
Abstract
Introduction:
Endometriosis is a burdensome chronic disease that can be difficult to diagnose, yet few studies examine experiences along the continuum of disease state. We sought to explore women’s journeys to an endometriosis diagnosis, experience with endometriosis pain, and interactions with healthcare practitioners.
Methods:
An anonymous 23-question online survey was distributed to women (aged >19 years) who self-identified as having a surgical or nonsurgical diagnosis of endometriosis and living in seven English-speaking countries through the social media network MyEndometriosisTeam.com.
Results:
From January through April 2018, 317 women in the United States and 134 women outside the United States completed the survey. More than 50% of the women waited 6 or more years for a diagnosis of endometriosis. Overall, 54.3% experienced endometriosis-related pain daily. Respondents (US/non-US) reported a significant impairment in quality of life that interfered with their family (45.7%/45.5%) and social life (40.1%/44.0%), education/career (42.9%/46.3%), and sexual function (68.1%/70.1%). Women reported their disease led to other conditions, including fatigue (93.6%), gastrointestinal issues (91.8%), and difficulty sleeping (87.4%). Many women were not satisfied with their practitioner’s ability to listen to concerns and felt that their practitioner’s treatment recommendations lacked consistency with their own goals/needs.
Conclusion:
Women still experience long delays and difficult journeys to an endometriosis diagnosis. Disease-associated pain is pervasive and has direct and indirect impacts on quality of life. Women are frequently not satisfied with disease-management options presented to them by their practitioners. These results suggest a need for improved medical education on disease state for both patients and practitioners.
Introduction
Endometriosis is a chronic gynecological disorder, affecting approximately 10% of women.1–5 Dysmenorrhea, chronic pelvic pain, and dyspareunia are common symptoms of endometriosis; however, the disorder can also be accompanied by other symptoms, including subfertility and menorrhagia. 6 Many endometriosis symptoms, including menstrual pain, chronic pelvic pain, bloating, changes in bowel frequency, and urgency and urinary frequency are described by patients with other pelvic conditions, such as irritable bowel syndrome, interstitial cystitis, or urinary tract infections.6–8 This symptom overlap can make endometriosis difficult to diagnose; therefore, patients may experience long delays before receiving and initiating treatment.8–16
The high burden of endometriosis is comparable to other chronic diseases. 17 Endometriosis-related pain can negatively impact a woman’s mental and physical health, leading to decreased quality of life (QoL) and interfering with the ability to function socially and professionally.12,18–20 Endometriosis-related pain and symptoms may cause women to miss work17,21,22 and may contribute to substantial losses in productivity in the workplace and at home. 23
Given the devastating burden of endometriosis, it is critical to identify new avenues to improve patients’ well-being and QoL while they live with the disease. Reports from recent investigations in fertility care24,25 and endometriosis 26 suggest that healthcare practices that are responsive to individual patient needs/values may improve patients’ overall QoL. Despite the importance of patient-centered care, few studies have examined patients’ perspectives on the endometriosis burden and the care received outside research settings. 27 Recent investigations provide important leads that can inform patient-centered endometriosis care. For example, quicker diagnosis may help women feel validated and empowered,28,29 and effective communication with their practitioners could help women manage the endometriosis burden. 30 Although informative, most existing studies examining the patient’s experience with endometriosis to improve patient-centered care use small sample sizes with little geographic diversity. 27
Understanding patients’ pain experiences, journey to diagnosis, and perceptions about interactions with practitioners may help clinicians better inform patient-centered healthcare and avoid diagnostic delays. Therefore, we designed a multicountry survey to describe what patients report regarding their journey from symptom onset to eventual diagnosis. We specifically wanted to determine the (1) length of time that it took for patients to receive a diagnosis of endometriosis; (2) number of conversations had with practitioners about symptoms; (3) number and types of diagnoses received before endometriosis; (4) experience with endometriosis-related pain, severity, and impact of pain on QoL; (5) satisfaction with practitioner interactions; and (6) personal goals for endometriosis treatment and consistency of these goals with practitioner goals.
Methods
An online survey was conducted from 31 January through 15 April 2018. The survey was developed by AbbVie and MyHealthTeams, a company that creates social networks for people living with/caring for someone with a chronic condition with the purpose of providing a safe place for people to discuss/share information about their disease and experience a sense of community/support among people with similar chronic conditions. One of the MyHealthTeams social networks—MyEndometriosisTeam.com—was created specifically for women living with endometriosis. MyEndometriosisTeam.com has over 74,000 members from 13 countries.
Survey development
Survey questions were based on a review of organic discussions between women on MyEndometriosisTeam.com about their journeys with endometriosis-related pain and the challenges they faced in obtaining a correct diagnosis. Examples of comments posted in the MyEndometriosisTeam.com forum chats are provided in Figure 1.
Representative comments posted during organic conversations in the MyEndometriosisTeam.com forum chats.
From these discussions, we identified medical gaps (e.g., delays in diagnosis) and topics of continuous interest (e.g., pain) that we used as a starting point to develop the survey questions. The final survey contained 23 questions about women’s experiences with endometriosis.
Most survey questions were closed ended, and participants were provided answer options from which to choose. Some questions were partially closed ended and allowed subjects to provide additional symptoms, pain triggers, or details not included in provided answer options. Survey questions and answer options are provided in Supplementary Material 1. Standard practice for pretesting a quantitative questionnaire consists of reviewing the tool during a telephone interview or in-person interview with 3–5 relevant stakeholders (e.g., diagnosed patients) to gain feedback on clarity and relevance of the questions. Before finalization, a pilot survey was provided to five women living with endometriosis (sample population) who had laparoscopic diagnosis of endometriosis and who were not part of the social network but based on demographic data were representative of MyEndometriosoisTeam.com participants as a whole.
Participant eligibility and recruitment
Participants for the survey were recruited through MyEndometriosisTeam. Members of this social network received email invitations, and additional participants were solicited via invitations posted on the MyEndometriosisTeam public Facebook page. Participation in the survey was limited to women who were at least 19 years of age who self-identified as ever receiving a surgical or nonsurgical endometriosis diagnosis. The survey was administered to women in the United States and six other English-speaking countries (Australia, Canada, Ireland, New Zealand, South Africa, and the United Kingdom). The US portion of the survey was approved by the Advarra Institutional Review Board (Columbia, MD). Survey respondents anonymously opted in to participate and provided written consent to participate in the research before survey questions were administered.
Survey analysis and sample size
Responses from women in the United States were analyzed separately from responses from the other countries. Descriptive statistics were used to tabulate responses to the survey. Two-tailed Student’s t-tests with a 95% confidence significance level (α = 0.05) were used to identify response differences between respondents in the US and respondents in non-US countries.
We performed a post hoc sample size evaluation to determine whether our sample is representative of the population of women living with endometriosis. Based on an estimate of 176 million women in the world living with endometriosis, 31 we calculated that to obtain a representative sample (±5% margin of error, 95% confidence level, and 10% response rate) 3850 women would need to be invited to participate to yield a required sample size of 385 surveys. Thus, we believed our final sample size of 451 respondents was an adequate representation of this population.
Results
Survey response
The survey was emailed to approximately 28,000 women. Sixteen percent of women opened the email, and 10% of these completed the survey. Of 451 responses, 317 (70%) were from the United States and 134 (30%) from outside the United States (United Kingdom: 54; Australia: 22; South Africa: 21; Canada: 16; New Zealand: 12; and Ireland: 9). Respondents ranged in age from 19 to over 60 years, with almost half of respondents (46.7% US, 47.8% non-US) between the ages of 30–39 years. A large proportion of the respondents (43.8% US, 39.6% non-US) self-reported having Stage 3 or 4 disease (Table 1).
Demographics and women’s paths to diagnosis.
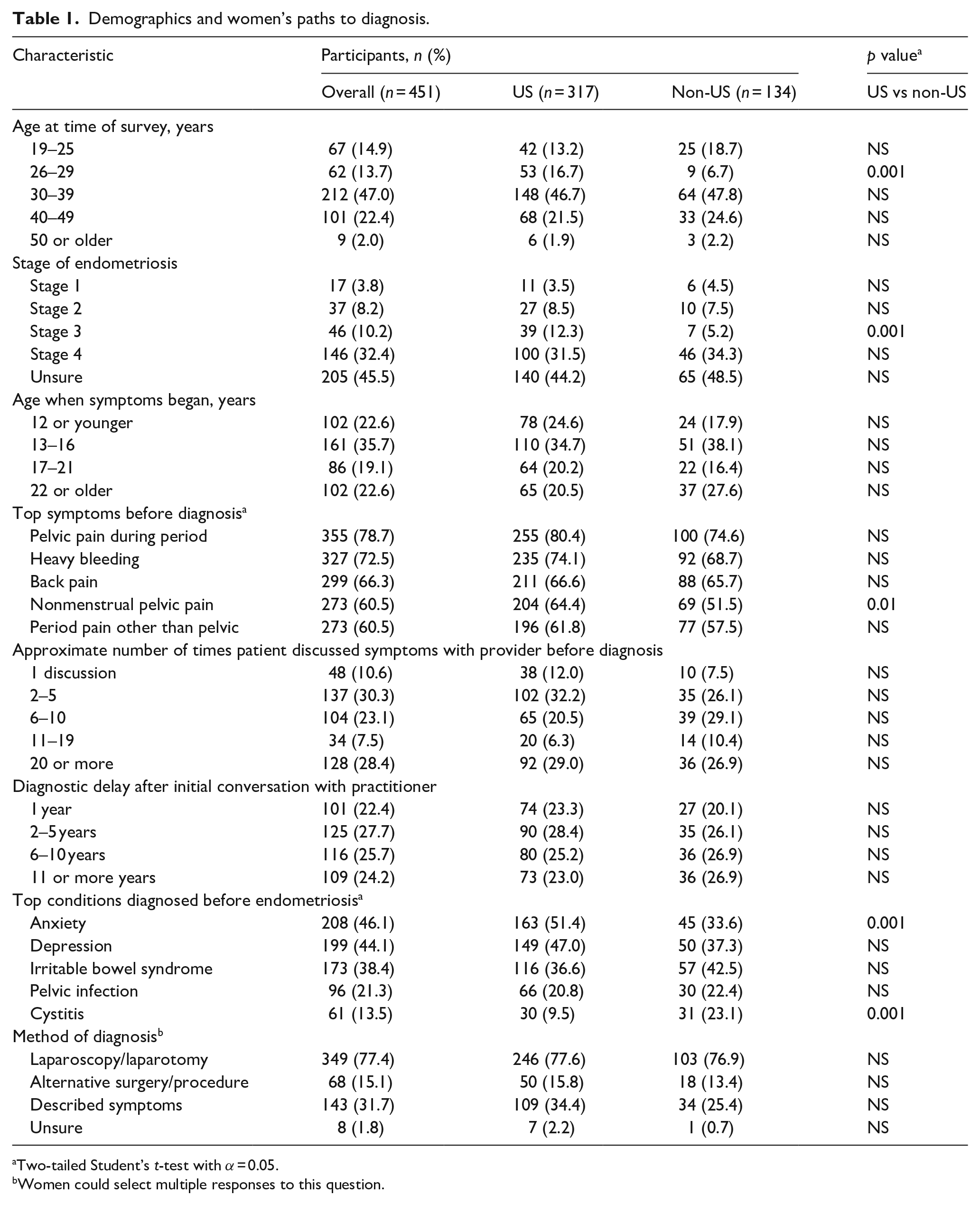
Two-tailed Student’s t-test with α = 0.05.
Women could select multiple responses to this question.
Women’s paths to diagnosis of endometriosis
Clinical presentations of endometriosis
Most respondents (59.3% US, 56.0% non-US) began experiencing endometriosis symptoms by the time they were 16 years old (Table 1). Most women reported menstrual pain and heavy bleeding among symptoms that made them seek a diagnosis. Women most commonly reported seeking a diagnosis when the severity of their pain limited their daily activities (86.4% US, 84.3% non-US). They also reported seeking medical help when pain severity impacted their mood (68.5% US, 60.4% non-US), their pain was nonstop (63.1% US, 47.8% non-US), they experienced pain during sex (57.1% US, 42.5% non-US), or they required prescription painkillers (44.8% US, 47.0% non-US).
Diagnosis of endometriosis
Many women reported having ⩾20 conversations about their symptoms with a practitioner before receiving a diagnosis (Table 1). Roughly half (48.3% US, 53.7% non-US) reporting that it took ⩾6 years from the initial conversation with a practitioner about their symptoms until a diagnosis of endometriosis. Many respondents were diagnosed with other conditions like anxiety, depression, or irritable bowel syndrome before their endometriosis diagnosis (Table 1). Women who indicated that they experienced many endometriosis symptoms were also more likely to experience a diagnostic delay.
Most respondents (82.6% US, 77.6% non-US) received their endometriosis diagnosis from a gynecologist. When asked to identify which methods their practitioner used to diagnose their disease, 77.6% US respondents and 76.9% of non-US respondents stated laparoscopy/laparotomy.
Women’s experiences with endometriosis-related pain
All endometriosis-related pain
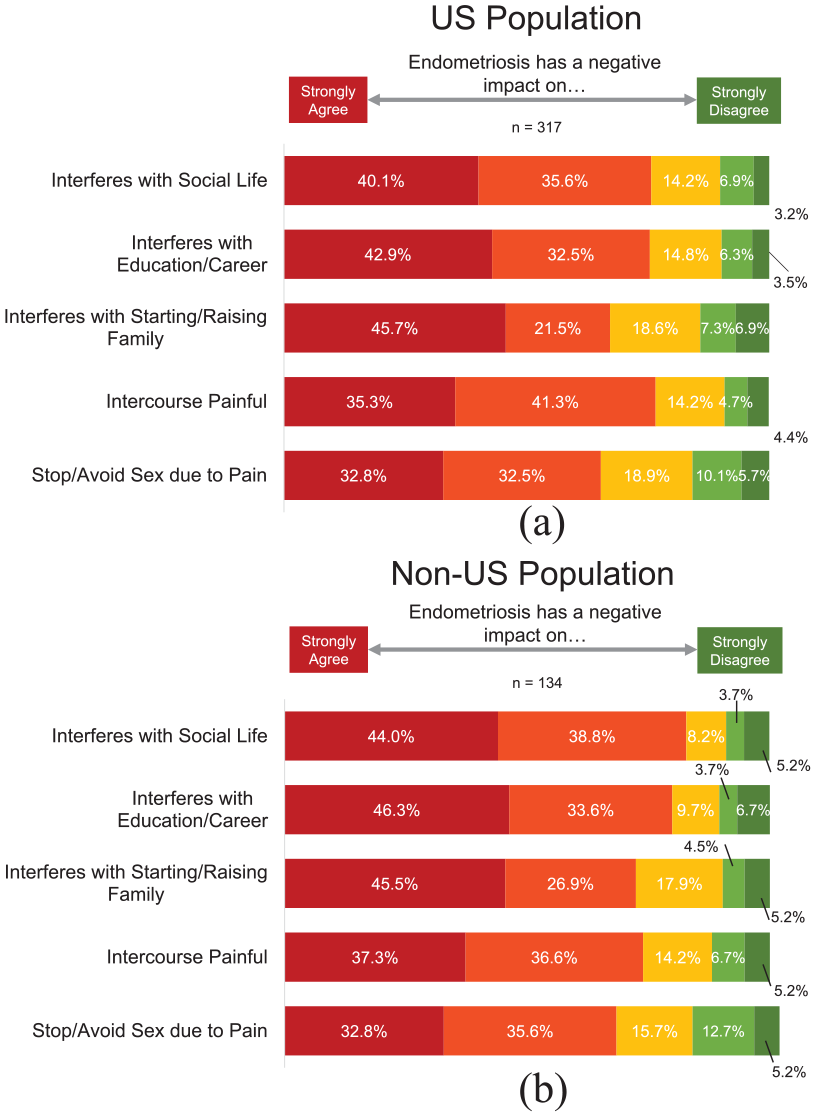
Women reported experiencing back pain, nonmenstrual pelvic pain, and pelvic pain during periods (Table 2). Respondents also reported experiencing endometriosis-related pain daily while other women stated they experienced pain on a weekly basis. Many reported experiencing fatigue, gastrointestinal issues, and difficulty sleeping. Most women either “strongly agreed” or “agreed” that endometriosis had a widespread negative impact on their social life, education/career, or starting or raising a family (Figure 2). Women similarly indicated that painful intercourse impacted their sex life. Women stated several different triggers for this pain, including menstruation, time just before menstruation, or sexual intercourse.
Women’s experience with endometriosis pain.
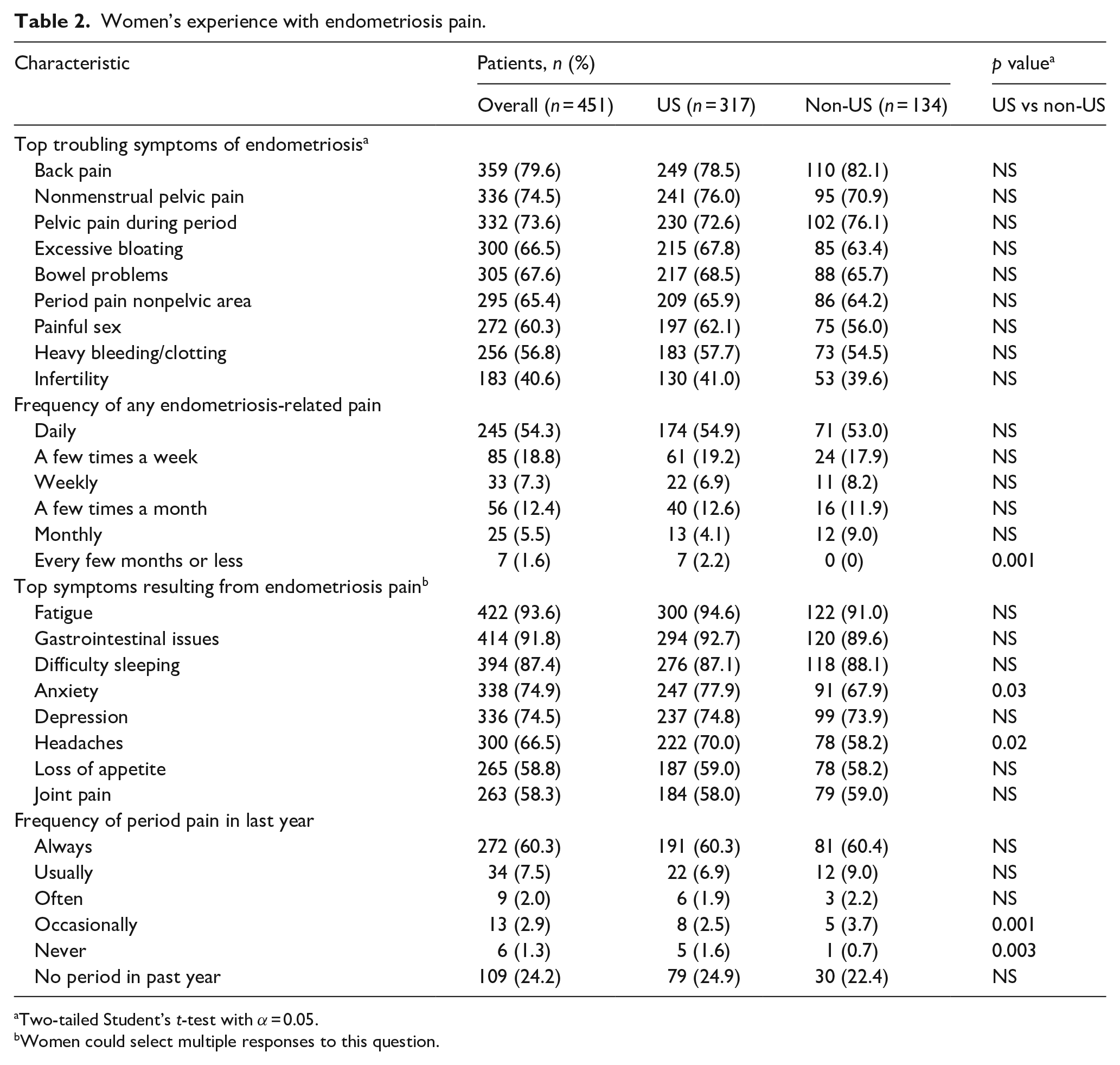
Two-tailed Student’s t-test with α = 0.05.
Women could select multiple responses to this question.
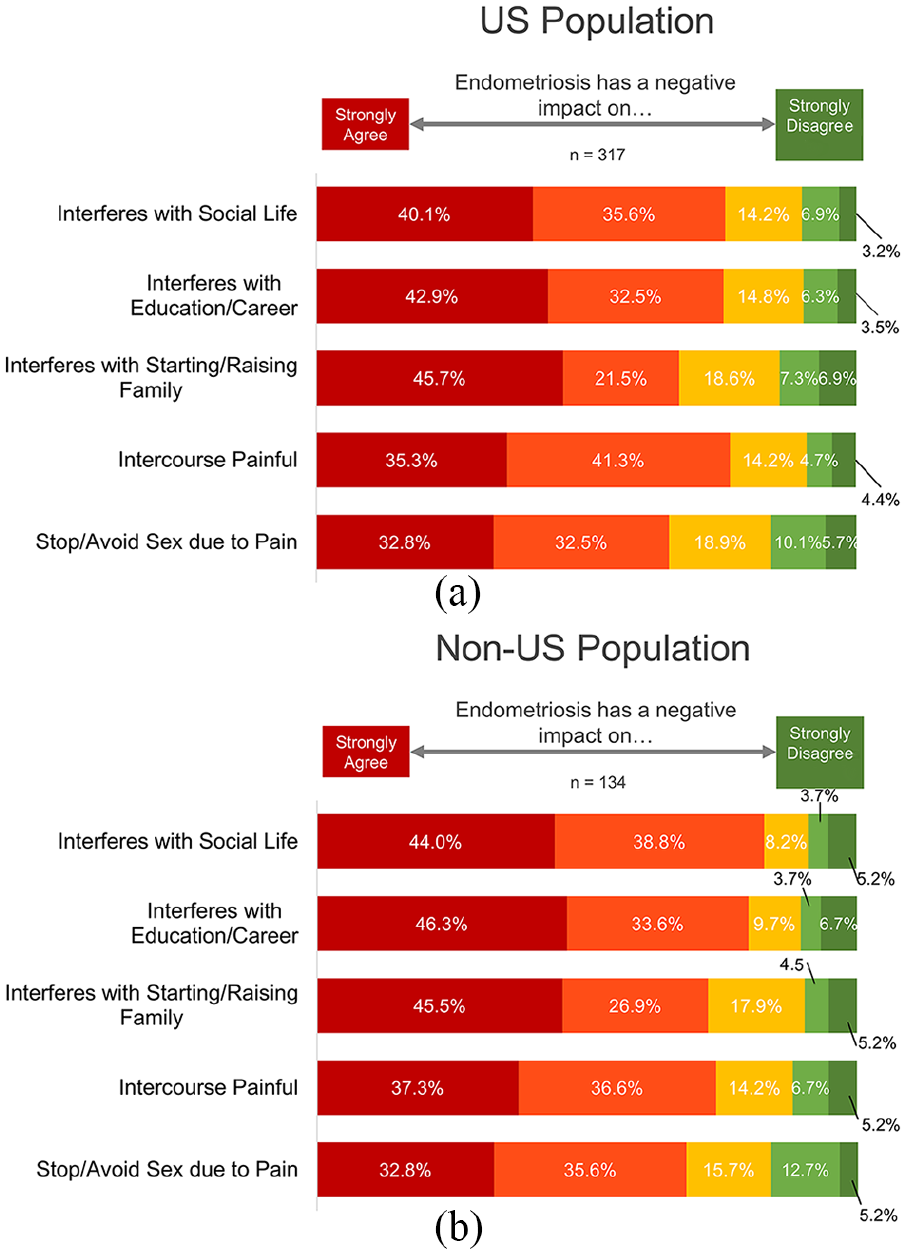
Negative impact of endometriosis pain on various aspects of quality of life. Respondents in the (a) US population and (b) non-US population were asked to indicate how much they agreed or disagreed their endometriosis interfered with their social life, education/career, starting/raising a family, caused painful intercourse, or made them stop or avoid sex due to the pain.
Menstrual-related pain
Among those who experienced menstrual-related endometriosis pain, the pain was severe cramps (77.3% US, 76.1% non-US) or moderate cramps (16.4% US, 19.4% non-US). Most respondents (86.8% US, 87.1% non-US) experienced menstrual-related endometriosis pain at 16 years of age or younger. The majority of respondents who experienced menstrual-related pain stated they always had this pelvic pain during their periods (Table 2). Over 85% of women indicated that the severity of their menstrual-related pelvic pain was greater than 7 on a scale of 0 (no pain) to 10 (worst imaginable pain) (Figure 3).
Severity of pelvic pain during periods rated by women on a scale of 0–10. Respondents who had a period in the last 12 months were asked to rate how severe their pelvic pain during their period was at its worst in the last year. Percentages below 5% are not labeled on the graph.
Women’s experiences with healthcare practitioners and treatment
Most respondents (73.8% US, 48.5% non-US) reported receiving endometriosis treatment from a gynecologist, although many women outside the United States also received treatment from a family practitioner (5.0% US, 32.8% non-US). A majority of respondents (61.5% US, 69.4% non-US) were not satisfied with how well their practitioner listened to their concerns surrounding endometriosis (Figure 4(a)). Similarly, most women (64.7% US, 77.6% non-US) indicated that practitioner treatment recommendations were “somewhat consistent,” “not very consistent,” or “not at all consistent” with their own goals and needs (Figure 4(b)). Women cited intolerable medication side effects (51.7% US, 45.2% non-US) and treatments that delay (36.6% US, 42.3% non-US) or prevent (28.3% US, 18.3% non-US) pregnancy as the most common ways their doctor’s treatment priorities were not consistent with their own needs.
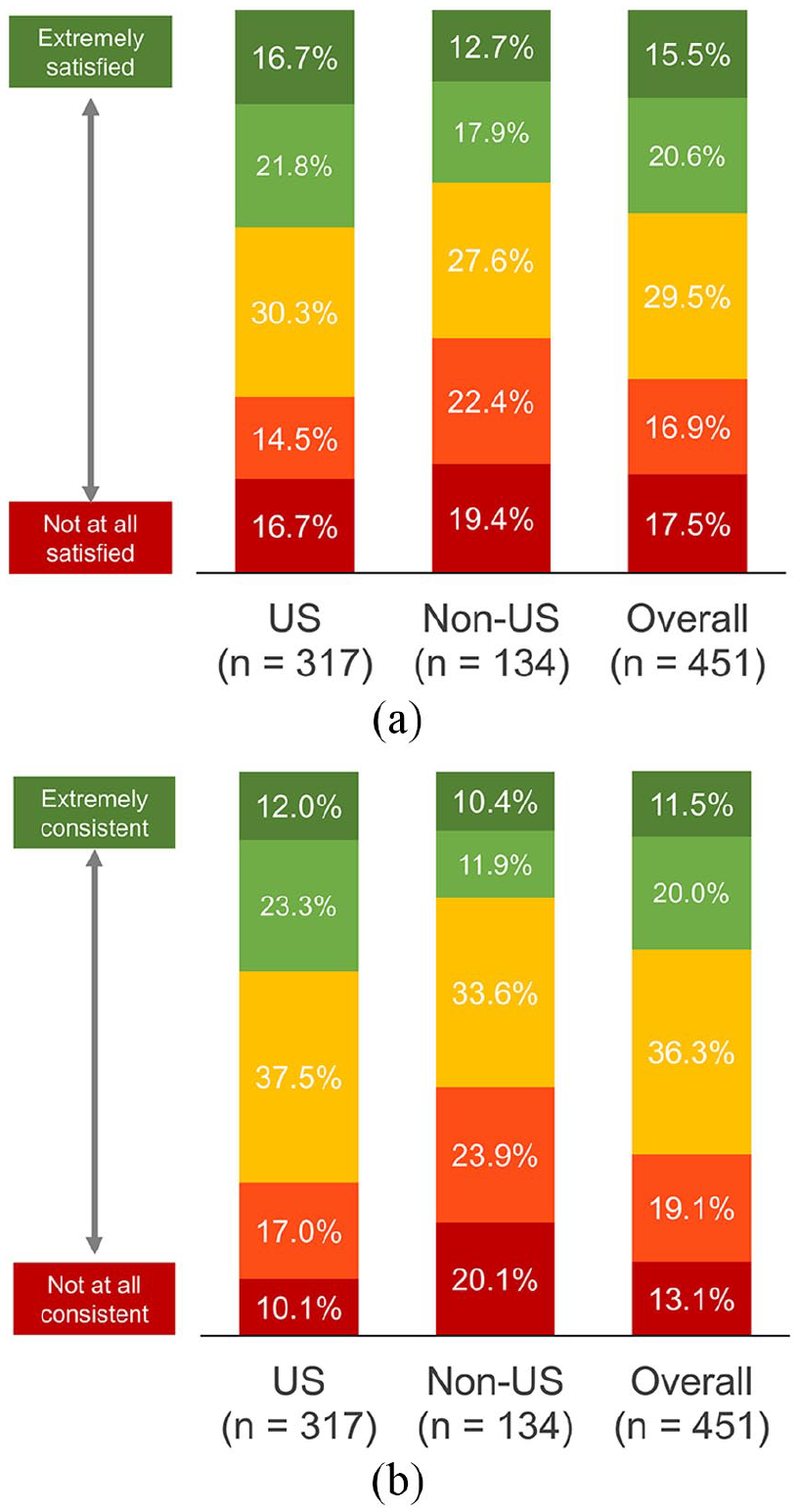
Patient satisfaction with healthcare practitioners. Respondents were asked to rate (a) their overall satisfaction with how well their healthcare practitioner listens to concerns regarding endometriosis, and (b) to what degree their practitioner’s treatment recommendations were consistent with their own goals and needs.
Discussion
In general, surveyed women described having negative experiences characterized by lengthy time to diagnosis, multiple conversations with their healthcare practitioner before a diagnosis, receiving other diagnoses before endometriosis, various severe pain symptoms and significant QoL impairment, poor satisfaction with healthcare provider interactions, and poor consistency between their treatment goals and the practitioner’s goals. Specifically, women noted long time intervals and having many discussions with practitioners before receiving a diagnosis of endometriosis. This finding is consistent with a host of studies demonstrating that women with endometriosis tend to experience some degree of diagnostic delay,8–16 comparable with the gap of ⩾6 years observed in this survey. On the other hand, results from a recent study supported a downward trend in delays in endometriosis diagnosis, possibly driven by improved public and physician disease awareness. 9 Respondents who started experiencing symptoms at younger ages seemed to experience longer diagnostic delays than did the general sample of respondents, with a majority of US respondents who started feeling endometriosis symptoms by age 13 reporting it took ⩾11 years to receive a diagnosis compared with the delay of ⩾6 years observed in the general sample. This finding is consistent with discoveries from a number of previous reports suggesting that younger women experience extended diagnostic delays compared with older women.9,11,16 This overall trend is thought to be partially associated with younger women being less familiar with endometriosis and its symptoms, 32 seeking treatment from pediatricians or clinicians who may not be as familiar with endometriosis, not having their symptoms taken seriously by their doctors, or not being able to differentiate between a “normal” and “abnormal” menstrual experience.9,16
Women who had many conversations with practitioners before their endometriosis diagnosis also indicated experiencing a higher number of symptoms than did women who were diagnosed after only one conversation. This finding is consistent with results from an earlier study that found a positive association between delayed diagnosis and the number of pelvic symptoms experienced by patients, ostensibly because a delay in diagnosis allows the disease to further progress. 12 We suspect fewer reported symptoms might make it faster and/or easier for practitioners to pinpoint the root cause of symptoms. Results from previous studies demonstrated that receiving a diagnosis can be empowering for patients and validates their symptoms.28,29 However, we do not yet know whether a more rapid diagnoses will lead to earlier treatment, pain alleviation, prevention of disease progression, and improvements in the overall care of endometriosis patients.
As in other research, most endometriosis diagnoses (83% US, 78% non-US) are made by gynecologists.9,16 Interestingly, women in our study were frequently diagnosed with conditions like anxiety, depression, or irritable bowel syndrome before receiving an endometriosis diagnosis. This finding is similar to conclusions reached in previous studies, although it is not clear whether these comorbidities further delay diagnosis or develop as a result of untreated endometriosis.8,10,33 These findings highlight difficulties that practitioners may experience when patients present with complex overlapping symptoms, further emphasizing the need for improved education to facilitate differential diagnosis or a speedy referral for multidisciplinary care. Provider and patient education may be helped by better diagnostic guidelines and a greater awareness of the complexity of endometriosis symptoms.
Results from our survey confirm that endometriosis pain is pervasive and can reduce patient QoL. Most respondents experience some type of endometriosis-related pain daily and severe pain during periods, consistent with findings in previous studies.12,19 A majority of respondents reported significant impairment in QoL that interfered with family/social life, education/career, and sex life, consistent with previous reports.12,18,19 Similar to other studies,11,12,19,34 most respondents in our survey indicated that symptoms like fatigue, gastrointestinal issues, anxiety, and depression resulted from their endometriosis pain. This again emphasizes that endometriosis is a complex disease, where these comorbidities are important to patients and are important to address in disease management.34,35
Women’s dissatisfaction with their healthcare practitioners and feelings of not being heard are concerning because negative practitioner interactions can have a major impact on a patient’s well-being and her ability to cope with a chronic condition. Results from one study indicated that poor communication with practitioners made women more likely to use the Internet to retrieve information about their condition, leading to increased stress and reliance on ineffective self-treatment strategies. 7 Conversely, patients who are happy with their healthcare are more likely to comply with prescribed treatments and will continue to see their practitioner.36,37 Endometriosis in particular is a complex disease that demands practitioners spend more time listening to patients and understanding their needs.
Findings from previous studies have suggested that quality patient-centered care could help improve overall QoL of patients undergoing fertility care.24,25 More recently, a cross-sectional study of endometriosis patients in the Netherlands showed a strong association with patient-centered care and patient health-related QoL. 26 We speculate that aligning treatment goals may help improve patient/practitioner interactions and lead to better overall healthcare.
This survey had some general limitations associated with its design. The sample was recruited from a social network that provides resources and support to women with endometriosis. Social networks are more likely to recruit samples that are not representative of the general population. 38 For example, older generations are usually less likely to utilize social networks. 39 In addition, the social network used to recruit the sample in this survey was created specifically for patients. This type of network may be more likely to draw discontented women who have endured their disease longer and desire support. In fact, results from a recent study support this idea and demonstrate that populations acquired from patient associations are more likely to report longer diagnostic delays and a lower QoL due to the disease. 20 Relatedly, women who respond to email inquiries or Facebook advertisements for the survey may be more likely to have had negative experiences with endometriosis or their practitioners, further impacting survey results. Finally, using patient reports instead of medical records relies on women’s recollection and understanding of past diagnostic evaluations and treatment.
Although sample recruitment from patient support networks has inherent limitations, it also provides distinct advantages. Use of an online social network helped secure a meaningful sample size for detecting differences in perceptions of women with respondents in seven separate countries. Access to a social network also provided useful information that assisted in intelligent survey design/analysis. Discussions between members of MyEndometriosisTeam.com about their experiences with endometriosis helped guide the development of survey questions. We confirmed that the sample population was representative of women with endometriosis by comparing their demographic data with those of women on the social network. Finally, the anonymous nature of the survey was another strength in that it may have enabled respondents to answer questions honestly about sensitive/taboo subject areas without influence from practitioners or researchers. 40
A lack of surgical diagnosis in 23% of women may be considered by some to be a study limitation; however, it has been suggested that clinical diagnosis of endometriosis should play a larger role in the diagnosis process, allowing for a more whole-body approach to endometriosis diagnosis.41–43 The primary purpose of our study was to describe the personal perspective and pathway to diagnosis for all women with endometriosis, regardless of whether the diagnosis was made clinically or with laparoscopy. Exclusion of women who are diagnosed clinically is a limitation of many other endometriosis studies that diminishes the experiences of clinically diagnosed women as less significant. Furthermore, although it is well known that other chronic pain syndromes (e.g., irritable bowel syndrome) contribute greatly to the pain experienced by patients with endometriosis, excluding these patients from the study would not be representative of what a patient with endometriosis experiences.
Conclusion
Women experience challenging and lengthy journeys to receive their diagnosis of endometriosis and attain appropriate treatment. Women report that endometriosis pain is pervasive and has a negative impact on QoL, and they perceive diagnostic delays as prolonging acquisition of effective treatments and pain relief. Furthermore, delay in diagnosis may also propel worsening and spreading of symptoms. Collectively, our findings suggest further research is needed about factors that decrease delay in diagnosis, improve provider–patient interactions, and facilitate overall patient perception of well-being. Additional studies obtaining real-world data will provide further insight on the burden of endometriosis and the patient’s journey from symptoms to diagnosis and from diagnosis to symptom control.
Supplemental Material
Endometriosis_Pain_and_Path_to_Diagnosis_Supplementary_Material – Supplemental material for Path to diagnosis and women’s perspectives on the impact of endometriosis pain
Supplemental material, Endometriosis_Pain_and_Path_to_Diagnosis_Supplementary_Material for Path to diagnosis and women’s perspectives on the impact of endometriosis pain by Georgine Lamvu, Oscar Antunez-Flores, Mona Orady and Beth Schneider in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Acknowledgements
Medical writing support, funded by AbbVie, was provided by Michael Schofield, PhD, and Lamara D. Shrode, PhD, ISMPP CMPP™, of JB Ashtin, who developed the first draft based on an author-approved outline and assisted in implementing author revisions throughout the editorial process.
Author contributions
G.L. participated in concept/design, statistical analysis, manuscript writing, and data interpretation. O.A-F. participated in concept/design and data interpretation. M.O. participated in data interpretation. B.S. participated in concept/design, data acquisition, statistical analysis, and data interpretation. G.L., O.A-F., M.O., and B.S. critically reviewed the manuscript and approved the final version for submission. All authors accept overall responsibility for the accuracy of the data, its analysis, and this report. All authors had full access to all of the data and take complete responsibility for the integrity of the data and accuracy of the data analysis. All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.L. has served on the Daichi Sankyo ObGyn Advisory Board. She also serves as a research consultant for AbbVie and Urosape LLC. She is a recipient of the Pfizer Grants for Learning and Change and is currently chairman of the board for the International Pelvic Pain Society. O.A.-F. is a full-time employee of AbbVie and may hold stock or stock options. M.O. has received honorarium for consultancy from AbbVie, Transenterix, Cooper Surgical, and Teleflex. B.S. has received funding from AbbVie for conducting the research.
Ethical approval
Ethical approval was not sought for the present study because this study is an analysis of an online survey; respondents of the survey did not receive treatment or intervention based on responses to the survey. Respondent privacy was maintained throughout the study. The US portion of the survey was approved by the Advarra Institutional Review Board (Columbia, MD).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial assistance in development of the survey and data collection was provided by AbbVie. In partnership with MyHealthTeams, AbbVie participated in the interpretation of data, review, and approval of the manuscript, and was involved in the decision to submit the article for publication.
Informed consent to participate
Respondents to the survey anonymously opted in to participate in the survey and provided written consent to participate in the research before the survey questions were administered.
Informed consent to publish
Informed consent to publish was not sought for the present study because respondents of the survey did not receive treatment or intervention based on their responses to the survey and responses to the survey were anonymous.
Trial registration
Trial registration is not applicable because this study was not a clinical trial.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.