.001) following acupuncture, 38 and clinically important changes following CHM in all domains of the EHP-30 (>0.5 point change). 40 There was moderate evidence of small improvements in both control groups provided with placebo treatments,38,40 however placebo treatments in CHM are often physically identical to non-placebo treatments. 47
VAS/NRS
Improvements to pain scores were reported in the intervention group of all studies. Significant, yet weak evidence showed improvements to pain (p < 0.001) in studies of acupuncture 37 and dietary supplementation. 41 The control groups of these weak studies reported increased pain through placebo use, 41 and usual pharmaceutical care, although results were not significant (p = 0.08). 37 Moderate evidence showed significant improvements to pain scores in another acupuncture study (p < 0.001), 38 and clinically relevant changes in period pain (31.5%), and pain on intercourse (55.2%) following CHM. 40 The control groups of both moderate studies were provided placebo treatments38,40 which showed initial improvements but were not maintained after 2 months. 38
Summary of physical interventions
The weak quality of two studies37,41 precludes their influence in the appraisal of effectiveness and reliability in wider application. Acupuncture 38 and CHM 40 provide moderate evidence of effectiveness of physical interventions offering improvements to pain management and body image. Weaknesses were identified in selection bias, lack of sociodemographic variability, and confounders in participants. One study conducted an ITT analysis 37 suggesting there is promise in the rationale of this, and the other studies in this review if the above methodological issues are addressed.
Combined physical and psychological interventions
Intervention
Two studies (total n = 107) investigated mind-body interventions in endometriosis; yoga 39 and psychotherapy with somatosensory stimulation (acupuncture point stimulation). 42 They were both randomised control trials39,42 conducted in outpatient settings, utilising a gynaecologic practice, 42 and delivered by specialist practitioners, in traditional Chinese medicine, 42 psychosomatic medical specialists 42 and qualified yoga instructors. 39 The experimental group interventions ranged from 8 39 to 12 42 weeks, with an average of 8 42 to 16 sessions. 39 Session duration ranged from 60 42 to 120 min. 39 The control groups received the same treatment as the intervention after a 3 months wait, 42 or standard care and one physical therapy session each week. 39 As found in the physical interventions, only one study conducted an intention to treat analysis. 42
Outcomes
Both studies were moderate quality, so the above methodological considerations should be accounted for before conclusions on their effectiveness can be made. In one study, 39 significant large effects were found for pain (d = 1.04, p = 0.0046) but small effects for self-image (d = 0.08, p = 0.0087). In the other study, significant large effect sizes for pain were found at 3 months (d = 0.87–1.18, p < 0.001). 42 However, effect sizes reduced over the 3–24 months follow ups (d =0.36–33). 42
EHP-30
In the yoga group, statistically significant improvements were found over time in most of the core EHP-30 domains, including pain (p = 0.0046) and self-image (p = 0.0087). EHP-30 improvements were also observed in the control group, however they were offered physical therapy. The study also found that improving one domain may have affected other domains, for example, having more control, potentially improving self-image, again highlighting the importance of targeting multiple facets of endometriosis. 27
VAS/NRS
Significant reductions in VAS pain scores were observed in the yoga group, compared with cis-women in the control group (p < 0.001), whose pain tended to increase. 39 However, retrospective ratings were used which may lead to recall bias. The psychotherapy study observed NRS scores reduce to a clinically significant amount (p < 0.001). 42
Summary of combined physical and psychological interventions
Yoga 39 and psychotherapy 42 provide moderate evidence of effectiveness, of combined interventions offering improvements to pain management and body image in endometriosis. Weaknesses were identified in selection bias, blinding, confounding and withdrawals. As both combined physical and psychological interventions were delivered face to face, adaptations may need to be considered in future, as this may have impacted dropout rates.
Discussion
The aim of the current review was to describe and compare quality and effectiveness of non-pharmaceutical, non-surgical biopsychosocial interventions, in reducing pain and improving body image in those with endometriosis. All the studies examined pain management as a primary outcome, but despite the known impact of endometriosis on body image, no interventions measuring body image, using body image specific scales, were identified. The review considered a wide range of interventions, and six studies resulted from screening.
Discussion of studies
Sample characteristics
The samples participants were not representative of wider sociodemographic populations, reducing their external validity. Research on the impact of ethnicity on endometriosis treatment accessibility is scarce. 48 Those from lower income or limited educational backgrounds 49 have less access to care for chronic pain, and those from lower socio-economic backgrounds feel health professionals are less likely to take their complaints seriously. 50 This highlights a necessity for increased research on treatment choice, availability and accessibility in different sociodemographic variables.
It is not clear from the studies if observed effects would differ dependent on length of diagnosis, or disease severity. There is a risk of spectrum bias from the current studies, as all participants have diagnosed, symptomatic endometriosis. The impact of such interventions on those with symptoms, without an endometriosis diagnosis, needs consideration.
Quality
The interventions showed promising rationale for pain management, but their lower quality meant the evidence of effectiveness could not be affirmed. This corresponds with findings of another systematic review on complementary treatments in pain management in endometriosis, which also identified complementary treatments alleviated symptoms, but higher quality studies were required to confirm their effectiveness. 49
Using the EPHPP to examine quality, common weaknesses identified were selection bias, blinding and confounders. The moderate studies had weak ratings in one of these domains.38–40,42 Weak studies had low ratings in at least two of these domains.37,41 Participants were mainly recruited from clinics or self-referred. Issues surrounding selection bias and confounders is a common issue identified within the endometriosis population, due to the many sociodemographic and diagnostic differences surrounding the condition. 51 People born with female-assigned reproductive organs self-referring, particularly from self-help groups, may present with more treatment-resistant disease than broader groups of people receiving conventional treatment, 52 potentially due to their scepticism and mistrust of doctors, whose expertise on the condition they doubt. 53 Furthermore, the complex process of diagnosis may impact recruitment of participants representative of the wider endometriosis population, as it does not account for those with symptoms but without diagnosis. Most studies reduced this bias by randomising participants to groups, but future studies would benefit from stratification, or minimisation, to equalise allocation proportions across groups. Blinding of care providers, outcome assessor and participants was also a weakness, risking detection and reporting bias. In future, where ethically and logistically possible, allocation concealment should be conducted. Lastly, confounding variables such as sociodemographic factors were not always reported, making it unclear whether groups were equally balanced at baseline, and unclear if there were differing outcomes for each demographic. Stratification or matching would benefit future studies to prevent issues around confounding. Dropout rates and subsequent disproportionate allocation of participants was an issue with two studies.37,40 One study was a feasibility study, 37 so this did not affect planned analysis, but a fully powered study is required before conclusions about its effectiveness can be drawn. Participants could be stratified by disease severity to reduce issues surrounding confounding variables. Intention to treat analyses could also reduce this issue. 40 Adding extra participants in the control group could reduce attrition bias, as it accounts for potential drop out due to lack of treatment.
Intervention
Most of the interventions included were delivered face to face, something now more challenging due to the ongoing Covid-19 pandemic. There has since been increased acceptability towards telehealth, not only minimising geographic barriers, but also improving accessibility for those with limited ability to travel to healthcare settings due to their endometriosis pain. 54 Therefore, adaptations may need to be made to current delivery methods, with increasing virtual delivery options where possible. This may reduce withdrawals and dropouts, an issue often faced in similar literature. 55
Outcomes
Effect sizes could not be calculated for one study. 41 One weak study 37 reported small to large effect sizes (d = 0.29–1.2), and the moderate studies38–40,42 also reported small and large effect sizes (d = 0.55–2.3). Larger effect sizes were reported for pain-related outcomes, compared with self-image outcomes, suggesting a stronger relationship between the interventions and their effects on pain than self-image. However, as two studies were of weak quality,37,41 and four of moderate quality,38–40,42 despite promising rationale, their effectiveness cannot be confirmed.
EHP-30
Four studies used the EHP-30 to gather outcomes.37–40 All showed statistically significant improvements. Acupuncture, 38 CHM 40 and yoga 39 provided moderate evidence that these interventions offer promise in improving ‘pain management’ and ‘self-image’ in endometriosis. Acupuncture had a total EHP-30 score, not subscales, but showed significant overall improvement (p = <0.001). Subscale scores for pain were significant in yoga (p = 0.0046) 39 and clinically important in CHM (>0.5 point change). 40 Subscale scores for self-image were significant in yoga (p = 0.0087) 39 and clinically important in CHM (>0.5 point change). 40
VAS/NRS
All studies showed improvements to pain levels on VAS/NRS scales,37–42 indicating the positive effects of such interventions. Acupuncture, 38 CHM, 40 yoga 39 and psychotherapy 42 provided moderate evidence that these interventions offer promise in improving pain management in endometriosis. Clinically relevant reductions were reported for period (31.5%), and intercourse pain (55.2%) in the CHM study, 40 global pain in the psychotherapy study (p < 0.001), 8 and reductions in pain in acupuncture (p < 0.001), 38 and yoga (p < 0.001). 39 However, the science and methodology behind these studies was not strong, therefore findings should be taken with caution.
Outcomes and their statistical significance were not all reported, with statistical analysis plans omitted in one study. 41 No studies reported effect size, and not all provided enough detail for it to be calculated either. Many lacked confidence intervals, suggesting a lack of statistical rigour, a challenge frequently observed in social science research. 52
Furthermore, Intention To Treat approaches should be used to account for missing data in the studies, and all patients included for randomisation accounted for when reporting the results. This is more reflective of a practical clinical scenario, accounting for deviation from the protocol and non-compliance, providing less biased estimates of treatment effects. Without this, the effects found are conflated. In endometriosis research, this approach can be useful to negate frequent issues surrounding high drop-out (70). Future research would benefit from including data on those just assessed for eligibility, to increase generalisability of trials.
Limitations
There were limitations to the review processes. To examine effects against control groups, only quantitative research was included. However, exploratory research on thoughts and feelings of participants may add useful insight into the intervention, and outcomes. The yoga study 39 conducted a complementary qualitative study, 56 where themes were established on participant’s expectations, physical/emotional state, pain management, and acquisition of self-knowledge. Participants did not refer to body image, focusing instead on pain management. However, it highlights a more comprehensive understanding that can be gained on the impact of interventions when a range of research methods are used.
The EPHPP Quality tool used in this review assessed internal and external validity of evidence. Overall intervention integrity, rating how many participants received the exposure of interest, and appropriateness of analysis, whilst documented, does not contribute towards the global rating of the papers. This risks the quality and effectiveness of assessed interventions being overstated.
Implications
Practice and policy
This systematic review built on the previous narrative review on complementary therapies and sexological concerns in endometriosis, 11 examining effectiveness of interventions on additional endometriosis facets, pain and body image. There were more randomised control trials available, and this review included only human participants, making findings more transferrable, as the previous review included animals. The results of this review could be considered alongside reviews of the effectiveness of surgical/pharmaceutical treatments. However, there remains a need for more high-quality studies in this field of research. This echoes earlier findings that lack of investment in the health of people born with female-assigned reproductive organs, has resulted in less being known about conditions affecting only these individuals, and the impact of such conditions. 20
Future research
The searches showed no papers examining the influence of social interventions in pain and body image, highlighting an area currently lacking in research and would benefit from additional focus in future. There was also limited evidence available from the included interventions to conclude the effects on body image. The self-image domain of the EHP-30 included questions on body appearance, confidence and clothing. However, the interchangeable use of self-image and body image terminology in the literature presents an issue when interpreting results and drawing conclusions. There are over 14 terms used to describe body image dimensions, 57 so describing the body image dimension to be investigated and targeted by the intervention is key. 58 This review defined body image as individual perceptions surrounding body size, attractiveness and associated emotions. Therefore, EHP-30 questions met the outcome of interest. However, future research with established, psychometrically strong body image scales, for example Body Image Scale (BIS) or Body Appreciation Scale (BAS), 59 is required to understand the body image dimensions in need of further investigation and intervention. More qualitative interventions are also required, to increase understanding of the impact and experiences of interventions on body image and pain, to increase patient choice.
Adapting interventions to be delivered remotely, particularly during the Covid-19 pandemic, is a priority, to increase patient choice, and offer solutions for accessibility. 52 This would require acceptability and feasibility trials first, but could enable wider demographics of participants to be included in research, potentially targeting existing challenges surrounding selection bias and confounders, found in this review. Remote delivery may also reduce issues around blinding, as demonstrated in studies utilising online intervention software. 60 To advance optimal treatment for endometriosis, research could benefit from examining intervention effects on multiple facets of endometriosis, 12 as research that does so, is still lacking.
There is also an absence of health psychology theoretical basis in the current literature. The COM-B model 61 considers the knowledge, capability, barriers, facilitators and motivators to making change. Therefore, creating interventions based on established health psychology models and theories could increase the likelihood of addressing psychological, behavioural and cultural factors potentially influencing health-related outcomes and quality of life of those with endometriosis.
Conclusion
Of the six biopsychosocial interventions included in this review, there were no strong quality papers on interventions using Acupuncture, Chinese herbal medicine, dietary supplementation, yoga and psychotherapy with somatosensory stimulation. Therefore recommendations based on intervention effectiveness cannot be made. To draw stronger conclusions on intervention effects on body image, future studies could benefit from using psychometrically tested valid and reliable standardised body image measures. Stronger quality evaluations, large enough to be suitably powered, with participants from wider demographics, and more specific outcome measures are required. Increased emphasis on health psychology theory, is also necessary to determine the effectiveness of these treatments on both pain and body image.
Footnotes
Data access
All studies included in this review are publicly available online, and further details on any of the above, can be obtained on request to the author.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The primary reviewer is a volunteer for Endometriosis UK, but otherwise, there are no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no financial support, funders or sponsors towards this review, as it was conducted as part of the first author’s self-funded Professional Doctorate in Health Psychology.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.