
Abstract
Background:
Anticoagulant therapy is high-risk and requires pharmacists to be highly competent in its management. In Saudi Arabia, the confidence of pharmacists in providing such care is not well-established. This study aimed to assess the self-reported confidence levels of pharmacists in Saudi Arabia regarding the provision of pharmaceutical care for patients on anticoagulants.
Methods:
A cross-sectional online survey was distributed to pharmacists across various healthcare settings in Saudi Arabia. The questionnaire assessed confidence across multiple domains of anticoagulant care, including knowledge, adverse event management, and patient counseling. Data were summarized using descriptive statistics. Confidence scores were compared across groups with t-tests, and predictors were analyzed using logistic regression.
Results:
Among 194 respondents, overall self-reported confidence was moderate (70.3%). While a strong majority felt confident in foundational tasks, such as discussing indications and benefits (over 79%) and adverse effects (71%), considerably lower confidence was reported in managing critical scenarios, including controlling bleeding events (~60%). This indicates a disparity between theoretical knowledge and confidence in practical application. Hospital pharmacists reported higher confidence levels than community pharmacists. The most frequently referenced resources were Lexicomp (18.6%) and clinical guidelines (17.5%).
Conclusions:
While Saudi pharmacists report foundational knowledge of anticoagulants, a significant confidence gap exists in the management of serious complications. These findings suggest that continuing education programs should move beyond theoretical knowledge and focus intensively on practical, case-based training in bleeding management and emergency response. A key limitation of this study is its reliance on self-reported data, which may not reflect objective competence.
Introduction
Anticoagulant therapy is a critical, high-risk intervention for conditions like venous thromboembolism (VTE) and atrial fibrillation (AF).1,2 The management of this drug class has evolved significantly with the widespread adoption of direct oral anticoagulants (DOACs), which, despite offering advantages over warfarin, such as fewer drug-drug interactions and no required routine monitoring, present new challenges.3–7 These challenges primarily concern ensuring adherence due to their short half-lives and managing complications without a readily available reversal agent or standard monitoring test. 8
In this complex landscape, pharmacists play a vital role in optimizing patient outcomes. Evidence from various settings demonstrates that pharmacist involvement in anticoagulation management, through patient education, monitoring, and collaborative care, significantly improves therapeutic outcomes, reduces bleeding and thromboembolic events, and decreases hospitalizations. This role is now shifting from traditional warfarin management based on INR monitoring to a focus on counseling, adherence checking, and managing drug interactions for patients on DOACs.9–12
Saudi Arabia presents a unique and critical context for this evolution of the practice. The Kingdom is undergoing a major healthcare transformation aligned with Vision 2030, which emphasizes pharmaceutical care and expanding the clinical roles of pharmacists. 13 Concurrently, the burden of cardiovascular diseases and risk factors for thrombosis (e.g. an aging population, high prevalence of metabolic syndrome) is rising, likely increasing the use of anticoagulants.14–18 Despite this, the specific confidence and preparedness of Saudi pharmacists to take on this expanded role remain completely unassessed.
While previous studies have established the value of pharmacists in anticoagulation management globally, the applicability of these findings to the Saudi healthcare system, with its distinct educational pathways, practice settings, and cultural considerations, is unknown. A simple replication of a “confidence survey” is not the goal; the imperative is to understand the readiness of the Saudi pharmaceutical workforce to safely manage a high-risk drug class within a rapidly transforming health system. Therefore, this study aims to assess the confidence level of pharmacists in Saudi Arabia in providing pharmaceutical care for patients on anticoagulants. The findings will identify specific educational needs and practice gaps, providing essential data for policymakers, educators, and professional bodies to develop targeted training programs. This is a crucial step toward ensuring patient safety and effectively integrating pharmacists into advanced clinical roles within the Saudi healthcare system.
Methods
Study design
Between June 2024 and August 2024, a cross-sectional study was conducted to assess pharmacists’ confidence and educational needs regarding anticoagulants among pharmacists in various clinical settings in Saudi Arabia. Data were collected through an online self-administered questionnaire distributed via Google Forms. While this approach facilitated wide and efficient dissemination, it introduces potential limitations, particularly selection bias, as participation required internet access and familiarity with online platforms. Consequently, the sample may over-represent younger, more technologically adept pharmacists, which should be considered when interpreting the findings. A non-probability convenience sampling method was employed to recruit participants. The inclusion criteria for the study were: (1) licensed pharmacists currently practicing in Saudi Arabia, (2) involved in any capacity with the management of patients on anticoagulants (e.g. dispensing, counseling, inpatient monitoring). The exclusion criteria were: (1) pharmacy students or unlicensed interns, (2) licensed pharmacists not currently in active practice, and (3) survey responses that were substantially incomplete. The reporting of this cross-sectional study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Statement for cross-sectional studies. The completed STROBE checklist is provided as a Supplemental File.
Ethical approval
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Research Ethics Committee of Prince Sattam bin Abdulaziz University (Approval Number SCBR-065-2023). Participation was voluntary. Before the study, all respondents were presented with a detailed information page outlining the study’s purpose, procedures, risks, benefits, and their right to withdraw. Written informed consent was obtained from all respondents before any study procedures began.
Sample size
Raosoft’s sample size calculator was used to estimate the required sample size (response distribution 50%, margin of error 5%). Although a 95% confidence level is typically used, we selected 80% to account for practical constraints in recruiting participants within the study timeframe. This resulted in a minimum required sample of 163 respondents. While this approach allowed the timely completion of the study, it introduces a limitation in statistical confidence that should be considered when interpreting the results.
Data collection
A structured questionnaire consisting of 27 items was developed for this study. The first section collected basic demographic characteristics, including age, gender, region, years of pharmacy experience, education level, and practice department. The second section assessed the frequency of encountering anticoagulants in pharmacy practice. The third section explored pharmacists’ confidence in managing anticoagulant therapy, while the final section assessed sources of information and educational needs related to anticoagulant use.
The questionnaire was developed after a review of the literature on pharmacist knowledge and confidence in anticoagulant therapy. Although no universally validated scale specific to pharmacist confidence in anticoagulant use was available, the items were adapted from existing surveys assessing clinical confidence in medication management and then refined for relevance to the Saudi clinical context. The draft questionnaire underwent a multi-step validation process. First, content validity was evaluated by two clinical pharmacy faculty members with expertise in survey development, who reviewed each item for relevance, clarity, and comprehensiveness. Minor revisions were made based on their feedback. The questionnaire was then pilot-tested with five practicing pharmacists to assess clarity, readability, and item interpretation. Feedback from the pilot testing led to further refinement of the wording and response options. Finally, the internal consistency reliability of the confidence scale was assessed using Cronbach’s alpha, which yielded a value of 0.89, indicating good internal consistency. The final questionnaire was converted into an online format using Google Forms and distributed to pharmacists via email and professional networks.
Data analysis
Chi-square tests (χ²) were used to examine associations between categorical variables, such as years of experience and encounter frequency, as well as between experience and preferred training format. Independent samples t-tests and one-way ANOVA were applied to compare mean confidence scores across demographic groups (e.g. gender, region, and years of experience). Binary logistic regression analysis was then performed to identify predictors of high confidence in providing anticoagulant care. A p-value of <0.05 was considered statistically significant for all analyses.
Results
Demographic characteristics
A total of 194 pharmacists completed the survey (response rate: 64.7%), based on 300 distributed invitations. Table 1 summarizes participant demographics. Most were male (60.8%) and under 40 years old (91%). The majority practiced in the central region (63.4%), had fewer than 5 years of experience (55.7%), and worked primarily in hospital settings (51.6%).
Demographic characteristics of respondents (n = 194).

Pharmacists’ exposure to anticoagulants
More than half of respondents reported at least sometimes encountering anticoagulants in practice: 55.2% for warfarin, 57.2% for low-molecular-weight heparins, and 59.8% for direct oral anticoagulants (DOACs). Only 14.4% were currently involved in a Warfarin Medication Therapy Adherence Clinic.
A chi-square test showed a significant association between years of experience and frequency of anticoagulant encounters (χ² = 10.82, p = 0.004), with those having ≥10 years of experience more likely to encounter anticoagulants regularly.
Confidence in anticoagulant care
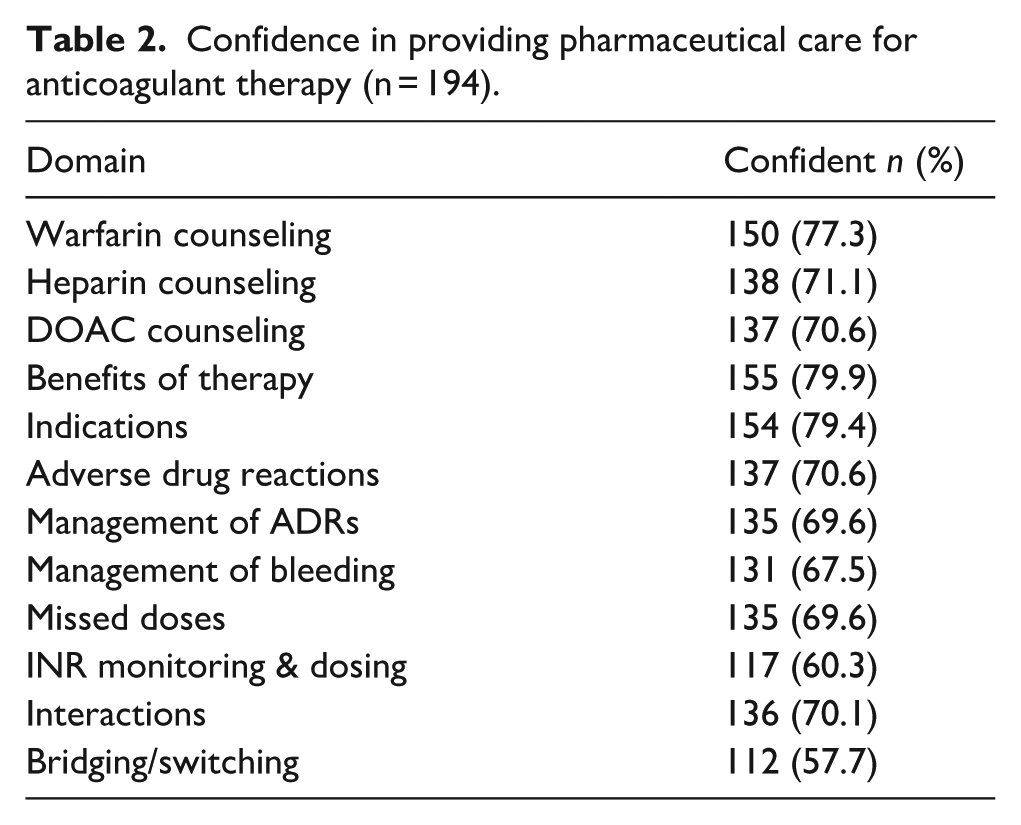
For each domain, the confidence level was calculated as the percentage of participants who reported being confident. Based on common clinical interpretation, confidence was pre-defined as: Low (0%–59%), Moderate (60%–79%), and High (80%–100%). Pharmacists reported moderate to high confidence across all domains (mean confidence score = 70.3%). Confidence was highest for discussing the indications (79.4%) and benefits (79.9%) of therapy, while it was lower for bridging/switching anticoagulants (57.7%) and INR monitoring (60.3%) (Table 2).
Confidence in providing pharmaceutical care for anticoagulant therapy (n = 194).
Inferential analysis revealed several significant associations. Pharmacists with ≥10 years of experience had higher mean confidence scores (M = 75.2, SD = 8.9) than those with <5 years (M = 68.4, SD = 10.7; t (190) = 3.64, p < 0.001). Similarly, those practicing in the central region reported higher confidence (M = 72.8, SD = 9.4) than those in other regions (M = 66.9, SD = 11.2; t (192) = 3.27, p = 0.001). No statistically significant differences were observed by gender (p = 0.21) or education level (p = 0.25).
Predictors of confidence
Logistic regression identified two significant predictors of higher confidence (Table 3). Pharmacists who frequently encountered anticoagulants were more than twice as likely to report high confidence (OR 2.3, 95% CI 1.2–4.4, p = 0.01). Practicing in the central region was also associated with higher confidence (OR 1.9, 95% CI 1.1–3.6, p = 0.015). Other factors, including age, gender, years of experience, and education level, were not significant predictors.
Logistic regression analysis of factors associated with pharmacist confidence.

Sources of information and training needs
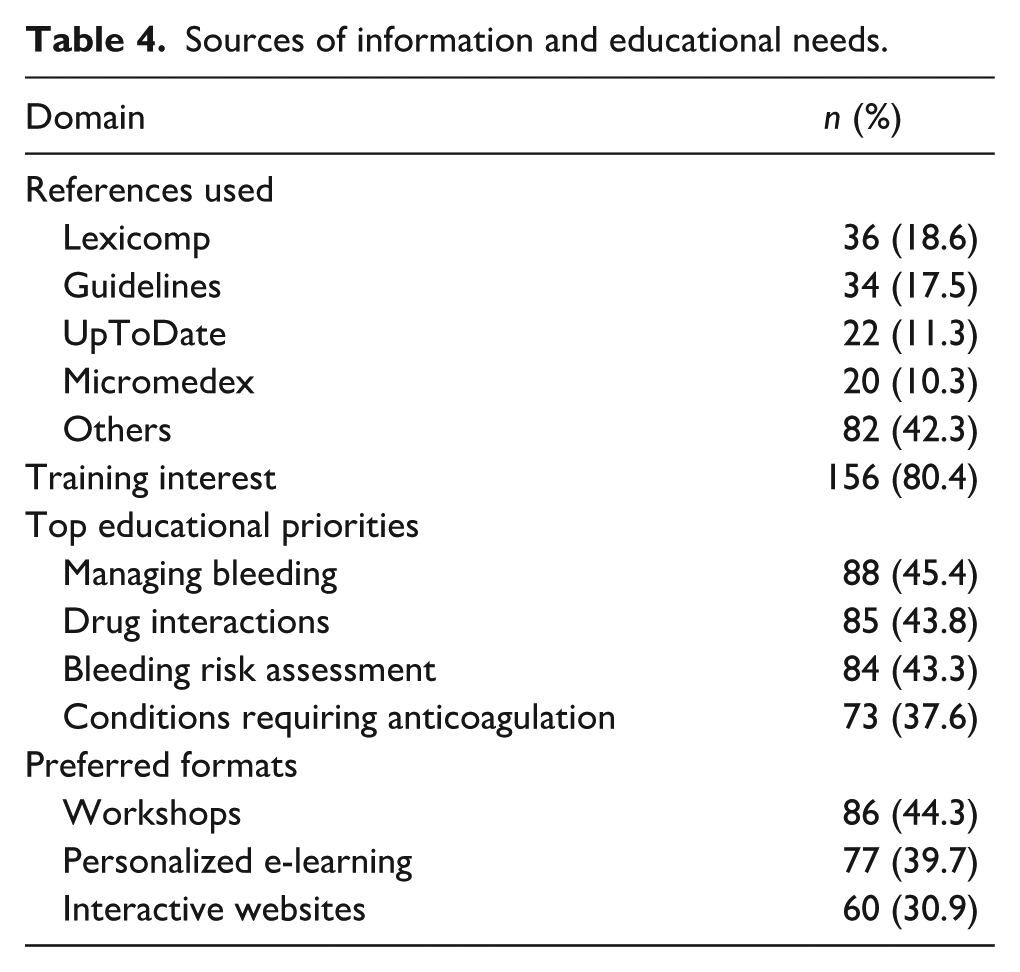
Pharmacists most commonly consulted Lexicomp (18.6%), clinical guidelines (17.5%), and UpToDate (11.3%) for information on anticoagulants. Over 80% expressed interest in additional training, particularly in managing bleeding (45.4%), drug interactions (43.8%), and assessing the risk of bleeding (43.3%). Workshops (44.3%) and personalized e-learning (39.7%) were the preferred formats for continuing education (Table 4). A chi-square test indicated that pharmacists with <5 years of experience were more likely to prefer e-learning formats, whereas those with ≥10 years of experience preferred workshops (χ² = 7.21, p = 0.027).
Sources of information and educational needs.
Discussion
To the best of our knowledge, this is the first questionnaire survey conducted in Saudi Arabia to examine pharmacists’ confidence in managing anticoagulants. Our findings reveal a gradient of confidence among Saudi pharmacists, with the highest confidence reported in managing warfarin (77.32%), followed by heparins (71.13%) and direct oral anticoagulants (DOACs) (70.62%). This pattern is consistent with international studies. A multinational survey reported mean confidence levels of 78.2% for vitamin K antagonists and 53.0% for DOACs, 8 while research in Malaysia showed a similar disparity (88.3% for warfarin vs 38.9% for DOACs). 11 This suggests a global trend where longer-established therapies inspire greater confidence than newer agents.
However, merely noting this trend is insufficient; the crucial question is why this pattern exists within the Saudi context. We posit that the observed confidence gradient is not merely a function of time but is directly shaped by specific systemic and educational factors within the Saudi healthcare system. The significantly higher confidence with warfarin is likely a direct result of its entrenched role as the primary anticoagulant in government healthcare facilities, where most pharmacists undergo their foundational training and early career development. This prolonged and widespread use provides repeated, hands-on experience. Furthermore, as noted, warfarin management and patient counseling are often formalized components of pre-registration training, creating a structured educational foundation that is often lacking for newer DOACs. 12 The rapid adoption of DOACs globally has arguably outpaced the integration of comprehensive, standardized training programs into pharmacy curricula and continuing education in many regions, including Saudi Arabia, leaving pharmacists to bridge this knowledge gap through self-directed learning.
Although the overall confidence level was moderate (70.3%), interpreting this finding in the context of pharmacists’ characteristics provides deeper insight. Pharmacists with more years of professional experience generally demonstrated higher confidence scores, suggesting that repeated exposure to anticoagulant management may enhance competence over time. Differences were also observed across practice settings, where pharmacists working in hospital or clinical environments tended to report greater confidence compared with those in community settings, likely due to more frequent involvement in anticoagulant therapy monitoring and dose adjustments. Furthermore, pharmacists who had previously received anticoagulant-related training or continuing education showed higher confidence levels than those without such training, highlighting the importance of targeted educational programs. These patterns emphasize that confidence is not uniform across the profession and may be shaped by both experiential and educational factors, underscoring the value of structured anticoagulation training initiatives in Saudi Arabia.
Beyond drug-specific confidence, our study identified areas of universal strength and weakness. While pharmacists were confident discussing the indications and benefits of anticoagulation, they reported lower confidence in managing complex scenarios like bleeding events and adverse drug reactions. This aligns with the findings of Ghadrdan et al., indicating a common challenge across practice settings: translating theoretical knowledge into advanced clinical management. 8 This decline in confidence with increasing clinical complexity underscores a critical gap in practical, applied training.
The overwhelming desire for further education (>80% of respondents) powerfully reinforces this interpretation. This expressed need moves beyond a simple result and becomes a key finding in itself, highlighting a perceived deficiency in current training structures. The preferred modalities—workshops, tailored e-learning, and interactive websites—suggest a demand for engaging, case-based, and practical learning over passive formats. This aligns with global trends,8,11,19 but must be viewed through a local lens: the centralization of specialized healthcare and expert knowledge in major regions like Riyadh (Central Region) may limit learning opportunities for pharmacists in peripheral areas. This is supported by our finding that pharmacists in the Central Region reported higher confidence, suggesting that proximity to specialized centers and their associated training programs is a key contextual factor influencing confidence.
This study addresses the critical and under-investigated area of anticoagulant management by pharmacists in Saudi Arabia. As one of the first of its kind, it provides a crucial baseline assessment that identifies specific educational needs, offering valuable data to guide the development of targeted training and policy. This study has several limitations that should be taken into account when interpreting the results. Firstly, the reliance on self-reported data is susceptible to social desirability bias. Participants may have overstated their confidence levels, which suggests that the gap between knowledge and confidence identified in our findings might be even more pronounced in actual practice. Secondly, the cross-sectional design provides a snapshot of the current situation but cannot establish causal relationships. For example, while we observed an association between years of experience and higher knowledge scores, we cannot conclude that experience directly caused this improvement. Thirdly, despite employing a broad sampling strategy, the potential for selection bias must be acknowledged. Pharmacists with a pre-existing interest or greater confidence in anticoagulation were likely more motivated to participate. Consequently, our sample may overrepresent this group, potentially leading to an overestimation of the overall knowledge levels among the wider population of pharmacists in Saudi Arabia. Finally, although the study relies on self-reported data, which may be subject to recall bias, there is also a possibility of social desirability bias, whereby participants may overestimate or underreport their actual confidence or practices. Future studies should incorporate objective performance measures—such as direct observation, skills assessments, or standardized clinical vignettes—to validate and complement self-reported confidence levels.
Based on our analysis, we recommend a multi-faceted strategy addressing root causes: integrating enhanced, standardized anticoagulant modules, especially on DOACs, into pharmacy curricula; developing accredited, case-based virtual continuing education to improve accessibility; implementing a competency-based certification program to ensure proficiency; and promoting clinical decision support tools in electronic health records. Given the gap identified between theoretical knowledge and practical confidence, targeted educational strategies are needed to better prepare pharmacists for real-world anticoagulation management. Simulation-based training workshops—using case scenarios, interactive decision-making exercises, and virtual patients—could help pharmacists practice complex dosing, monitoring, and management of bleeding or thrombotic complications in a safe learning environment. Additionally, establishing structured certification programs focused on anticoagulant stewardship, similar to anticoagulation management certification courses used internationally, could standardize competencies across the profession in Saudi Arabia. Integrating these models into continuing professional development programs would provide pharmacists with hands-on skills and validated credentials, ultimately enhancing the quality and safety of anticoagulant care.
Conclusion
This study assessed Saudi Arabian pharmacists’ self-reported confidence in managing common anticoagulants, including warfarin, heparins, and DOACs. The findings indicate a gradient in perceived confidence, with the highest levels reported for warfarin and lower levels for direct oral anticoagulants. Importantly, it must be emphasized that this study measured confidence as a perception and did not objectively assess clinical competence. Pharmacists expressed the greatest confidence in discussing indications and benefits, but the least in managing critical scenarios like bleeding complications. These findings highlight a crucial need for targeted, practical education and training programs. Future efforts must focus not only on improving confidence but, more critically, on verifying and ensuring actual competency to safely manage patients on these high-risk medications.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251407189 – Supplemental material for Pharmacists’ self-reported confidence in providing pharmaceutical care on anticoagulants in Saudi Arabia
Supplemental material, sj-docx-1-phj-10.1177_22799036251407189 for Pharmacists’ self-reported confidence in providing pharmaceutical care on anticoagulants in Saudi Arabia by Ghada Alem, Nehad Jaser Ahmed, Noura Albarak, Amirah Almakawini, Dania Almousa, Ziyad Almalki, Abdullah Alahmari, Ahmed Alshehri and Mohammed Balaha in Journal of Public Health Research
Footnotes
Ethical considerations
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Committee of Prince Sattam bin Abdulaziz University (Approval Number SCBR-065-2023). Participation was voluntary, and informed consent was obtained electronically from all respondents after they were presented with a detailed information page outlining the study’s purpose, procedures, risks, benefits, and their right to withdraw.
Author contributions
G. Alem supervised the study. N. Ahmed performed the formal analysis and drafted the initial manuscript. G. Alem, Z. Almalki, and A. Alahmari contributed to reviewing and editing the manuscript. A. Alshehri and M. Balaha handled the conceptualization and methodology. N. Albarak, A. Almakawini, N. Ahmed, and D. Almousa were responsible for software and data curation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2022/03/20509).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All information and data for this research will be made available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.