
Abstract
Background:
Human Development Index (HDI) as a composite measure to assess well-being across districts, incorporating life expectancy, education, and living standards. In Indonesia, district-level HDI disparities may influence maternal health outcomes and the success of public health initiatives. The Triple Elimination Program, which targets the prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B, shows uneven coverage. This study aims to evaluate the association between the HDI of each district in East Java and the implementation of the Triple Elimination Program.
Design and Methods:
A cross-sectional study analyzed January–December 2023 secondary data from all 38 East Java Province districts. HIV, syphilis, and hepatitis B screening was provided by the Provincial Health Information System and Statistics Indonesia HDI. Spearman’s rank correlation analyzed relationships. STROBE was followed for reporting.
Result:
HIV, syphilis, and hepatitis B case reporting in East Java varied by District Human Development Index. Syphilis screening rates for pregnant women range from 10.9% to 148.4% (Mean: 78.5%; ρ: 0.80). Pregnant women’s HIV screening rates range from 9.2% to 118.3% (mean: 79.6; ρ: 0.742) and Hepatitis B screening rates range from 59.8% to 118.5% (mean: 80.2; ρ: 0.902).
Conclusion:
There was no significant association between district-level HDI and Triple Elimination Program implementation, suggesting that screening performance may be influenced more by health system factors than socioeconomic conditions. A key limitation is the reliance on projected pregnant-women estimates, indicating the need for improved data accuracy and stronger local reporting systems to enhance program coverage.
Introduction
Global efforts to combat vertical transmission of Human Immunodeficiency Virus (HIV), Syphilis, and Hepatitis B in pregnancy have been made, but it continues to be a significant threat, especially in Indonesia, where testing rates remain below target.1,2 In response, the Indonesian Ministry of Health has committed to improving maternal and child healthcare to prevent vertical transmission of diseases such as HIV, Hepatitis B, and Syphilis, as part of the “Triple Elimination Program.” The Indonesian Ministry of Health Regulation provides the legal framework for the Triple Elimination Program. 3 The success of this program in each district depends on the collaboration of key stakeholders, including decision-makers, district health officers, healthcare providers, and the general community.
The United Nations Development Programme (UNDP) created the Human Development Index (HDI) as a composite measure to assess well-being across districts, incorporating life expectancy, education, and living standards. It serves as a key indicator of human capital, reflecting the capacity of populations to achieve a decent standard of living and contribute to societal development. HDI helps policymakers identify areas in need of improvement, design targeted interventions, and track progress toward development goals, ultimately guiding resources and public policies to enhance quality of life. 4
In 2022, Indonesia’s national HDI was 72.91, while East Java, one of the most populous provinces, had an HDI of 72.75. 5 There is a marked variation in HDI across districts, which may have an effect on the level of public health, including the triple elimination program. This phenomenon can be attributed to factors such as decentralized government policies, district prioritization using targeted maternal health interventions, especially in underserved districts, as seen in other LMICs. 6
Decentralization has a positive impact on maternal health services, although the impact is not equally strong across governance models. 7 There is a division of authority between the central and local governments. Some of the central government’s authority includes providing national guidelines and logistics. Additionally, international donors and multilateral agencies, such as UNICEF and WHO, contribute significantly to these programs through technical support and funding, particularly in the context of strengthening maternal health services, particularly in low-income and middle-income countries. 8
Examining the association between HDI and the implementation of the Triple Elimination Program is important because HDI reflects a district’s development and well-being. Improvements in HDI are generally linked to better access to healthcare services. However, HDI does not always predict program performance because implementation is also shaped by health system governance, logistical readiness, and local-level management capacity. Districts with similar HDI levels may therefore show different outcomes depending on how effectively they mobilize resources, organize service delivery, and sustain stakeholder collaboration. This study aims to evaluate the association between the HDI of each district in East Java and the implementation of the Triple Elimination Program.
Method
Data collection
This study employed a cross-sectional design using secondary data from January–December 2023, covering all 38 districts of East Java Province, Indonesia. Data on screening coverage were obtained from the Maternal and Child Health Program section of the East Java Provincial Health Office’s routine health information system and were verified by the Provincial Health Office to minimize reporting errors. The denominator, representing the total number of pregnant women, was derived from government estimates prepared by the Ministry of Health through the Center for Data and Information (PUSDATIN). These estimates were not based on direct census data but on demographic projections of women of reproductive age and pregnancies, as published by Statistics Indonesia (BPS) in the Population Projection of Indonesia 2020–2050 based on the 2020 Population Census. Complementary data on the Human Development Index (HDI) were also obtained from BPS. Ethical clearance for this study was obtained from the Ethical Board of the Faculty of Dental Medicine, Universitas Airlangga (Approval No. 0342/HRECC.FODM/IV/2024).
Inclusion criteria
This study included districts that had implemented the Triple Elimination Program in East Java Province and possessed complete HDI data for 2023, resulting in a population-level analysis without the need for sample size calculation.
Exclusion criteria
Districts with incomplete data of the Triple Elimination Program or HDI variables were excluded from the analysis to ensure validity and reliability.
Research variable
Dependent variable
The dependent variable was the implementation coverage of the Triple Elimination Program, defined as the proportion data of pregnant women screened for HIV, syphilis, and hepatitis B relative to the total number attending antenatal care in each district.
Independent variable
The independent variable was the district-level HDI. HDI values were analyzed both as continuous variables and as categorical variables classified into four levels—low (<0.550), medium (0.550–0.699), high (0.700–0.799), and very high (≥0.800)—following UNDP standards to improve interpretability for policymakers. 9
Statistical analysis
Spearman’s rank correlation test was used to assess the association between district HDI (both continuous and categorical) and screening coverage for HIV, syphilis, and hepatitis B. HDI categories followed UNDP standards to enhance comparability with national and international reports. Screening coverage data were extracted from routinely reported health information verified by the Provincial Health Office, and HDI data were obtained from official BPS publications for 2023. Correlation was selected instead of regression because available district-level data included only screening coverage outcomes and HDI without additional covariates required for multivariable modeling, and the non-normal distribution of variables made non-parametric correlation more appropriate. Potential sources of bias were minimized by using standardized government data sources, applying uniform inclusion and exclusion criteria, and conducting complete case analysis to avoid missing-data bias. Confounding factors such as geographic accessibility, availability of healthcare workforce, and nationally standardized health policies were acknowledged but not quantitatively adjusted due to data limitations. The reporting of this study conforms to the STROBE statement (Strengthening the Reporting of Observational Studies in Epidemiology).
Results
East Java Province spans an area of 48,036.84 km2, divided into two main districts: the East Java mainland and the Madura Islands. The mainland constitutes 88.70% or 42,541 km2, while the Madura Islands account for 11.30% or 5422 km2. In 2022, the province’s population was recorded at 41.15 million. Administratively, East Java comprises 38 regencies/municipalities, including 29 districts and 9 cities; 34 regencies/municipalities are located on Java Island, while 4 are situated on Madura Island 10 (Figure 1).

Distribution of HDI in East Java provinces Indonesia created by the author using QGIS 3.34 with spatial data from Indonesian Central Statistics Agency 2023.
Despite its considerable economic resource potential, the Human Development Index (HDI) of East Java Province in 2023 stood at 73.38, the last rank among the provinces on Java Island. 5 The Human Development Index (HDI) serves as a multidimensional indicator that encapsulates three fundamental dimensions of human welfare: income, health, and education. By assessing these key elements, the HDI provides insights into how effectively a population can leverage its available opportunities and resources to improve overall well-being. 11
Table 1 shows the achievements of the Triple Elimination Program in East Java Province by 2023, associated with the Human Development Index (HDI). The results reported disparities between districts or municipalities. The average HDI across districts was 74.6 (SD = 4.8), placing most districts in the high to very high category. Screening coverage among pregnant women showed mixed achievements: hepatitis B screening had the highest average coverage (84.2%), followed by syphilis (80.4%) and HIV (79.4%). However, standard deviations—particularly for syphilis (23.2%) and HIV (20.5%)—indicate significant variation between districts, with some districts reporting coverage as low as 9.3% for HIV and 10.9% for syphilis. In several districts, reported screening coverage exceeded 100%, with syphilis reaching 148.4%, HIV 132.9%, and hepatitis B 136.0%. This over coverage likely reflects a mismatch between the estimated number of pregnant women—used as the denominator—and the actual number accessing antenatal care, since government projections may not capture real-time population changes.
The distribution of HDI category and coverage of triple elimination program across districts in East Java, Indonesia.

The minimum and maximum values in Table 1 represent the lowest and highest screening coverage actually reported by districts in the 2023 routine health information system. These values reflect real program performance rather than predefined thresholds, with low coverage indicating operational barriers in certain districts. The exceptionally high values observed in some areas (>100%) result from discrepancies between projected and actual numbers of pregnant women, as the denominator relies on population estimates rather than real-time counts.
Figure 2 presents the distribution of key variables related to the implementation of the Triple Elimination Program and the Human Development Index (HDI) across 38 districts and cities in East Java Province. The histogram of the total number of pregnant women indicates a right-skewed distribution, with the majority of districts recording fewer than 20,000 pregnancies per year, while a small number of districts contribute disproportionately higher figures. This reflects demographic variation across the province. A similar pattern is observed in the histograms for the number of women tested for hepatitis B, HIV, and syphilis, suggesting that testing volumes are closely tied to population size and potentially to healthcare service availability.
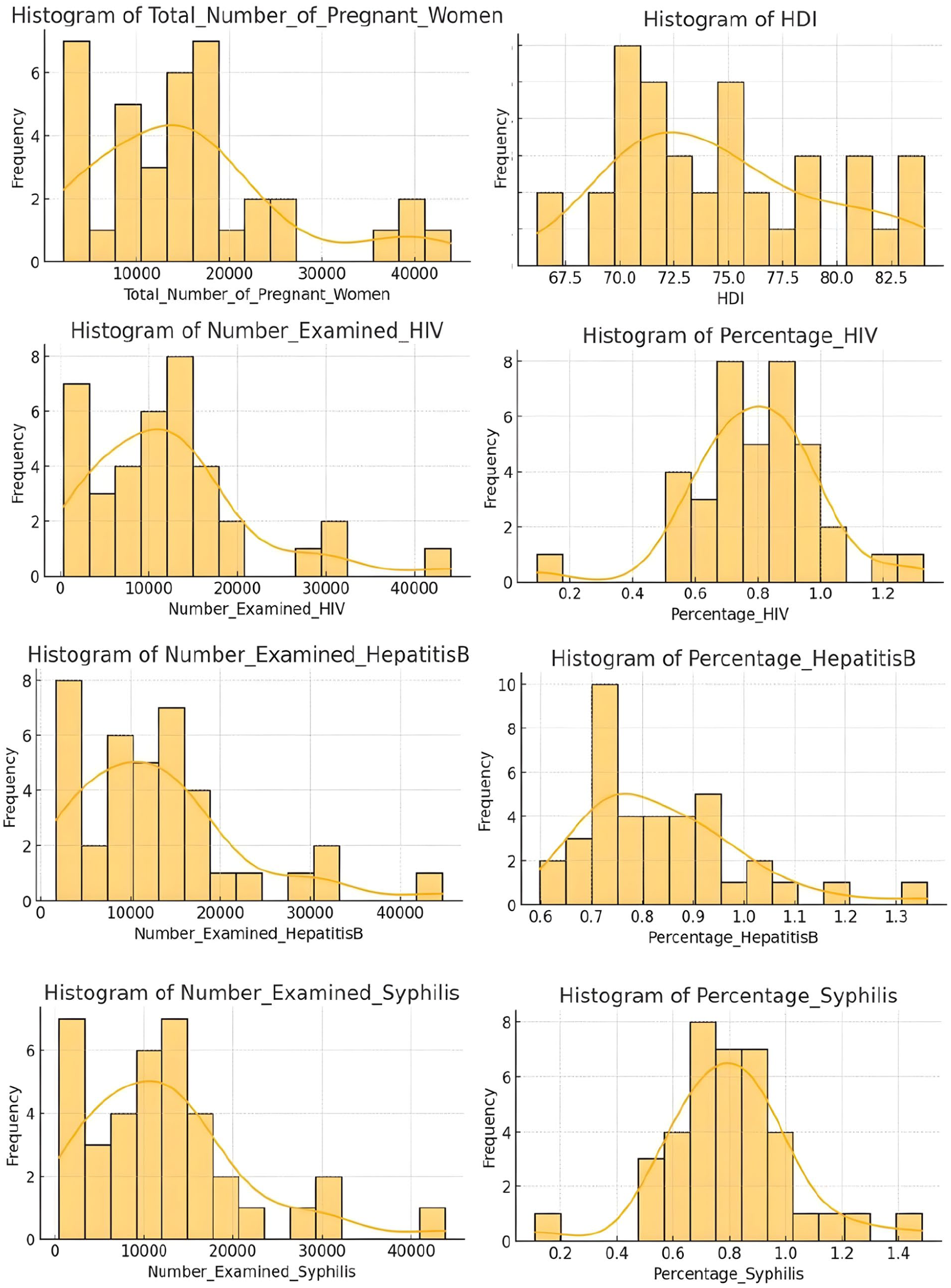
Distribution of variable related to the triple elimination program and human development index across districts in East Java, Indonesia, 2023.
In contrast, the percentage-based indicators reveal more centralized distributions. The percentage of pregnant women tested for hepatitis B and syphilis demonstrates mild skewness toward higher coverage rates, with most districts achieving screening levels above 70%. The HIV screening percentage displays a near-normal distribution, with coverage clustering around 80%, indicating more uniform program implementation across districts. Notably, the distribution of syphilis screening percentage is broader, with some districts falling below 50%, which may reflect programmatic or systemic gaps in service delivery.
The histogram of HDI values shows a mildly right-skewed distribution, with most districts concentrated in the “High” category (HDI between 70.00 and 79.99). Fewer districts approach the “Very High” threshold (HDI ≥ 80.00), and only a limited number fall below 70.00. These distributional patterns emphasize inter-district disparities in both human development and maternal health service coverage, highlighting the need for targeted interventions to enhance program reach and effectiveness in lower-performing areas (Figure 3).

Heat map visualization of district-level distribution of antenatal screening coverage for Hepatitis B, HIV, and syphilis from maternal and child health program section of the East Java provincial health office’s in East Java Province, Indonesia, 2023.
A heat map visualization of antenatal screening coverage for Hepatitis B, HIV, and syphilis across districts in East Java Province by 2023 shows generally good program performance, with most districts achieving coverage levels equal to or above the national target of 95%. High-performing cities such as Surabaya and Malang consistently report near-universal screening for all three infections. However, significant heterogeneity exists across the province. While many districts reported coverage above 80%, some districts exceeded 100%, likely due to pregnant women from outside the district being screened at better-equipped health facilities. In contrast, large disparities were observed in poorly performing districts, particularly Probolinggo City, where screening rates were below 20% for all test types, and one district had HIV screening coverage of only 9%. These data indicate a potential problem with a variety of contributing factors in each district.
Table 2 presents the correlation between district-level Human Development Index (HDI) and screening coverage for syphilis, HIV, and hepatitis B among pregnant women in East Java. Across all 38 districts, no statistically significant associations were observed. Syphilis screening demonstrated a very weak negative correlation with HDI (ρ = –0.040, p = 0.810), while HIV screening showed a similarly weak negative correlation (ρ = –0.055, p = 0.742). Hepatitis B screening exhibited a slight positive correlation (ρ = 0.021), although the association remained non-significant (p = 0.902).
The result of correlation analysis between HDI category and triple elimination program coverage across districts in East Java, Indonesia.

The Spearman coefficients, all close to zero, indicate the absence of a meaningful monotonic relationship between HDI and screening performance. A ρ value near zero reflects no association, whereas negative or positive values indicate inverse or direct trends, respectively. In this study, the extremely small ρ values demonstrate that neither the direction nor the strength of correlation suggests any substantive relationship. These findings imply that differences in district HDI levels do not correspond to variations in antenatal screening coverage for HIV, syphilis, or hepatitis B in East Java.
Discussion
The implementation of the Triple Elimination Antenatal Care Program in Indonesia, aimed at preventing vertical transmission of HIV, syphilis, and hepatitis B among pregnant women to their children, continues to face critical challenges. Despite a national policy mandating routine antenatal screening, our study revealed no statistically significant association between district-level Human Development Index (HDI) and screening rates. This finding contradicts common assumptions that districts with higher HDI would exhibit better health service coverage. 2
Several factors may explain this result. First, the strong central mandate and national-scale policies may have equalized screening efforts across districts, overriding local variations in development. The Ministry of Health’s directive on obligatory screening, supported by centrally distributed laboratory reagents and a basic monitoring framework, may have enabled lower-HDI districts to catch up with their higher-HDI counterparts in screening coverage. 2 Second, HDI is a broad socio-economic indicator and may not adequately reflect health system readiness, leadership quality, or frontline implementation capacity, factors that directly influence service delivery. Districts with similar HDI scores may still differ substantially in health governance, logistic chain efficiency, and staff training levels. Finally, donor or NGO involvement in specific districts could have enhanced screening implementation independently of HDI.
Although socioeconomic development is expected to improve health outcomes, our findings suggest that HDI has only a weak influence on Triple Elimination screening coverage because program performance depends more on system readiness than on development status. The availability of trained health workers, continuous logistics, and strong local monitoring often plays a more decisive role than socioeconomic conditions alone.
Health decentralization in Indonesia is governed by several key regulations. These frameworks delegate substantial authority over health services, including maternal and child health, to provincial and district governments. In the context of the triple elimination program, which targets the prevention of vertical transmission of HIV, syphilis, and hepatitis B, the program itself is centrally designed. The central government is responsible for setting national standards, developing standard operating procedures, and supplying essential logistics such as test kits and treatments.
However, the implementation of the program is decentralized and largely reliant on district-level health authorities. This means that while the policy direction and core resources are standardized nationally, the success of the program depends heavily on the capacity, commitment, and coordination within each district. Decentralization can facilitate partnerships with NGOs and development agencies, allowing for greater flexibility, local adaptation, and resource mobilization. 7 Nonetheless, the variability in local governance and health system capacity contributes to disparities in program outcomes across districts, which may help explain the uneven distribution of progress in maternal and child health indicators, including those reflected in the Human Development Index (HDI). Districts with stronger leadership, better health infrastructure, and more effective local coordination are more likely to achieve the intended outcomes of the triple elimination program.
Beyond system-level determinants, demographic and contextual characteristics may also affect screening coverage. Population mobility, urban–rural composition, cultural norms surrounding antenatal care, and perceived stigma toward sexually transmitted infections can shape maternal health-seeking behavior and influence screening uptake independently of health system readiness. Future studies incorporating these contextual dimensions would be valuable to clarify how community-level characteristics interact with program implementation.
These findings align with previous studies from other low- and middle-income countries (LMICs), where program success is often separated from development indicators. For instance, in India and the Philippines, variations in antenatal screening coverage were attributed to differences in local health system performance and program prioritization rather than districtal wealth or education levels. Similarly, Brazil has seen rising congenital syphilis rates despite improved antiretroviral coverage, highlighting the limitations of fragmented monitoring systems. In sub-Saharan Africa, decentralized governance, resource constraints, and poor inter-sectoral coordination have further impeded consistent implementation of maternal screening programs, regardless of national development status. 12
While Indonesia has made commendable efforts to standarize triple elimination screening, several gaps persist. The national target for the Triple Elimination program mandates that 90% of pregnant women be screened for HIV, syphilis, and hepatitis B. However, national coverage in the first quarter of 2023 reached only 16.1% for HIV, 13% for syphilis, and 24.87% for hepatitis B. 13 Based on the data collected from the local health office, the screening coverage among pregnant women in the district shows relatively high percentages. Specifically, 80.4% of pregnant women were screened for syphilis, 79.4% for HIV, and 84.2% for hepatitis B. These figures indicate significant progress toward achieving the national target of the Triple Elimination program. However, despite these encouraging numbers, nearly half of the cities and regencies in East Java Province still report screening coverage rates below the provincial average. This highlights the need for strengthening local health systems to ensure more equitable and consistent implementation across all districts.
To address these challenges and strengthen implementation, several targeted strategies should be considered. One key approach is to develop and enforce real-time, district-level digital monitoring systems that are fully integrated into existing health information systems. Performance-based incentives should be allocated to health districts based on their ability to meet coverage targets and ensure treatment completion. Standardizing training modules for health workers, particularly those operating in rural and under-resourced areas, is also essential to improve service quality. Additionally, ensuring the regular distribution of test kits and reagents through strengthened supply chain mechanisms will help maintain service availability. Finally, effective multisectoral coordination between central and district health offices is needed to align priorities and funding, thereby enhancing the overall effectiveness of the program.
Limitations of this study include the reliance on secondary data, which may introduce inaccuracies or reporting bias, particularly because the quality of surveillance and reporting varies across districts. However, all districts reported complete data for the variables included in this analysis, so no observations were excluded and the results were not affected by missing-data bias. Additionally, the denominator used to calculate screening coverage was based on projected estimates of pregnant women rather than real-time counts, which may lead to over- or underestimation of coverage in some districts. HDI may also not fully capture operational aspects of healthcare delivery. Other contextual variables, such as district leadership quality, NGO presence, and community health engagement, were not examined but may influence program performance. As this study analyzed all districts in East Java using routinely collected health data, the findings are likely generalizable to other Indonesian provinces with similar health system structures, though caution is advised when extrapolating to regions with very different contexts.
Future research should explore the implementation dynamics of the triple elimination program through qualitative studies involving healthcare providers and district health authorities to better understand local barriers and facilitators. Examining health workers’ perspectives on service quality and program delivery may offer valuable insights to improve coverage and ensure equitable, patient-centered care. In parallel, longitudinal studies are needed to assess the impact of new policy interventions on screening coverage, treatment rates, and perinatal outcomes related to the Triple Elimination program. Quantitative analyses linking antenatal screening uptake to neonatal health indicators would provide critical evidence of program effectiveness. Additionally, expanding future analyses to include facility readiness, health worker density, and budgetary allocations could offer a more comprehensive understanding of the structural factors influencing the success of the Triple Elimination program.
Conclusion
There is no significant association between district-level HDI and the implementation of the Triple Elimination Program in East Java Province, Indonesia. While national policies have supported overall screening progress, gaps remain across districts, highlighting the influence of local health system capacity, governance, and resource allocation. Strengthening data accuracy through routine updates of target population figures using real-time maternal service records and validating them with district demographic reports, along with enhancing local facilities’ capacity for monitoring and reporting program indicators, can directly improve service coverage and reduce disparities in implementation.
Footnotes
Acknowledgements
The researchers acknowledge to staff of the Department of Health in East Java Province, Surabaya and Sampang Health Officer, who gave support during the research.
Ethical considerations
Ethical Board of the Faculty of Dental Medicine Universitas Airlangga with the number 0342/HRECC.FODM/IV/2024.
Author contributions
Budi Prasetyo: Conceptualization, Supervision, Project administration, Writing – Review & Editing.
Alifina Izza: Methodology, Formal analysis, Writing – Review & Editing.
Zalfa Dinah Khairunnisa: Formal Analysis, Visualization, Interpretation of Results.
M. Masrur Rizal: Formal Analysis, Visualization, Interpretation of Results.
Fabella Elisa Cahyaningtyas: Data Curation, Writing – Original Draft, Validation.
Fayka Putri Poempida: Methodology, Resources.
Dewi Setyowati: Formal Analysis, Data Visualization.
Agnestia Naning Dian Lovita: Writing – Original Draft.
Farah Sajidah: Data Curation, Validation, Investigation.
Bersellynica Azarine Azzahra: Data Curation, Validation, Investigation.
Intan Fairuz Zakia: Data Curation, Investigation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Universitas Airlangga with the grant number: 4483/B/UN3.FK/PT.01.03/2024.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this study were obtained from the East Java Provincial Health Office and are not publicly available due to institutional data-sharing policies. However, the data are available from the corresponding author upon reasonable request and with permission from the East Java Province Health Office.