
Abstract
Objective:
This study aimed to cross-culturally adapt and validate the Self-Regulation Questionnaire for Dental Home Care (SRQDHC) for use among Vietnamese children and to examine the relationship between motivation for oral hygiene and dental caries status.
Methods:
The SRQDHC was translated and culturally adapted for Vietnamese children aged 9–10 years using cross-sectional study. A total of 200 students were randomly selected from a primary school in Hanoi. Clinical dental examinations were conducted to assess caries experience using the dmft and DMFT indices. Subsequently, participants completed the Vietnamese version of the SRQDHC to evaluate their oral hygiene motivation. Internal consistency and factor loadings were analyzed to assess the questionnaire’s reliability.
Results:
Dental caries was observed in 84.5% of participants. The mean dmft and DMFT scores were 3.20 ± 3.18 and 2.15 ± 2.37, respectively. The SRQDHC demonstrated acceptable internal consistency (Cronbach’s alpha = 0.7021) and strong factor loadings (>0.3). A statistically significant correlation was found between motivation scores and caries status.
Conclusion:
The Vietnamese version of the SRQDHC is a reliable tool for assessing dental home care motivation in children. Given the high prevalence of caries in this population, motivation-based oral health interventions are warranted. Further refinement of selected questionnaire items is recommended to enhance its utility in clinical and research settings.
Introduction
Routine oral hygiene education has long been a widely implemented strategy by dental professionals and students to enhance patients’ knowledge and technical proficiency in maintaining oral health at home. However, despite these preventive efforts, the global and national burden of dental diseases remains significant. The 2022 Global Oral Health Survey by the World Health Organization (WHO) reported that oral diseases affect over 3.5 billion people worldwide, marking an increase of more than 1 billion since 1999. 1 In Vietnam, the 2019 National Oral Health Survey found that 86.4% of children aged 6–8 suffer from tooth decay. 2 These findings suggest that existing preventive measures, including routine oral hygiene education, have not been sufficiently effective in reducing the prevalence of oral diseases at a population level, highlighting the need for more comprehensive and impactful intervention strategies.
Dental education alone has limited impact when learners’ awareness and attitudes are not aligned. For instance, Soldo et al. study on a group of 14- and 15-year-old children in Croatia showed that the plaque index of the group receiving oral hygiene instruction increased again after 3 months, even though their brushing skills generally did not diminish. 3 This gap between skills and sustained behavior has shifted research attention toward understanding and strengthening motivation. Human behavior is inherently driven by a set of motivations, making it crucial to build and reinforce these factors to increase compliance with dental treatment and oral hygiene practices at home. 4 Over the past three decades, growing recognition of the role of behavioral motivation in health has led to the application of Self-Determination Theory (SDT) in dentistry. This psychological framework has been increasingly utilized to investigate patients’ motivation for maintaining oral health.
According to SDT, motivation is categorized into two main types: intrinsic and extrinsic. Intrinsic motivation arises when an individual engages in a behavior for inherent satisfaction, whereas extrinsic motivation is driven by external outcomes. Due to the repetitive and habitual nature of oral health behaviors such as brushing, individuals often exhibit extrinsic motivation toward these activities. However, extrinsic motivation exists along a continuum of internalization, ranging from external and introjected regulation to more autonomous forms—identified and integrated regulation. As motivation becomes more internalized, individuals experience greater autonomy, with identified and integrated regulation representing autonomous motivation, where behaviors are performed willingly and with personal endorsement. 5
Studies have consistently shown a positive correlation between autonomous motivation and adherence to health-related behaviors.6–8 For instance, a randomized controlled clinical trial by Aleksejūniene et al. demonstrated that interventions enhancing patients’ autonomous motivation led to improve plaque index outcomes. 8 Based on these findings, Halvari et al. developed a method to assess the motivation for dental health care behavior at home using the “Self-Regulation Questionnaire for Dental Home Care” (SRQDHC), under the guidance of Edward L. Deci, the author of SDT. 9 Additionally, Halvari et al. introduced targeted strategies to enhance autonomous motivation, significantly improving patient adherence to oral hygiene behavior.6,10
Despite these advancements, research on motivation in dental home care remains limited in Vietnam. Furthermore, elementary school students—key targets of dental education programs—are at a critical stage for developing oral hygiene habits. Therefore, this study aims to adapt and validate the SRQDHC for Vietnamese children aged 9–10 in Hanoi and investigate the correlation between motivation and oral health care behavior in this population.
Materials and methods
This study was approved by the Hanoi Medical University Institutional Ethical Review Board (Ref. No. HMUIRB1596). Prior to conducting the study, the primary school board approved and granted permission to conduct the study. Additionally, all children assented to participate, and informed consent was obtained from their parents.
Study design and participants
This descriptive cross-sectional study was conducted between October 2023 and July 2024 among fourth-grade students (aged 9–10 years) at Kim Lien Primary School, Hanoi (see Supplementary material).
Eligibility criteria included the provision of written informed consent by a parent or legal guardian, as well as the child’s good general health and willingness to cooperate during the clinical examination. Exclusion criteria included not meeting the inclusion criteria, lacked parental/legal guardian consent, requiring care or support for psychiatric disorders, and being absent from school or missing responses during the data collection period.
Sampling technique
The required sample size was calculated using the following formula:

Where:
n: Required sample size.
α: Statistical significance level, in this study α = 0.05
p: The estimated prevalence of the condition of interest; here, p = 0.864, based on the prevalence of primary tooth decay among 6–8-year-old children in Vietnam reported by Thị Hồng Minh and Đình Hải. 2
d: Margin of error, set at 0.05 (5%).
Based on the calculation, the minimum required sample size was 178. To improve data robustness and account for potential exclusions, the final sample size was increased to 200 students. A gender-stratified random sampling method was employed, selecting 100 male and 100 female fourth-grade students from Kim Lien Primary School. Analyses were conducted on complete cases. Participants with missing responses for a given variable were excluded from that specific analysis; no imputation was performed.
The recruitment process included distributing information and consent forms to parents, compiling a list of students with confirmed parental consent, and conducting clinical examinations and structured interviews. Students who did not meet the inclusion criteria or were uncooperative were excluded. These steps ensured a valid sampling process and comprehensive data collection on dental health and related factors.
Clinical examination and questionnaire survey
Clinical examination
Six dentists (Vietnamese Ministry of Health–certified) completed training and calibration on using International Caries Detection and Assessment System (ICDAS), including photo-atlas review, image-based practice, and a supervised clinical session assessing 20 non-study children to align diagnostic criteria. 11 The inter-examiner reliability of ICDAS assessments, calculated using Cohen’s kappa on 20 non-study children, was 0.82 (95% CI: 0.75–0.89), reflecting substantial agreement. Intra-examiner reliability, determined through re-examination of 10 children after a 2-week interval, ranged from 0.78 to 0.85 among the examiners, confirming strong intra-examiner reproducibility. 12 Caries prevalence, dmft, and DMFT indices were subsequently calculated from the finalized data.
Questionnaire survey
The original questionnaire was adopted from the “Self-Regulation Questionnaire for Dental Home Care” (SRQDHC) by Halvari et al. 9 It consists of 15 items assessing 5 factors regulating motivation: Integrated regulation, Identified regulation, Introjected regulation, External regulation, and Amotivation. The cross-cultural adaptation process followed established guidelines, including translation, back-translation, and expert revision by a panel of dentists and dental researchers proficient in English. 13
The preliminary Vietnamese version of the SRQDHC was pilot-tested on 20 fourth-grade students from Kim Lien Primary School to assess semantic clarity. Subsequently, 200 fourth-grade students from the same school were randomly selected to participate in the study, ensuring representativeness.
Two trained dentists conducted the survey, providing students with instructions and interviews to facilitate accurate responses. A seven-point Likert scale was employed to comprehensively assess motivation levels. Before data collection, the two examiner-interviewers completed a standardization session to harmonize instructions and administration. Each examiner then practiced with a separate group of 20 non-study children (n = 40 total) and subsequently switched groups to evaluate inter-examiner consistency. To assess intra-examiner reliability, each pilot group was re-interviewed by the same examiner 1 week later. Because the instrument yields continuous subscale/total scores from Likert items, agreement was quantified using a two-way random-effects intraclass correlation coefficient for absolute agreement, single-measure (ICC[2,1]). Intra-examiner ICCs were 0.85 and 0.82 (each n = 20; 95% CI: 0.73–0.89), and the inter-examiner ICC on a common subsample (n = 20) was 0.86 (95% CI: 0.68–0.91), indicating high consistency of administration and scoring.
Statistical analysis
Data were analyzed using STATA software version 14 (Stata Corp. LP, College Station, United States of America). Listwise deletion method was used to handle missing data before analysis. The distribution of quantitative variables was assessed using skewness and kurtosis tests (sktest), which evaluate normality based on skewness and kurtosis and provide an overall test statistic. Descriptive analysis was performed to summarize the study variables.
To assess the reliability of the SRQDHC, internal consistency was measured using Cronbach’s alpha, with a threshold of ≥0.7 considered acceptable. The structural validity of the instrument was examined through exploratory factor analysis (EFA) using principal components analysis. EFA was employed to verify construct validity, ensuring that item distributions aligned with the original questionnaire and assessing the relationships among items. Data analysis indicated that Bartlett’s Test of Sphericity (Chi-Square = 667.13, p < 0.05) and the KMO Measure of Sampling Adequacy (0.74) supported the suitability of conducting factor analysis (EFA), with factors considered significant if their eigenvalues exceeded 1.0.
Subgroup analyses were conducted by sex, comparing mean scores for each motivational factor between boys and girls using independent-sample t tests. The Mann-Whitney U test was used to test the difference in caries prevalence, index (dmft/DMFT), and SRQDHC scores between sexes. Regression models were used to test the association between SRQDHC scores and dmft/DMFT index in the study group. Specifically, a linear regression model will be implemented.
Results
Descriptive results
Demographic characteristics
Initially, all fourth-grade students were invited (364 students). This study consisted of 200 children aged 9–10 years randomly selected from 312 eligible students, of which males and females were equally selected. The average age was 9.3 (see Table 1).
Demographic characteristics of the study group.

Caries prevalence
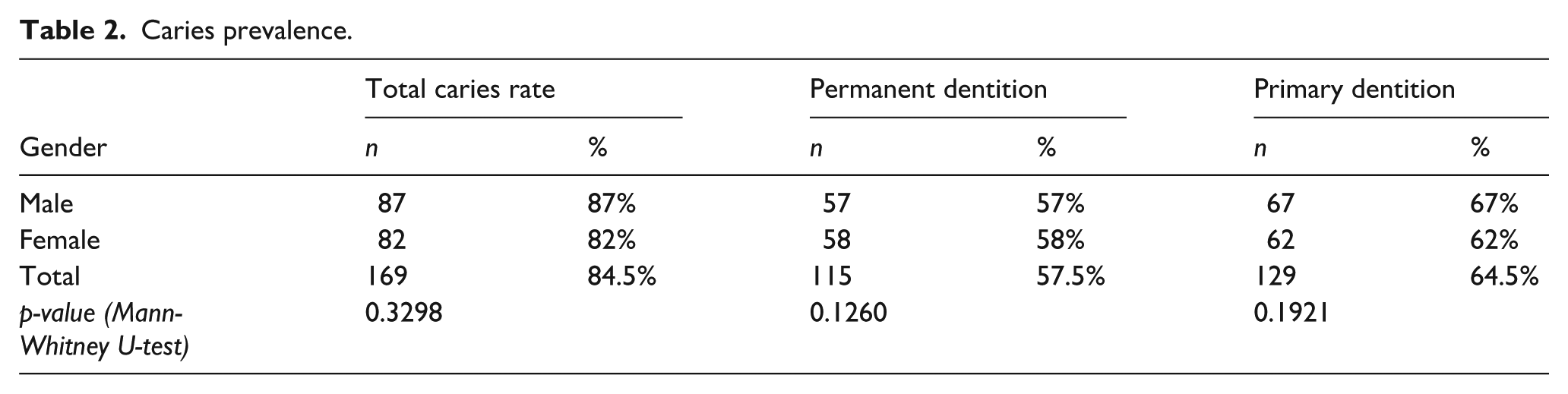
The results revealed a high overall prevalence of dental caries, with rates of 84.5%, 57.5%, and 64.5% for total caries, primary dentition, and permanent dentition, respectively. Notably, primary tooth decay was more prevalent in male students (67%) compared to female students (62%). In contrast, permanent tooth decay was slightly less common in males (57%) than females (58%). However, these differences were not statistically significant (p > 0.05, Mann-Whitney U-test; see Table 2).
Caries prevalence.
Decayed, missing, and filled teeth indices, including DMFT and dmft
The average dmft index of the research group was 3.20, with a noticeable difference between the sexes: 3.63 for males and 2.78 for females. However, this difference was not statistically significant. On the other hand, the average DMFT index for the research group was 2.15, with no significant difference between the two genders (see Table 3).
DMFT and dmft indices.

Questionnaire analysis
Motivational survey results
The results of the motivational survey using the Vietnamese version of the SRQDHC questionnaire are presented in Table 4. Overall, factors associated with higher levels of autonomy (Autonomous Motivation, Integrated, Identified) yielded slightly better results compared to those with lower autonomy (Controlled Motivation, Introjected, External). The average score for Autonomous Motivation was around 34, while the average score for Controlled Motivation was approximately 27.
Average motivation survey results.

p-values obtained from the Mann-Whitney U-test
p-value < 0.1; **p-value < 0.05.
When comparing genders, female students exhibited higher motivation scores than male students across most motivational factors, with the exceptions of External Regulation and Amotivation. Additionally, statistically significant differences were observed between the sexes (p < 0.05) in the factors of Autonomous Motivation and Identified Regulation.
Reliability and construct validity assessment
The Cronbach’s alpha coefficients of the questionnaire’s items can be seen in Table 5. Relatively high levels (>0.7) of internal consistency (Cronbach’s alpha) emerged.
Reliability coefficients.

Exploratory factor analysis (EFA; Table 6) yielded five factors with eigenvalues greater than 1 and loadings above 0.30, capturing the underlying structure of the 15 items. These five factors accounted for 60.31% of the total variance, exceeding the 50% threshold, indicating a strong explanation of the data variation by the extracted factors. The rotation matrix results showed that 15 observed variables were grouped into five factors, with most variables having factor loadings above 0.3. However, two variables, Q2 and Q4, had low factor loading values (below 0.3).
Exploratory factor analysis results.

The factor loadings of the questions on their originally hypothesized factor are indicated in bold.
Correlation between motivation score and caries status
Spearman’s analysis results support the relationship between motivational issues and dental caries status (see Table 7). Specifically, the statistically significant results indicate a negative correlation between motivational factors and dental caries status, as measured by the decayed, missing, and filled tooth (dmft/DMFT) indexes. Conversely, the Amotivation factor shows a positive correlation with these indexes, suggesting that higher levels of amotivation are associated with increased dental caries.
Correlation between motivation score and decayed, missing, and filled teeth index.

Note. ρ: Spearman’s rank correlation coefficient; p-value < 0.05 are indicated in bold.
Linear regression analysis revealed a statistically significant linear correlation between motivational factors and dental caries status (see Table 8). Notably, Integrated Motivation was inversely associated with caries experience (β = −0.29, 95% CI −0.48 to −0.12, p = 0.001), with the model explaining 5.9% of the variance (adjusted R2 = 0.059). The correlation is more modest for the Controlled Motivation factor, with a reduction of 0.077 units per point increase. In contrast, the Amotivation factor shows a positive linear correlation with dental caries, with each point increase in this factor resulting in an increase of 0.179 units in the total caries index (dmft + DMFT).
Linear regression coefficients.
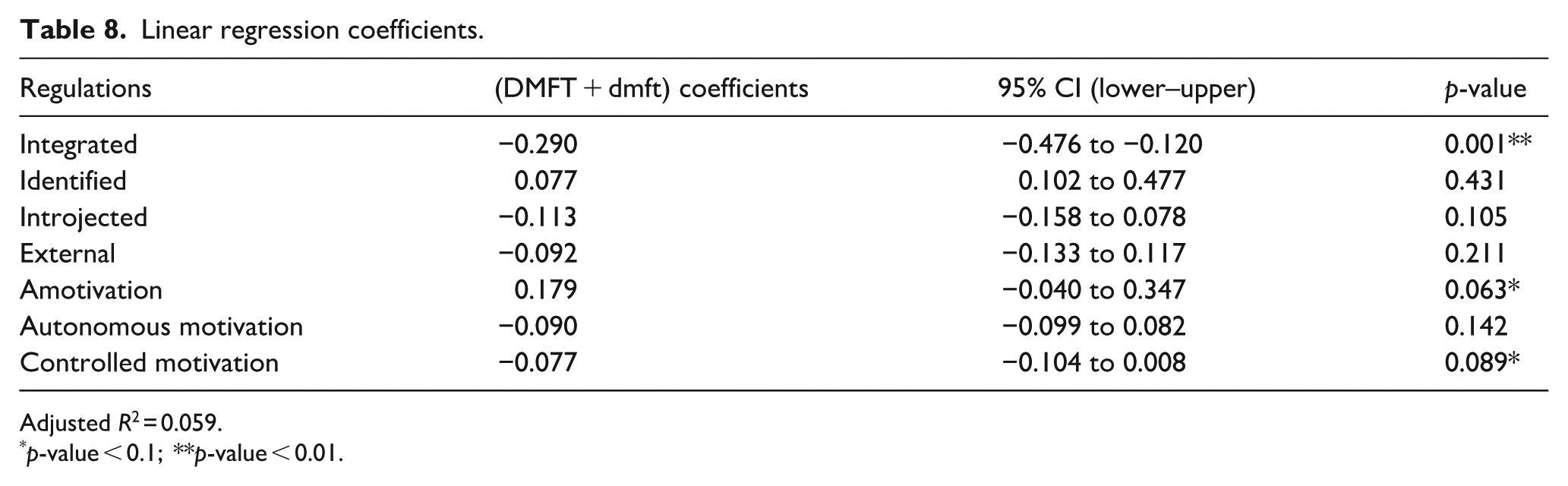
Adjusted R2 = 0.059.
p-value < 0.1; **p-value < 0.01.
Discussion
This study provides a comprehensive overview of the prevalence and severity of dental caries among 9–10-year-old students at Kim Lien Primary School, Hanoi. The results indicate a notably high overall rate of dental caries rate of 84.5%. DMFT and dmft indices for our study group (demonstrated in Table 3) were also relatively high, reflecting the severity of the condition and underscoring oral health as a pressing public health concern in this population. While male students exhibited higher prevalence rates for both overall and primary tooth decay than their female counterparts, the differences were not statistically significant, but they may point to behavioral or biological factors worth exploring further.
When compared to the National Oral Health Survey of Vietnam (2019), our study shows a higher prevalence of dental caries in primary teeth (64.5% vs 52%). 2 Likewise, both DMFT and dmft indices in this study surpassed those reported nationally in 1999 (DMFT: 0.93, dmft: 1.93). 14 These discrepancies may stem from variations in sample characteristics, with our study focusing on an urban Hanoi district, where dietary habits, parental supervision, and access to care may differ from rural or suburban contexts.
Internationally, the caries prevalence in permanent teeth (57.5%) observed in our study is lower than the 91% reported in Laos (Nitthasack et al.), 15 but substantially higher than the 3.5% documented in the United States (Bashir). 16 These disparities highlight the significant role of socioeconomic status, public health infrastructure, and educational outreach in shaping oral health outcomes.
In terms of DMFT/dmft indices, our results are higher than those from Bangkok, Thailand (Luksamijarulkul et al. ; DMFT: 1.37(±1.84) 17 and Saudi Arabia (Aqeeli et al.; DMFT: 1.43, dmft: 2.66), 18 but lower than findings from Thailand (Wittayapipitporn et al.; dmft: 6.11) 19 in and India (Sevekar et al.; dmft: 4.47). 20 These comparisons confirm that dental caries remains a widespread concern in many developing nations and is shaped by a complex set of determinants, including individual behaviors, familial practices, social and environmental conditions, and the accessibility and quality of dental care services.
Through culturally adapted translation, testing, and validation, the Vietnamese SRQDHC (Self-regulation Questionnaire for Dental Home Care) demonstrate strong reliability. In 200 students aged 9–10 years at Kim Lien Primary School revealed a Cronbach’s alpha of 0.7021, indicating strong reliability and internal consistency. According to Nunnally and Bernstein, a Cronbach’s alpha greater than 0.7 indicates high reliability and internal consistency of the questionnaire. 21 Compared to global studies, our result exceeds those of Syrjälä et al. 22 (Cronbach’s alpha of 0.56) and Borkowska et al. 23 (0.59). However, our results are slightly lower than those of Halvari et al. 9 and Rachmawati et al., 24 who reported Cronbach’s alpha values of 0.76–0.86 and 0.929, respectively. Despite this, excessively high internal consistency can reduce the validity of the questionnaire, making it too narrow and less comprehensive. 21 Therefore, Cronbach’s alpha of 0.7021 suggests that the SRQDHC Vietnamese version is reliable for comprehensively assessing dental home care motivation across its many facets.
Exploratory Factor Analysis (EFA) confirms that the questionnaire effectively describes the motivation factors theorized by SDT. However, Questions 2 and 4 exhibited low factor loadings and reduce the overall consistency. Removing these questions improves Cronbach’s alpha, suggesting they may not be well-suited for this age group. A likely explaination is age: our 9–10-year-old participants are still developing their oral hygiene habits and may not view these behaviors as “normal” or “self-directed,” which are reflected in the content of Question 2 and 4. Future research should refine and test these items with similar age groups to better illustrate dental home care motivation. Additionally, the SRQDHC should include questions to assess intrinsic motivation, which, —though less dominant—, could provide a more comprehensive understanding of its role in shaping long-term oral health behaviors. 4
Our study found that female students scored higher than male students on most of the motivational factors surveyed, except for External Regulation and Amotivation. Notably, the differences were statistically significant (p < 0.05) for Identified Regulation and Autonomous Motivation. This aligns with common social perceptions that girls tend to exhibit greater self-discipline and conscientiousness in personal hygiene compared to boys, who are often characterized by higher levels of physical activity and risk-taking behavior. This difference in motivation might explain why boys often show lower compliance with routine health behaviors like home dental care. Supporting this, study by Tetering et al. 25 found that girls in the Netherlands had higher self-regulation scores than boys. Conversely, research by Weisberg et al. 26 in Canada indicated that such gender differences in personality traits tend to diminish by adulthood.
The motivation disparity between genders could contribute to the observed differences in DMFT and dmft indices, as shown in Tables 3 and 4, with girls having higher motivation scores and lower caries indices than boys. This suggests a promising correlation between home dental care motivation (assessed by the Vietnamese version of the SRQDHC, based on SDT) and dental caries status.
The results from Table 7 show statistically significant correlations between motivation for home dental care and the dmft and DMFT indices, suggesting that higher levels of motivation, particularly Integrated Regulation, Autonomous Motivation, and Controlled Motivation, are associated with lower caries indices. In comparison, a lack of motivation (indicated by higher Amotivation scores) is linked to higher caries levels.
Linear regression analysis further substantiated these findings. Specifically, for each unit increase in Integrated Regulation, caries status (as measured by dmft/DMFT indices) decreased by 0.29 units. This strong correlation highlights the potential of motivation, especially Autonomous Motivation, in influencing dental caries outcomes and underscores its importance in promoting effective home dental care behaviors. Although the variance explained was modest (adjusted R2 ≈ 0.06), this is consistent with effect sizes typically observed in behavioral and psychosocial health research, where outcomes such as dental caries are influenced by multiple biological, environmental, and behavioral determinants. The effect sizes and confidence intervals therefore provide more meaningful evidence than model fit alone.
Similarly, Halvari et al. observed a negative correlation between Autonomous Motivation and plaque and gingivitis. 9 Staunton et al. found a positive correlation between Identified Regulation and increased flossing frequency. 27 Aleksejūniene et al. demonstrated that increased Autonomous Motivation led to lower plaque indices in adolescents. 8
Conversely, Rachmawati et al. reported a negative correlation between External Regulation and caries experience. 24 However, many studies have documented that while extrinsic motivational factors, such as parental pressure or criticism from dental professionals, can significantly alter behavior in the short term, they often undermine intrinsic motivation and long-term change. 4 Consequently, fostering Autonomous Motivation while minimizing external influences is crucial for sustainable improvements in oral health outcomes.
The SRQDHC is a practical, psychometrically sound instrument for profiling motivation toward dental home care across the full self-determination spectrum. Beyond measurement, it enables targeted action: because autonomous motivation reliably predicts sustained oral hygiene behaviors, clinicians and program leads should prioritize shifting patients from external and introjected regulation toward identified and integrated regulation. Doing so strengthens agency and makes adherence durable rather than episodic.
To operationalize this, we advance a scalable school–parent–professional pathway: (i) use the SRQDHC to map motivational orientations at baseline; (ii) deliver brief, autonomy-supportive classroom modules and aligned take-home tasks tailored to those profiles; and (iii) monitor progress with implementation-friendly indicators—monthly brushing calendars, SRQDHC subscales, and periodic plaque/caries checks. This framework is intentionally light-touch, low-cost, and implementation-ready, closing the intention–behavior gap with tools that teachers and dental teams can deploy within existing workflows. It also yields clear evaluation endpoints suitable for pragmatic trials and routine quality improvement.
For community programs, the SRQDHC functions as a pre-assessment that converts “one-size-fits-all” education into precision behavior support. Its simplicity makes it viable in underserved or remote settings where chair time and specialist capacity are constrained. By uncovering specific motivational barriers and facilitators, implementers can co-design interventions with families and schools, target resources where they matter most, and track equity-relevant outcomes over time. In short, the SRQDHC is not only a measure—it is a lever for delivery and accountability, offering a credible route from theory to population-level oral health gains.
However, motivation does not always translate into behavior change. Sheeran estimate that only around 47% of individuals who intend to change actually do so. 28 Therefore, targeted strategies are essential for translating motivation into sustained action. For instance, Lally and Gardner propose two fundamental steps in habit formation: (1) translating intention into behavior and (2) promoting continued repetition. 29
Despite its contributions, this study has limitations. The SRQDHC questionnaire, despite rigorous validation, showed suboptimal factor loadings for two items (Q2 and Q4), likely due to age-related cognitive differences. Future studies should refine and test the questionnaire across age groups to improve reliability. Additionally, the exclusion of intrinsic motivation is a limitation, warranting further exploration.
This study was conducted in a single urban Grade-4 cohort (ages 9–10) from one Hanoi school, which limits external validity. Motivational profiles and caries burden may differ in rural settings, other regions, age groups, and schools with different socioeconomic and service contexts. Replication in multi-site, urban–rural cohorts with broader ages—and, ideally, longitudinal designs—is warranted. Several key confounders that could influence the relationship between motivation for dental home care and caries status were not assessed, including socioeconomic status (family income, access to care), dietary habits (especially sugar intake), parental supervision of oral hygiene, and fluoride exposure (water or toothpaste). These omissions may have overestimated the independent effect of motivation. The single-school urban sample also introduces selection bias, further restricting generalizability and potentially underestimating caries prevalence in rural or lower-socioeconomic populations. Additionally, the interviewer-administered questionnaire may have induced moderate social desirability bias, as evidenced by higher autonomous motivation scores among females. A potential limitation arises from conducting the examination during the mixed-dentition period, when distinguishing between physiological shedding of primary teeth and tooth loss attributable to caries proves particularly challenging, thereby affecting the accuracy of dmft/DMFT indices.
To overcome these limitations, future studies should use multivariable regression to adjust for confounders, employ mixed-methods designs (e.g. self-administered surveys combined with objective behavioral measures) to reduce bias, and focus on children with fully erupted permanent dentition. Further research should also develop and evaluate dental education interventions grounded in SRQDHC and SDT.
Conclusion
In conclusion, the Vietnamese-adapted SRQDHC questionnaire shows high reliability and a robust structure, though certain items require refinement. Dental caries remain prevalent and severe among 9–10-year-old students at Kim Lien Primary School in Hanoi, highlighting the need for targeted interventions. Notably, motivation levels, particularly autonomous motivation, show a strong inverse correlation with caries prevalence, emphasizing its role in improving oral health outcomes.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251410261 – Supplemental material for Cross-cultural adaptation of motivational questionnaire for dental home care and its correlation to caries status of students at Kim Lien Primary School, Hanoi
Supplemental material, sj-pdf-1-phj-10.1177_22799036251410261 for Cross-cultural adaptation of motivational questionnaire for dental home care and its correlation to caries status of students at Kim Lien Primary School, Hanoi by Anh Dung Ho, Duc Phu Do, Huu Vi Hoang, Manh Tuan Vu and Duc Long Duong in Journal of Public Health Research
Supplemental Material
sj-pdf-2-phj-10.1177_22799036251410261 – Supplemental material for Cross-cultural adaptation of motivational questionnaire for dental home care and its correlation to caries status of students at Kim Lien Primary School, Hanoi
Supplemental material, sj-pdf-2-phj-10.1177_22799036251410261 for Cross-cultural adaptation of motivational questionnaire for dental home care and its correlation to caries status of students at Kim Lien Primary School, Hanoi by Anh Dung Ho, Duc Phu Do, Huu Vi Hoang, Manh Tuan Vu and Duc Long Duong in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the students who participated in this study, as well as their parents and teachers for their kind cooperation and support. Your willingness to contribute your time and effort made this research possible. We also extend our appreciation to the school administrators for facilitating the clinical examinations and data collection process. Your participation played a vital role in helping us better understand the importance of motivation in children’s oral health care.
Ethical considerations
This study was approved by the Hanoi Medical University Institutional Ethical Review Board (Ref. No. HMUIRB1596).
Consent to Participate
The study was approved by the primary school board. Informed consent was obtained from parents or legal guardians, and assent was obtained from the children themselves following age-appropriate explanations, prior to the start of the study.
Author contributions
Anh Dung Ho, Duc Long Duong; Methodology, Anh Dung Ho, Duc Long Duong: Conceptualization. Anh Dung Ho, Huu Vi Hoang and Duc Phu Do: Software. Anh Dung Ho, Huu Vi Hoang, Duc Phu Do and Manh Tuan Vu: Investigation. Anh Dung Ho and Manh Tuan Vu: Data Curation. Huu Vi Hoang, Duc Phu Do and Manh Tuan Vu: Formal analysis. Anh Dung Ho, Duc Long Duong: Writing – Original Draft. Anh Dung Ho, Duc Long Duong and Manh Tuan Vu: Writing – Reviewing and Editing. Anh Dung Ho: Visualization.Duc Long Duong: Supervision. All authors discussed the results, reviewed, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.