
Abstract
Background:
The COVID-19 pandemic drastically increased work demands and stress for medical professionals.
Aim:
To complement knowledge on detrimental long-term consequences of stress, we examine short-term dynamics of the stress processes, especially anticipation of stress and recovery.
Design and methods:
This diary study assessed anticipation of and recovery from work stress as well as individual differences therein related to self-efficacy, optimism, and neuroticism. Before and after up to eight work shifts in winter/spring 2021, 146 medical professionals (42.5% male, Mage = 32.3 years, SD = 10.6) reported their affective well-being, anticipated stress, experienced stress, perceived exertion, perceived recovery, and non-work activities.
Results:
Multilevel models revealed that anticipating stress was associated with already lower affective well-being before the shift, but it did not buffer or amplify associations between experienced stress and affective well-being after work. Lower affective well-being after a shift led to less recovery, which in turn was associated with lower affective well-being following the next shift. Above-average engagement in pleasant activities, and even completing chores, as well as less rumination were associated with more pronounced recovery. Self-efficacy and neuroticism, but not optimism, were associated with affective well-being before and after work shifts.
Conclusions:
Neuroticism and low self-efficacy may place medical professionals especially at risk in medical crises. Promoting leisure activities to support recovery may replenish resources for handling work-related stress.
Keywords
Public health significance
The study addresses as daily activities as predictors for occupational health, specifically recovery from work demands of hospital shifts. The findings offer insights for hospital management, that is, on staff potentially at risk to insufficiently recovering from work demands. At the same time, it highlights the potential of recovery processes through daily activities to maintain and improve the health of medical staff, which experience very high demands in many sectors and countries.
Introduction
During the COVID-19 pandemic, the work demands for medical professionals have drastically increased. 1 This included not only the number of patients, but also the psychological demands, such as fear of transmission. 2 While it is commonly known that increased levels of stress have negative long-term health consequences (for a review see Ref. 3 ), little is known about how daily dynamics of the stress process unfold in medical professionals’ daily lives. Specifically, stress can already emerge before a work shift when high demands are anticipated for that specific day.4,5 This, in turn, may reduce well-being even before the actual work demands are encountered. Following the shift, a person needs to recover to be able to work effectively during the subsequent shift. If this recovery process becomes disrupted, negative performance and health consequences are likely to emerge. 6 Therefore, the first aim of this diary study is to investigate the dynamic interplay between the anticipation of, reactivity to, and recovery from work-related stress. The second aim is to identify individual and behavioral protective factors that may modify these dynamic associations and may buffer against stress and help individuals to recover following a demanding work shift. 7 Understanding the interplay of the stress responses and how to intervene upon them may help to design interventions that aid medical professionals under exceptional work demands similar to the ones experienced during the COVID-19 pandemic.
Stress dynamics over time
According to the classical literature, stress is caused by an imbalance between situational demands and available coping resources when a situation is judged to be relevant and potentially threatening. 8 This is associated with a temporal sequence of different affective and physiological changes. After the exposure to a stressor, negative affect is increased, thus well-being decreased, compared to a non-stressor baseline.9,10 However, when a stressful situation is expected to occur (e.g. a demanding work shift), a state of elevated negative affect may already arise even before the actual stressor is encountered. Thus, the classical stimulus-reaction dynamics can be preceded by an anticipated stress phase.4,11 Once the stressful situation is resolved, recovery occurs which implies a return toward the resting state. 10
Examining reciprocal effects among stress reactivity and recovery has recently received increasing attention in the domain of psychological well-being. For example, people may show stronger responses to minor stressors and require more time to recover from them when multiple stressors occur in short temporal succession. That is, the impact of successive stressors seems to pile-up with insufficient recovery time. 12 This means that the experience of stressors may interfere with recovery which would be required to respond adequately to future stressors. Increased reactivity has in turn been linked with long-term declines in physical and mental health.13,14 Thus, identifying how dynamics between reactivity and recovery unfold in everyday job activities is critical to preventing long-term declines in well-being.
While the dynamics of reactivity and recovery have received considerable attention, anticipated stress has rarely been examined in the context of work. However, because the anticipation period precedes reactivity and recovery, 4 it could have a direct influence on the subsequent phases. For example, emotional reactivity is typically extracted from within-person changes relative to a particular baseline. If a person anticipates stress in an upcoming situation, the emotional state may worsen even before the actual stressor is encountered and also affect well-being during the actual exposure to the stressor (e.g. Refs.5,11). This has not yet been assessed when considering medical professionals’ work stress.
Following the temporal order of anticipation, reactivity and recovery, we derive the following pre-registered hypotheses:
Behavioral and individual factors in stress and recovery
While recurring stressors are typically considered detrimental for psychological well-being, several factors can help to buffer against the negative impact of stressors or help an individual to recover more quickly. These factors can be divided into behavioral variables and individual characteristics.15,16 For example, the activities someone engages in during their time off work may function as a promotive behavioral factor. Specifically, such activities directly influence how people recover from their work demands which, in turn, influences the affective responses to new demands the coming day. Two key factors during non-work time that enhance recovery following a demanding work shift are pleasant social contact and detachment from work. 15 Additionally, physical activity or exercise have also been shown to accelerate the recovery rates after work. 17 In other words, disengaging from one’s duties beyond the scheduled hours and instead engaging in enjoyable activities (with others) can help to maintain a stable state of mental well-being over time by promoting recovery.18,19 On the contrary, ruminating on the events (e.g. from the workday after the shift has ended) relates to prolonged negative affect and thus seems to slow down the recovery process.20,21 These factors are particularly important to understand for medical professionals facing additional demands during the COVID-19 pandemic and beyond as they might indicate potentials for health interventions.
Apart from momentary experiences and activities, relatively stable personality characteristics may explain individual differences in being more or less prone to stronger stress responses and slower recovery processes. 22 One of the key personality characteristics in this context is neuroticism – a personality trait marked by a low tolerance to stress. 22 People higher in neuroticism experience stressors as more intense and experience more negative emotions, such as anger or anxiety.22,23 In contrast, neuroticism does not seem related to how long it takes people to recover after daily stressors. 24 Instead, recovery from stressors takes longer the more people ruminate about the events.21,24 However, because higher neuroticism is associated with engaging more in rumination, 25 rumination and neuroticism have to be considered in tandem in the context of recovery.
In contrast to neuroticism, dispositional optimism may reflect a factor that both reduces the reactivity to a stressor and enhances the recovery process. 26 People high in optimism expect more pleasant and more successful outcomes in various situations. 27 Therefore, individuals with greater optimism may perceive situations as less threatening and more manageable compared to individuals with little dispositional optimism. Similarly, self-efficacy describes people’s beliefs of being able to manage the demands of a situation. Accordingly, high personal self-efficacy can help to buffer against work stress 28 and help an individual to recover more quickly. 29 Recent research has shown that coping self-efficacy has a beneficial effect on medical first responders during the pandemic 30 but it is unclear whether these results extend to daily affective processes and recovery as well as to medical professionals more broadly.
The current study
The aim of the current study was to (a) examine the dynamic process of anticipation of, reactivity to, and recovery from medical professionals’ everyday work stress under exceptionally high demands during the COVID-19 pandemic and (b) identify factors that enhance or reduce stress reactivity and the recovery processes in this context. We designed an ecological momentary assessment study 31 during which medical professionals reported on their experiences before and after their work shift for several days. This method captures the stress dynamics and recovery related behavioral factors as they occur naturally in close temporal proximity to participants’ work shifts. Therefore, the results of this study provide a realistic insight into the stress dynamics of medical professionals alongside potential measures to counter detrimental stress effects.
Methods
Participants
Participants were recruited through distribution of flyers and emails in local hospitals, medical centers, and medical emergency services. Inclusion criteria were: (a) medical staff or medical first responders, who have contact with people (potentially) infected with COVID—19; (b) German speaking. A total of 152 medical professionals signed up to participate in the study; six (3.9%) people were removed from the sample because they participated in the momentary assessments on less than 3 days, as was determined in the pre-registration. Therefore, 146 people (84 female, 62 male) with an average age of 32.3 years (SD = 10.6; range 18–63) were included in the final sample. Most of the participants worked as medical students (n = 42), paramedics (n = 37), or physicians (n = 30), others as nurses (n = 18), medical assistants (n = 14), or other (ambulatory) services (n = 5). A priori simulations for multilevel models with cross-level interactions conducted with Mplus (https://osf.io/rmtgj?view_only=88d43f79568b4ee5b9ab9317e993ad4c) yielded a necessary sample size of approximately 200 participants to detect medium to large effects of between-person differences on within-person associations. The data collection was terminated before the intended sample size was achieved because of time constraints, which we discuss under Strengths and limitations.
Procedure
After receiving ethical approval from the institution’s IRB (Heidelberg University, AZ Fr 2022 1/1), the study was preregistered on the Open Science Framework (https://osf.io/23r56/?view_only=88d43f79568b4ee5b9ab9317e993ad4c). Participants were provided with the information on the study and gave informed consent as part of an online baseline assessment. In this baseline assessment, participants also indicated when their shifts were scheduled to start and when they would end. This information was used to prompt text messages, which were sent out shortly before and immediately after each shift for 8 days and included the link to the shift-related diary questionnaires. Since work schedules and off-days differed between participants, assessments were aligned to each participant’s shifts. Most participants worked for either 3 or 4 days in a row, followed by 1 day off. The baseline questionnaire took at maximum 20 min to complete. The daily diary questionnaires before and after the shift were completed within a maximum of 2 min each. The assessment stopped after the eight full days of pre- and post-shift assessments. All questionnaires were administered via the online platform SoSciSurvey. Participants who completed the baseline questionnaire and at least six momentary questionnaires before or after their shifts were compensated with a financial reward of 20 EUR; participants who completed at least 14 out of 16 momentary questionnaires received 40 EUR.
Data was collected between February 4, 2022 and September 15, 2022. During this time, the number of new COVID19 infections varied between 187,159 and 1,588,891 per week, while the number of deaths per week ranged from 213 to 1934 in Germany according to the WHO covid dashboard (https://data.who.int/dashboards/covid19/). Note that in the winter and spring months, social gatherings including restaurant visits and attending sports events were permitted for individuals with an immunization certificate or negative test result, while the restrictions were largely lifted during the summer.
Materials
The questionnaires were divided into (a) the baseline questionnaire of demographic information and individual characteristics, (b) the recurring diary questionnaire before each shift, and (c) the recurring diary questionnaire following each shift (see Table 1 for an overview). The baseline assessed participants’ demographics (see section “Participants”), as well as neuroticism, optimism, and dispositional self-efficacy with validated questionnaires (references are provided in Table 1). Before each shift, participants reported their affective well-being, anticipated stress for the upcoming shift, their perceived recovery from the previous shift, and how much they engaged in seven different non-work activities after their last shift (Table 1). Following each shift, participants again reported their affective well-being alongside their rate of perceived exertion during the shift.
Overview of questionnaires and included items.
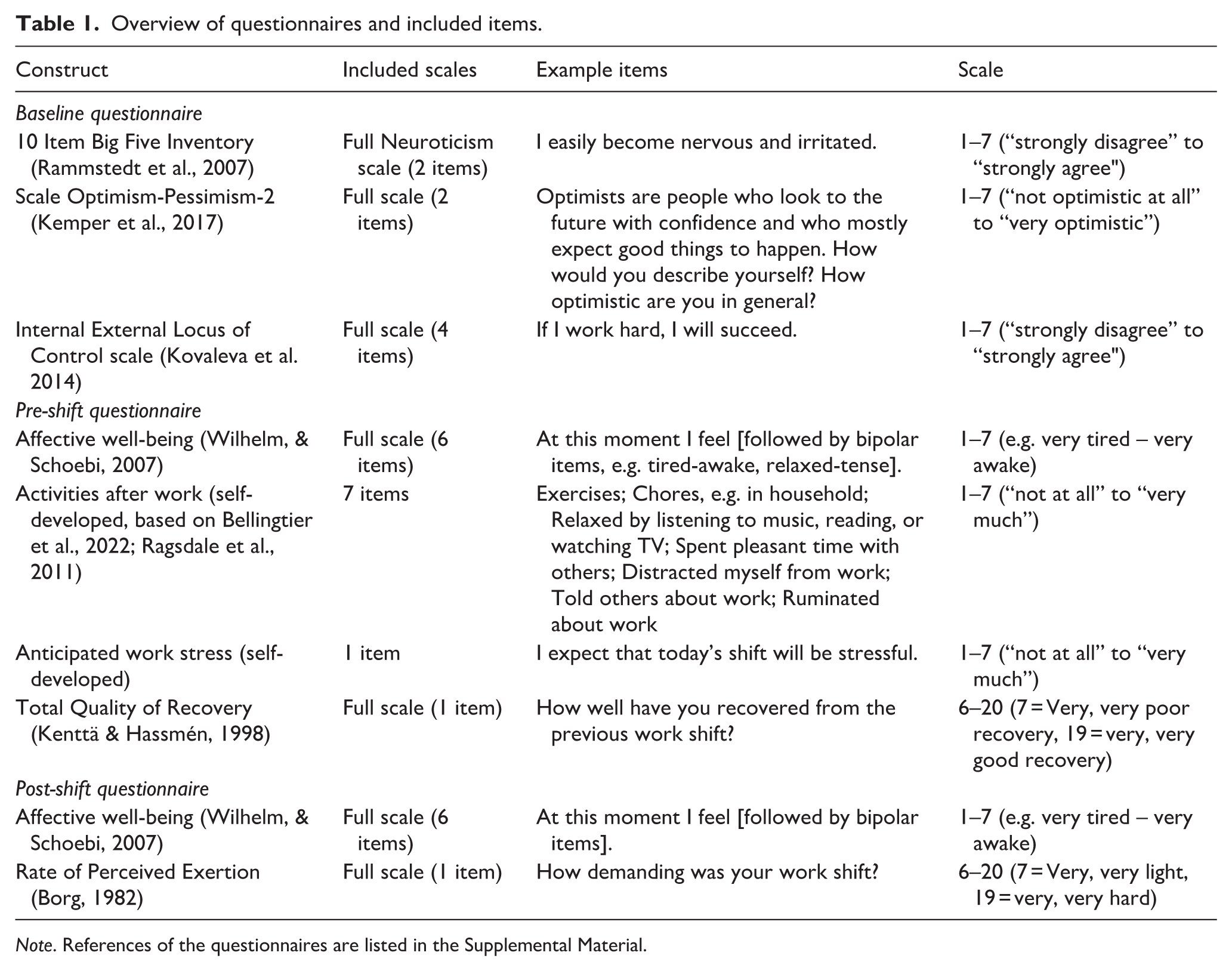
Note. References of the questionnaires are listed in the Supplemental Material.
Data analysis
The 146 included participants provided data from 1078 different shifts. Note that for the different hypotheses, either only the pre-shift, only the post-shift, or a combination of data from pre- and post-shift questionnaires is required. Missing data in pre- or post-shift assessments led to different numbers of observations available for the analyses of the specific hypotheses.
Because both reactivity-recovery dynamics and protective factors show individual differences that may not be represented in group-level findings, we implemented multilevel models. 32 Multilevel models allow for assessing individual-level variations in the overall effects and time-lagged associations, while adjusting for dependence in the data (i.e. multiple data points stemming from the same individual). The models for hypothesis testing were computed using the restricted maximum likelihood estimation procedure in the lme4 and lmerTest packages.33,34 Each model development sequence started with an intercept-only model, which was first extended by including fixed effects of the predictor variables and then random slopes for the predictor variables. Because including random slopes did not improve the models and led to issues with fit and convergence (in all models but one), we report results from models without random slopes except for the model regarding H1. Parameter estimates were standardized using the R package parameters.
In contrast to the pre-registration, we did not operationalize reactivity as the change (i.e. difference) in affective well-being from prior to the shift to after the shift because difference scores have been strongly criticized regarding their reliability and interpretation. 35 Instead, we considered affective well-being after the shift as a proxy for people’s reactivity to their work stress. Before inclusion in the models, all scores for predictor variables that were collected once (i.e. neuroticism and optimism) were centered on their grand mean and all repeatedly assessed variables were centered on the individual-level mean. The anonymized data and analysis code can be found under the OSF registration.
Results
We report descriptive statistics of the variables in Table 2 and illustrate their intercorrelations in Figure 1. For the sake of clarity and conciseness, central results from the multilevel models concerning the hypotheses are reported in the text as standardized coefficients (including 95% confidence intervals) and full model results can be found in the Supplemental Material (Tables S1–S7).
Descriptive statistics of study variables.

Note. iSD = intra-individual standard deviation. No iSD is available for Neuroticism, Optimism, and Self-Efficacy because these measures were only assessed once during the baseline questionnaire.

Within-person (a) and between-person (b) correlations between study variables.
Hypothesis testing
In line with H1, we found that on days when people anticipated more stress, they reported lower affective well-being before their shift, β = −0.18, 95% CI [−0.25, −0.11]. Contradicting H2, people reported lower affective well-being on days with more work stress, β = −0.50, 95% CI [−0.55, −0.44], independent of their anticipated work stress. For full results from the models regarding H1 and H2, see Supplemental Table S1.
Supporting H3a, when people experienced lower than usual affective well-being after a shift, they reported less pronounced recovery until the beginning of the next shift, β = 0.10, 95% CI [0.02, 0.17] (see Supplemental Table S2 for full model results). In contrast, on days when people reported less pronounced recovery from the previous shift at the beginning of a shift, they did not report stronger perceived exertion, β = −0.06, 95% CI [−0.12, 0.00], yet, lower affective well-being at the end of the shift, β = 0.10, 95% CI [0.03, 0.16], which partially supported H3b (full model results, Supplemental Table S3).
As hypothesized in H4a, when participants reported more physical activity, β = 0.12, 95% CI [0.06, 0.17], more pleasant social contact, β = 0.12, 95% CI [0.06, 0.18], and more detachment, β = 0.14, 95% CI [0.08, 0.20], after a shift, they also reported more pronounced recovery until the beginning of the next shift. Surprisingly, performing more chores than usual was also associated with participants reporting more pronounced recovery until the beginning of the next shift, β = 0.13, 95% CI [0.08, 0.19], whereas ruminating more than usual was associated with less pronounced recovery until the beginning of the next shift as predicted, β = −0.12, 95% CI [−0.18, −0.07]. Thus, the results partially support H4b (full model results in Supplemental Table S4).
Next, we analyzed how person characteristics moderate affective experiences and recovery after a shift. Our findings show that people with higher levels of neuroticism experienced lower affective well-being after a shift (affective well-being: β = −0.27, 95% CI [−0.5, −0.09]). Yet, this effect was substantially reduced when the average level of rumination was controlled (see Supplemental Table S5 for full model results). Higher levels of neuroticism did not predict recovery: β = −0.18, 95% CI [−0.38, 0.02]. These results partially support H5a. Partially supporting H5b, people with higher self-efficacy reported better affective well-being after a shift, β = 0.37, 95% CI [0.17, 0.56] but not more pronounced recovery until the next shift, β = 0.19, 95% CI [−0.03, 0.42]. Optimism was not significantly associated with affective well-being after a shift, β = 0.05, 95% CI [−0.15, 0.24], or recovery until the next shift, β = 0.18, 95% CI [−0.04, 0.39] (full model results in Supplemental Table S6).
Exploratory analyses
We observed some correlation between individual personality characteristics and the specific non-work time activities (see Figure 1, Panel B): More neurotic people tended to ruminate more (r = 0.17). More optimistic people and people with higher levels of self-efficacy engaged more in social contact (r = 0.23 and r = 0.20, respectively). Also, people with higher levels of self-efficacy talked more to others about their work (r = 0.18). With increasing age, participants reported less listening to music, reading, or watching TV (r = −0.17), less social contact (r = −0.26), and less talking to others about their work (r = −0.31). Surprisingly, women reported less social contact than men (r = −0.21).
To explore whether specific non-work time activities were especially beneficial for affective well-being for certain individuals, we assessed interaction effects between individual characteristics and non-work time activities in predicting well-being (Supplemental Table S7). The only person-activity interactions occurred for physical activity and were probed using Johnson-Neyman intervals. Specifically, engaging in more physical activity was associated with more pronounced recovery after a shift for people (1) whose level of optimism was lower than 0.64 units above the sample mean, (2) whose self-efficacy was higher than 0.76 units below the sample mean, and (3) who were 23.5 years old or older. The associations for values at the mean as well as 1 SD above and below the mean are visualized in Figure 2.

Interactions of physical activity with optimism (a), self-efficacy (b), and age (c) in predicting recovery.
Discussion
The aim of the current diary study was to examine the dynamic process of anticipation of, reactivity to, and recovery from medical professionals’ everyday work stress. Accompanying these stress-dynamics, we aimed to identify personality characteristics and behavioral factors that enhance or reduce reactivity and recovery processes across several days. The results showed that anticipatory, reactive, and recovery processes are interrelated substantially. First, we found that anticipated stress was associated with lower concurrent affective well-being but did not moderate reactive associations between experienced stress and affective well-being after work. The results regarding lagged associations between affective well-being and recovery suggested a potential vicious cycle with lower well-being after a day of work predicting worse recovery which in turn predicted lower affective well-being after work the next day. Most non-work activities were associated with more pronounced subjective recovery, whereas individual differences only had limited associations with reactivity and recovery processes.
Stress processes
The results from the current diary study illustrate that stress anticipation, affective states after stressful work shifts, and recovery are interrelated over time. We found that anticipating more stress before a shift was associated with lower concurrent affective well-being (H1). However, in contrast to H2, anticipating stress did not change how much the occurrence of stress itself impacted affective well-being after a shift. These results speak against so-called anticipatory coping, 5 that is, people did not seem to take efficient measures to reduce the effects of the anticipated stress (cf. Ref. 36 ). Similar results were observed with anticipated stress concurrently and longitudinally predicting affective well-being but not decreasing the effect of actually occurring stressors. 11 In contrast to previous research, people in the current study did not reliably predict actual stress, which might be partly due to a limited statistical power to detect small within-person associations. Correctly anticipating stress may be difficult in unpredictable environments like acute health care. Note that previous research mainly asked participants to forecast whether a stressor (i.e. a singular stressful event) was likely to occur within the next hours, whereas this study assessed the anticipation of how stressful the entire shift was going to be. While these two types of forecasting are conceptually linked, they are not identical. 5
Turning from anticipation to recovery, lower affective well-being following a shift was associated with diminished recovery until the beginning of the next shift (H3a), indicating that it might be more difficult for people to recover when they felt worse after a shift. Similarly, when people reported lower recovery from the previous shift, they also experienced lower affective well-being after the current shift (H3b), which could indicate a potential vicious cycle. These dynamics may thus be the basis for negative long-term health consequences of insufficient recovery. 6 However, interestingly, our data suggests that less complete recovery from the last shift may not be associated with perceived exertion from the current shift. Thus, even though affective well-being and recovery seem to become diminished over time, the perceived demands of the work were not affected. This suggests that an accumulation of stressors (e.g. stressor pile-up 12 ) may not change how individuals perceive the demands of a situation, but may be limited to their affective reactions to them. Importantly, while previous work mainly studied such stress processes in time scales ranging from minutes to a few hours,11,36 the current study demonstrates that anticipatory and recovery processes also occur over longer periods, at least within a work context. We thus extend theoretical frameworks on stress anticipation and recovery 5 by demonstrating that different time scales need to be considered and could have distinct implications for mental and physical health. 6
Protective and promotive factors
In line with hypothesis H4a, engaging more in the leisure activities physical activity, pleasant social contact, and distraction after a shift was associated with more pronounced subjective recovery until the beginning of the next shift. Surprisingly, this was also true for doing more chores, contrary to H4b. The results align with previous research indicating that pleasant activities and activities that support detachment from work can promote recovery (e.g. Refs.15,17). Thus, encouraging people to engage in pleasant or productive non-work activities could be useful to promote recovery, which in turn, might “replenish” resources needed for emotion regulation. Importantly, people still need to have energy for activities after work. If the work demands are too high and overly straining, people will be too exhausted to engage in beneficial non-work activities. Doing chores might also work as a distraction 37 or could instill a sense of accomplishment 38 which could improve recovery. However, this has not been supported universally with some research indicating that doing more housework can lead to less pronounced recovery. 39 Alternatively, people might generally profit from activities that make them feel happy while engaging in them. Experiencing positive emotions like feelings of happiness while performing work related activities or housework can buffer against the potential negative effects of those activities and stimulate recovery. 40
Negative experiences after work, on the other hand, can disrupt the recovery process. As predicted (H4b), ruminating about work during time off was associated with less pronounced subjective recovery. Rumination can inhibit successful emotion regulation and detachment from work and thus prolong negative affective states and impede the process of recovery.20,21 As a potential consequence, long-term negative effects of rumination on medical professionals’ health have also been discussed. 41 When rumination was considered in the same model, the association between neuroticism and affective well-being was reduced (H5a). The results thus support the notion that rumination may be one of the mechanisms through which higher neuroticism is associated with worse affective outcomes in the work context.
Unexpectedly, optimism was not associated with affective well-being or recovery – that is, more optimistic people did not seem to feel better after their shifts or detach from their work more easily. However, more situation-specific measures of self-efficacy revealed higher levels of affective well-being (H5b). In contrast to previous findings, 30 our results did not indicate that self-efficacy believes facilitate recovery. This discrepancy may be due to the operationalization of the self-efficacy measure: While our study focused on general trait self-efficacy, previous studies 30 explicitly measured self-efficacy for coping.
The exploratory analyses showed that the association between engaging in physical activity and subsequent recovery was moderated by personality characteristics and age. Specifically, physical activity was more beneficial for people with low and medium levels of optimism, medium and high levels of self-efficacy, or for people in their mid-twenties and older. Research on well-being has called for further investigations into how physical activity and optimism may jointly impact well-being to better understand unique and interactive mechanisms, such as potential buffering effects of PA for people low in optimism. This kind of inquiry may help in interpreting the current findings as well. 42 Regarding self-efficacy, other research has found that self-efficacy partially mediated associations of physical fitness with resilience. Thus, self-efficacy and resilience may be part of the mechanisms linking physical activity with recovery, which could be interesting to address in future research. 43 Taken together, these findings suggest that some people benefit more than others from physical activity, and potential reasons such as engaging in different types or intensities of physical activity need to be addressed in future studies. We emphasize that the current findings should be considered as exploratory and need to be confirmed in future research before discussing them further. If these findings are indeed confirmed, they could provide interesting opportunities for targeted interventions, for example, informing medical staff about personality differences in health benefits of physical activity and inviting certain groups more frequently.
Strengths and limitations
This study gives unique insights into medical professionals’ daily affective stress and recovery processes and thus provides rare data on the work-related experiences of an especially burdened population. While this was especially true during the pandemic, 2 we believe the results to be relevant more broadly and apply to medical professionals beyond the pandemic as well. Still, the burden of this sample of very occupied medical professionals also impeded participant recruitment. As a result, the sample did not reach the pre-specified sample size of n = 200, although the assessments were kept very short. Accordingly, the sample might not cover medical staff in its full breadth as nurses and medical assistants were somewhat less represented, while paramedics and physicians participated more frequently. Still, highly burdened medical staff might not even have participated because participation was voluntary. In addition, the achieved statistical power was somewhat reduced and the sample size might not have been sufficient to calculate random slopes as most models including random slopes did not converge. The reduced statistical power mainly affected within-person associations (i.e. associations hypothesized in H1 to H4b), with the current sample size still allowing to detect moderate within-person associations in 77% of models, and large within-person associations in 96% of models. The achieved sample size hardly affected moderate Level 2 effects (i.e. associations hypothesized in H5a & H5b) and cross-level interactions (i.e. beneficial effects of different leisure activities), which could be detected in 91% and 96% of models, respectively. Future research may profit from explicitly considering heterogeneity in associations between different people, for example to identify opportunities for personalized interventions.
Because of the study set-up of assessments before and after shifts and the resulting data structure, we could not apply the standard operationalization of reactivity as the increase of negative affect following stressor exposure compared to assessments without stressor exposure because there was no non-stressor baseline. Instead, we analyzed the affective well-being immediately after a shift as an indicator of stress reactivity. As a result, we cannot draw conclusions regarding short-term changes in affective experiences as it is usually done in daily life studies on stress. 10 A higher temporal resolution with more densely repeated measures of affect could allow for more nuanced insights into both the reactivity and recovery trajectories. Despite this being difficult in the context of medical professionals’ daily work lives, it would be relevant to better understand short-term stress processes within shifts and during time off work in this work domain as well. We mainly used validated measures and adapted existing measures for assessing activities and emotion regulation after work. Only for assessing anticipated stress, we developed the single item ourselves. The observed associations with experienced stress and reduced affective well-being after the shift suggest sufficient validity, yet further systematic validation in diverse settings would be desirable. Future work might furthermore consider adding passive sensing components to complement the burdensome collection of repeated self-reports. For example, measures of heart rate variability 44 or sleep actigraphy 45 may offer additional insights into stress reactivity and recovery processes.
Conclusion
Anticipated stress, stress during work shifts, and recovery processes are associated substantially with medical professionals’ affective well-being during a large-scale medical crisis, yet likely also during normal work shifts, which are often highly demanding. In addition to ensuring a manageable workload, the results from this study emphasize the importance of non-work activities to promote recovery, especially because insufficient recovery and lower affective well-being after a shift may form a vicious cycle. Interventions aiming to ameliorate stress in medical professionals could focus on improving recovery, for example through the promotion of non-work activities or by strengthening emotion regulation abilities.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261428548 – Supplemental material for Examining the daily life dynamics of anticipation and recovery from work-related stress in frontline medical professionals during pandemic work demands
Supplemental material, sj-docx-1-phj-10.1177_22799036261428548 for Examining the daily life dynamics of anticipation and recovery from work-related stress in frontline medical professionals during pandemic work demands by Anna J. Lücke, Yannick Hill, Anke S. Baetzner, Stefan Mohr, Mascha O. Fiedler-Kalenka, Uta Merle, Erik Popp, Marie O. Frenkel and Cornelia Wrzus in Journal of Public Health Research
Footnotes
Ethical considerations
Ethical approval from the last author’s institution IRB was granted, # AZ Fre 2022 1/1.
Author contributions
A. J. Lücke: Conceptualization, Formal Analysis, Visualization, Writing – original draft, Writing – review and editing; Y. Hill: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review and editing; A.S. Baetzner: Conceptualization, Investigation, Data curation, Writing – review and editing; S. Mohr: Conceptualization, Investigation, Writing – review and editing; M.O. Fiedler: Writing – review and editing; U. Merle: Writing – review and editing; E. Popp: Writing – review and editing; M.O. Frenkel: Conceptualization, Investigation, Project Administration, Funding Acquisition, Writing – review and editing; C. Wrzus: Conceptualization, Project Administration, Funding Acquisition, Writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study and manuscript was prepared with funding from the European Union’s Horizon 2020 project: Medical First Responder Training using a Mixed Reality Approach featuring haptic feedback for enhanced realism (MED1stMR). For the publication fee, we acknowledge the financial support by Heidelberg University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.