
Abstract
Background:
Non-communicable diseases (NCDs) are responsible for over 70% of the global mortality, disproportionately affecting low-and middle-income countries. Simultaneously, climate change is escalating health risks by intensifying climate-related hazards and climate-mediated environmental risk factors that affect NCD prevention and management, including extreme heat, air pollution, and food insecurity. These dual crises increasingly intersect and demand integrated policy response.
Objective:
This scoping review protocol outlines a systematic approach to map, examine, and analyze global strategies, policies, programs, and management models for NCD prevention and control in the context of climate change. It will evaluate how climate and environmental factors are incorporated into health system governance, implementation, and performance, and identify gaps for strengthening NCD strategies.
Methods:
Following Arksey and O’Malley’s framework and PRISMA-ScR guidelines, a systematic search was conducted using PubMed, Scopus, Web of Science, Embase, and relevant gray literature sources. Studies and reports from 2004 to 2025 that focus on NCD-related policies with explicit reference to climate change will be included. Data extraction will be conducted independently by two reviewers and synthesized thematically to identify common approaches, challenges, and innovations.
Expected outcomes:
This review will map existing global practices, highlighting integrated policy components, implementation levels, and reported outcomes. It will also identify knowledge gaps and inform the development of climate-resilient NCD strategies, particularly in vulnerable regions.
Conclusion:
As climate change and NCDs converge into a global syndemic, understanding integrated health-system responses is crucial. This review will support policymakers in designing effective context-specific interventions to build resilient and sustainable healthcare systems.
Introduction
In recent decades, non-communicable diseases (NCDs), such as cardiovascular disease, diabetes, cancer, and chronic respiratory conditions, have emerged as major global health concerns, accounting for over 70% of global deaths. These diseases disproportionately affect low- and middle-income countries and are closely linked to behavioral risk factors such as poor diet, physical inactivity, and tobacco use. 1 While global attention to NCDs has increased substantially in recent years, particularly following the Sustainable Development Goals, earlier global health agendas and funding mechanisms historically prioritized communicable diseases, contributing to structural gaps in NCD preparedness within many health systems.2–4 This review primarily focuses on the four major non-communicable diseases—cardiovascular diseases, diabetes, cancer, and chronic respiratory diseases—while remaining open to other chronic conditions where relevant to climate-related policy and management frameworks.
Climate change has become a major global health threat. Primarily driven by human-induced greenhouse gas emissions, climate change results in rising global temperatures and an increased frequency of extreme weather events such as heat waves, floods, and droughts.5–8 These environmental disruptions exacerbate the existing health risks and introduce new challenges for NCD management. For example, heat waves and high temperatures can worsen cardiovascular and respiratory conditions, 9 while air pollution, often intensified by climate-related factors, is linked to an increased risk of heart and lung diseases. 10 Poor air quality and extreme heat can also reduce outdoor physical activity, compounding the NCD risk factors.
Climate change jeopardizes food and water security. Shifts in rainfall and prolonged droughts decrease agricultural productivity and increase the risk of malnutrition. Simultaneously, disasters such as floods can disrupt clean water access. These disruptions elevate the risks for both undernutrition and obesity, which are key contributors to the NCD burden. 11 Thus, climate change is increasingly recognized not only as an environmental crisis but also as a public health emergency, particularly due to its impact on NCD-related health outcomes. The World Health Organization (WHO) has listed climate change as one of the top 10 global health threats for the coming decade, 12 emphasizing the need for urgent health system responses.
Recent research has emphasized that countries must develop adaptive strategies to cope with both immediate and long-term health threats posed by climate change and NCDs. Such strategies may include strengthening the healthcare infrastructure, improving access to primary healthcare, promoting healthier lifestyles, and investing in climate-sensitive disease surveillance and early warning systems.
As both NCDs and climate change are global in scope and cross national boundaries, international cooperation is essential.9,13 Encouragingly, some countries have begun integrating climate risks into NCD policies and planning. For instance, New South Wales in Australia developed a climate-health framework that incorporated chronic disease prevention. 14 Global assessments have also noted progress in embedding health considerations—including NCD prevention—into national climate adaptation plans.13–16
Given these developments, there is a growing need to systematically map and evaluate existing policies and models integrating NCD management with climate change adaptation. To address this need, a clear conceptual framing of climate change and its pathways of influence on NCD management is required.
In this review, climate change is conceptualized as a macro-level environmental determinant that influences non-communicable disease (NCD) management through multiple pathways. To ensure conceptual clarity, climate-related factors will be classified into three analytically distinct but interrelated categories. First, direct climate hazards will refer to acute and chronic climatic events that are explicitly attributable to climate change, including heatwaves, floods, droughts, and other extreme weather events. These hazards may directly exacerbate NCD morbidity and mortality or disrupt the continuity of care. Second, indirect climate-mediated environmental risks will include environmental conditions whose intensity or distribution is influenced by climate change, such as air pollution, food insecurity, and water scarcity. Although these factors may not be exclusively caused by climate change, they are increasingly shaped by climate dynamics and represent key pathways through which climate change affects NCD prevention and control. Third, health system stressors related to climate change will encompass disruptions to healthcare delivery, infrastructure, and supply chains, which disproportionately affect individuals living with chronic conditions. This conceptual framework will guide the definition of the review context, inform the development of the search strategy, and structure the interpretation of findings, allowing for a systematic distinction between climate-driven, climate-mediated, and health system–level mechanisms affecting NCD management.
In addition to examining strategies explicitly designed for NCD prevention and control that incorporate climate change considerations, this review will also consider climate adaptation, disaster risk reduction, and extreme weather management frameworks that explicitly address the needs of individuals living with NCDs. This bidirectional perspective acknowledges the evolving recognition of chronic disease management within climate and disaster governance and allows for a more comprehensive mapping of integrated policy responses.
Objective
This scoping review will aim to systematically map, examine, and synthesize global strategies, policies, and management models addressing NCD prevention and control in the context of climate change, and to analyze how, to what extent, and in what ways climate considerations are integrated into health system governance.
Guided by the Population–Concept–Context (PCC) framework, the review will be structured as follows:
Population: Global and national health systems, including their governance structures.
Concept: Policies, governance frameworks, or management models designed for NCD prevention and control and/or climate adaptation, disaster risk reduction, or extreme weather management frameworks that explicitly address the needs of individuals living with NCDs.
Context: Climate change and its interrelated pathways of influence on health, which will be operationalized as: (1) direct climate hazards (e.g. heatwaves, floods, droughts); (2) indirect climate-mediated environmental risks (e.g. air pollution, food and water insecurity); and (3) health system stressors (e.g. care disruption, infrastructure damage).
The primary research question will be: What are the key components and characteristics of existing models for NCD management that integrate climate change considerations?
Sub-questions will examine:
Which specific strategies or policy instruments have been implemented?
Which NCDs and which climate-related risks are primarily addressed?
What outcomes, lessons learned, or challenges have been reported?
What are the levels of implementation (local, national, international) and governing mechanisms (e.g. cross-sector collaboration)?
The findings will map existing integrated practices, highlight knowledge gaps, and inform the development of evidence-based, climate-resilient, and context-specific interventions to mitigate the dual burden of NCDs and climate change, particularly for vulnerable regions. The level of integration will be assessed descriptively based on whether climate considerations are (a) mentioned rhetorically, (b) incorporated into strategic objectives, or (c) embedded within operational implementation mechanisms and monitoring frameworks.
Review team
This review was conducted by an interdisciplinary team with expertise in epidemiology, health policy and management, climatology, and systematic review methods. This team composition (including experienced scoping review authors) strengthened the rigor and relevance of the review. Two reviewers will independently perform study screening and data extraction, with a third reviewer available to resolve any disagreements, ensuring a high level of reliability in the selection and extraction processes. The team’s expertise also helped to ensure that both health policy nuances and climate science aspects were appropriately considered when interpreting the findings.
Methodology
This protocol follows the five-stage framework proposed by Tricco et al. 17 for scoping studies, with enhancements made by Levac et al. and Joanna Briggs Institute (JBI) guidance.18,19 The methods used in each stage are outlined below. The review methods were planned in advance and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for coping reviews (PRISMA-ScR) checklist. 20 Following the PRISMA-ScR guidance, we documented the study selection process in a flow diagram and included the completed PRISMA-ScR checklist to ensure transparent reporting.
Identifying the research question (Step 1)
The research question was formulated using the population–concept–context (PCC) framework to ensure both breadth and focus. This study seeks to explore the key components of NCD management models that incorporate climate change across global health systems. A preliminary literature review confirmed the lack of existing scoping reviews at this intersection, affirming the originality of the study. The PCC framework defines population as a global health system, the concept of policies or governance models for NCD control, and the context of climate change. Sub-questions were developed to guide data extraction, focusing on the targeted NCDs, climate-related factors, and levels of implementation. This step ensured clarity and relevance throughout the review process.
Identifying relevant studies (Step 2: Search strategy)
A comprehensive search strategy (Table 1) was developed to identify both peer-reviewed and gray literature related to NCD management in the context of climate change. The search strategy will be explicitly designed to capture both NCD-focused policies incorporating climate considerations and climate or disaster-related frameworks that include explicit provisions for chronic disease management. The process was informed by prior literature, such as Ratter-Rieck et al., and refined with the support of an expert health sciences librarian to ensure coverage across the medical, environmental, and policy domains. 13 Searches will be conducted in PubMed, Web of Science, Scopus, and Embase, alongside gray literature sources, including WHO IRIS, UNFCCC, World Bank, and UNDP repositories. Google Scholar and Google Advanced Search also will be used to find additional policy documents. Recognizing that relevant policies and models may be documented in both academic and non-academic sources, the search strategy employs broad terms to capture peer-reviewed literature while also systematically searching key gray literature repositories (e.g. WHO IRIS, UNFCCC, national ministry websites) known to host policy documents and reports.
Search strategy syntax for databases.
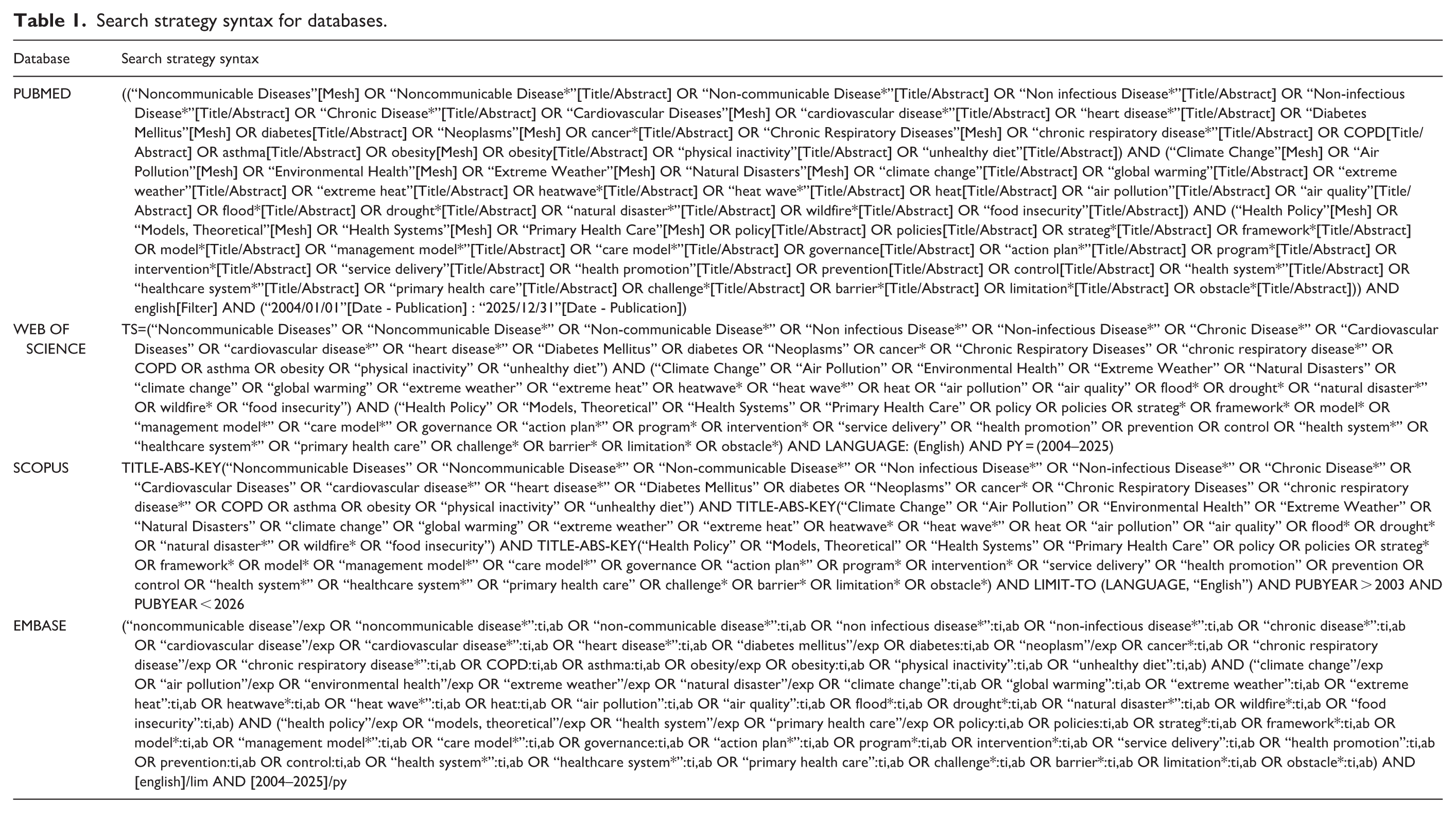
The search terms covered three domains: (1) NCDs (e.g. diabetes, cardiovascular disease), (2) climate-related phenomena (e.g. climate change, air pollution, and droughts), and (3) health governance (e.g. health policy, strategy, adaptation). To avoid missing relevant policies that may not explicitly use the overarching term “noncommunicable diseases,” disease-specific terms and key risk factors for noncommunicable diseases (e.g. obesity, physical inactivity and tobacco) will be included in the search strategy in cases that are relevant to policy and management contexts. Boolean operators and a database-specific syntax were applied. The search was restricted to English-language publications from 2004 to 2025, reflecting the period when NCD–climate linkages gained global attention. All results will be imported into EndNote and de-duplicated. Given the expected volume of literature, a rigorous screening process was planned to ensure relevance and comprehensiveness of the included studies. Disease-specific terms and major NCD risk factors were intentionally included alongside the umbrella term “non-communicable diseases” to capture relevant policies and frameworks that may not explicitly use contemporary NCD terminology.
Study selection (Step 3: Screening and eligibility)
Study selection will be followed a structured two-stage screening process. In Level 1, two independent reviewers will screen the titles and abstracts of all retrieved records to identify potentially relevant studies. A broad inclusion approach was applied at this stage to avoid missing any valuable literature. In Level 2, the full texts of the selected studies were reviewed against predefined inclusion and exclusion criteria. Discrepancies and uncertainties during both stages were resolved through discussion or by consulting a third reviewer.
Eligibility will be determined using the population–concept–context (PCC) framework. The inclusion criteria are as follows: (a) English-language publications from 2004 onward; (b) studies focused on managing NCDs in the context of climate change; (c) availability of full text; and (d) Eligible documents must primarily focus on describing, proposing, evaluating, or implementing a policy, strategy, governance framework, or management model that addresses NCD prevention/control in the context of climate change. This includes, but is not limited to: national or sub-national policy documents, action plans, clinical guidelines, legislative decrees, white papers, WHO or other international agency framework documents, government reports, disaster risk reduction plans with explicit NCD components, and peer-reviewed articles that analyze such policies or models. Studies that solely examine epidemiological associations between climate variables and NCD outcomes, without a focus on policy or management responses, non-English documents, pre-2004 publications, pre-prints, and studies that lack alignment with the review’s conceptual scope or fail to integrate both the NCD and climate change dimensions, will be excluded.
For the purposes of this review, peer-reviewed scientific studies will be eligible only if their primary focus is the analysis, evaluation, comparison, or proposal of governance frameworks, policy instruments, regulatory mechanisms, service delivery models, or implementation strategies related to NCD prevention and control in the context of climate change. Empirical studies (qualitative, quantitative, or mixed-methods) will be included only when the unit of analysis is a policy, system-level intervention, or governance mechanism rather than epidemiological associations, clinical outcomes, or risk-factor prevalence. This clarification ensures that the review remains policy- and systems-oriented, with policies and governance models as the central analytical unit.
A pilot screening of 15 studies was conducted to harmonize the reviewers’ interpretations of the criteria and ensure inter-rater agreement (Cohen’s kappa > 0.75). Studies that only discussed NCDs or climate change in isolation or those with a purely biomedical focus lacking policy or management relevance were excluded.
The final outcome of the selection process will be illustrated using a PRISMA-ScR flow diagram, displaying the number of records identified, screened, excluded (with reasons), and ultimately included for data extraction. This ensures transparency and adherence to PRISMA-ScR guidelines. By the end of this stage, a refined set of studies, meeting all criteria, and aligned with the research question, will be ready for systematic data extraction and analysis in the next steps of the review.
Data extraction and charting (Step 4)
For each included study or document, data will be systematically extracted using a predesigned and pilot-tested data-charting form. This form (Table 2) will capture essential information, such as author(s), year, country or region, source type (e.g. empirical study, policy report), methodology (if applicable), and descriptions of policies or NCD management models. Importantly, we will extract details related to climate change components, such as mitigation, adaptation, and resilience strategies, and specific NCD outcomes or targeted risk factors (e.g. cardiovascular health, heat-health action plans, and air pollution).
Preliminary items of the data extraction form.

The form also will record whether a theoretical or governance framework was used (e.g. WHO guidelines), the level of implementation (local, national, or global), and the health system level involved (primary care, public health, or multi-sectoral initiatives). Key components, such as policy objectives, sectors involved, interventions, reported outcomes, and recommendations, will be documented. This comprehensive charting ensured a clear understanding of how climate change is integrated into NCD policy and planning.
To reduce bias, two independent reviewers will extract the data and compared the results, resolving discrepancies through consensus or third-party adjudication. This dual review process will increase the reliability of the findings. Following data extraction, we will conduct a qualitative thematic analysis using an inductive approach based on Braun and Clarke’s methodology. 21 Rather than using a predefined framework, codes and themes will be allowed to emerge organically from the data.
Thematic coding will be performed using software (NVivo or Excel). Two reviewers jointly will develop the coding scheme from a subset of studies to ensure consistency and then applied it to the dataset. This process will enable us to identify common trends, innovations, and contextual differences in how countries integrate climate risk into NCD management strategies.
In line with the conceptual framework, extracted data will be explicitly categorized according to three climate-related pathways: (1) direct climate hazards, (2) climate-mediated environmental risks, and (3) climate-related health system stressors. Each included policy or model will be mapped against these categories to assess which pathways are addressed and to what extent. This structured categorization will allow comparative analysis across different governance contexts.
Collating, summarizing, and reporting results (Step 5)
After data extraction and thematic analysis, the findings will be collated and presented in both tabular and narrative formats. A summary table will be developed to map the key characteristics of each included study, including setting, focus, climate context, and main findings or policy recommendations. This table acts as an evidence map to understand the global landscape of climate-related NCD policy initiatives.
Narrative findings will be organized under thematic headings that emerged from the analysis, such as “Surveillance and early warning systems,” “Cross-sector governance,” and “Community-level interventions.” Under each theme, the literature will be synthesized to highlight representative strategies, regional differences, and innovative practices. Quantitative summaries, such as the number of studies by region or the types of climate risks addressed (e.g. heatwaves and air pollution), were supported by simple graphs or charts. Where relevant, themes will distinguish between NCD-focused policies incorporating climate adaptation and disaster or extreme-weather frameworks that integrate chronic disease management. This distinction will help clarify bidirectional policy integration.
The Discussion section interprets these findings, identifying knowledge and policy gaps, such as limited attention to NCDs, mental health in climate plans, or a lack of evaluation data. It also explores the lessons learned, suggesting that commonly used governance models (e.g. multisectoral committees or integrated climate-health strategies) could be adapted in other contexts. Barriers such as limited resources or siloed planning are common challenges.
In alignment with the scoping review methodology, no formal quality appraisal will be conducted, as the aim is to map strategies and not assess effectiveness. However, the review comments on the nature of the evidence, including possible overrepresentation in high-income countries.
Transparency will be maintained through the PRISMA-ScR documentation and OSF registration. The results will be shared via journals, conferences, and policy briefs to inform future research and decision-making.
Timeline
We have outlined a timeline for the review’s key activities to ensure timely completion. Figure 1 presents a Gantt chart of the projected schedule from the initial literature search through screening, extraction, analysis, and write-up. In summary, literature search and screening will take place in the first 2–3 months, followed by data extraction and analysis in the next 2 months, and synthesis and reporting in the subsequent month. This timeline will help monitor progress and align the team efforts at each stage.

Gantt chart for scoping review activities.
Summary – Ethics and dissemination
This scoping review is part of a PhD project in health service management and was approved by the Ethics Committee of the Mashhad University of Medical Sciences (IR.MUMS.FHMPM.REC.1403.098). As it involves only published literature, there are no ethical concerns regarding human subjects. The findings will be submitted to a peer-reviewed journal on health policy or environmental health and shared with relevant stakeholders in Iran and internationally. To promote transparency, the protocol is registered in the Open Science Framework (DOI: https://doi.org/10.17605/OSF.IO/RJMHQ), where any future methodological updates will also be documented and made publicly accessible.
Discussion
This scoping review addresses a significant knowledge gap by mapping global strategies for managing non-communicable diseases (NCDs) in the context of climate change. It aims to identify key components of existing policies, such as intersectoral governance mechanisms, community engagement strategies, and targeted interventions, such as heat-health alert systems for patients with chronic conditions. By clarifying these elements, this review supports the development of evidence-based models that integrate NCD management into climate-resilient health systems. The findings will help policymakers understand the successful strategies implemented elsewhere and adapt them to their local contexts.
The review is also expected to highlight gaps in both policy and research—for example, limited inclusion of NCDs such as mental health or chronic kidney disease in climate adaptation plans or a stronger focus on climate mitigation rather than health system adaptation. Identifying these gaps will guide future research and policy priorities, such as developing emergency response plans tailored to NCD populations during weather events.
Methodologically, a key strength of this scoping review is its comprehensive and flexible design, which allows for the inclusion of diverse literature types across multiple contexts. Unlike systematic reviews, this approach enables broader synthesis of emerging and complex evidence. The use of established frameworks (Arksey & O’Malley, PRISMA-ScR) and duplicate review processes further ensures rigor, transparency, and credibility.
Limitations
This study had several limitations. First, restricting the search to English-language sources may have led to the exclusion of relevant studies published in other languages, thereby introducing potential language bias. However, efforts will be made to include major international reports that are often available in English and to consider translated summaries when accessible. Second, as a scoping review, no formal quality appraisal of the included sources will be conducted. The focus will be on mapping existing strategies rather than evaluating their effectiveness, which limits conclusions about the success of specific policies. This highlights the need for future outcome evaluations and effectiveness studies.
Third, the wide heterogeneity of sources—spanning academic and gray literature—poses challenges for synthesis, which will be addressed through flexible thematic analysis. Publication bias is another concern, as successful or innovative strategies are more likely to be published, whereas failures may remain undocumented. In addition, by limiting the timeframe to 2004–2025, earlier foundational work may have been excluded, although any seminal pre-2004 sources identified during screening could be considered for contextual relevance.
Despite these limitations, this study has several practical implications. In countries like Iran and other middle-income nations facing climate and NCD burdens, the findings can inform the integration of climate considerations into NCD action plans, such as including air quality and heatwave response protocols. This review also underscores the need for holistic, cross-sectoral policy approaches that align NCD goals with climate change adaptation strategies.
Finally, the review will identify key gaps in research and practice, calling for implementation studies and capacity-building efforts, particularly in low-income or underrepresented regions, to develop climate-resilient health systems.
Conclusion
Climate change and NCDs represent converging challenges for global health, often described as syndemic or twin crises. By systematically scoping the landscape of policy and management responses to this challenge, our review clarifies how current NCD prevention and control initiatives incorporate climate change considerations and identifies what can be done to strengthen these efforts. We hope that the insights gained will support policymakers and health managers in utilizing successful global experiences to develop more effective and integrated strategies for NCD prevention and control in an era of climate change. In particular, for countries grappling with both climate impact and high NCD rates, this study can inform the design of context-specific models that protect vulnerable populations and build healthier and more resilient communities. Furthermore, this study will serve as a foundation for subsequent research and could spur the development of comprehensive “climate-smart” health policies that ensure the sustainability of NCD control efforts under changing environmental conditions.
Footnotes
Acknowledgements
The authors would like to thank all those who collaborated in this study.
Ethical considerations
The study was approved by the Ethics Committee of Mashhad University of Medical Sciences (IR.MUMS.FHMPM.REC.1403.098).
Consent to participate
Not applicable.
Consent for publication
Not applicable. This manuscript does not contain any individual personal data or identifiable information that requires consent for publication.
Author contributions
AGh participated in the preliminary literature review, drafting of the overall protocol, scoping frameworks, and analysis. EH contributed to the drafting of the protocol and initial study methods and reviewed the draft protocol. EMF was involved in drafting the protocol, conducting preliminary analyses, and reviewing the draft protocol. MK contributed to identifying keywords and developing the search strategy. MS contributed to identifying keywords and developing the search strategy. SST contributed to the drafting of the protocol and initial study methods and reviewed the draft protocol. JM participated in drafting the protocol and initial study methods and reviewed the protocol draft. All authors approved the final version of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Clinical trial number
Not applicable.