
Abstract
Background:
Stunting is a global health challenge with high prevalence in Asia and Africa. Although many studies have discussed its determinants, fragmented evidence and regional differences still hinder the formulation of effective policies.
Objective:
This study aims to identify and map predictors of stunting in children under 5 years of age, focusing on socio-demographic, prenatal, natal, and postnatal factors, as well as distinguishing universal and contextual determinants across regions.
Design and methods:
This systematic review followed the PROSPERO protocol (CRD42025633321) and the PRISMA 2020 guidelines. Literature searches were conducted in databases (Scopus, Web of Science, PubMed, ProQuest, ScienceDirect, Taylor & Francis, and Emerald). Included articles were original English-language studies published between 2015 and 2024 that examined predictors of stunting in children aged 0–59 months. Methodological quality was assessed by two independent reviewers using the JBI Critical Appraisal Tools. Data were then extracted, narratively synthesized, and mapped according to UNICEF regional classifications.
Results:
Of the 5094 initial records, 92 studies met the inclusion criteria. Maternal education, socioeconomic status, sanitation, maternal age, maternal height, birth weight, and exclusive breastfeeding and complementary feeding practices emerged as the most consistent and universal predictors. Other factors were more contextual, depending on the region. Cross-regional analysis confirmed the existence of universal determinants as well as specific regional risk factors.
Conclusion:
Stunting is a multifactorial problem across life phases. Regional mapping enriches theoretical understanding and provides a scientific basis for context-based policies. These findings emphasize the need for multi-level interventions and cross-regional longitudinal research with uniform measurement standards.
Keywords
Introduction
Stunting represents a persistent nutritional issue that continues to be a worldwide challenge. In 2020, 22% or 149.2 million children under 5 years old were stunted, with the majority of cases concentrated in Asia (53%) and Africa (41%). The prevalence of stunting based on country income level is predominantly observed in lower-middle-income countries (59%) and low-income countries (25%). 1 Growth retardation commences in utero during the initial phases of fetal development and intensifies after the introduction of supplemental foods post-weaning at 6 months of age. 2 The continued high prevalence of stunting increases the need to understand sociodemographic factors as a general approach in stunting-related studies. This understanding helps comprehend the complexity of stunting, reframing policies, and designing more specific actions to address the issue. 3 Prenatal, natal, and postnatal factors also play important roles in stunting. The role of the mother during the prenatal stage is a key determinant for preventing stunting in children. Maternal nutrition is crucial in fetal growth, infant survival and health, and child growth and health in the long run. During the first half of the critical 1000-day period (conception to 6 months), the mother is the sole source of nourishment for the unborn and the child’s first 6 months in the womb and then during the first 6 months of life when the child is exclusively breastfed. Adverse prenatal conditions may be a factor in the susceptibility to stunting among children. Thus, prenatal determinants need to be prioritized in early stunting prevention programs. 4
Children who experience growth deficits from birth (natal period) significantly increase their risk of stunting and chronic diseases later in life. Infants with low birth weights (LBWs) exhibit a heightened susceptibility to illnesses such as diarrhea and lower respiratory tract infections, along with various additional problems. 5 During the postnatal stage, the nutritional requirements during the initial 2 years of a child’s life must be adequately met to promote growth and development. Repeated infections during this time can significantly raise the risk of stunting. The role of mothers in this phase is to meet the nutritional requirements of infants and children, initiate early breastfeeding, practice exclusive breastfeeding, provide appropriate complementary feeding, optimize the environment for child growth and development, maximize family support, and avoid various psychosocial factors that can be detrimental to the growth and development of children 4
This literature review aims to identify and map predictors of stunting in children under 5 years of age, focusing on socio-demographic, prenatal, natal, and postnatal factors and distinguishing universal and contextual determinants across regions. Through this evidence-based approach, we hope to gain a deeper understanding of the complexity of stunting’s causes and support the development of more effective policies and interventions to reduce its prevalence.
Materials and methods
The study protocol was finalized prior to the start of the study and has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42025633321. This systematic literature review was conducted via the following steps:
Development of research questions with the PICO framework
Specific research questions were determined to guide the literature search and selection process. This systematic review used the PICO framework. PICO is an acronym for Patient, Population, or Problem (P), Intervention, Exposure, or Prognostic Factor (I), Comparison (C), and Outcome (O). This framework is used to formulate research questions and effective search strategies. 6 In this systematic review, the PICO components used were as follows: the population (P) of interest in this study was children under five or toddlers. The intervention (I) applied is a predictor. The comparison (C) is not applied in this study. Moreover, the outcome (O) that is the focus of this study is stunting.
Identification Process
The literature identification process in this systematic review was conducted via databases: Proquest, ScienceDirect, Scopus, Web of Science, Taylor Francis, PubMed, and Emerald. Search strategies were developed specifically for each database using relevant keywords. The keywords used were TITLE-ABS-KEY (“children under five” OR “infants” OR “children 0–59 months”) AND (“predictors” OR “risk factors”) AND (“stunting”). Using multiple databases and customized search strategies, this review comprehensively identified relevant literature. 7
Screening process
Explicit inclusion criteria used in this systematic review helped to pinpoint relevant research for the screening process. Articles published between 2015 and 2024 in English, with an eye toward stunting predictors for children under five, made up the inclusion criteria. Screening excluded studies using a systematic design, meta-reviews, book chapters, or qualitative research. Using the systematic application of inclusion and exclusion criteria during the screening process, the review guaranteed to include only the most pertinent and high-quality studies. A well-organized systematic review depends on a thorough screening procedure to guarantee that the conclusions are formed from the most trustworthy evidence. 8
Quality assessment
The risk and methodological quality of the studies were assessed via the Joanna Briggs Institute (JBI) Critical Appraisal Tools, which include standardized checklists for assessing various designs. 9 Two independent reviewers (HIA and NN) assessed each study using the relevant JBI tools according to the study design. Disagreements were addressed via discussion or involving a third reviewer (VW). The reviewer worked independently throughout the quality assessment process. No automation tools were used in this process; the reviewers conducted all assessments manually. Each study was classified as having a low, moderate, or high risk of bias based on the JBI criteria. The risk of bias assessment results are presented in tabular format based on studies with a lower risk of bias.
Data extraction
The extracted data included study characteristics, sample size, design, variables studied, and main results. Articles that met the criteria were then categorized based on four groups of factors: sociodemographic, prenatal, natal, and postnatal. In addition, to ensure clarity of regional perspective, all findings were extracted and mapped using UNICEF’s (2023) regional classification: East Asia and Pacific (EAP), South Asia (SA), Sub-Saharan Africa (SSA), and Latin America & Caribbean (LAC).
Data synthesis
Synthesis was conducted narratively and visually. Narrative synthesis was organized into themes and key patterns, while visual synthesis was presented through tables and charts. In addition to being based on factor categories, the synthesis was also conducted using UNICEF’s regional perspective to distinguish between universal predictor factors and factors that are more contextual in nature according to regional characteristics. This study did not conduct a meta-analysis due to the heterogeneity of the research designs, populations, and measurement methods in the included studies.
Strengths and limitations of the review strategy
This systematic review has several notable methodological strengths. The research protocol was previously registered in PROSPERO (CRD42025633321) with a clearly defined PICO framework, ensuring a focused and systematic approach. The search strategy covered seven major databases—Scopus, Web of Science, Taylor & Francis, PubMed, ScienceDirect, ProQuest, and Emerald—with keyword adjustments according to the characteristics of each, thereby expanding the scope of relevant literature. In addition, quality assessment using the Joanna Briggs Institute (JBI) Critical Appraisal Tools by two independent assessors increased the reliability of study selection.
However, there are a number of limitations that need to be considered. Variations in study design, population, and measurement methods meant that meta-analysis could not be performed, thus limiting the generation of quantitative estimates. Restricting the search to English-language articles published between 2015 and 2024 excludes relevant studies in other languages or from different periods. The absence of qualitative studies limits our understanding of contextual factors and life experiences that are not fully reflected in quantitative data. Attempts to contact authors were not always successful in obtaining additional information, which could lead to selection or reporting bias. In addition, differences in the recording and measurement of stunting outcomes between studies make direct comparisons difficult.
Results
Based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist, the search and resource choosing process outcomes are shown in Figure 1. Figure 1 illustrates the specifics of the identification, screening, and inclusion process.

PRISMA 2020 flow diagram for systematic reviews.
A summary of the systematic literature review (SLR) process used to identify studies on predictors of stunting in children under 5 years of age, based on the PRISMA diagram, is presented. This diagram illustrates the rigorous selection process to ensure that only relevant and high-quality studies were included in the review. The results of the database identification yielded a total of 5094 articles, with the following details: This PRISMA diagram illustrates the systematic selection process of studies for a literature review. In the identification stage, a total of 5094 records were identified from various databases: Scopus (3139), WoS (320), Taylor & Francis (909), PubMed (117), Science Direct (214), Proquest (173), and Emerald (222). Before the screening process, 687 duplicate records were removed. Of the 4407 records remaining for screening, a large number (4179) were excluded for various reasons: publications before 2015 (1421), non-English language articles (733), review articles (132), conference proceedings (14), conference articles (54), books and book chapters (20), editorials and notes (97), and irrelevant titles and abstracts (1719). In the next stage, 217 reports were identified for inclusion, but 23 could not be retrieved. Of the 193 reports assessed for eligibility, 101 were excluded: 98 because the full text was outside the scope of the research question and three because they did not meet the JBI quality assessment criteria. Finally, 92 studies were included in the final review. This systematic review aims to identify and map predictors of stunting based on sociodemographic, prenatal, natal, and postnatal factors. The synthesized results of 92 studies that met the inclusion criteria are presented in the following table.
Table 1 maps the socialdemographic determinants of stunting across UNICEF regions. Four universal predictors—socioeconomic status, education, sanitation, and maternal age—are consistently significant across all regions. These factors influence households’ ability to provide nutritious food, access and utilize health services, and implement good parenting practices. Conversely, variables such as toilet facilities, water sources, gender, child age, household size, maternal occupation, and residence show heterogeneity of findings across regions. Some determinants are highly contextual—ethnicity/caste and household head characteristics—which are particularly prominent in South Asia and Sub-Saharan Africa. This overall pattern confirms the existence of a combination of universal factors that can be targeted by global policies and context-specific factors that require region-based intervention strategies.
Predictive factors of stunting in the sociodemographic by regional area.

(√): consistently significant evidence across regions; (±): inconsistent or mixed findings across regions; (−): limited evidence (few studies).
In terms of prenatal factors, maternal height emerged as the most consistent significant predictor across all regions. This confirms the importance of the mother’s chronic nutritional status before and during pregnancy on the risk of stunting in children. Other factors, such as maternal weight, maternal nutritional status, maternal body mass index (BMI), and multiple pregnancies (multiparity), were found in several regions, particularly East Asia and Sub-Saharan Africa, but did not show universal consistency. Other predictors, such as gestational age, pregnancy interval, antenatal care (ANC) visits, deworming during pregnancy, and unplanned pregnancy, were reported more frequently in Sub-Saharan Africa, with a limited number of studies, and can therefore be categorized as context-specific factors (Table 2).
Predictive factors of stunting in the prenatal phase by regional area.
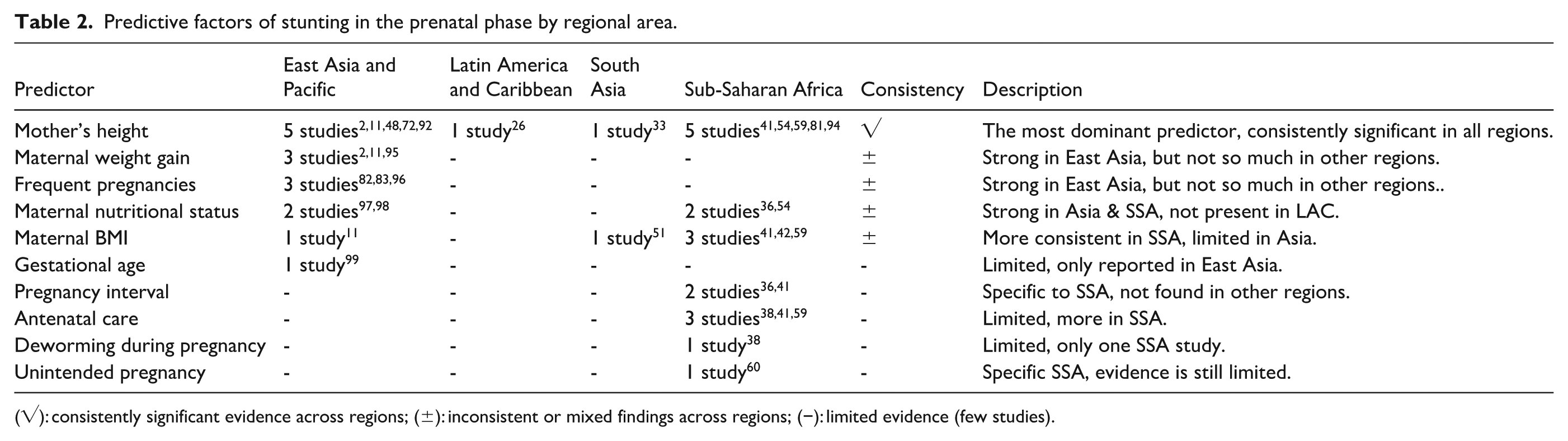
(√): consistently significant evidence across regions; (±): inconsistent or mixed findings across regions; (−): limited evidence (few studies).
In terms of natal factors, birth weight is the most dominant and consistent predictor across all UNICEF regions. Other variables, such as birth length, birth size (small for gestational age/SGA), and early breastfeeding initiation (EBI), were found in several studies, particularly in Asia and Sub-Saharan Africa, although not entirely consistent. Other more contextual predictors include place of delivery and birth order, which are dominant in Sub-Saharan Africa. Only a few studies report age at first birth, birth attendant, type of delivery (normal or cesarean section), and multiple births (Table 3).
Predictive factors of stunting in the natal phase by regional area.

(√): consistently significant evidence across regions; (±): inconsistent or mixed findings across regions; (−): limited evidence (few studies).
In the postnatal category, a history of childhood infections, exclusive breastfeeding, and complementary feeding are the most consistently significant factors in almost all regions. These findings confirm the importance of child health and feeding practices in early life as key determinants of stunting. Child nutrition intake, which includes dietary diversity, energy, protein, and micronutrients, is reported to be adequate in Asia but limited in other regions. Other factors that vary more widely are immunization, weight-for-age, and the prevalence of contraception among couples of childbearing age. Several other predictors emerged in limited studies and tended to be region-specific, such as inadequate feeding practices, dietary diversity, health worker education, parenting, colostrum, and childhood anemia (Table 4).
Predictive factors of stunting in the postnatal phase by regional area.

(√): consistently significant evidence across regions; (±): inconsistent or mixed findings across regions; (−): limited evidence (few studies).
Discussion
Predictors of stunting based on sociodemographic factors
The results of this systematic review confirm that socio-demographic factors are important determinants of stunting in children under 5 years of age, with four universal predictors that are consistently significant across regions, namely maternal education, socioeconomic status, sanitation, and maternal age. This consistency shows that stunting is not only influenced by biological factors, but also by structural contexts that determine access to resources, health services, and parenting practices. UNICEF’s cross-regional patterns show a combination of universal determinants relevant to global policy and contextual factors requiring region-specific interventions.
Maternal education consistently emerges as a protective factor against stunting. This finding is in line with a study in Indonesia showing that mothers with low education have a three times greater risk of giving birth to stunted children. 84 Other research also confirms that maternal education improves nutrition knowledge, health practices, and utilization of health services.108,109 Socioeconomic status has also been shown to be strongly associated with stunting. Poverty increases the risk of malnutrition, while families with higher incomes can provide nutritious food and better access to health services. 83 Socioeconomic disparities even have intergenerational effects through low maternal education and low birth weight. 110
Maternal age presents a double risk pattern: adolescent pregnancy (<20 years) increases the risk of stunting due to nutritional competition and psychosocial unpreparedness, while advanced maternal age (>35 years) is associated with obstetric complications and chronic diseases.111,112 This underscores the importance of programs promoting delayed marriage and family planning. Sanitation and access to clean water are also consistently significant. Children living in environments with poor sanitation are more vulnerable to diarrhea, worm infections, and environmental enteric dysfunction that impedes nutrient absorption.113,114 A study in Myanmar confirms that the use of unsafe sanitation facilities increases the risk of stunting by almost threefold. 115
Conversely, a number of factors indicate heterogeneity. Maternal occupation for example, can protect children by increasing income, but it also increases the risk of stunting due to reduced quality of care.87,116,117 Large household size tends to increase the risk of stunting due to limited food distribution, as shown by studies in Rwanda and Ethiopia.110,118 Other factors, such as residence, ethnicity, or household head characteristics, are more specific to certain contexts, particularly in Sub-Saharan Africa and South Asia.
Theoretically, these results reinforce UNICEF’s framework on child nutrition determinants, which places structural factors at the root cause of stunting. Practically, these findings underscore the need for multi-level policies: global interventions focused on maternal education, poverty reduction, and sanitation improvements, while local interventions address contextual issues such as cultural norms, household structures, or women’s work patterns. Future research needs to develop cross-regional longitudinal studies with uniform measurement standards to address the heterogeneity of findings, while deepening the analysis of cultural and gender factors that remain under-explained in the literature. 119
Predictors of stunting based on prenatal factors
This study shows that maternal height is the most consistent and universal prenatal predictor across all UNICEF regions. In contrast, maternal weight/weight gain, nutritional status (including BMI), and multiparity are strong predictors in East Asia and Sub-Saharan Africa but are not consistent across regions. Other factors—age at first pregnancy, birth spacing, ANC coverage, deworming during pregnancy, and unplanned pregnancy—were more frequently reported in Sub-Saharan Africa, with a limited number of studies, making them more context-specific. These findings address the study’s objective of mapping universal versus context-specific prenatal determinants and explaining the risk pathway from preconception to pregnancy.
Findings on maternal height are consistent with biological evidence that short stature reflects chronic nutritional deprivation, limited pelvic/uterine capacity, and reduced placental nutrient transfer leading to LBW and susceptibility to infection.5,120,121 Higher multiparity correlates with limited household resources and exposure to childhood infections, thereby increasing the likelihood of stunting.122,123
The results regarding ANC are consistent with evidence that adequate ANC contact improves birth weight and breastfeeding/PMBA practices after birth.96,124,125 Evidence of iron deficiency during pregnancy, increasing the risk of poor perinatal outcomes and immune disorders, is also consistent126,127 A South Asian meta-analysis confirms the benefits of IFA ≥ 120 tablet compliance in reducing stunting, 128 and the latest Indonesian cohort data reinforces the role of adequate IFA in preventing maternal anemia. 129
Discrepancies/contradictions arise regarding maternal BMI/weight and ANC: some studies find strong associations, while others find weak ones. This variation is likely influenced by differences in variable definitions/measurements (e.g. pre-pregnancy BMI vs during pregnancy), ANC recording quality, and population nutritional status heterogeneity. A new contribution of this study is a comparative cross-regional mapping that places each predictor on a universal–contextual spectrum, thereby clarifying where and when each factor is most relevant.
Theoretically, these results reinforce the nutritional causal model that places chronic maternal malnutrition as the root cause mediating the LBW-stunting pathway through the intrauterine environment and epigenetic programing. 121 Practically, interventions before and during pregnancy are crucial: preconception nutritional status screening, quality ANC packages (nutritional counseling, weight gain monitoring, anemia management), availability and compliance with IFA at a minimum according to national standards, as well as prevention of early/close pregnancies through contraception and delayed marriage.128–131 At the policy level, lower-middle-income countries need to combine universal interventions (IFA fulfilment, ANC strengthening) with contextual refinement: handling multiparity in SSA, strengthening preconception nutrition in Asia, and integrating deworming in endemic areas. This approach is in line with the SLR results, which call for adaptive policies per region.
The limited evidence and inconsistencies in ANC, BMI, and nutritional status across regions are quite surprising, given the strong biological rationale. Possible explanations include: variations in the quality of ANC services, misclassification of BMI (pre-pregnancy vs trimester), differences in cut-offs, and socioeconomic confounding factors that are not fully controlled for in observational studies. The predominance of deworming and unplanned pregnancy reporting in SSA may also reflect program focus and disease burden specific to that region, rather than the absence of effects in other regions.
Multi-regional longitudinal studies accompanied by standardized measurements are needed to assess the causal pathway from preconception nutrition → high/BMI of mother → LBW → stunting. The effectiveness of preconception-ANC intervention packages (intensive IFA, nutrition counseling, energy-protein supplementation, deworming in endemic areas) needs to be compared across contexts. Future research should also explore the epigenetic mechanisms and interactions between social and biological factors that mediate the influence of maternal deprivation on children’s linear growth.
Predictors of stunting based on natal factors
The results of this study confirm that birth weight is the most dominant and consistently significant birth predictor across all UNICEF regions. Other variables, such as birth length, birth size, gestational age, and early breastfeeding initiation (EBI), appear mainly in Asia and Sub-Saharan Africa, but are not entirely consistent. Place of delivery and birth order are more prominent in SSA. In contrast, age at first birth, birth attendant, type of delivery, and multiple births were found in only a few studies and can therefore be categorized as contextual factors. These findings reinforce the study’s objective of identifying universal versus region-specific predictors of birth factors.
Findings on birth weight are associated with LBW due to IUGR, which increases the risk of stunting through intrauterine growth deficit, immune system immaturity, and susceptibility to infection.5,124,132 Similarly, birth length has been shown to be an important indicator of long-term stunting risk; children born short (<48 cm) have a higher risk of stunting up to 24 months of age.133,134 Findings related to birth attendants and place of birth support evidence that the presence of trained health personnel and births in health facilities reduces the risk of stunting through risk monitoring, nutrition education, and neonatal services.135,136
Recent studies also highlight the influence of delivery type. Babies born via cesarean section tend to have limited microbiota colonization and an underdeveloped immune system, which increases susceptibility to infection and the risk of stunted growth. 137 Evidence from India shows a lower prevalence of stunting in children born normally compared to those born via cesarean section. 28 However, some results remain contradictory, for example, on the variable of birth order, which is significant in SSA but not in Asia. These differences likely reflect variations in family structure, access to contraception, and fertility norms. A new contribution of this study is the cross-regional comparative mapping, which shows differences in the distribution of natal factors based on regional context. This gap has rarely been addressed in previous systematic reviews.
Theoretically, these results reinforce the “developmental origins of health and disease (DOHaD)” framework, which places birth weight and birth length as indicators of intrauterine status that influence long-term growth trajectories.133,137 In practical terms, interventions need to focus on preventing LBW/IUGR through strengthening maternal nutrition, monitoring ANC, and detecting pregnancy risks. At the policy level, it is important to ensure delivery in health facilities with trained personnel and to regulate the use of cesarean sections according to medical indications. In the SSA region, fertility control and birth spacing policies are also relevant and in line with findings on birth order. Future research needs to explore the biological mechanisms of gut microbiota related to the type of delivery and its association with linear growth. Cross-regional longitudinal studies are also needed to assess the relationship between EBF, place of delivery, and birth order with uniform measurement standards. In addition, further research should integrate prenatal, natal, and postnatal factors to understand the interacting causal pathways.
Predictors of stunting based on postnatal factors
The synthesis shows three postnatal factors that are most consistent and cross-regionally associated with stunting: history of infection, exclusive breastfeeding, and complementary feeding. These results confirm that child health and feeding practices during the first 1000 days of life are the dominant risk/protection pathways. Other variables—nutritional intake/food diversity, immunization, and inadequate feeding practices—show variation between regions; they are strong in Asia but weaker in other regions. More contextual factors include colostrum (more common in LAC), vitamin A supplementation and childhood anemia (more common in SSA), and health worker education, parenting, ready-to-eat foods, and postnatal visits, which are primarily reported in Asia. These findings align with the study’s objective to distinguish universal versus context-specific determinants in the postnatal phase.
Findings on infection are consistent with evidence that repeated exposure to pathogens triggers environmental enteric dysfunction and malabsorption, which impedes linear growth.113,138 Exclusive breastfeeding has been shown to be protective through complete nutritional supply, immune components, and reduced exposure to contamination, and is a pillar of stunting prevention.139,140 Inappropriate timing/type/frequency of complementary feeding increases the risk of infection and malnutrition; conversely, dietary diversity and adequate protein intake—particularly animal protein—support growth141–143
Evidence consistently shows that colostrum provides early protection through immune factors and microbiota formation; children who do not receive colostrum are at greater risk of stunting.144,145 Current wasting/low weight is strongly correlated with stunting and shows a non-linear relationship, highlighting the need for early nutritional intervention.146–148 Differences emerged in immunization and postnatal visits that were not always significant across studies/regions—possibly due to variations in service coverage, quality of recording, and socioeconomic confounders. Consumption of ready-to-eat foods is also still limited, but early signals point to the risk of poor-quality diets. 149 A new contribution of this study is its cross-regional mapping, which explicitly shows where postnatal factors are universal and where they are context-dependent, thereby closing a gap in previous reviews that were generally single-region in nature.
Theoretically, the results reinforce UNICEF’s framework that the infectious disease ↔ intake pathway works synergistically through the mechanisms of EED, mucosal immunity, and early life programing.113,150 Practically, intervention priorities include promoting and supporting exclusive breastfeeding, providing timely/appropriate/frequent complementary feeding with affordable animal protein, and preventing and managing infections through WASH and integrated infant care. At the policy level, integrated nutrition-health-WASH packages need to be context-specific: strengthening infection + WASH and complementary feeding in Asia; preventing infections, anemia, and promoting colostrum/breastfeeding in SSA; and supporting mothers’ work so that breastfeeding practices are not disrupted in urban areas.
The variability in the association between immunization and postnatal visits is relatively surprising. Differences may influence this in service packages, indicator definitions (e.g. vaccine type, visit time window), recall bias, and residual confounding by education/poverty. The signal of ready-to-eat foods as a risk is also new and likely reflects nutritional transitions in cities, so its effect depends on family access and consumption patterns.
Longitudinal studies are needed to examine the interaction between infection, intake, and WASH on linear growth. The effectiveness of exclusive breastfeeding + nutritious complementary feeding + WASH promotion packages needs to be evaluated across regions. Measurements of dietary diversity and animal protein portions need to be standardized. Evidence on colostrum outside of LAC and the effects of ready-to-eat/ultra-processed foods on toddlers in LMICs is still minimal. Research also needs to assess mediators (microbiota, EED markers) and moderators (maternal education, work support/lactation rooms) to design precision interventions.
Conclusion
This systematic review shows that stunting in children under five is a multifactorial problem influenced by socio-demographic, prenatal, natal, and postnatal factors. Some predictors are universal and consistent across regions—including maternal education, socioeconomic status, sanitation, maternal age, maternal height, birth weight, history of infection, exclusive breastfeeding, and complementary feeding practices. On the other hand, there are more contextual factors specific to regional characteristics, such as multiparity, place of delivery, birth order, colostrum, vitamin A supplementation, and cultural and household structure factors. This synthesis emphasizes that preventing stunting requires an understanding across life stages and strategies that combine universal determinants with local factors.
This study makes an important contribution to the development of science by presenting a comparative mapping across regions based on the UNICEF framework. This approach clarifies the patterns of universal determinants that are relevant to global policy while identifying contextual factors that require locally based interventions. Theoretically, the results of this study reinforce the framework of child nutrition determinants and causal models that link chronic maternal deprivation, LBW, infection, and breastfeeding practices with the risk of stunting. In practical terms, these findings have implications for policy priorities: improving women’s education, alleviating poverty, strengthening antenatal and safe delivery services, and supporting adequate breastfeeding and complementary feeding. Stakeholders at the global, national, and local levels need to tailor interventions according to a combination of universal and local factors to be more effective.
Although comprehensive, this review has limitations in the form of research design heterogeneity, limitations in English-language publications from 2015 to 2024, and the absence of qualitative studies that can explore contextual experiences. Data gaps between regions and variations in indicator definitions also pose obstacles to direct comparison. Therefore, future research should conduct cross-regional longitudinal studies with uniform measurement standards, explore biological-social mechanisms (e.g. the role of microbiota and gender-cultural factors), and assess the effectiveness of nutrition-health-WASH intervention packages that are adaptive to the local context. Thus, scientific evidence can further strengthen global and regional efforts to accelerate the reduction of stunting prevalence.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251403945 – Supplemental material for Exploring the multifactorial predictors of stunting in children under five: A systematic review of the literature, 2015–2024
Supplemental material, sj-pdf-1-phj-10.1177_22799036251403945 for Exploring the multifactorial predictors of stunting in children under five: A systematic review of the literature, 2015–2024 by Heti Ira Ayue, Nurdiana Nurdiana, Viera Wardhani, Ani Budi Astuti, Heri Prayitno, Agung Dwi Laksono and Tonny Sundjaya in Journal of Public Health Research
Footnotes
Acknowledgements
We gratefully acknowledge the Varians Statistik Kesehatan for providing the boot camp and mentoring to improve the manuscript writing.
Abbreviations
ARI: Acute Respiratory Infections
ANC: Antenatal Care
BMI: Body Mass Indeks
DOHaD: Developmental Origins of Health and Disease
EBI: Early Breastfeeding Initiation
EED: Enviromental Enteric Dysfunction
HAZ: Height-for-age
IFA: Iron Folic Acid
IUGR: Intra-Uterine Growth Retardation
JBI: Joanna Briggs Institute
LAC: Latin America and Caribbean
LBW: Low Birth Weight
LAZ: Length-for-Age Z score
PICO: Patient, Population, or Problem; Intervention, Exposure, or Prognostic Factor; Comparison; Outcome
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PROSPERO: International Prospective Register of Systematic Reviews
SD: Standar Deviation
SGA: Small for Gestational Age
SLR: Systematic Literature Review
SSA: Sub-Sahara Africa
UNICEF: United Nations Children’s Fund
WASH: Water, Sanitation, and hygiene
WHO: World Health Organization
Author contributions
HIA, ADL, and HP conceptualized the study, registered the protocol, formulated the research questions, and conducted the identification, screening, extraction, and synthesis processes. NN and VW independently assessed the risk of bias and methodological quality, with ABA as the third reviewer to resolve disagreements. TS contributed to review of the manuscript. All authors made substantial contributions to conducting the research and drafting the manuscript, critically revised the manuscript, and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.