
Abstract
Introduction:
We aimed to appreciate the diagnostic and therapeutic journey of young women with endometriosis including disease presentation, obstacles to diagnosis and management, and impact on their life.
Methods:
We employed a mixed-method design, including chart review, 94-item questionnaire assembled from components of the EPHect EPQ-S and semi-structured interviews. The study setting was Kingston Health Sciences Centre in Kingston, Ontario. Participants were women under 28 years with severe dysmenorrhea. Questionnaire data was analyzed using descriptive statistics. Interviews were coded using the constant comparative analysis method by two analyzers and inter-rater reliability was calculated, then data were compared using a cross-sectional method.
Results:
Twenty-four participants were identified through chart review, 10 completed the questionnaire, and 5 participated in the interviews. Questionnaire participants, mean age 24.5 years ± 2.3, reported initial pelvic pain at a mean age of 13.9 years (SD 1.9). Fifty percent of participants have an endometriosis diagnosis, at a mean age of 19.2 years (SD 2.6). Three major themes emerged from our analysis. The journey with disease and therapy begins long before diagnosis and creates a culture of self-directed care. Lack of knowledge about endometriosis and women’s health by health care professionals and the public delays diagnosis and therapy. Endometriosis broadly impacts every aspect of an individual’s life.
Conclusion:
We found that young adults with severe dysmenorrhea and/or endometriosis present with symptoms at a young age. They encounter multiple obstacles in reaching a diagnosis and obtaining therapy. They often self-manage their pelvic pain and experience reduced quality of life.
Keywords
Introduction
Dysmenorrhea, defined as pain during menses, impacts up to 50%–90% of the female population1,2 and a profound negative impact on an individual’s quality of life.3–5 There are number of effective first line strategies that can help individuals manage dysmenorrhea, 6 including exercise, heating pads and anti-inflammatory medications.7–9 When such strategies are not effective, seeking medical care is appropriate and evaluation for potential pathological causes of dysmenorrhea should be undertaken. 8
Endometriosis, a multisystemic, chronic inflammatory condition stemming from the growth of endometrial like tissue outside the uterine lining is the next most common cause of dysmenorrhea, occurring in approximately 10% of reproductive aged females.10,11 Dysmenorrhea is the most common presenting symptom of endometriosis, however patients with endometriosis are also more likely to experience pain with intercourse, urinary or bowel movements, fatigue and infertility. 12 As such, endometriosis can have a profound negative impact across physical, psychological, social, interpersonal, sexual, educational, occupational, and financial aspects of individual’s lives.13–15 Despite the common prevalence of this condition, patients typically experience a diagnostic delay of 5–10 years. 13 During this time, individuals experiencing dysmenorrhea repeatedly suffer in pain and psychological distress, leading to development of chronic pelvic pain, depression, underperformance at school/work, and relationship conflict. 16 Agarwal et al. 17 states endometriosis is “nothing short of a public health emergency.” Too often severe pain is misdiagnosed and characterized as a “normal” part of puberty. 12
Many women have reported that prior to their diagnosis, doctors minimized their pain and normalized their menstrual experiences. 18 Part of the delay can be attributed to a lack of awareness and stigma about pelvic pain. 18 A study by Gupta et al. 19 had a focus group discussion with adolescents to investigate perceptions of endometriosis symptoms. They found key themes leading to less help-seeking behavior including that menstruation was stigmatized, symptoms were invisible, and adolescents felt unable to speak about painful intercourse. 19 These may be unique factors that contribute to the delay in diagnosis for adolescents. Since effective medical and surgical options exist for dysmenorrhea and endometriosis-related symptoms, 12 this delay in diagnosis leads to unnecessary suffering and needs to be addressed.
Dysmenorrhea is a significant cause of absenteeism and presenteeism (reduced productivity at work).20–22 Among adolescents, 12% have missed school or work due to dysmenorrhea. 20 One study estimated that 10.8 h of work are lost per week due to endometriosis. 21
The impact of endometriosis on adolescent quality of life remains understudied. Gallagher et al. 23 demonstrated that endometriosis patients scored significantly lower on physical and mental functioning compared to healthy controls. Given the disabling presentation of this disease, it is important to investigate how pain impacts quality of life and day to day functioning in this population.
It is clear that a knowledge translation gap exists, given the persistent delays in diagnosis and access to care in the face of well-established, evidence-based guidelines. 12 The primary objective of this study was to characterize the therapeutic journey of adolescents and young patients experiencing dysmenorrhea, using a mixed methods study design. This type of study design allows examination of a breadth of experience via the chart review and questionnaire, but also to probe deeper into the patient experience in order to understand where and how these barriers are encountered and overcome. 24
Methods
This study was conducted in Kingston Ontario, at Kingston Health Sciences Center. The study was approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (HSREB) (approval number #6029585).
A mixed-method study design was utilized, comprised of chart review, quantitative questionnaire data, and qualitative interview data. Mixed methods were utilized to provide the most comprehensive assessment of the experience of patients with dysmenorrhea and suspected endometriosis. Understanding the nature and magnitude of effect required insight from multiple analytic perspectives. Triangulation of all data from chart review, questionnaire, and interviews was performed at the end, finding inferences from the connections and relationships amongst all data ultimately leading to the points made in the discussion.
Persons younger than 28 years old with dysmenorrhea and/or suspected or diagnosed endometriosis were identified through a retrospective review of gynecology rosters at a tertiary hospital and eligible individuals were invited to complete an online questionnaire. This cut age off was selected due to the known delay of 5–10 years between presenting symptoms and attainment of specialist care. 23 We wanted to ensure that we were able to capture individuals’ experience from start of symptoms to seeking and receiving treatment.
Each participant was sent an invitation by mail that included a letter of information and link to the questionnaire. Two weeks later, participants received a follow up phone call. Participants were invited through July–September 2020. Informed consent was obtained online through review and acknowledgment of the informed consent form prior to questionnaire completion. Participants who completed the questionnaire were invited to complete a semi-structured phone interview in September or October 2020.
The 94-item questionnaire was assembled from components of the EPHect EPQ-S. 25 Sections included general health, personal information and lifestyle, medical history, pain, and menstrual history. Questionnaire data were analyzed using descriptive statistics.
Qualitative data was gathered and analyzed using a phenomenological lens. The researchers’ need to understand the particulars and the essence of participants’ lived experiences, and uncover the subjective nature of the participants’ life with disease, required active and deep listening with semi-structured interviews to be responsive to opportunities to probe in directions participants indicated were important to them and their experience. Researcher bias was remediated with (a) close attention to what the data offered, letting the data speak through a three-step process of constant comparison analysis 26 (b) having the same researchers who performed the interviews also analyze the data, and (c) additionally, complete an inter-rater reliability test. A last analytic action to increase trustworthiness of emerging qualitative themes involved a third senior researcher with extensive qualitative and mixed methods experience in a data and analysis audit to confirm relationships of data to themes.
Interviews (N = 5) were conducted over the phone by ALR with JM present for four of the five. Written and verbal consent for the interview was obtained. The interviews were approximately 30–45 min and were audio-recorded, with permission. Major topics covered included pelvic pain timeline, treatment, experience with pain, obstacles, impact of pain, and supports. Interviews were transcribed verbatim by ALR.
The inductive analytic process began with identifying open codes—words and terms that appear important to the topic of the study and the participants’ lives. Once a subset of the data was open-coded, inter-rater reliability was calculated using Scott’s index of inter-coder agreement on a third of the data set. 24 Inter-rater reliability was 92.1%. Thereafter, the rest of the data was divided between ALR and JM and open coding was completed. ALR and JM then worked together to group the codes into categories, which were further assembled into themes.
Results
Chart review
Twenty-four eligible patients were identified through chart review. The majority (16/24, 67%) of patients had visited the emergency department for dysmenorrhea or symptoms of endometriosis prior to their consultation with a gynecologist. Of these, 10 (42%) completed the study questionnaire and 5 (20.8%) participated in the interview.
Questionnaire results
Table 1 outlines the characteristics of participants completing the questionnaire. The mean age of participants completing the survey was 24.5 ± 2.3 years and mean BMI was 24.8 ± 5.1 kg/m2. Half of the participants were currently in school. Over 50% of the participants had attained a university or postgraduate degree. Most participants self-identified as white, were moderately active, and did not use tobacco or cannabis. The majority of participants (90%) did use alcohol. Half of the participants reported that they viewed their health as excellent or very good.
Characteristics of participants who completed the questionnaire (N = 10). All data presented as n (%) unless otherwise specified.
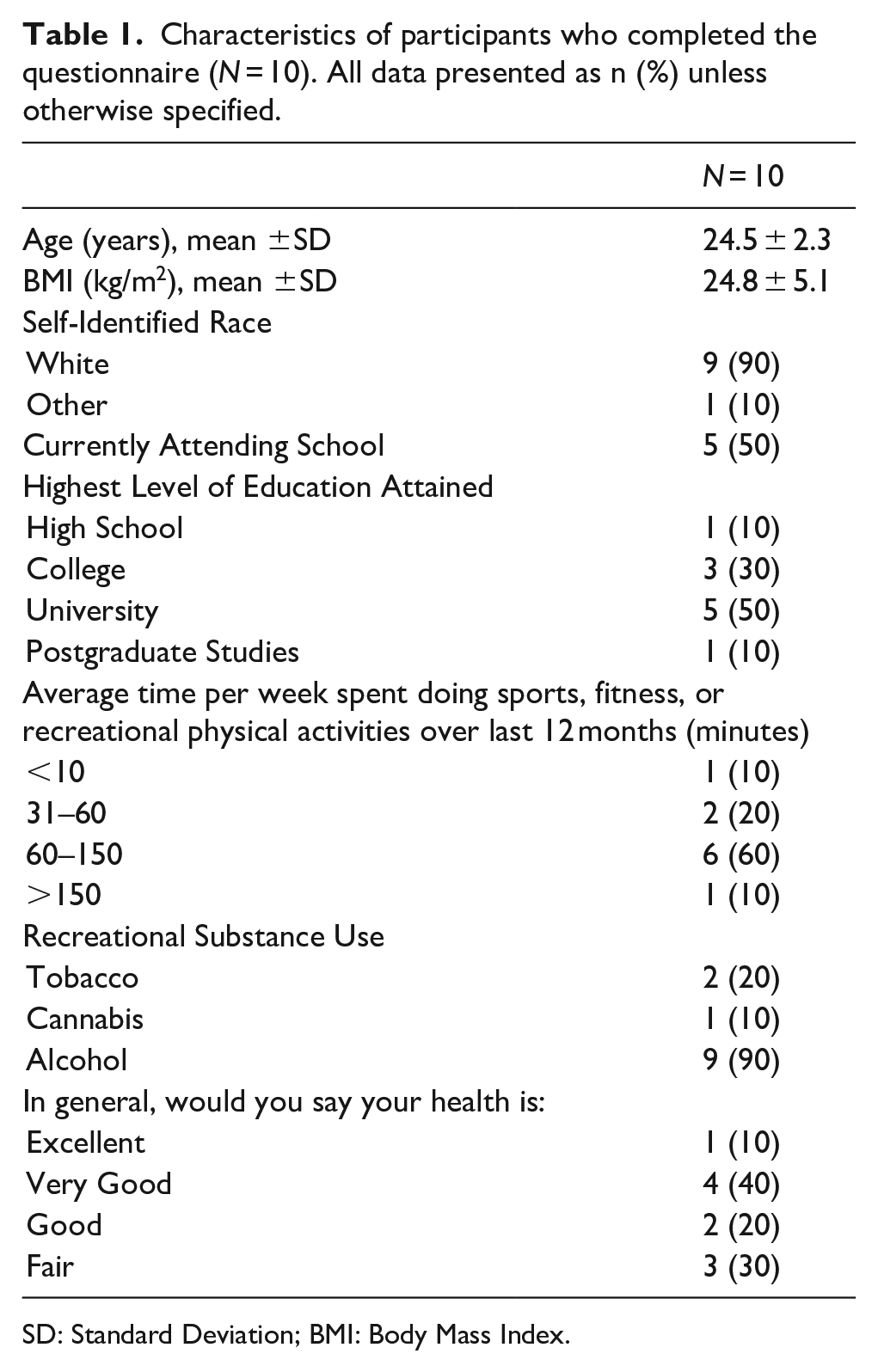
SD: Standard Deviation; BMI: Body Mass Index.
Table 2 outlines the diagnostic history, symptomatology and severity of disease experienced by questionnaire participants. Onset of pelvic pain was reported at a mean age of 13.9 ± 1.9 year. In the last 3 months, eight (80%) participants had pelvic pain during their periods, with an average pain score of 6.9 ± 2.7 when the pain was at its worst. Among these participants, most reported interruptions in their daily activities and requiring medications to treat the pain. Nine (90%) participants reported ever having pain during intercourse, with seven reporting that they have avoided intercourse due to pain. Four of seven describe quite a bit or extreme interference with sexual intercourse, and 6 said intercourse or orgasm make their pain worse. Five (50%) identified that they have an endometriosis diagnosis, diagnosed at a mean age of 19.2 ± 2.6 years.
Diagnostic history, symptomatology and severity if disease experienced by participants who completed the questionnaire (N = 10). All data presented as n (%) unless otherwise specified.
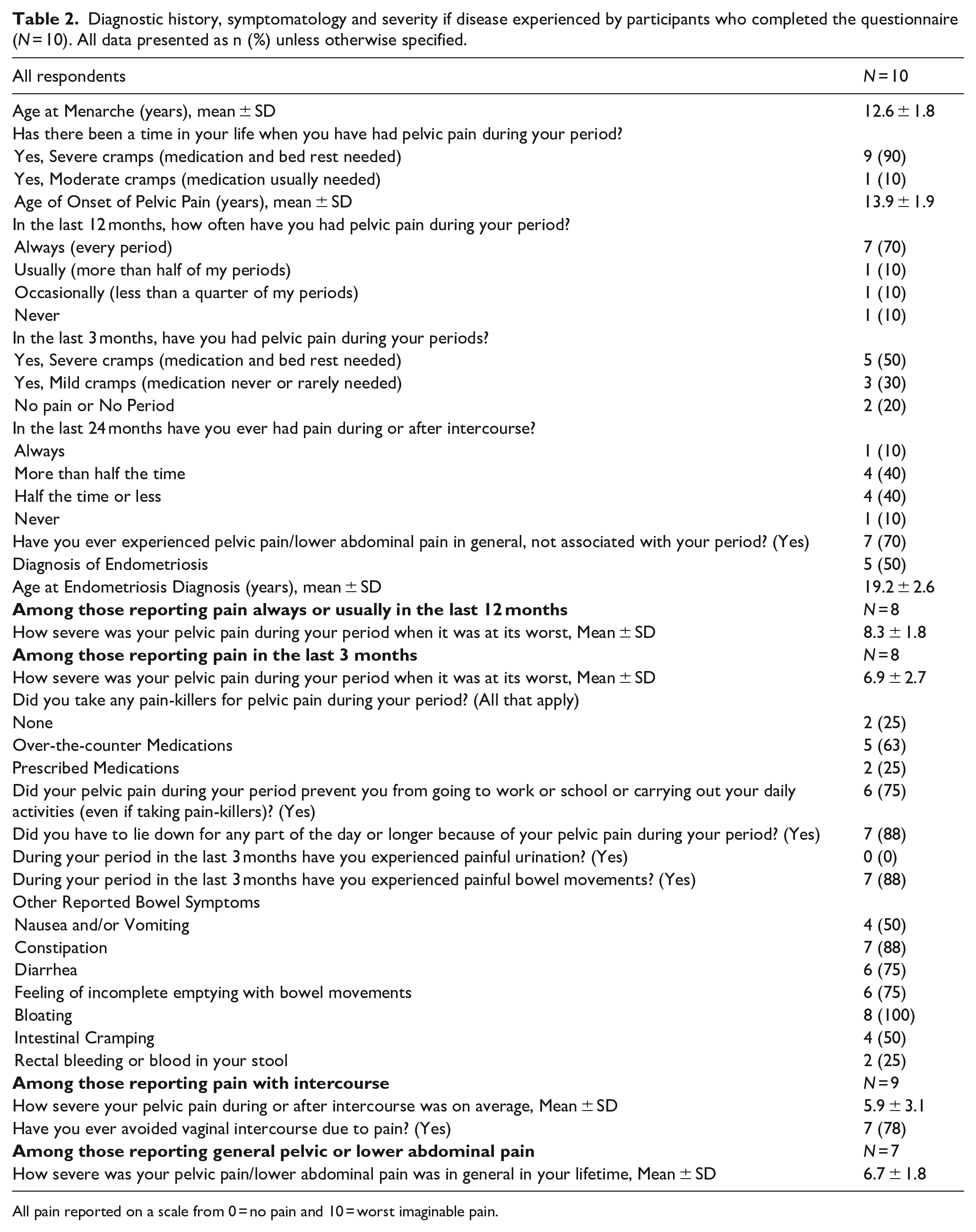
All pain reported on a scale from 0 = no pain and 10 = worst imaginable pain.
Participants were presented with 13 statements describing thoughts and feelings that may be associated with pain and were asked to indicate how often they have these thoughts or feelings when they are experiencing pain (Figure 1). 60% of respondents indicated always feeling or thinking that, “I become afraid that the pain will get worse,” and, “It’s awful and I feel that it overwhelms me.”
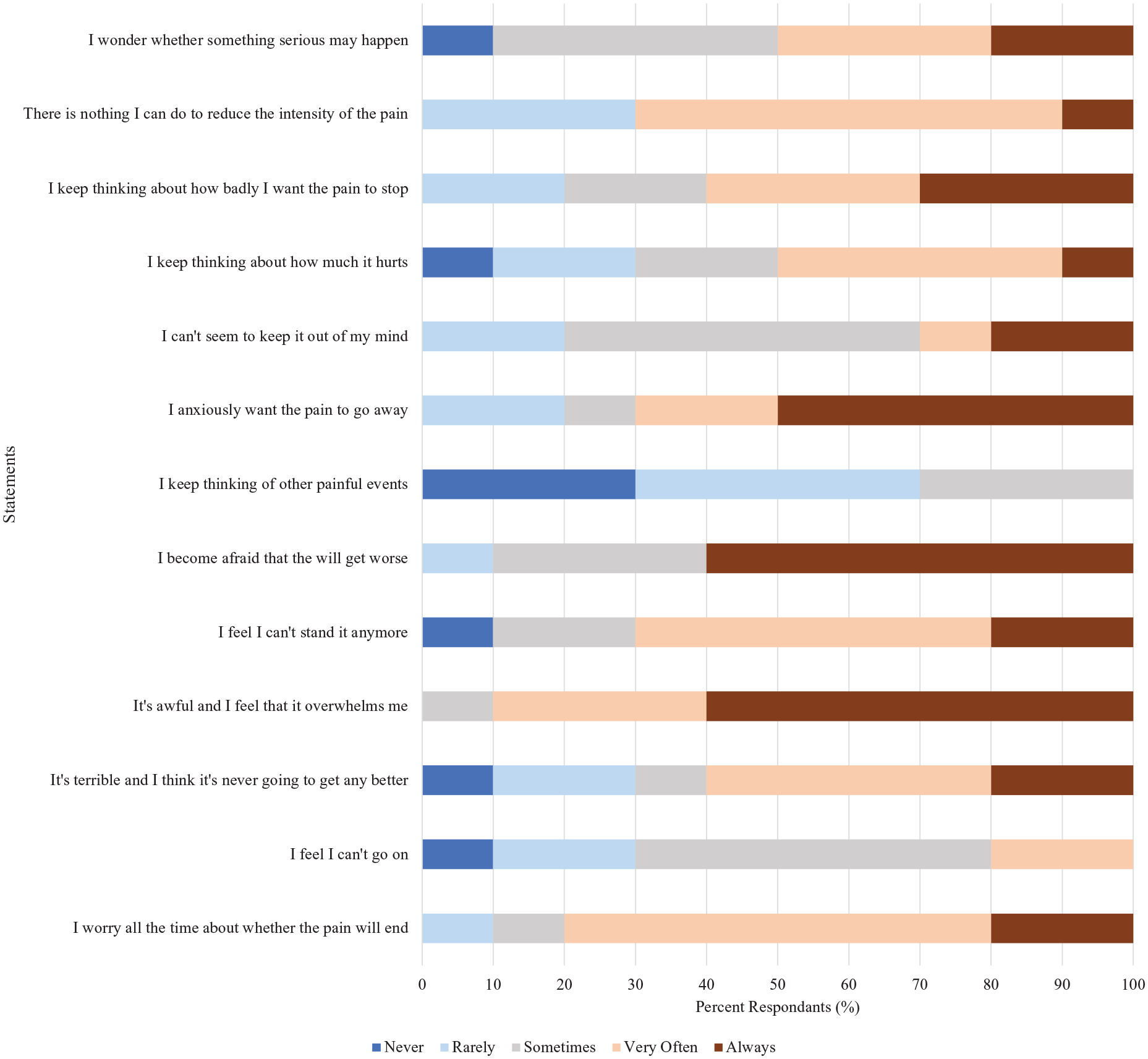
Thirteen statements describing different thoughts and feelings that may be associated with pain. Participant responses indicate how often they have these thoughts and feelings when they are experiencing pain (N = 10).
Participants who reported experiencing pelvic/lower abdominal pain that was not associated with their periods (N = 7) were asked to what extent this pain has interfered with activities such as sleep, work, and sports in the last 3 months (Figure 2). Most participants reported that the pain interfered extremely or quite a bit with their sleep and daily activities at home.
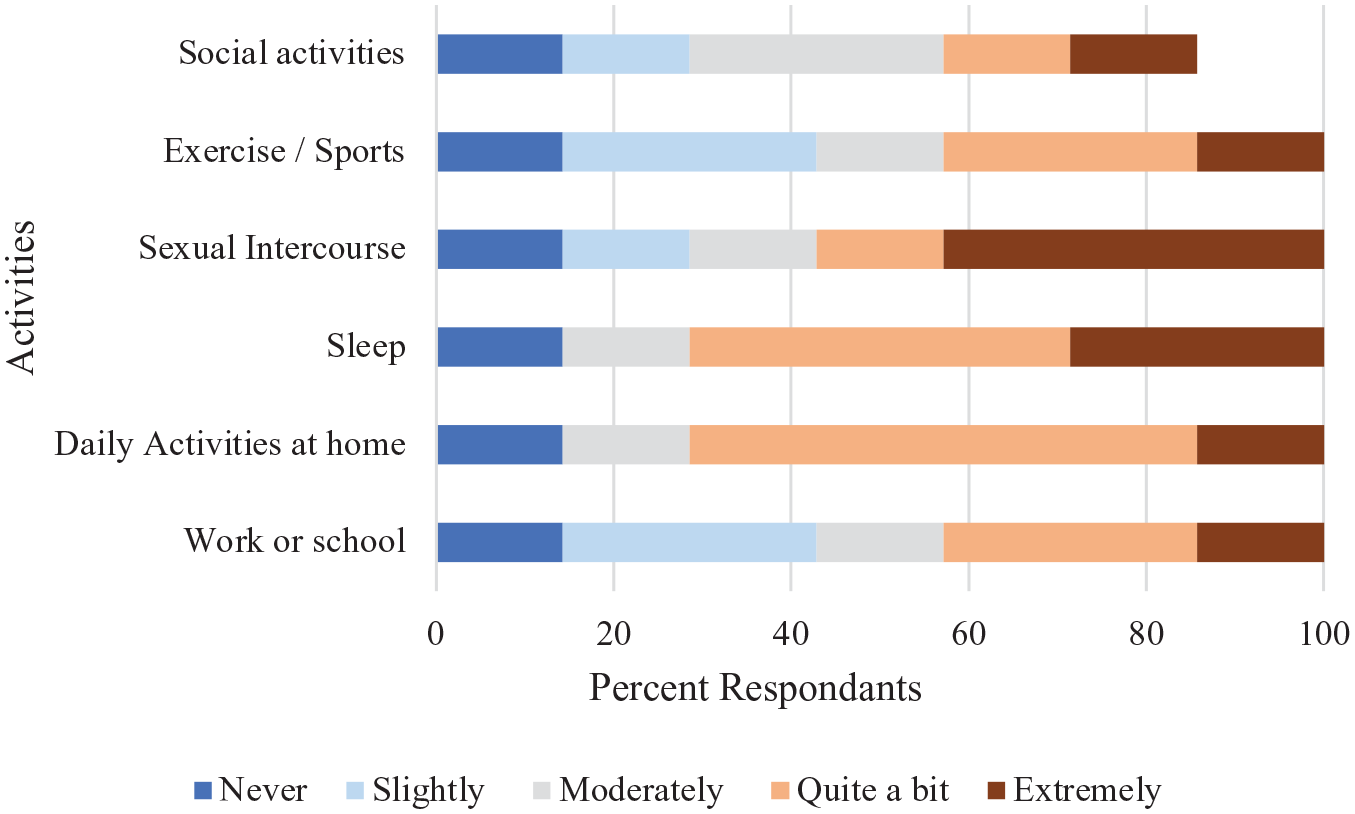
Among those participants who reported experiencing pelvic/lower abdominal pain that was not associated with their periods (N = 7). In the last 3 months, to what extent has your pelvic/lower abdominal pain interfered with each of the following activities? Activities included social activities, exercise/sport, sexual intercourse, sleep, daily activities.
Interview themes
Three major themes are supported by 14 categories (Appendix 1 ). First, endometriosis broadly impacts every aspect of an individual’s internal and external life. Second, lack of knowledge about endometriosis and women’s health by both health care professionals and the public creates delays for diagnosis and therapy. And third, the journey with disease and therapy begins long before diagnosis and creates a culture of self-directed care.
Endometriosis broadly impacts every aspect of an individual’s internal and external life
The omnipresent impact of endometriosis on individuals’ lives was confirmed by the participants in our study, who spoke of reduced quality of life, social isolation, cost, and the impact on work, school, sexual life, and important events. One of the unique psychological impacts captured in this study was the concept of “tolerating suffering as coping.” In discussing her pain, one respondent stated, “There is nothing I can do to make it fully go away. I’ve kind of accepted that.” The pain these participants were experiencing was not a level that they would choose to tolerate in the face of other options, hence it was deemed tolerating suffering, not simply pain. Participants also described the psychological turmoil caused by delay in diagnosis and what they perceived as persistent dismissive attitudes from health care providers, which generated feelings of self-doubt. When one participant’s symptoms were dismissed as normal, they described feeling, “Like I was absolutely losing my mind.”
Lack of knowledge about endometriosis and women’s health by both health care professionals and the public creates delays for diagnosis and therapy
One of the initial barriers to getting a diagnosis was encounters with primary care providers. Participants often faced skepticism. “I just wish they listened a little bit more instead of just dismissing it.” This contributed to the well-known delay in diagnosis of endometriosis for some of these participants and led to a distrust in the health care system and providers. “Doctors just tend not to help me.”
People with dysmenorrhea also lack support from their social circle and the public. As one participant described, “Yeah it would’ve been great if my family took me seriously [laughs]. When I was telling them about it- it was a lot of no you are just overreacting and that kind of stuff.” Participants identified frequently that this stemmed from lack of knowledge about endometriosis and normal menstruation by the general population.
The journey with disease and therapy begins long before diagnosis and creates a culture of self-directed care
With numerous delays in reaching a diagnosis from the medical system, participants with dysmenorrhea self-diagnose and self-manage. At some point, they realized the pain was pathologic, sometimes in comparisons with their peers. Participants described the insight they gained into their symptoms and responses to over-the-counter treatments. Participants reached a point of exhaustion with defending and grappling with their disease.
Participants described that having a knowledgeable care team, particularly one specializing in women’s health, led to more positive health care experiences. Participants expressed that having their health care providers believe their accounts and, furthermore, receiving a diagnosis, were significant steps toward healing. This was one of the several types of support found along the therapeutic journey, while others included support from family, friends, and the community of people suffering from endometriosis.
Of note, three of the five interview participants stated they had a diagnosis of endometriosis.
Discussion
People with endometriosis encounter significant barriers to timely diagnosis and effective management of their condition, leading to significant negative consequences to their physical and mental health, as well as quality of life. The burden of disease, including experience of pain during various activities, associated symptoms, and impact on quality of life is consistent with other studies exploring dysmenorrhea in adolescents and young adults. 23 Although we did not have a control group in our study, our findings were consistent with Gallagher et al. who demonstrated that adolescents and young adults with endometriosis had significantly lower physical and mental component summary in the SF-36 questionnaire compared to their peers. 23 Previous work has shown that depression and anxiety scores are higher and quality of life is impaired in those with dysmenorrhea; with the extent of each related to symptoms.27,28 Our findings also highlight the fact that patients with dysmenorrhea experience worry about their symptoms, ability to cope with pain, and that the pain will get worse. The range of psychological symptoms experienced with endometriosis and other chronic pain disorders is not limited to anxiety and depression, but also psychological stress. 29 While a measure of stress like the PROMIS scale 29 was not used in this study, future research should consider its use. It is important to health care providers caring for young patients experiencing dysmenorrhea to ask regarding comorbid psychological symptoms. They should also appreciate that these are related to symptoms severity. Providers should appreciate that patients may be particularly worried about the management of their pain symptoms, and ensure this concern is addressed.
Our mixed methods study of adolescents’ therapeutic journey with dysmenorrhea identified important themes that can be used to help health care providers tailor their approach to care for these patients to improve outcomes. Similar work by Allyn et al., who sought to understand the impact of dysmenorrhea in adolescents identified two main themes: (1) dysmenorrhea affects the whole person and (2) coping mechanisms of patients include passive and active coping strategies. 5 These themes complement our findings, highlight importance of consideration of these themes in providing patient care. More recent work by Wren and Mercer, who focused specifically on the diagnostic experience of young patients with endometriosis, identified the themes of “the pursuit of a diagnosis,” “adjusting to a new normality” and the “importance of effective support.” 30 Our study describes some of the adjustments that young people experiencing endometriosis make as they await their diagnosis and how they adjust—similar to patients with other chronic diseases, people with endometriosis become very proficient in self-management. They learn to respond to symptomatic cues, assess how much relief they receive from therapy, and organize their school and work lives to accommodate their disability. Although many healthcare providers will initiate treatment of dysmenorrhea prior to establishing a definitive diagnosis of endometriosis (or exclusion of such) in keeping with clinical care guidelines,8,12 our work suggests that this may indeed result in patient confusion and frustration.
One barrier to effective care that our participants report was lack of health care provider knowledge regarding care and investigations for patients presenting with dysmenorrhea. Primary care providers are often the first point of access for patients. In this study, 70% of participants had presented to the emergency department before accessing specialist care. Education regarding first line management of dysmenorrhea, when to consider secondary causes of dysmenorrhea, and when to refer would be valuable to primary care and emergency providers.
Strengths
There were several strengths to our study. We believe our study is part of an emerging methodological choice for research to explore adolescent endometriosis and/or severe dysmenorrhea from a mixed method perspective. The methodology allowed us to do a comprehensive assessment of the experience of patients with dysmenorrhea and suspected endometriosis. It emphasized that severe pelvic pain in the adolescent population continues to be normalized and one contributing aspect is lack of knowledge at the primary care level. Novel themes included that the delay in diagnosis leads individuals to become very proficient in self-management of their disease. Finally, the impact of the disease is akin to other chronic diseases, therefore endometriosis requires the same level of attention and therapy.
Limitations
The results of our study must be interpreted in the context of study design. First, we had a small sample size. However, it remains an important examination of the experiences of young women with severe dysmenorrhea and endometriosis and the impact on their lives. Last, our sample was from a single academic center and 9 of 10 participants were white so this data may not represent the experiences of racialized people and communities.
Conclusion
This study confirmed that endometriosis broadly impacts every aspect of an individual’s life. Specifically, participants reported mental health impacts such as tolerating suffering as a coping mechanism, feeling dismissed, and that this leads to feelings of self-doubt. Public ignorance of women’s health issues including endometriosis also creates delays to diagnosis, with barriers to diagnosis in the Netherlands recently described by van der Zanden et al. 31 Primary care providers, including emergency providers, would therefore benefit from education on recognizing potential presentations of endometriosis such as the recent guide published by Nadeau et al. 32 Establishing referral networks would also overcome barriers for patients to access specialist and decrease the delay in diagnosis. People with endometriosis have significant expertise in managing their illness due to long delays in diagnosis and adequate treatment and should be seen as a key member of their treating team.
Footnotes
Appendix
Themes and categories.
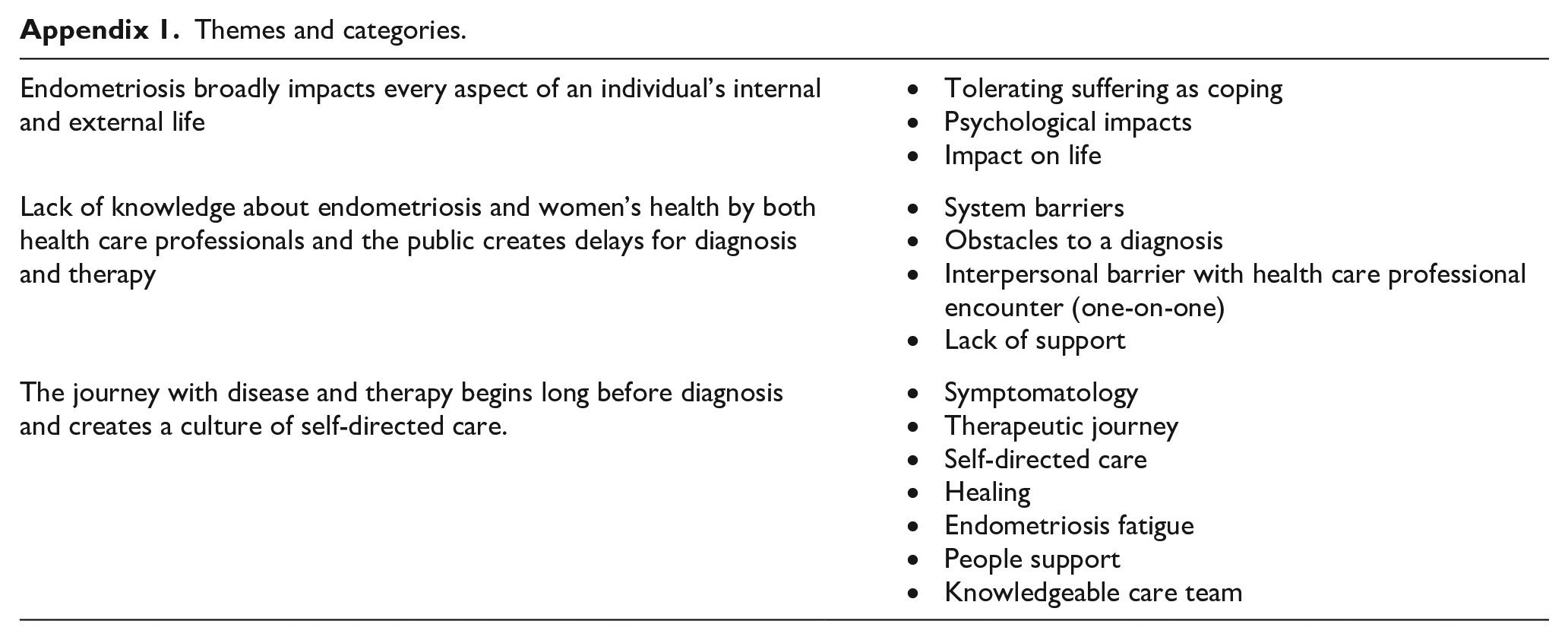
| Endometriosis broadly impacts every aspect of an individual’s internal and external life | • Tolerating suffering as coping • Psychological impacts • Impact on life |
| Lack of knowledge about endometriosis and women’s health by both health care professionals and the public creates delays for diagnosis and therapy | • System barriers • Obstacles to a diagnosis • Interpersonal barrier with health care professional encounter (one-on-one) • Lack of support |
| The journey with disease and therapy begins long before diagnosis and creates a culture of self-directed care. | • Symptomatology • Therapeutic journey • Self-directed care • Healing • Endometriosis fatigue • People support • Knowledgeable care team |
Study conducted: Kingston, ON Canada
Study presented: SOGC Annual Clinical and Scientific Conference on June 2021 (virtual)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.