
Abstract
Objective
Preeclampsia and periodontitis are characterised by altered lipid metabolism. Meta-analyses indicate a higher risk of preeclampsia among women with periodontitis, suggesting a plausible biological connection. Understanding their interaction on fasting lipid levels may reveal targets for integrated strategies to reduce maternal and cardiometabolic risks.
Methods
This case-control study was conducted at the Tamale Teaching Hospital from January to September 2025. The study involved 155 pregnant women, ≥ 20 weeks of gestation, including 52 (33.5%) diagnosed with preeclampsia. The women were aged between 19 and 45 years. All the women underwent periodontal examination before a fasting venous blood sample was collected, and then analysed for fasting lipids.
Results
Results showed that preeclampsia was associated [adjusted odds ratio (95%CI)] with periodontal diseases [3.079 (1.414-6.704)] and, particularly, periodontitis [8.905 (3.574-22.188)]. Sub-group analysis showed that the comorbidity of preeclampsia and periodontitis was characterised by higher levels (mmol/L) of total cholesterol (6.4±1.4 vs 4.9±0.7, P<0.010), low-density lipoprotein cholesterol (4.4±1.2 vs 3.0±0.7, P<0.001), and non-high-density lipoprotein cholesterol (5.1±1.3 vs 3.6±0.8, P<0.010) than preeclampsia alone. However, no significant differences in fasting lipids were observed between normotensive pregnant women with and without periodontitis. Moreover, there were significant interactions between preeclampsia and periodontitis on fasting lipid levels.
Conclusion
The study demonstrates a distinct dysregulated lipid profile among preeclamptic women, which appears to be significantly exacerbated by the presence of periodontitis. These results highlight the need for an integrated antenatal care that includes periodontal screening and management, particularly in women at high risk for preeclampsia.
Introduction
Preeclampsia (PE) remains a major contributor to maternal and perinatal morbidity and mortality globally, where sub-Saharan Africa, including Ghana, is disproportionately affected. 1 PE is characterised by new-onset hypertension and proteinuria or end-organ dysfunction after 20 weeks of pregnancy. PE is increasingly recognised not only as an acute obstetric complication but also as a marker of future cardiometabolic risk for the mother and the child. 2 Altered or dysregulated lipid metabolism is a well-documented feature of PE, with numerous studies, including meta-analyses, reporting elevated maternal triglycerides, low-density lipoprotein (LDL), and very low-density lipoprotein (VLDL) and altered lipoprotein indices compared with normotensive pregnancies. Studies show that these lipid abnormalities are implicated in oxidative stress and endothelial dysfunction, which are central mechanisms in the pathogenesis of preeclampsia and in long-term cardiovascular disease risk. 3 PE pregnancies are also characterised by placental hypoxia and inflammation.4,5
Periodontitis is a chronic, microbially driven inflammatory disease of the supporting tissues of the teeth or periodontium. It is highly prevalent in many low- and middle-income populations (LMICs) and has been documented in Ghanaian communities and antenatal populations.6,7 Aside from local oral effects, periodontitis induces transient bacteremia, systemic inflammation, and exposure to bacterial products, such as lipopolysaccharides (LPS) from bacterial cell walls, which can disturb maternal immune and metabolic homeostasis. 8 Previous experimental and clinical studies have associated periodontal inflammation with dyslipidemia, endothelial activation and insulin resistance in pregnant and nonpregnant cohorts, supporting plausible mechanistic pathways by which oral infection could affect pregnancy outcomes. 9
A growing body of literature has explored the association between maternal periodontitis and adverse pregnancy outcomes, including preeclampsia. Previous meta-analyses and systematic reviews generally report an elevated risk of preeclampsia among women with periodontitis, albeit variations in effect sizes and certainty due to heterogeneity in study designs, periodontal case definitions and confounding control.10,11 Previous randomised trials of periodontal therapy initiated during pregnancy have shown that non-surgical periodontal treatment is safe and improves oral health; however, evidence that treatment reduces obstetric complications such as preeclampsia remains inconclusive. The possible explanation could be that interventions are often given too late to influence placentation, or that trials were underpowered for hypertensive outcomes. 12 These inconsistencies underscore the need for context-specific, prospective research that integrates standardised oral health assessment with biochemical and obstetric measures.12,13
In Ghana, routine antenatal care programs rarely integrate lipid profiling or periodontal screening despite compelling evidence of overlapping burdens of infectious and noncommunicable disease risk factors. 14 Local Ghanaian data on the co-occurrence of periodontitis and preeclampsia and on how this interaction may influence maternal lipid profiles are sparse or non-existent.15,16 Understanding whether periodontitis modifies the relationship between fasting plasma lipid levels and preeclampsia has both mechanistic and public health relevance. If periodontal inflammation amplifies dysregulation of lipid metabolism in preeclampsia, this could identify an actionable target for integrated preventive strategies that reduce immediate obstetric risk and long-term cardiometabolic sequelae among Ghanaian women. 17 Therefore, this study aims to determine the associations between periodontitis, preeclampsia and their interaction on fasting plasma lipid levels among pregnant women.
Materials and methods
Study design and setting
An unmatched case-control study was conducted among pregnant women attending the antenatal clinic at the Tamale Teaching Hospital in the Northern Region of Ghana, between January and September 2025. Tamale is a metropolis and the capital city of the Northern Region of Ghana. Tamale Teaching Hospital serves a mixed urban and peri-urban population and provides tertiary-level care. The hospital has several specialised departments, including functional antenatal and dental clinics that provide obstetric and periodontal examination services to the population of the Northern Region and surrounding regions such as Upper West, Upper East, North-East, and the Savanna regions.
Study population and sample size
The study involved 155 pregnant women, including 52 (33.5%) diagnosed with preeclampsia, while the rest were pregnant women with normotensive pregnancies who served as controls. The women were aged 19 to 45 years in their second or third trimester (≥20 weeks of gestation). The cases and controls (Participants) were recruited consecutively and concurrently from the same clinic to reduce selection bias and bias due to seasonal and environmental factors. Women with systemic diseases unrelated to pregnancy, such as chronic kidney disease, diabetes mellitus, liver disease, tuberculosis or chronic kidney disease and those on lipid-lowering medications, or with recent periodontal therapy or antibiotic use within the past three months, were excluded. The minimum required sample size for this investigation was calculated using the Fleiss formula with Continuity Correction in Epi Info v7 (https://www.cdc.gov/epiinfo/pc.html). Periodontitis was designated the main exposure variable. Reports from previous studies showed that the pooled prevalence of periodontitis among pregnant women in Africa is 58%.18,19 In addition, a meta-analysis reported that women with periodontitis were over three times more likely to develop preeclampsia (OR 3.18, 95% CI 2.26–4.48). 20 Assuming a 95% confidence level, 80% power, and a 1:2 ratio of cases to controls, the sample size required for the study came to 155 participants in total (52 cases and 103 controls).
Diagnosis of preeclampsia
The diagnosis of preeclampsia was based on the definition according to the American College of Obstetricians and Gynaecologists criteria as new-onset hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on two occasions at least 4 hours apart after 20 weeks of gestation). The hypertension is accompanied by proteinuria (≥300 mg per 24-hour urine collection or ≥1+ on dipstick) or evidence of systemic involvement, such as elevated liver enzymes, thrombocytopenia, renal insufficiency, or pulmonary oedema. 21 The controls were pregnant women of similar gestational age as the cases who were free of chronic hypertension and did not meet the clinical definition of preeclampsia.
Periodontal examination
A board-certified periodontist diagnosed periodontitis following the standardised procedure and classification by Armitage, Wu. 22 Recruited participants underwent a comprehensive periodontal examination (CPE). Periodontal parameters (PP) for selected teeth in each of the four quadrants were recorded using individual periodontal charts. Three previously trained examiners conducted inter-examiner calibration and pretesting. All periodontal parameters were recorded twice independently for each quadrant of the mouth, and the results were compared using periodontal charts until at least 90% of duplicate measurements were within 1 mm. Individual periodontal charts captured parameters for specific teeth in all four quadrants, including bleeding on probing (BOP), clinical attachment loss (CAL), probing pocket depth (PPD), missing teeth, and plaque index (PI). All teeth were examined for each participant. Manual instruments, rather than electronic devices, were used throughout the examination. The instruments, including dental mirrors, periodontal probes, and Naber’s probes, are manufactured by Janbro International, United Kingdom. Bleeding on probing (BOP) was recorded as present or absent. Clinical attachment loss (CAL) was measured from the cementoenamel junction (CEJ) to the base of the periodontal pocket, calculated as probing pocket depth (PPD) minus the CEJ–gingival margin distance in cases without recession, or as the sum of recession and PPD when recession was present. Measurements were taken using a UNC-15 periodontal probe with 1 mm graduations at six sites per tooth (distobuccal, midbuccal, mesiobuccal, distolingual, midlingual, and mesiolingual). A probing force of 0.25 N and a 5° angulation were maintained. X-ray images were not taken to reduce the risk of exposure of the developing foetus to radiation. Periodontitis was defined based on the 2017 World Workshop criteria as the presence of interdental clinical attachment loss (CAL) at two or more non-adjacent teeth or buccal/oral CAL ≥3 mm with a pocket depth (PD) of more than 3 mm.
Blood sample collection and biochemical analysis
The women were prepared a day before with fasting requirements and duration. A 5 mL venous blood sample was collected following an overnight fast of 8–12 hours. The blood samples were dispensed into gel separator tubes and allowed to clot at room temperature. The blood samples were then centrifuged at 3000 rpm for 5 minutes to obtain serum. Serum was separated and aliquoted into Eppendorf tubes and then stored at -20 °C for later analysis. Total cholesterol (TCHOL), high-density lipoprotein (HDL) cholesterol, and triglycerides (TRIG) were determined enzymatically using standard and an automated biochemistry analyser using the manufacturer’s recommended reagents, calibrators, and quality control materials. The LDL cholesterol, non-HDL cholesterol, the atherogenic index (TCHOL/HDL), and the cardiovascular risk (LDL/HDL) were then calculated. All assays were performed under strict quality control with internal and external proficiency checks.
Data collection and variables
Socio-demographic, clinical, and obstetric data were obtained through interviewer-administered questionnaires and reviewing medical records. The dependent variable was preeclampsia (yes/no). The independent variables were periodontitis (yes/no) and their interaction term (preeclampsia × periodontitis), fasting plasma lipid levels, including total cholesterol, LDL, HDL, and triglycerides, as well as their derivatives such as non-HDL cholesterol, total cholesterol/HDL, and LDL/HDL cholesterol ratios. Covariates with confounding potential included maternal age, gestational age, parity, body mass index (BMI), and oral hygiene practices. Potential confounding was addressed using statistical approaches since there was no matching of cases and controls.
Statistical analysis
Data were collected into an MS Excel Spreadsheet and then analysed using IBM SPSS Statistics version 27. The normality of the continuous variables was checked using the Shapiro-Wilk test before being summarised as means ± standard deviations (SD). The categorical variables were summarised as frequencies and percentages. Independent t-tests and one-way ANOVA, with post hoc test for multiple comparisons, were used for group comparisons of continuous variables. Tests of associations were achieved using the Chi-square test or univariable and multivariable binary logistic regression analysis. Multiple linear regression models were fitted with 2-way interaction terms between preeclampsia and periodontitis to evaluate the main and interaction effects of preeclampsia and periodontitis on cardiometabolic factors, adjusting for potential confounders. The interaction term (preeclampsia × periodontitis) was included in the regression model to assess whether the combined presence of both conditions had a multiplicative effect on lipid levels. The assumptions of multivariable linear regression were tested for significant PE*Periodontitis models using the variance inflation factor for multicollinearity diagnosis, the P-P plot for multivariable normality, and the scatter plot (predicted vs residual values) for homoscedasticity. All statistical tests were two-sided, and significance was set at P < 0.05, and 95% confidence intervals were reported. The manuscript was prepared following the STROBE recommendations for an observational case-control study.
Results
Participants
About 305 pregnant women in their second and third trimesters of pregnancy were potentially eligible for the study. However, 175 women were examined for eligibility, and 161 women were confirmed eligible. A total of 155 women were finally included in the study because six women declined periodontal examination. There was no follow-up in this study, and all 155 were included in the final analysis.
Socio-demographic, anthropometric, obstetric, and clinical characteristics of the study sample
The anthropometric and obstetric characteristics of the study sample
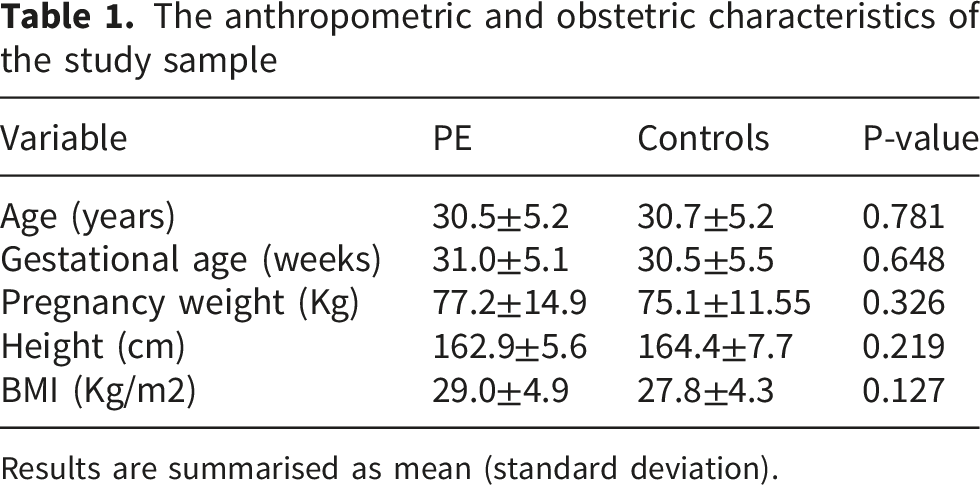
Results are summarised as mean (standard deviation).
Socio-demographic, obstetric and clinical characteristics of the study sample
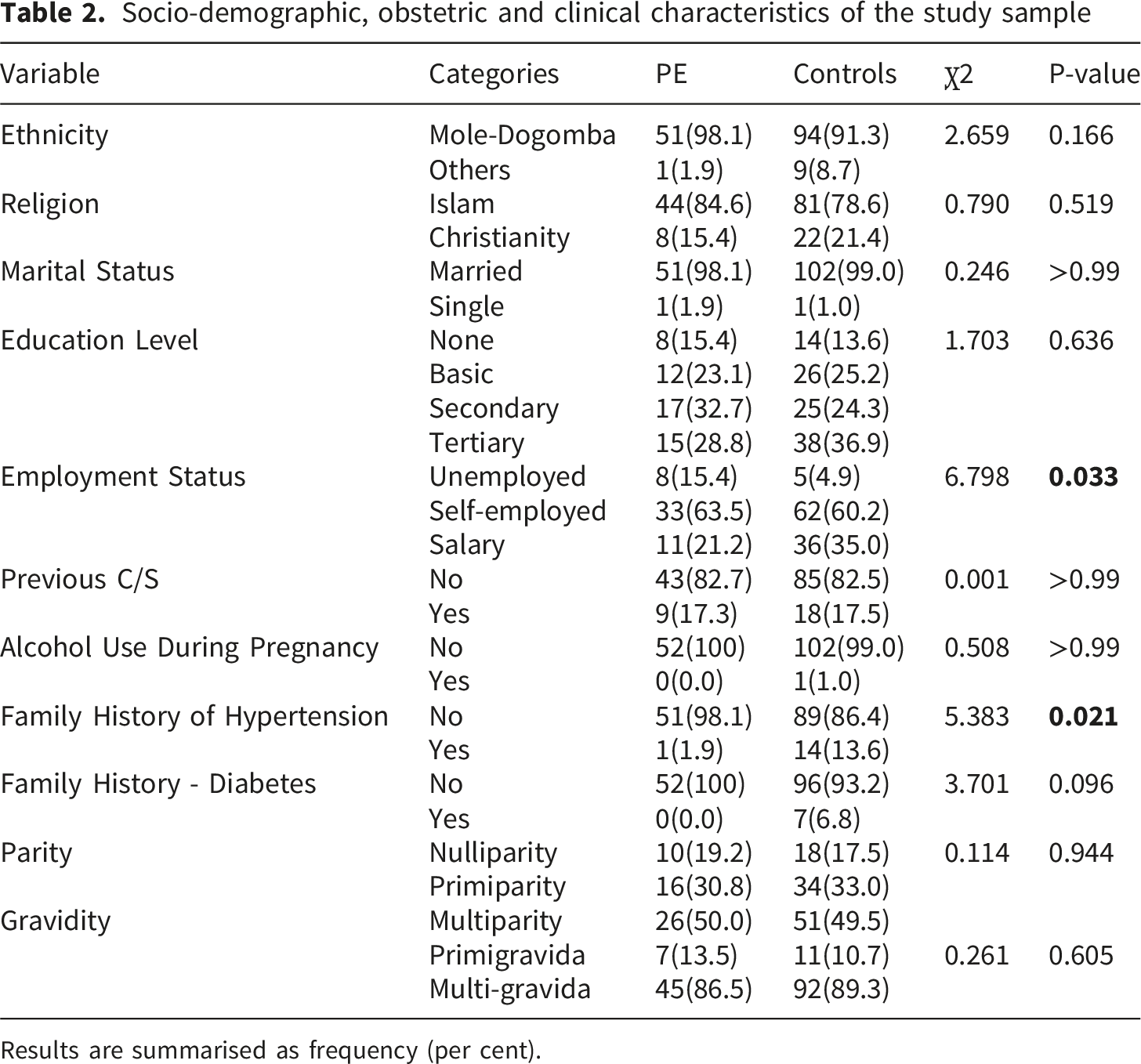
Results are summarised as frequency (per cent).
Association between preeclampsia and periodontitis
Comparing the probing pocket depth (PPD), clinical attachment loss (CAL) and plaque index (PI) between preeclampsia and controls
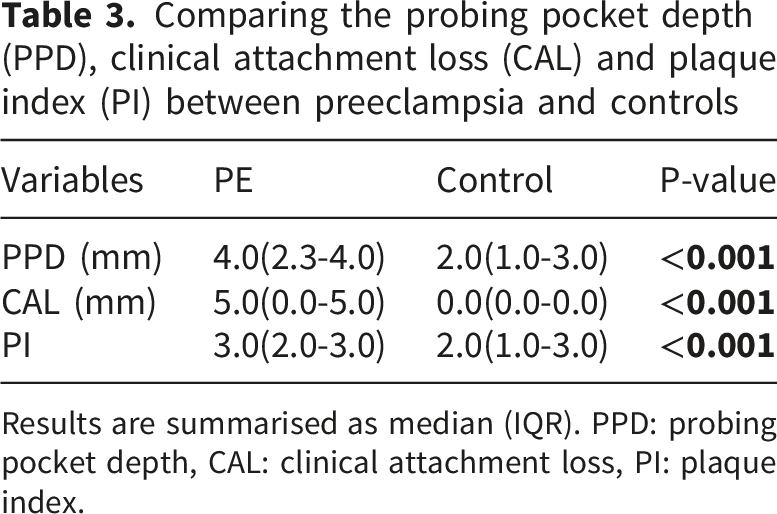
Results are summarised as median (IQR). PPD: probing pocket depth, CAL: clinical attachment loss, PI: plaque index.
Prevalence of oral cleaning habits and periodontal diseases between preeclampsia and controls
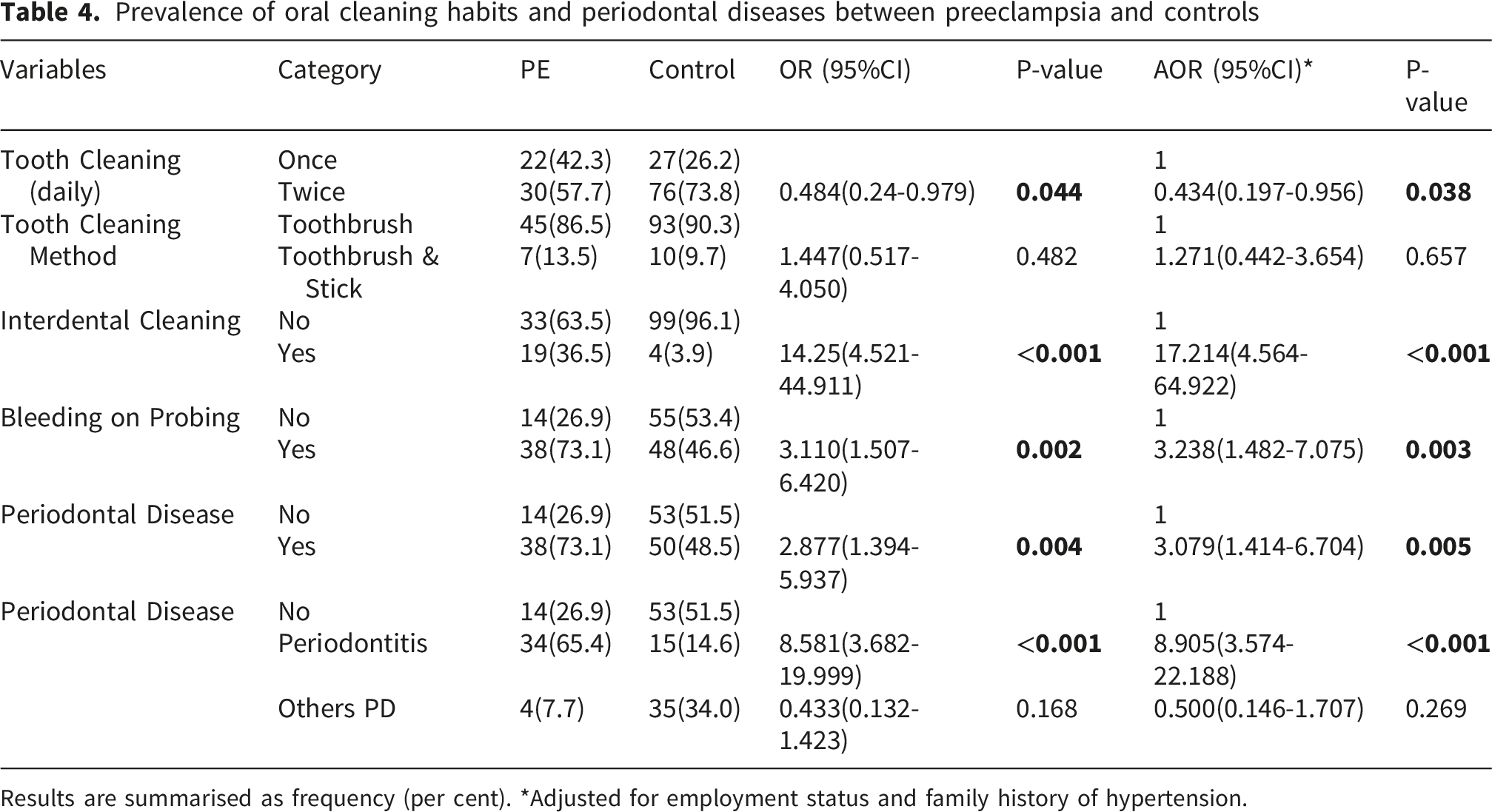
Results are summarised as frequency (per cent). *Adjusted for employment status and family history of hypertension.
Variations in lipid variables in preeclampsia and periodontitis
Variations in fasting lipids between preeclampsia and controls
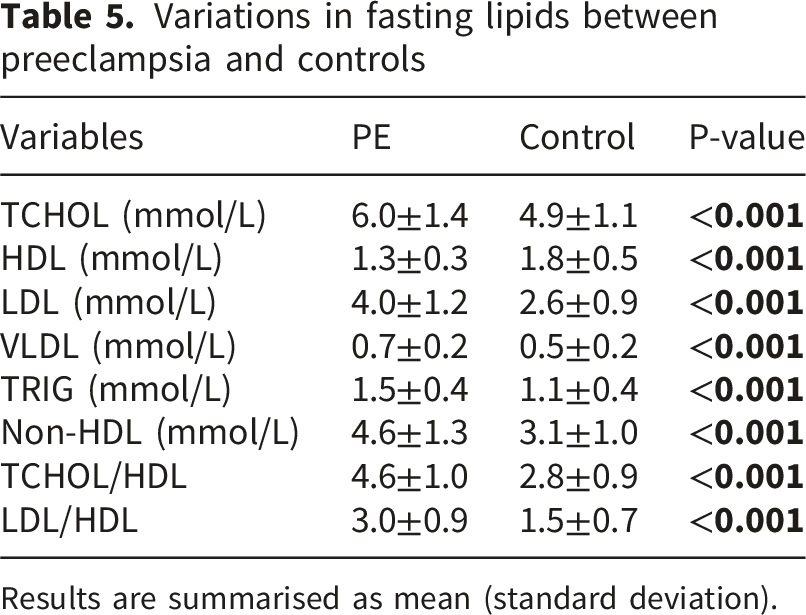
Results are summarised as mean (standard deviation).
Variations in fasting lipids between pregnant women with and without periodontal disease
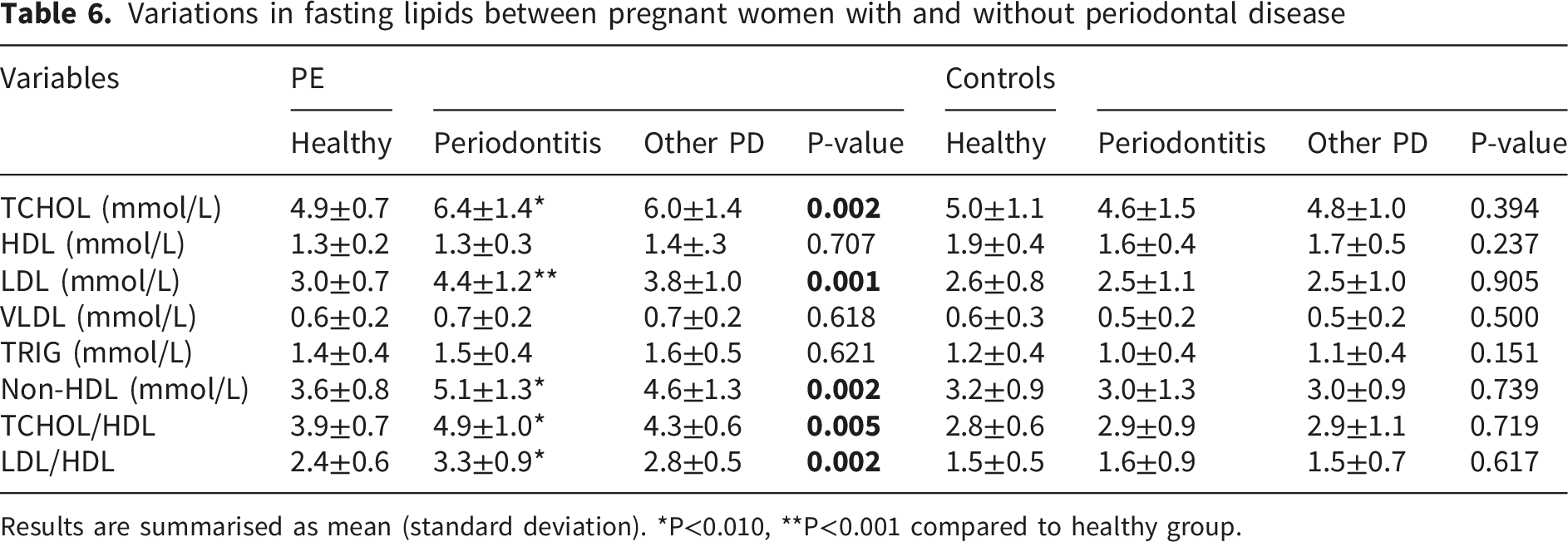
Results are summarised as mean (standard deviation). *P<0.010, **P<0.001 compared to healthy group.
Interactions between preeclampsia and periodontitis on fasting lipid variables
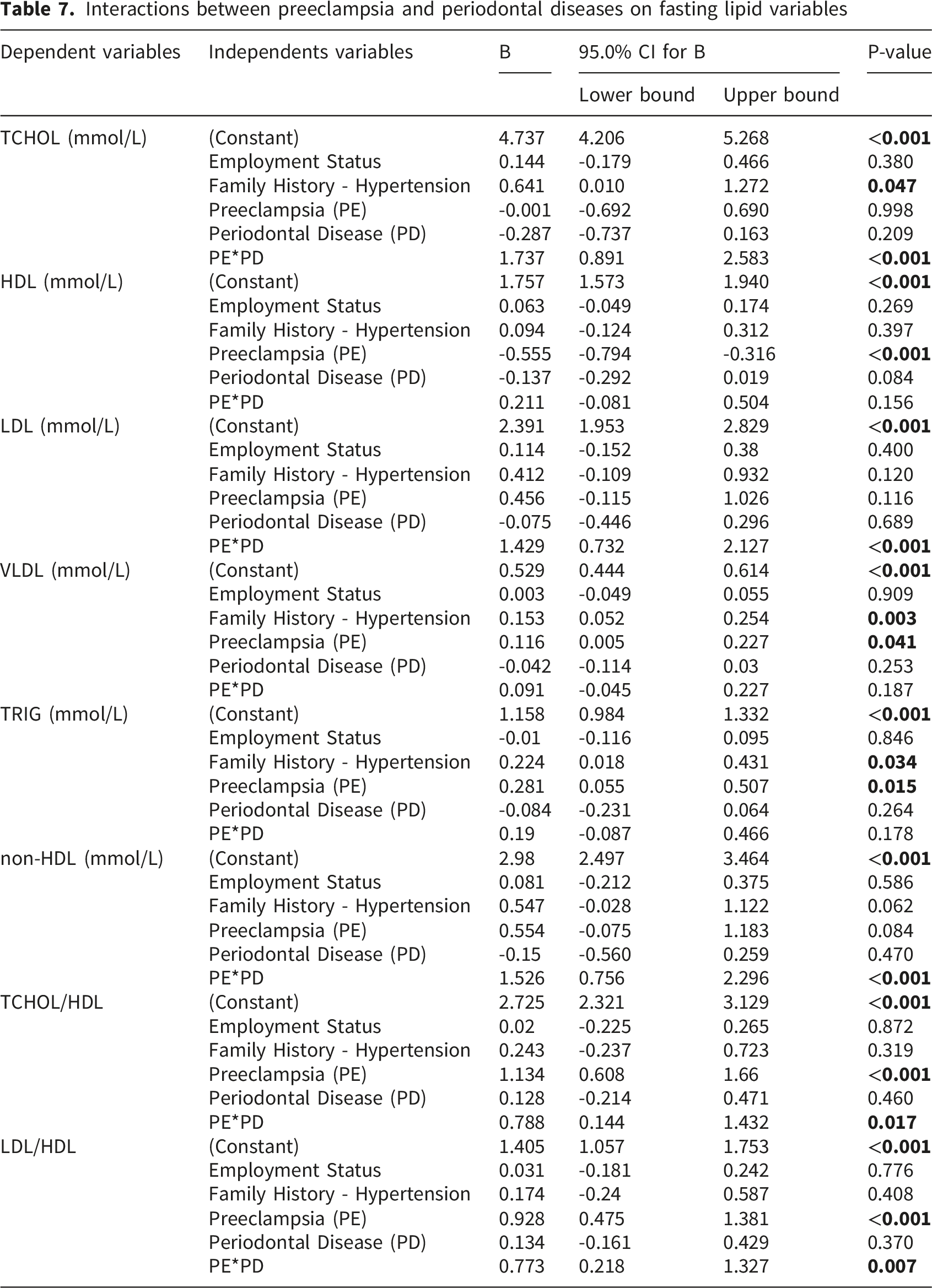
Interactions between preeclampsia and periodontal diseases on fasting lipid variables
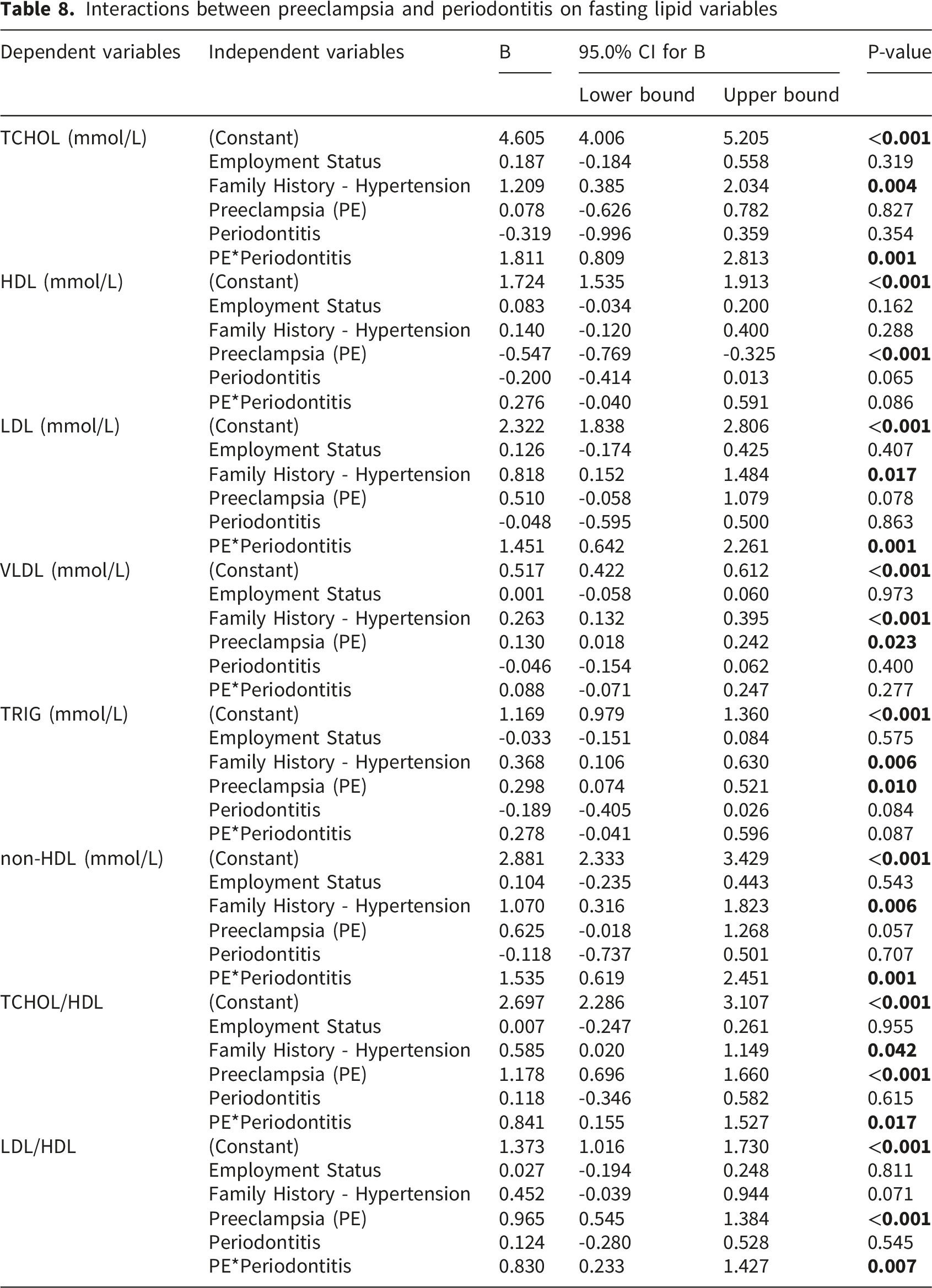
Interactions between preeclampsia and periodontitis on fasting lipid variables
Discussion
The study aimed to investigate the relationship between preeclampsia and periodontitis on fasting plasma lipid levels. The women diagnosed with preeclampsia were not significantly different from the controls in chronological age, gestational age and body mass index. It was observed that preeclampsia was significantly associated with periodontitis. Sub-group analysis showed that the total cholesterol, LDL, non-HDL, total cholesterol/HDL, and LDL/HDL were higher in preeclamptic women with periodontitis than in those without periodontitis. However, there were no significant differences in lipid variables between normotensive pregnant women with and without preeclampsia. It was also observed that significant interactions between preeclampsia and periodontitis or periodontal disease occurred on fasting plasma lipid variables.
The current study supports growing evidence that maternal periodontitis is associated with preeclampsia, one of the major causes of maternal and perinatal morbidity and mortality. Previous observational studies and meta-analyses have demonstrated that women with periodontal disease, including periodontitis, are approximately two to four times more likely to develop preeclampsia compared with their periodontally healthy counterparts.23,24 This positive association may suggest that chronic oral inflammation may contribute to systemic vascular and immune disturbances that characterise preeclampsia.
The observed association between preeclampsia and periodontitis have biological plausibility. It has been observed that periodontal pathogens, such as Fusobacterium nucleatum and Porphyromonas gingivalis, can translocate into the systemic circulation, leading to endothelial dysfunction and a maternal inflammatory response.25,26 These mechanisms parallel the pathophysiology of preeclampsia, which is characterised by exaggerated inflammatory and oxidative stress responses, endothelial activation and abnormal placentation. High levels of inflammatory mediators, including cytokines such as tumour necrosis factor-alpha, interleukin-6, and C-reactive protein, in women with periodontal disease may amplify endothelial injury and placental ischemia, predisposing to hypertensive complications during pregnancy.27,28 Although observational studies consistently show a positive relationship, causality remains uncertain due to heterogeneity in diagnostic criteria for periodontitis, study design and potential residual confounding by socioeconomic status, obesity, smoking and chronic diseases.23,29 In addition, previous randomised controlled trials of periodontal therapy during pregnancy have demonstrated improvements in oral health but have not consistently reduced the incidence of preeclampsia or other adverse pregnancy outcomes. 12 This observation may be due to the late timing of intervention or the irreversible nature of placental alterations once preeclampsia is established. However, maintaining periodontal health remains vital during pregnancy, as treatment is safe and may reduce systemic inflammation. 30
Disparity in fasting lipids between pregnant women with and without periodontitis was only observed among the preeclampsia group, but not the controls. This demonstrates a distinct dysregulated lipid profile among preeclamptic women, which is made worse by the presence of periodontitis. This suggests a potential synergistic interaction between the two conditions, as was observed in the study. 31 The absence of marked differences in lipid variables between normotensive pregnant women with and without periodontitis indicates that periodontal inflammation alone may not be sufficient to disrupt lipid metabolism in healthy pregnancies. 32 This observation reinforces the concept that periodontitis may act as an effect modifier, which amplifies pre-existing conditions characterised by metabolic disturbances such as preeclampsia, rather than acting as an independent risk factor. 33
This study found significant interactions between preeclampsia and periodontitis on fasting plasma lipid levels. This may indicate that the coexistence of both conditions may synergistically worsen maternal lipid metabolism during pregnancy. 23 This finding supports the growing body of evidence associating both periodontitis and preeclampsia with oxidative stress, systemic inflammation, and endothelial dysfunction, which are known to impact lipid homeostasis. 7 Preeclampsia is marked by perturbed lipid metabolism, commonly manifesting as elevated total cholesterol, low-density lipoprotein and triglycerides levels, along with decreased high-density lipoprotein concentrations. 34 Similarly, chronic periodontitis has been associated with dysregulated lipid metabolism, potentially due to systemic dissemination of inflammatory cytokines and bacterial endotoxins such as lipopolysaccharides that stimulate hepatic lipid synthesis. 17 The observed interaction suggests that inflammatory mediators derived from periodontal infection may worsen the lipid abnormalities typically seen in preeclampsia, amplifying the risk of vascular dysfunction. This synergistic effect between preeclampsia and periodontitis could be mediated by overlapping pathophysiological pathways of the disease conditions. Periodontal pathogens like Porphyromonas gingivalis and Fusobacterium nucleatum can invade the bloodstream, activating toll-like receptors and triggering the release of pro-inflammatory cytokines such as IL-6, TNF-α, and CRP. 35 These cytokines not only contribute to endothelial injury but also impair lipid transport and oxidation, which may lead to hyperlipidemia and oxidative modification of LDL particles. In preeclamptic women with concurrent periodontal disease, this compounded inflammatory burden may promote greater vascular lipid deposition and endothelial activation, consistent with our finding of elevated plasma lipid levels in those with both conditions. 36 Although causality cannot be inferred, the significant interaction between preeclampsia and periodontitis on lipid levels underscores the potential cardiometabolic link between oral and systemic health. 37
This study contributes vital baseline data regarding the link between oral and systemic health that is scarce or non-existent in the Ghanaian population. In addition, previous studies were largely association studies, which did not establish the possible synergistic effect between preeclampsia and periodontitis on cardiometabolic factors. However, causality could not be inferred due to the case-control design of the study. It was also not possible to determine changes in fasting lipid levels since the study was not longitudinal in design.
Conclusion
The study found that preeclampsia is associated with periodontal diseases, particularly periodontitis. In addition, there is an interaction between preeclampsia and periodontitis of cardiometabolic risk factors in pregnancy. These results highlight the need for an integrated antenatal care that includes periodontal screening and management, particularly in women at high risk for preeclampsia.
Supplemental material
Supplemental material - Preeclampsia, periodontitis and their interactions on cardiometabolic risk markers in pregnancy: A case-control study
Supplemental material for Preeclampsia, periodontitis and their interactions on cardiometabolic risk markers in pregnancy: A case-control study by Richard Ayimbire, Moses Banyeh, Gabriel Abbam, Laud Anthony W. Basing, Shafiat Omotoyosi Shittu, Michael Antunmuni Yelibora, David Ayim Antwi, Munkaila Adam, Issah Zabsonre Alhassan in Journal of Public Health Research
Footnotes
Acknowledgements
The researchers wish to acknowledge the Institute for Interdisciplinary Studies (IIR) of the University for Development Studies for facilitating the funding process of the study. In addition, Dr Jonathan Adongo Akeleyigna, Dr Asoma Awudu and Dr Nimat’ullah Obeitor, of the Dental, Eye, Ear, Nose and Throat (DEENT) sub-BMC and the staff of the Antenatal Clinic of the Tamale Teaching Hospital are acknowledged for granting the researchers access to the clinic and clients to enable us to obtain data for the study.
Ethical considerations
The study was approved by the institutional review board of the University for Development (Ref#: UDS/RB/0085/25). Permission to undertake the study was obtained from the Tamale Teaching Hospital. The study complied with the recommendations of the 1964 Declaration of Helsinki and its later amendments regarding human subject studies. Participation was voluntary, and confidentiality of all data was maintained. Pregnant women diagnosed with preeclampsia received prompt obstetric care according to national guidelines, and those who were diagnosed with periodontitis were referred for appropriate periodontal management.
Consent to participate
Written informed consent was obtained from all participants.
Consent for publication
The participants gave consent to publish the findings of the study.
Author contribution
RA, MB, GA, LAWB, SOS, IZA-Conceptualisation, methodology; RA, MAY, DAA, MA-experimentation, data collection; RA, MB- data analysis and interpretation, writing-draft; All authors have read and approved the final version of the manuscript. The corresponding author had full access to all of the data in this study, and he takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the University for Development Studies Research Fund (Ref#: CALL 24-1).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.