
Abstract
The burden of type 2 diabetes mellitus in Africa is growing rapidly due to socio-economic changes, urbanization, and substitution of traditional and nutritious, high-fiber diets with ultra-processed, high-energy foods. This review explains the protective value of traditional African diets that contain native grains and fermented foods, but are under threat of westernization and cultural transitions. Moreover, cultural beliefs, social practices, dietary limitations, and gender roles strongly influence diabetes prevention and management practices on the continent. Community-based programs, school nutrition initiatives, and fiscal policies aimed at promoting healthy food settings can be taken as promising interventions. In spite of these considerations, there is an urgent gap in quality research studies especially randomized controlled trials and rural population studies. Culturally sensitive multisectoral strategies are pivotal to reversing the diabetes epidemic in Africa and to achieve sustainable health results.
Keywords
Introduction
The growing prevalence of diabetes mellitus in Africa is a major public health concern, which is aggravated by the rapid socioeconomic shifts and changing eating habits. The continent has experienced a radical nutrition transition over the last 20 years; a transformation that has happened through the replacement of the traditional subsistence-based lifestyles by new modernized food systems that are shaped by globalization and economic growth. This shift has contributed to a surge in type 2 diabetes, and sub-Saharan Africa (SSA) is set to face the greatest global increase in diabetes cases by 2045, as the number of cases is projected to rise from 19 million in 2019 to 47 million.1,2
This epidemiological change is consistent with the dual burden of malnutrition as undernutrition is associated with over nutrition, resulting in an increase in the risk of non-communicable diseases (NCDs) including diabetes, obesity, and cardiovascular diseases. The key feature of this nutrition change is the abandonment of high-fiber, vegetarian diets, based on the use of whole grains, legumes, starchy roots, and vegetables, and little animal products, in favor of processed, energy-dense foods rich in refined sugars, saturated fats, and sodium. Traditionally, African diets focused on nutrient-rich staples such as millet, sorghum, cassava, and local vegetables, which contain protective factors against metabolic diseases due to their high fiber content and low glycemic indices. But recent reports indicate a sharp change in consumption of ultra-processed food (UPF) like sugary drinks, snacks, and fast food which replaces these traditional components. For instance, in SSA, UPF consumption has increased exponentially, and is associated with increased body mass index (BMI) and obesity prevalence, as populations shift to higher calorie-density foods, replacing minimally processed foods.3,4
Urbanization accelerates these changes. The urban population of SSA increases by 4.1% per year, doubling the global rate, creating unplanned settlements that restrict access to fresh food and promote the consumption of processed foods which are more affordable.2,5 This is further compounded by westernization where economic development and media coverage legitimize high-sugar, high-fat diets resembling those of high-income nations and undermine the cultural inclination toward traditional fare. The shift toward refined carbohydrates has increased BMI and prevalence of diabetes among such groups as the Maasai, highlighting the metabolic burden. 6
In spite of these obstacles, the traditional diets in Africa provide a chance to prevent and control diabetes. Plant-based diets, which are high in fiber and antioxidants, can be revitalized to reduce risks, as demonstrated by reduced NCD rates in adherent populations. Culturally sensitive interventions, which tackle urbanization and westernization, are needed to capitalize on these diets during transitions.5,7 This narrative review discusses the effect of traditional diets and cultural beliefs on managing diabetes in Africa with special focus on methods of re-inverting the negative changes.
Methodology
An extensive literature review was carried out to draw up existing scientific findings on the role of traditional diets and cultural beliefs in preventing and managing diabetes in African populations. To select peer-reviewed journal articles in reference to the African situation, four large academic databases (PubMed, Scopus, Web of Science, and Google Scholar) were searched systematically, and further searching was done in regional publications, as well as gray literature to provide wide geographic and cultural coverage of the African situation.
The search period was mainly the publications between January 1, 2019, and September 30, 2025. This timeline was selected to ensure that the most up to date information on nutrition shifts, epidemiology of diabetes, and culturally-sensitive health interventions developing in Africa are incorporated.
Search strategy and keywords
A search of the literature was performed with a mixture of free-text keywords and controlled vocabulary terms (including MeSH where it is relevant) to ensure that as many dimensions of the topic could be covered as possible. Key terms included: “Sub-Saharan Africa,” “Traditional African diets,” “indigenous grains,” “fermented foods,” “diabetes prevention,” “diabetes control,” “dietary patterns,” “nutrition transition,” “metabolic health,” “bioactive compounds,” “food practices,” “cultural beliefs,” “body size perceptions,” “food taboos,” “gender roles,” “food insecurity,” “food access,” “processed food marketing,” “urbanization,” “school feeding programs,” “urban agriculture,” “community gardens,” “food policy interventions,” “randomized controlled trials,” and “policy evaluation.” Search results were refined with Boolean operators like AND, OR and NOT, and database-specific syntax. Reference lists of key studies and pertinent reviews were also screened manually to find other relevant publications in addition to the first electronic search results.
Eligibility criteria
The priority was given to peer-reviewed journal articles published in English within 2019–2025.
Included studies were conducted in African countries or focused on populations of African ancestry.
The areas of research included traditional diets, indigenous foods, cultural food practices, barriers to healthy eating, diabetes prevention/control interventions, and associated policy measures.
Eligible study designs included human studies, including randomized controlled trials (RCTs), cohort studies, cross-sectional studies, community-based studies, qualitative studies on cultural beliefs and practices, and policy review reports.
In vitro or animal-only studies, preprints, dissertations, and conference abstracts and other types of non-peer-reviewed materials were excluded to maintain high-evidence standards.
Study selection and screening
Titles and abstracts from database searches were systematically screened by two independent reviewers against eligibility criteria. Potentially relevant full-text articles were then retrieved and assessed independently by the same reviewers. Disagreements were resolved through discussion to reach consensus, ensuring transparency and minimizing selection bias.
Data extraction and synthesis
Key features of the studies, such as design, population, dietary components, intervention details, diabetes related outcome, and sociocultural understanding were captured using a standardized data extraction tool. Special attention was given to clinical trial data, including Tanzanian SSAs, studies of native grains and fermented foods, and qualitative studies of cultural beliefs about diet and diabetes risk. Food insecurity, affordability, marketing factors, and challenges of city living were listed among the barriers to healthy traditional diets and the community and policy-level facilitators (e.g. school feeding programs, urban agriculture, fiscal policies favoring traditional foods, etc) were listed. Existing gaps, particularly the relative lack of RCTs and culture-specific diabetes self-management education, informed future research priorities. Narrative synthesis organized findings thematically into descriptive summaries and tables, collating evidence on consistencies, discrepancies, and limitations across studies.
Quality assessment
Two independent reviewers conducted systematic critical appraisal of all included studies. Assessments systematically evaluated methodological transparency (clear reporting of methods), data credibility (appropriate analysis, reliable measures), sample adequacy (sufficient power where applicable), relevance to African contexts, risk of bias domains (selection, confounding, measurement where identifiable), and generalizability. Studies were categorized as high-quality (robust methods, low identifiable bias, strong African applicability), moderate-quality (minor limitations such as self-report or smaller samples), or low-quality (major bias; excluded from synthesis). Only high- and moderate-quality studies informed the review findings, with greater weight assigned to RCTs, longitudinal studies, and culturally contextualized qualitative research. Key limitations across studies such as predominant urban focus, reliance on self-reported dietary data, and short intervention durations, were explicitly noted and considered when interpreting evidence strength.
This methodology was used to guarantee the development of a solid, culturally contextualized evidence base that sheds light on the impacts of traditional diets and cultural beliefs on diabetes outcomes in Africa and which forms a strong starting point to evaluate the effectiveness of interventions and determine the critical future research and policy priorities.
Traditional African diets in diabetes prevention and control
The themes presented in this review have logical progressions driven by rapid urbanization in sub-Saharan Africa. The role of urban development and economic change has enhanced food insecurity and diminished access to traditional foods, increasing the shift toward ultra-processed, energy-dense diets. These shifts in diet interplay with culturally instilled beliefs, perceptions of body size, and social food practices, collectively influence the risk and management of diabetes.8,9 This interconnected pathway is the foundation of framing diabetes in the context of analyzing the dietary, cultural, and policy-related evidence as will be provided in the sections below.
The rise of diabetes mellitus presents unique and new public health challenges on the African continent; the underlying causes of this phenomenon are multifactorial and often intertwined with genetics, the environment, and lifestyle. The unique cultural and dietary practices on the African continent, as opposed to high-income economies, present some challenges associated with the prevention and control of diabetes.10,11
Although a number of reviews have focused on the epidemiology of diabetes, dietary patterns, or lifestyle interventions in sub-Saharan Africa, few have combined traditional dietary practices with culturally-infused beliefs and food-system transitions within one framework,5,12 . The review uniquely synthesized evidence on indigenous African diets, cultural perceptions of body size, traditional healing practices, and structural determinants like urbanization and food insecurity, thus providing a culturally contextualized approach to the prevention of diabetes and its management in Africa.
In sub-Saharan Africa, medical therapy for diabetes is scarce and expensive, causing many patients to turn to traditional therapies. A literature review published in 2025 showed that individuals with diabetes in sub-Saharan Africa frequently prefer traditional therapies. These therapies include spiritual healing or prayer sessions and traditional remedies, such as saltwater, bitter vegetables, and local plants, to neutralize and dilute blood glucose levels. 13
Besides the various traditional remedies, religious and fasting practices have shown various benefits, including improving physical health by reducing various chronic illness risk factors and psychological health by enhancing one’s sense of well-being. These practices, however, also require some sort of planning to mitigate some of the challenges that come with it, especially when it comes to diabetes patients 14
The risk factors associated with diabetes could be counterbalanced with traditional African diets, which mainly consist of unprocessed grains and fermented foods. However, because of the socio-economic and cultural transitions of the continent, the traditional diets are gradually being abandoned. Furthermore, the socio-cultural environment and practices are determinants of health behaviors, which include the risk of diabetes. The potential of traditional diets for diabetes and its complications is still underutilized for diabetes control in African populations, as seen in the clinical studies and the potential role of bioactive elements in traditional diets as a control mechanism for diabetes.15–17 Innovative clinical integration of plant-based traditional diets, rich in indigenous grains and vegetables, improves diabetes outcomes through enhanced insulin sensitivity, lower HbA1c via antioxidants/fiber, and sustainable patient adherence via culturally tailored counseling. 18
Evidence from studies
A cross-sectional study was done in Tanzania that was focused on Dietary patterns and diabetes mellitus among people living with and without HIV. This study identified dietary patterns using Principal component analysis (PCA) and Reduced rank regression (RRR). The PCA identified two major dietary patterns, that is, vegetable-rich pattern (VRP) and vegetable-poor pattern (VPP) whereas RRR identified one dietary pattern, that is, carbohydrate-dense pattern (CDP). In comparison to females, males had higher adherence to VPP and CDP, but less to VRP. Higher socioeconomic status was associated with higher adherence to VRP and VPP but low adherence to CDP. Compared to younger people, older people had lower adherence to VPP. High adherence to CDP or VRP was positively associated with prediabetes. Higher adherence to VRP was associated with a borderline decrease in diabetes. No association was observed between VPP with either prediabetes or diabetes. 19
Another study that explored the perception and preventive practices among diabetes patients in rural areas of Nigeria, more particularly the Efik people that inhabit areas of Cross River State. Although this study had a few limitations like the use of secondary data and some missing data; the study made important insights that give insight into the impact various cultural and religious beliefs have on the awareness and occurrence of diabetes. This study mentions the use of “Fattening Rooms” within the study population. These rooms are used to make young women more appealing toward future partners. It involves isolating them, overfeeding them. This coupled with the diet of foods high in starch and calories as well as the lack of physical activity all add up to cause insulin insensitivity and a higher occurrence of diabetes. 20
Role of indigenous diets
Traditional African diets consist of a very large variety of food components and methods of preparation. Some of these include the use of fermented foods and drinks as well as various indigenous grains. 21 However, cultural norms, social identity, and health and body image perceptions have a strong impact on the sustainability and uptake of indigenous diets, which can either enhance or weaken their protective value against diabetes.
A Randomized controlled trial conducted in the Moshi district in the Kilimanjaro region of northeastern Tanzania has provided evidence that supports the use of the “African Heritage Diet” that was commonly utilized in that area. This diet is rich in green vegetables, legumes, plantains, root and tuber crops, including cassava and taro, and whole grains (millet, sorghum), providing dietary fiber and bioactive compounds like polyphenols, known for their anti-inflammatory properties and beneficial metabolic effects. This diet also promotes a favorable gut microbiome composition and production of beneficial metabolites. 15
In addition, emerging evidence suggests that increasing microbiota awareness is a key driver for dietary adherence and metabolic health. Recent research indicates that higher microbiota literacy is significantly associated with improved adherence to fiber-rich patterns like the Mediterranean diet and correlates with lower markers of central obesity, such as reduced waist and neck circumference. 22 This underscores how gut microbiota literacy can support culturally rooted healthy dietary patterns for chronic disease prevention.
This study also emphasizes the potential health benefits of traditional fermented beverages. The fermentation process enriches these beverages with various bioactive metabolites and microbes which improve various immunologic functions and responses within the body. It has also been noted that the consumption of these fermented beverages should be balanced against risks such as the alcohol content and potential mycotoxin contamination. 15 Other benefits of fermentation are that it amplifies plant-based bioactives (e.g. peptides from grains), promoting metabolic effects like favorable microbiome shifts and inflammation reduction, as evidenced in heritage diet trials integrating these into the management of diabetes. 18
The risk of diabetes seems to be reduced in vegetable rich diets which reflects the beneficial effects of vegetables and fruits intake since it is known that vegetable and fruits contain antioxidants that may reduce insulin resistance and β-cells apoptosis thus reducing the risk of diabetes. 20
Cultural beliefs affecting diabetes prevention and control in Africa
With changing dietary patterns in the face of urbanization and food insecurity, cultural beliefs and social norms play a critical role in influencing how people perceive risks of diabetes and respond to dietary recommendations. The cultural implications of food, body size, and illness affect daily eating patterns and health-seeking behaviors, which reinforce or decrease the metabolic effects of dietary shifts in the previous section.8,9
Cultural beliefs and food practices
Studies in Uganda and Ethiopia show that communal eating, food symbolism, and social obligations, especially during ceremonies and family gatherings, make restricting portion sizes or changing staple foods very difficult. 23 In Benin, fruits and vegetables are sometimes seen as “foods for the poor,” reducing their desirability despite their health benefits. 24 Furthermore, in some settings, being overweight is viewed positively, symbolizing wealth and health, so weight loss or dieting may meet resistance or even stigma. 13 Such culturally specific perceptions imply that interventions related to diabetes should take into consideration local beliefs, food meanings, and social norms and not just offer biomedical instructions regarding the diet.
Perceptions of body size and diabetes risk
Perceptions of body size significantly influence diabetes risk across Africa. In most societies, being overweight is linked to health, prosperity, and social standing, whereas being thin is associated with poverty or illness, and therefore, personal weight is underestimated and less attention is given to the dangers of obesity. Studies indicate that such cultural ideals discourage weight control and delay recognition of diabetes risk, highlighting the importance of culturally sensitive intervention in the prevention and treatment. 5
Knowledge of body size as a risk factor for diabetes
Studies show that the majority of the population are aware that obesity is a modifiable risk factor for type 2 diabetes, along with unhealthy diets and physical inactivity. Between 56% and 95% of participants in many quantitative studies identified excess weight as a diabetes risk factor. 5 Qualitative studies from countries like South Africa show awareness of health consequences related to excess weight, including diabetes, though some populations underestimate the risk or perceive obesity only as very severe obesity. 25
Despite generally moderate to high knowledge of the link between body weight and diabetes risk, weight underestimation is widespread. In overweight or obese individuals, 79% of individuals who were overweight and 85% of those who were obese understated their own weight, with over 50% underestimation in most studies.26,27 This underestimation is partly attributed to the normalization of overweight in African societies and the misconception that obesity means only morbid obesity. Many individuals perceive their ideal body weight as lying between the midpoint of normal weight and the upper limit of overweight, often describing this ideal as “not too skinny but not too fat.” 5 Since type 2 diabetes develops at lower body weights in SSA than in high-income settings, the perception that overweight is the desirable body weight nevertheless carries a higher risk. 20 This perceptual gap carries heightened metabolic consequences, as greater obesity awareness has been shown to reduce food cravings, waist circumference, fasting glucose, and triglycerides in overweight/obese adults. 28
Cultural perceptions of body size in Africa
In the prevention and control of diabetes, one of the key factors that plays a significant role is perceptions toward body size. In many African communities, a larger body size is often positively perceived as a symbol of health, wealth, fertility, and prosperity, which contrasts with global medical perspectives linking overweight and obesity to increased diabetes risk.5,29 This leads to underestimation of personal weight and weakens the perceived urgency to prevent or control diabetes related to obesity because excess weight is culturally valorized.
The cultural notion that a fuller body indicates good health affects the dietary practices by encouraging the consumption of energy-rich traditional diets high in carbohydrates and fats, considered necessary to achieve or maintain this ideal body shape. 29 In some cultures, traditional fattening practices, particularly for women, are a ceremonial expression of cultural identity and fertility, which are unrecognized risk factors of diabetes. 20 The combined effect of dietary patterns and the widespread prevalence of a sedentary lifestyle in rapidly urbanizing African societies has been suggested as one contributory factor to the rising incidence of diabetes mellitus on the continent. The findings on participants’ knowledge and perceptions of body size and diabetes risk are summarized in Table 1.
Knowledge and perceptions of body size and diabetes risk.

Traditional healing, food taboos, and gender roles in food decision-making
In several African countries, social customs and cultural insights, including healing approaches, food restrictions, and gender responsibilities, influence diabetes treatment and prevention. These issues shape one’s attitudes toward the condition, treatment-seeking behaviors, dietary choices, and overall health outcomes. 13 In the following section, we will discuss how each of these issues impacts the management of diabetes across the African continent.
Traditional healing practices in diabetes care
Most rural and traditionally centered populations in Africa and parts of the world consider diabetes as a chronic condition of “curse, spirits, and moral failing” when in fact, diabetes is more of an issue of “insulin production and blood sugar management.” Similarly, People with diabetes often seek spiritual or traditional healers and, in addition to receiving care from health care professionals. 30
Such practices can range from the usage of local herbs and plant-based treatments to engaging in spiritual rituals, prayers, or ceremonies meant to expel evil forces or restore spiritual balance. It remains the most preferred option due to its low cost, accessibility, and congruence with the local health and disease beliefs. The use of traditional medicine among African people with diabetes is high, with records showing an average prevalence of 50% and ranges from 12.4% to 77.1% across different countries. 30 Oftentimes, traditional medicine is used alongside conventional medicine, with 35.4%–88.4% of patients combining both systems. However, the use of traditional medicine is hidden from health care systems most of the time (63.8%–91.3%) which poses risks due to a lack of patient-provider communication concerning potential drug-herb interactions and side effects. 31
Food taboos and their impact on diabetes management
Diabetes prevention and control is largely influenced by the food taboos and beliefs within the different cultures in Africa. The traditional African diet is based on carbohydrate staples such as maize, millet, and sorghum as well as plantains and yams, commonly made into fufu, ugali, banku, and nshima. In various African societies, some food taboos prevent the consumption of certain protein rich animal foods and some vegetables for spiritual and cultural reasons, as well as for some perceived health issues. While those taboos might be important for cultural identity, a lack of dietary diversity significantly complicates the control of diabetes. 12
Food taboos are culturally rooted traditions in many African communities that prohibit the intake of specific foods based on health, spiritual, or social concerns. These taboos may include limitations on specific foods, fruits, and vegetables during illness or certain life phases. In the context of diabetes management, such taboos may negatively affect dietary diversity and nutritional adequacy, which are vital for glycemic control. Some African societies, for example, forbid the use of protein-rich meals or particular fruits deemed “hot” or “cold,” potentially limiting access to balanced nutrition required for diabetic management. 32 Likewise, the price and accessibility of suggested diabetic foods, including some fruits and veggies, can make compliance with prescribed diets more difficult because of some of these taboos and issues. 33 Recent studies in Sub-Saharan Africa highlight how food taboos combined with food scarcity and socioeconomic difficulties lead to poor diets that negatively affect diabetes management and control glucose levels. 34
Additionally, food taboos pose psychological and social barriers to diabetes self-management. Patients deal with the social pressure of families and communities encouraging the consumption of forbidden and unhealthy foods, which adds to the already complex task of integrating traditional diabetes care practices with clinically recommended dietary management. The sociocultural factors contributing to the friction in diabetes care and management in Sub-Saharan Africa include the misconceptions that modern diabetes care is ineffective and even harmful, and a strong inclination toward the use of herbal remedies and diabetes care practices. 35
Economic factors, in particular poverty, worsen dietary noncompliance. Eating suboptimal diets and skipping prescriptions are ways some patients cope with the costs of prescribed foods and services. The intersection of these cultural, social, and economic factors presents a strong case for the need to include these factors in the design and delivery of diabetes self-management educational materials. To improve the integration of diabetes care with local customs, including local dietary practices, educational strategies for patients with diabetes should engage faith leaders, traditional healers, and peer support networks. 36 The key cultural factors affecting diabetes prevention and control in African contexts are summarized in Table 2.
Key cultural factors affecting diabetes prevention and control in African contexts.

Gender roles in food decision-making
Culturally influenced attitudes and gender norms shape the food people eat and how they manage diabetes. In some African cultures, men control the types and quality of food, but it is the women, because of their food preparation roles, who are tasked with the most diabetes care diet adjustments. Where social norms do not dictate women to prepare food that is enjoyed by men, they still do so, emphasizing the enjoyment of food that is least suited for diabetes management. On the other hand, women, who are seen as the gatekeepers to food, face the biggest impact, due to low income, poor food options, and lack of access to affordable, nutritionally rich food. 37
Barriers to maintaining healthy traditional diets
The erosion of the healthy traditional diets is not a phenomenon that takes place in isolation but rather the product of the interplay between urbanization, food insecurity, cultural preferences, and economic limitations. These combined forces enhance dependence on ultra-processed foods and constrain the practicability of culturally suitable dietary guidance, especially in rapidly urbanizing and resource-constrained environments.8,9
Food insecurity, cost, and accessibility
Facing a lack of adequate food is a major problem in Africa. Around 140 million people, or one in five Africans, were classified as suffering from severe food insecurity in 2022. That is twice the estimate for other parts of the world. In Burkina Faso, Mali, Niger, and South Sudan, more than 50% of people face undernourishment or food insecurity, a major disparity in the region. 38 Poverty makes it impossible to buy and access quality, nutritious, and culturally appropriate food, and many people are forced to buy cheaper, ultra-processed foods, which are only energy-dense. 8
Recent reports in Ethiopia show levels of dietary non-adherence of 31.8% in Addis Ababa and 62.5% in Dire Dawa, and 42.4% in central Ethiopia. Food cost, inadequate access to fruits and vegetables, lack of dietary education (up to 83%), and the inability to purchase healthy diets (71%) are cited as key barriers by diabetic patients. In Addis Ababa, cost and inaccessibility of markets were two of the most outstanding factors that led to the poor adherence. Lack of adequate dietary knowledge and affordability were the most commonly encountered barriers in Dire Dawa. High prices, and low frequency of markets as well as the distance to travel were also found to be significant impediments to healthy nutrition by Central Ethiopian patients, particularly in rural areas.39–41
In a cross-sectional study in Ghana, Ashanti region, dietary non-adherence in people with diabetes was reported to be 39.4%. Unavailability (84.6%), inaccessibility (80.8%), and unaffordability (60.1%) of healthy foods were cited as the main barriers. 42 In western Kenya, extreme food insecurity nearly doubled the probability of experiencing difficulty in seeking medical treatment among individuals living with HIV and NCDs; this was attributed to the cost of transportation and the trade-off between the food and care costs. 43 In urban slum areas, 93% of residents are moderately to severely food insecure, and as low in dietary diversity as rural populations. Extensive institutional inefficiencies and lack of resources also restrict access to and affordability of food among vulnerable groups. 8
Cost and urbanization-related transitions
The expansion of cities and the development of peri-urban regions tend to reduce the accessibility and physical availability of fresh and traditional staples in terms of affordability. In slums, up to 60% of the urban population in Africa has unstable access to affordable healthy food. Malawi and Tanzanian data demonstrate that urban residents face more ultra-processed and convenience foods but have a lower tendency to prepare their meals at home. To the urban poor, the rising cost of fresh food items hastens the changing trend of consuming more processed meals over traditional foods because of the affordability of the latter. 9
Marketing and availability of processed foods
The processed food industry is making ultra-processed, energy-dense foods more accessible and more attractive in urban African environments through aggressive marketing and the consolidation of supermarket chains. These food items are now dietary staple sources in Malawi and Tanzania due to a lack of time and urbanized living situations. 9 The proportion of food budgets spent by urban households in Southern and Eastern African cities on processed foods has risen to 63% as opposed to 36% in rural locations. Home-cooked, traditional meals have often been replaced by street and snack foods, particularly in urban families with limited time and working women.9,44 Development of preference toward globally standardized processed foods through targeting advertising campaigns around schools leads to an increase in cases of childhood obesity and juvenile diabetes. 45
Cultural shifts due to urbanization
Urbanization is linked to the loss of communal eating patterns and traditional eating habits, a trend worsened by a growing dependence on street foods, processed snacks, and restaurant meals.9,44 This is further hampered by the lack of individualized nutritional counseling and the low number of nutrition education programs within most low-resource urban and peri-urban health facilities.39,46 Changes in social norms and increased time pressures are eroding the process of imparting virtuous, traditional eating habits, especially to youngsters living in massive urban communities.9,44
Community and policy-level interventions
The increasing burden of type 2 diabetes in Africa that calls for a paradigm shift from predominantly clinical management of the disease to holistic approaches that address socio-economic and environmental determinants of health. Community and policy-level interventions are essential for creating supportive environments that promote traditional healthy diets and reduce exposure to factors driving the diabetes epidemic. This section synthesizes evidence on key intervention domains, including community-based programs, school nutrition, and fiscal policy.
Community-based programs and environmental shifts
Adapting global evidence to local realities, community-based interventions have proven real-world applications. One well documented example is the “Lifestyle Africa” program implemented by CHWs in South Africa. Another practical outcome was the demonstration of its cost-effectiveness, with an incremental cost-effectiveness ratio of $3443 per quality-adjusted life year (QALY) gained, which made it a financially feasible model in settings where resources are limited. 47 Adaptation to local realities ensured the program’s success, including local recipes, inexpensive food options, and group support sessions that were in tune with communal cultural practices.48,49
Food insecurity and the high price of healthy foods are cited as seemingly universal barriers in the systematic review, providing practical guidance for planners and program designers. 50 This approach was backed in a meta-analysis where community-based programs created a statistically significant reduction in HbA1c (−0.32%, p = 0.006) and fasting blood glucose levels, proving its geographical influence on clinical outcomes. 51 The parameters set forth for these models, such as accessibility, cultural acceptability, and having the community maintain ownership, can be applied to environmental interventions like urban agriculture and community gardens, which act as living classrooms for nutrition education and rejuvenate cultural ties to healthy eating.52,53
School feeding programs as a foundational intervention
Schools represent a critical yet underutilized setting in the inculcation of lifelong healthy dietary behaviors. The qualitative study from rural South Africa offered direct evidence from school managers, who revealed that their feeding programs were primarily meant to appease short-term hunger, and that the menus were based on cost and ease of preparation rather than on the nutritional value of food for long-term health. Regarding the stark practical gap of an infrastructure that gets little use for NCD prevention, it has been observed that the management of schools often views the issues related to school nutrition and non-communicable diseases as minor. This presents a clear action point for policy: the revision of the national school feeding guidelines to incorporate objectives for diabetes prevention and to include traditional foods and nutrient-dense foods into the food environment for the next generation. 54
Fiscal policies: Taxes and subsidies
Fiscal policies are practical and evidence-informed mechanisms that will influence all aspects of the food environment. The policy landscape provides practical evidence that taxes on sugar-sweetened beverages (SSBs) can be implemented in sub-Saharan Africa, even in the face of alcoholic industry opposition. A multi-country analysis identified that successful execution relied on specific tactics, including the formation of coalitions of public health advocates and policymakers and the designation of tax revenue for health programing, both of which increased public acceptance. 55
The potential health impact is substantial and measurable. For instance, a modeling study conducted in South Africa estimated that a 20% tax on fruit juice could avert over 100,000 obesity related cases and generate ZAR 3.5 billion (just under USD 185 million) in revenue over 10 years, and it is far cost-effective from both a societal and health of health care perspective. 56 Such findings provide policymakers a clear evidence-based financial mechanism to disincentivize unhealthy consumption, beyond SSB alone. Although the reviewed literature offers limited direct evidence on subsidies promoting traditional food consumption, the documented success of taxation policies provides a reasonable justification for reallocating tax revenues to subsidize healthy, traditional foods including indigenous fruits and vegetables thereby improving their affordability and accessibility. 57 Figure 1 presents a conceptual framework integrating community-based, school nutrition interventions, and fiscal policies, illustrating how these evidence-based strategies interact to create supportive food environments and achieve a sustained reduction in the burden of type 2 diabetes in Africa. The framework synthesizes evidence from dietary, sociocultural, and policy-focused studies, is grounded in literatures highlighting the protective role of traditional, nutrient-dense African diets, the influence of sociocultural contexts on dietary behaviors, and the effectiveness of population-level policy interventions. Informed by a socio ecological and food environment systems perspective, the model reflects a shift from individual, clinically oriented database management toward population level strategies that address broader socio economic and determinants of health, Though interconnected behavioral, nutritional and metabolic pathways, community programs, showing how community programs, school based nutrition initiatives, and fiscal measures interact to support long reductions in diabetes burden.
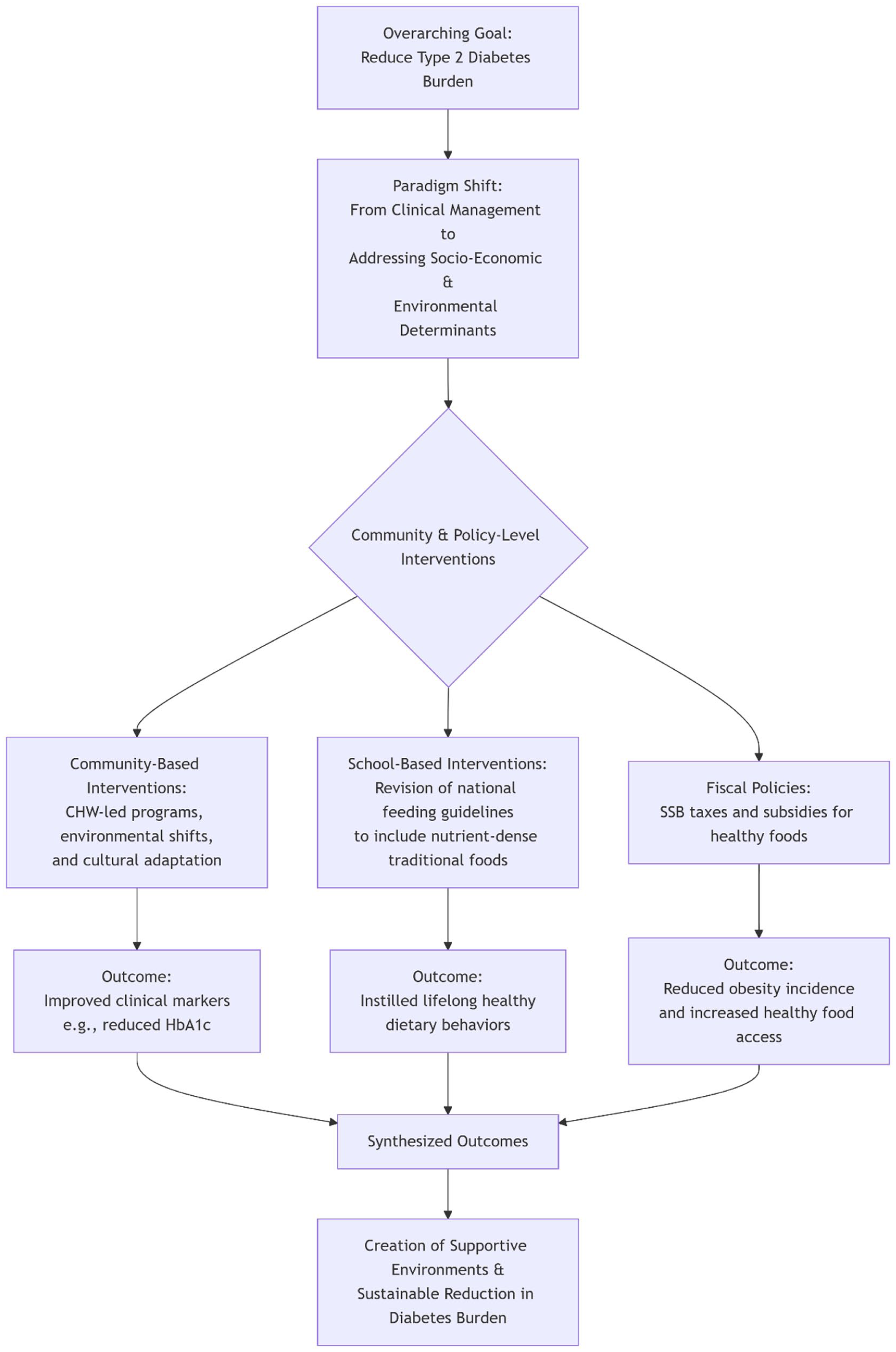
Integrated community school and policy-level interventions for sustainable reduction of type 2 diabetes burden.
Research gaps and future directions
Research gaps
One of the main contributions of this review is identification of research gaps that emerge at the intersection of diet, culture, and structural determinants, rather than within isolated biomedical domains. Through this integrative perspective on diabetes prevention and control, the review identifies the scarcity of culturally tailored randomized controlled trials and policy analyses that capture the real-world African food contexts and beliefs.
Africa’s diversity makes rigorous RCT complex, demanding designs that respect local contexts. The lifestyle Africa’s trial, which adapted the US diabetes prevention program for South African Communities, demonstrates both the potential and limits, highlighting the need for culturally adapted interventions that scale across communities. 49
Despite the growing awareness of diabetes mellitus in Africa, there is still a significant research gap remaining that hinders the development and implementation of effective preventive and control measures. Among the major gaps are the lack of adequate RCTs that address the increasing burden of DM in Africa. One systematic review shows that only 60 RCTs were identified across 15 African countries, which is just above one study per country, showing very limited evidence. And the pediatric interventions are scarce despite the growing burden. 58
On top of that, among the studies conducted, 75% were in urban areas, leaving the rural area underrepresented in the evidence base, even though most of the African population is in rural areas. When looking at the geographic disparities, only a few countries account for the majority of the RCTs that are done.58–60
Among these studies, there is a poor retention rate across sub-Saharan Africa, with high dropout rates compromising study validity, and most studies lasted ≤ 6, limiting the ability to draw meaningful conclusions and understand the possible long-term effectiveness of any intervention that is applied.59,61 The main research gaps identified in diabetes prevention and control studies across Africa are summarized in Table 3.
Summary of research gaps identified in the study.

Future directions
Future studies and interventions must focus on prevention and control of diabetes along the full causal pathway, from structural food environment and cultural norms to community-based programs and policy enforcement. To improve and bridge the gap and improve diabetes outcomes across Africa, it is required to make a significant effort to generate high-quality evidence through expanded RCTs and policy evaluation. Research should prioritize areas that are underrepresented, such as rural areas and primary care. 62
In many cases, it has been shown that there is a belief that diabetes is caused by supernatural influences, such as punishment from God. And this cultural belief led to misunderstanding about the etiology, signs and symptoms of diabetes and its control. Studies from Ghana, Kenya and other African countries demonstrated that many of these individuals prefer traditional healers, spiritual interventions, or herbal remedies over conventional medical care. For this integration of community organizations, cultural attitudes, beliefs, and social norms would significantly impact the health behavior of individuals and the community. 63
Healthcare provider education represents a critical component of successful cultural integration. Research indicates that many healthcare workers in African settings lack adequate knowledge about traditional medicine practices and cultural beliefs related to diabetes. Developing evidence-based training programs that prepare health providers to providers to respectfully engage with traditional practices while maintaining clinical safety standards represents an important research priority. 64 The overlapping barriers are illustrated in Figure 2.

Key overlapping barriers to effective diabetes prevention and control.
Future research must prioritize community-based participatory approaches that meaningfully engage traditional healers, community leaders, and patients in intervention design and evaluation. Such approaches can help ensure that interventions are culturally appropriate, sustainable, and effective in real world settings. The growing emphasis on person-centered care approaches that understand biopsychosocial factors influencing diabetes on person-centered care approaches that understand biopsychosocial factors influencing prevention provides a framework for this type of research.49,64
Cost-effectiveness analysis of culturally integrated diabetes prevention and management approaches remains critically needed. While traditional medicine is often more affordable and accessible than conventional care, comprehensive economic evaluations that consider long term health outcomes, healthcare utilization, and social costs are lacking. Such analyses would essentially provide evidence for policymakers considering the integration of traditional practices of national diabetes strategies.64,65
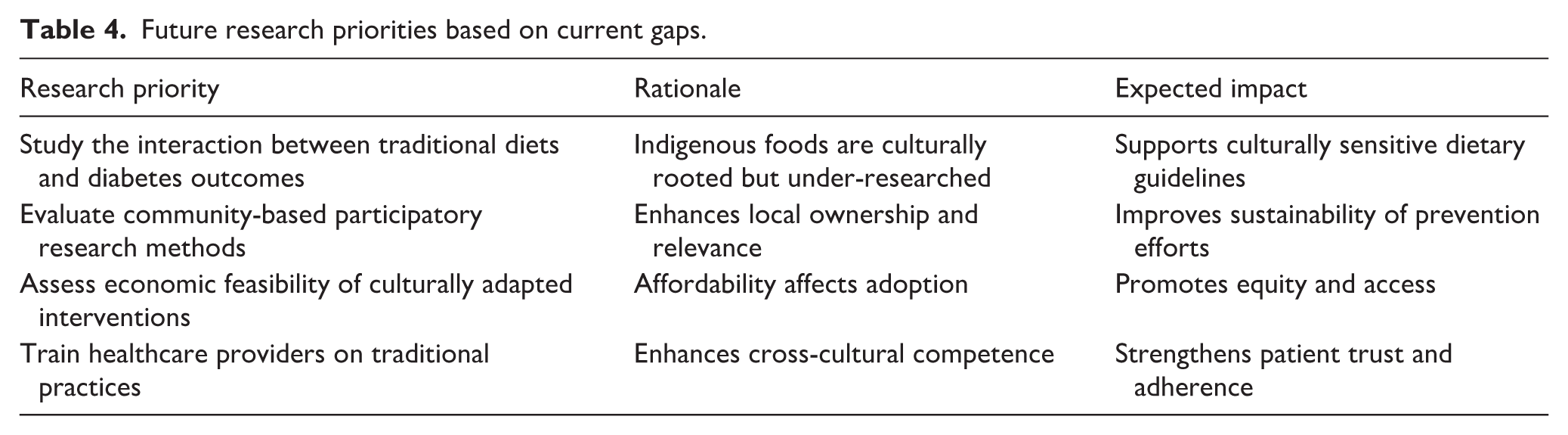
The research gaps identified highlight the urgent need for more rigorous, culturally sensitive, and contextually appropriate research approaches to diabetes prevention and control in Africa. Addressing the Gaps through well-designed RCTs, comprehensive policy, sustainable and culturally appropriate diabetes prevention and management approaches across the diverse African continent. The key future research priorities derived from the current evidence gaps are summarized in Table 4.
Future research priorities based on current gaps.
Conclusion
The current issue of increasing burden of type 2 diabetes in Africa requires a multisectoral, culturally sensitive, and comprehensive approach beyond traditional clinical management. This review has also pointed out the importance of the traditional African diets, which are rich in non-refined grains, fermented foods, and bioactive compounds in the prevention and management of diabetes, but these healthy practices are gradually being replaced by the Westernized, ultra-processed diets triggered by the intensive urbanization and socio-economic changes. The socio-cultural influences, such as local beliefs, gender roles, traditional healing, and food taboos, have a significant impact on health behaviors and diabetes management outcomes, which highlights the importance of culturally-sensitive interventions.
To deal with this epidemic, concerted community and policy measures must be implemented to ensure that there is a favorable environment of encouraging healthy traditional foods to be used and incorporated sustainably. Successful interventions should incorporate culturally relevant community initiatives, school nutrition guidelines related to native dietary habits, and financial strategies, including taxation of unhealthy foods and subsidies on traditional, nutrient-dense foods. Notably, a critical research gap exists concerning rigorous, context-specific investigations, particularly high-quality randomized controlled studies in underrepresented rural and primary care settings, to produce evidence that informs policy and programing.
To curb the escalating diabetes crisis in Africa, future interventions should incorporate holistic approaches that incorporate cultural context, enhance food security, and empower the communities. Healthcare providers, traditional healers, policymakers, and researchers must collaborate to develop and implement sustainable and evidence-based interventions. This holistic practice promises to maintain the rich African dietary heritage and at the same time fight the diabetes epidemic to enhance the health outcomes in African.
Footnotes
Acknowledgements
The authors acknowledged the researchers of primary studies for this comprehensive review.
ORCID iDs
Ethical considerations
Ethical approval is not required as this was a narrative review.
Consent to participate
Informed consent is not required as this was a narrative review.
Author contributions
Z.G.A.: Conceptualization-Lead, Data curation-supportive, Formal Analysis-Lead, Investigation-Lead, Project Administration- Lead, Supervision-Lead, Visualization-Lead, Writing original draft-Lead, Writing review & editing-supportive; A.S.K.: Conceptualization-Equal, Data Curation-Equal, Formal Analysis-Equal, Investigation-Supporting, Supervision-supporting, Validation-Equal, Visualization-Equal, Writing – review & editing-Equal; Y.A.Z.: Data curation-lead, Investigation-Supporting, Methodology-Lead, Validation-Supporting, Writing – original draft-lead, Writing – review & editing-lead, Prepared Table 1; B.G.W.: Data Curation-Supporting, Investigation- Supporting, Validation-Supporting, Visualization-Supporting, Writing–original draft-Supporting, Prepared Table 2; H.W.N.: Data Curation-Supporting, Investigation-Supporting, Validation-Supporting, Writing original draft-Supporting, Prepared Figure 1; Y.M.T.: Data Curation- Supporting, Validation-Supporting, Visualization-Supporting, Writing original draft-Supporting, Prepared Table 3; Y.B.K.: Formal analysis-supporting, Supervision-supporting, Writing original draft-supporting, Writing – review & editing-supporting; B.L.S.: Formal analysis- supporting, Investigation-Supporting, Visualization- supporting, Writing – review & editing-supporting, Prepared Figure 2; Y.T.T.: Visualization- supporting, Writing – review & editing-supporting; Y.T.A.: Visualization- supporting, Writing – review & editing-supporting, Prepared ![]() .
.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No new data were created or analyzed in this study. Data sharing is not applicable to this research.