
Abstract
Background:
Reproductive health literacy (RHL) is essential for informed decision-making and reducing high-risk behavior, yet gaps persist among adolescents, particularly in culturally conservative societies like Iran. In the present study, we sought to identify RHL levels and associated sociodemographic and educational factors among medical sciences students at Babol University of Medical Sciences.
Design and methods:
A cross-sectional study was carried out from October to December 2021, enrolling 475 students via stratified random sampling. Tools used for collecting data included validated socio-demographic questionnaires and WHO-based RHL tools. Independent t-tests and ANOVA were used for analyses in SPSS version 24.
Results:
The mean RHL score was 81.07 (adequate level). There were significant differences between the demographics and academic factors: higher RHL among married students than singles (d = 0.72, large effect), females scored higher than males (d = 0.28), and medical students scored higher than nursing (d = 0.68) and paramedical peers (d = 0.82). Older students (≥20 years) and higher academic years showed moderate-to-large improvements (d = 0.34–0.32). Conversely, younger students, males, and non-medical majors reported lower RHL. Sociocultural factors (e.g. residence type) had weaker but significant effects (d = 0.21).
Conclusion:
While RHL among these medical students was generally adequate, significant disparities were linked to gender, marital status, and academic major. Targeted interventions, such as revising non-medical curricula and introducing early RHL education, are recommended to address these inequities, particularly among males and younger students.
Introduction
Reproductive health, which constitutes the physical, mental, and social well-being of the reproductive system at all stages of life, 1 is a basis for both individual and public health. Reproductive health literacy (RHL)enables individuals to access, understand, and apply information, to make informed decisions about their reproductive health. This encompass knowledge of contraceptive services, STI prevention, safe pregnancy procedures, and postnatal care. 2 Despite its significance, RHL remains a paramount global issue, especially among the youth. 3 The Centers for Disease Control and Prevention (CDC) reports that 50% of new STI cases occur in individuals aged 15–24, with chlamydia and gonorrhea rates peaking among those aged 20–24. 4 These statistics underscore the urgent need to address gaps in RHL—a key determinant of informed decision-making and healthier behaviors.
The understanding of RHL is informed by a multifaceted interaction of demographic, social, and cultural constructs. Inequalities related to education and socioeconomic status have been reported 5 ; for instance, women and individuals of higher social status in Japan show better fertility awareness. 6 While in Iran, unmarried women under 25 years and persons with lower educational levels have lower RHL.7,8 Cultural norms further complicate these challenges.
In Iran, discussions around sexuality remain taboo, particularly among single youths, which inhibits open discussion and denies access to essential services. Female students face added societal censure, while the male students often receive minimal specialized training, thus perpetuating myths and risky behaviors. These challenges correlate with alarming statistics on unwanted pregnancies (30.6%), unsafe sex (34%), and poor knowledge of STIs among youths in Iran. 9 While general health literacy has been widely investigated, RHL requires specific focus due to its sensitive nature, involving culturally provocative topics such as STI prevention and contraception that are often stigmatized in the Iranian context. 10 Standard health literacy tools cannot fully address these facets, and significant gaps exist.
Despite Iran’s large youth population (46.9% under 30 years) and the pressing need for targeted interventions, there is limited research on RHL among university students, a key demographic vulnerable to poor sexual health outcomes. 11 The present study aimed to identify RHL levels and associated sociodemographic and educational factors among medical sciences students at Babol University of Medical Sciences. By investigating the determinants of RHL among Iranian medical sciences students—future healthcare providers—this study seeks to address this gap. The findings aim to underpin contextually appropriate policies and interventions to empower young people and reduce high-risk behaviors.
Material and methods
Study design and setting
This cross-sectional study was conducted at Babol University of Medical Sciences from October to December 2021. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The STROBE checklist has been completed and is provided as Supplemental Material.
Material
Participants and sampling
The study population included all students enrolled at the Babol University of Medical Sciences in the 2021–2022 academic year. A stratified random sampling technique was employed to ensure representativeness across faculties and gender. The sample size was calculated using G*Power software, with a power of 80%, a confidence interval of 95%, and an effect size of 0.3, resulting in a required sample of 475 participants.
Inclusion criteria were: age 18 years and above, Iranian nationality, and provision of written informed consent. Exclusion criteria included incomplete questionnaires and non-enrolled (e.g. visiting) students.
Data collection tools
Data were collected via two self-administered questionnaires:
The questionnaire uses a 5-point Likert scale, with total scores ranging from 37 to 185. For analytical clarity, scores were rescaled to a 0–100 range. RHL levels were categorized as: Poor (0–50), Moderately sufficient (50.1–66), Adequate (66.1–84), and Excellent (84.1–100). For statistical analysis, categories were merged into ‘Limited RHL’ (Poor + Moderately sufficient) and ‘Optimum RHL’ (Adequate + Excellent).
Data collection procedure
After obtaining ethical approval, eligible students were approached. Those who provided written informed consent received the questionnaires. Sampling continued until the target sample size was reached. Incomplete questionnaires were excluded and replaced (Figure 1).
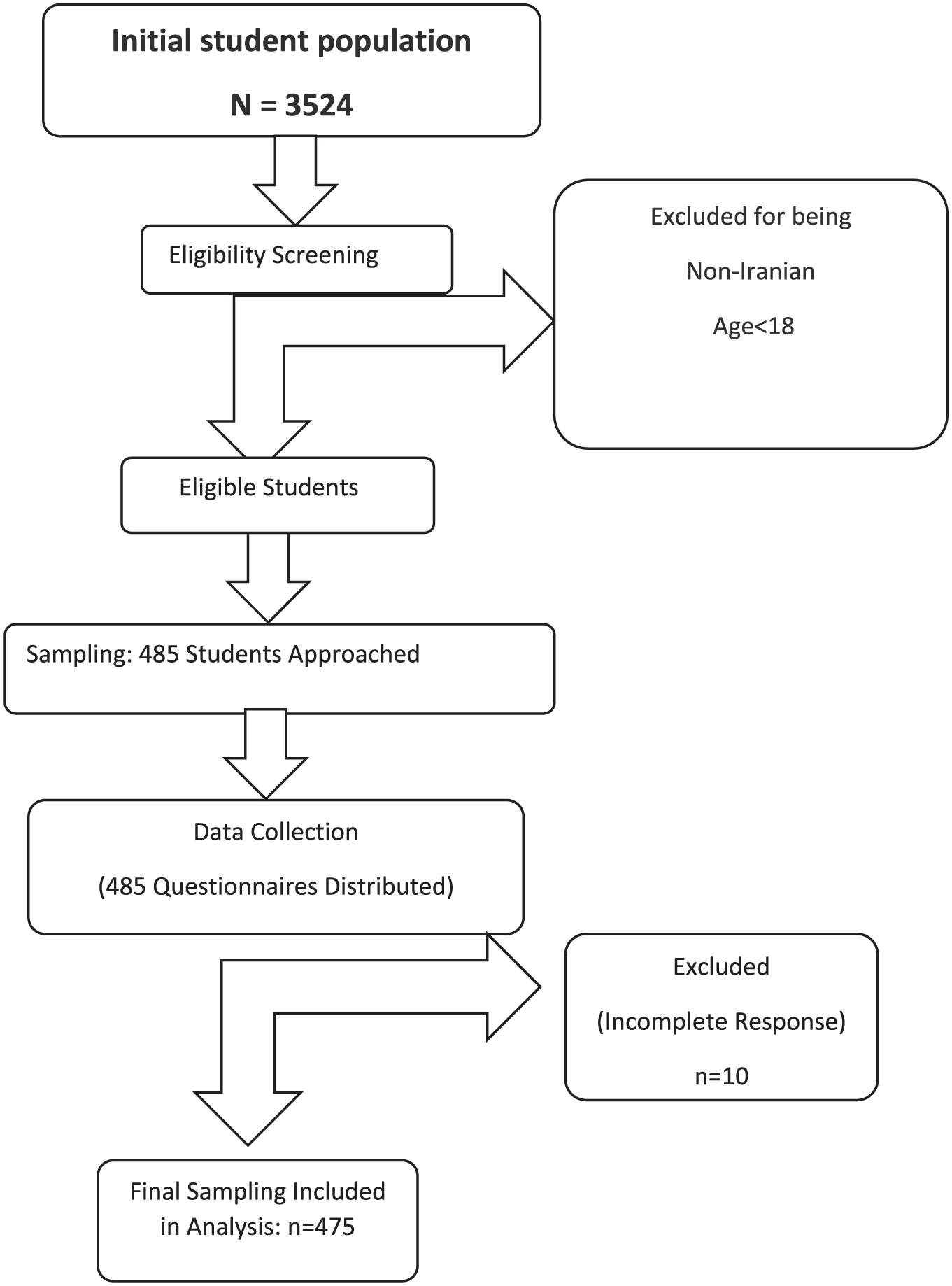
Study flow chart.
Statistical analysis
Data were analyzed using IBM SPSS Statistics (Version 24.0). Descriptive statistics (frequency, percentage, mean, standard deviation) were used to summarize sociodemographic characteristics and RHL scores. Independent t-tests and Analysis of Variance (ANOVA) were used to compare mean RHL scores across categorical variables. Post-hoc tests (Tukey HSD) were applied following significant ANOVA results to identify specific group differences. Effect sizes were calculated using Cohen’s *d* to determine the practical significance of findings, interpreted as small (d = 0.2), medium (d = 0.5), or large (d = 0.8). A p-value of less than 0.05 was considered statistically significant.
Ethics approval and consent to participate
The current study was approved by the Ethics Committee of Babol University of Medical Sciences, Babol, Iran (IR.MUBABOL.HRI.REC.1399.513). Written informed consent was obtained from all the participants. All methods were carried out in accordance with relevant guidelines and regulations and the Declaration of Helsinki
Results
Level of reproductive health literacy
The overall mean RHL score was 81.07 ± 12.9, which falls into the ‘Adequate’ category. Among the four dimensions of RHL, the highest mean score was in the ‘Understanding’ dimension (82.55 ± 16.11), and the lowest was in the ‘Evaluation’ dimension (79.75 ± 15.87; Table 1).
The status of reproductive health literacy and its dimensions among students.
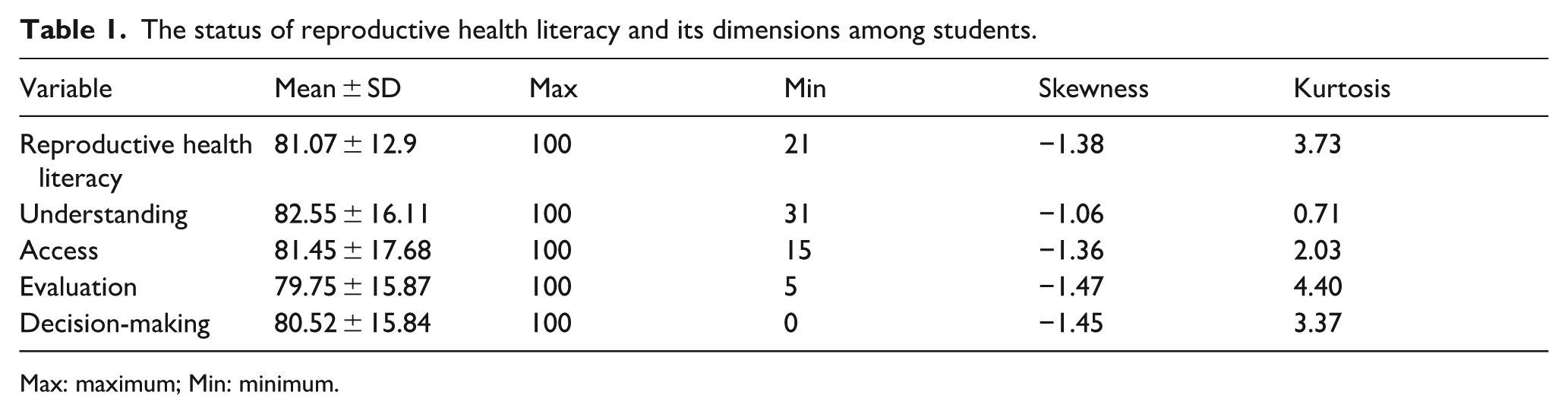
Max: maximum; Min: minimum.
Sociodemographic characteristics of participants
A total of 475 students completed the study. The majority were aged 20 years or older (66.3%, n = 315) and female (59.6%, n = 283). Most participants were single (85.5%, n = 406). The detailed distribution of all sociodemographic and academic characteristics is presented in Table 2.
Distribution of reproductive health literacy among students according to sociodemographic and educational characteristics.

B.Sc versus MD: d = 0.56 (Medium).
M.Sc versus MD: d = 0.87 (Large).
B.Sc versus M.Sc: d = 0.25 (Small)
First Year versus Second & Third Year: d = 0.27 (Small).
Second & Third Year versus Fourth Year & Above: d = 0.32 (Small).
Medical versus Nursing: d = 0.68 (Medium-to-Large).
Medical versus Paramedical: d = 0.82 (Large).
p-Value T test: between groups.
p-Value ANOVA test: between the first, second, and third groups.
Factors associated with reproductive health literacy
The results of bivariate analyses comparing RHL scores across different variables are presented in Table 2. Significant differences were found based on several factors:
Students aged 20 years or older had a significantly higher mean RHL score (82.52 ± 11.89) compared to those under 20 (78.20 ± 14.30), with a small-to-medium effect size (p = 0.001, d = 0.34). Female students had a significantly higher mean RHL score (82.51 ± 11.13) than male students (78.94 ± 14.93), with a small effect size (p = 0.003, d = 0.28). Married students scored significantly higher (88.79 ± 10.15) than single students (79.75 ± 12.87), with a large effect size (p < 0.001, d = 0.72). Students living at home had a significantly higher mean RHL score (82.77 ± 14.88) than those living in dormitories (79.97 ± 11.35), with a small effect size (p = 0.031, d = 0.21). A significant difference was observed across majors (p < 0.001). Post-hoc analysis revealed that medical students had significantly higher RHL scores than nursing students (86.69 vs 77.93, d = 0.68) and paramedical students (86.69 vs 76.48, d = 0.82). No significant difference was found between medical, dental, and midwifery students.
A significant difference was found across educational programs (p < 0.001). MD students had significantly higher scores than both B.Sc (d = 0.56) and M.Sc (d = 0.87) students.
A significant difference was observed (p = 0.005). Post-hoc tests indicated that fourth-year and above students had significantly higher scores than second- and third-year students (d = 0.32).
Furthermore, 86.7% (n = 412) of participants indicated that the optimal time for reproductive health education was during high school or before starting college.
Discussion
This study investigated the level of RHL and its influencing factors among students at Babol University of Medical Sciences. The findings reveal an overall adequate level of RHL, which is encouraging given the participants’ status as future healthcare professionals. This result was attributed to their education and knowledge of reproductive health, aligning with the findings of the present study. 14 However, in other studies with different research populations, RHL was not favorable.15–17 However, the study uncovered significant disparities linked to key demographic and academic variables, highlighting systemic inequities that require targeted intervention.
The association of higher RHL with older age aligns with cumulative learning theory, suggesting that knowledge accumulates with increased education and life experience.18–20 This is particularly relevant in a university setting, where students are continuously exposed to new information. The large effect size observed for marital status is a critical finding specific to the Iranian context. This can be largely attributed to the mandatory pre-marital counseling sessions in Iran, which include formal education on reproductive health.21,22 This policy appears to be effective and could serve as a model for structuring RHL interventions for the general youth population.
The significant gender gap, with female students demonstrating higher RHL, is consistent with global trends.6,23,24 This discrepancy can be explained through the lens of socio-ecological theory. In patriarchal societies like Iran, reproductive health is often erroneously perceived as a predominantly female domain.19,20 Cultural norms stigmatize male engagement in these topics, discouraging them from actively seeking information. This creates a feedback loop where lower initial knowledge leads to less engagement, further widening the gap. Our findings underscore an urgent need for culturally adaptive strategies that actively engage young men, perhaps by integrating RHL into general health or psychology courses marketed toward all genders.25–27 The low level of health literacy among males reflects their lower awareness of this area and highlights the inadequate knowledge of males in this matter.
In the present study, students living in the dormitory indicated lower RHL than students living out of the dormitory, which is consistent with the findings of Bagheri et al. 14
The most substantial disparities were academic. The significantly lower RHL scores among nursing and paramedical students, compared to medical students, point to a structural weakness in non-medical curricula. Medical curricula typically offer comprehensive modules on anatomy, sexual health, and preventative care. In contrast, nursing and paramedical programs might prioritize clinical skills and technical competencies, potentially at the expense of broader, preventative health education.28–32 This is supported by literature indicating that paramedical students receive scant training in sexual health counseling. 33 This curriculum gap is concerning as nurses and paramedics are often frontline providers who could play a pivotal role in patient education. A revision of these curricula to incorporate robust RHL components is strongly recommended.
Strengths and limitations of the study
A key strength of this study is its use of a validated instrument and a robust sampling method, enhancing the internal validity of the findings. The calculation of effect sizes provides a clear measure of the practical significance of each associated factor.
This study also has limitations. Its cross-sectional design prevents the establishment of causal relationships. The use of self-reported questionnaires introduces the potential for social desirability bias, particularly on a sensitive topic like reproductive health in a conservative setting. Furthermore, as the study was conducted in a single university, the generalizability of the findings to all medical students in Iran may be limited. Finally, while the tool was validated, some nuances of RHL in the specific cultural context might not be fully captured.
Conclusion
Overall, the level of RHL among medical sciences students at Babol University was satisfactory, but there were notable inequalities. Marital status, faculty of study, and gender were the strongest influential factors, with married, medical, and female students demonstrating superior RHL.
Based on these specific findings, we recommend: Integrate comprehensive, mandatory RHL modules into the core curricula of paramedical and nurse education programs to address the identified knowledge gap. Develop and implement school-based RHL education programs before university entry, as supported by the students’ own perceptions of the optimal timing for such education. Design and promote targeted RHL interventions aimed specifically at male students to counteract cultural stigmas and close the gender gap. Strengthen and potentially expand the scope of the existing pre-marital counseling program to include more comprehensive RHL topics.
Policymakers and educators should prioritize these culturally responsive, evidence-based strategies to ensure all future healthcare professionals are equipped with the necessary literacy to serve their communities and make informed decisions about their own health.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251399262 – Supplemental material for Reproductive health literacy and influencing factors among medical sciences students at Babol University of Medical Sciences, Babol, Iran
Supplemental material, sj-docx-1-phj-10.1177_22799036251399262 for Reproductive health literacy and influencing factors among medical sciences students at Babol University of Medical Sciences, Babol, Iran by Sanaz Bahrami-samani, Shabnam Omidvar and Vajihe Tahmasbpour in Journal of Public Health Research
Footnotes
Acknowledgements
We extend our sincere appreciation to the student research committee and the Research Vice-Chancellor of Babol University of Medical Sciences for approving the project. We thank all the students who participated in this study.
Ethical considerations
The current study was approved by Ethics Committee of Babol University of Medical Sciences, Babol, Iran (IR.MUBABOL.HRI.REC.1399.513). Written informed consent was taken from all the participants. All methods were carried out per relevant guidelines and regulations.
Consent to participate
Written informed consent was provided to all the participants. The study was conducted under the Declaration of Helsinki.
Author contributions
Shabnam Omidvar and Sanaz Bahrami-samani designed the study. Sanaz Bahrami-samani and Vajihe Tahmasbpour collected the data. Shabnam Omidvar supervised the study and did data analysis and interpretation, and drafted the manuscript. All the authors read and edited the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.