
Abstract
Background:
Globally diabetes affects over 530 million adults with Type II Diabetes (T2DM) accounting for approximately 98% of patients. T2DM is preventable, and its onset can be markedly postponed by increasing physical activity, reducing weight, and changing dietary habits, poor adherence to lifestyle modification was attributed to a number of factors such as poverty, and diet education. The main objective of this study was to explore factors affecting lifestyle modification among adults with type II diabetes mellitus at Mbale Regional Referral Hospital (MRRH)
Design and methods:
A descriptive cross-sectional study involving 262 participants was conducted in MRRH among T2DM patients attending the diabetic clinic. Quantitative data was collected through structured administered questionnaires. Simple random sampling was used to recruit respondents for the study. Quantitative data was analyzed at univariate, and bivariate levels using SPSS version 25. Qualitative data was analyzed using thematic analysis. Statistical significance was set at p-value of <0.05.
Results:
About 70.1% of the participants were females, 63.4% were above 50 years, and 29.7% of participants had high knowledge on T2DM. Most participants engaged in health practices like recommended diet, regular physical activity, body weight monitoring, blood sugar monitoring, and health checkups. Gender, religion, occupation, physical exercise, smoking, and weight management significantly affected lifestyle modifications. Qualitative results revealed three main themes namely, social support, health education, and having a conducive environment as promoters to lifestyle modification, while two main themes namely lack of social support and religious and cultural beliefs were the main barriers.
Conclusion:
Generally, participants had good knowledge on the lifestyle modifications of T2DM. Gender, religion, occupation, physical exercise, smoking, and weight management significantly affected lifestyle modifications. Social support, health education, and having a conducive environment were reported as promoters to lifestyle modification, while lack of social support and religious and cultural beliefs were the main barriers. It is recommended that health care workers should continuously educate the patients on the lifestyle modifications considering their financial status, and all other limiting factors. A holistic approach to lifestyle modifications needs to be taken in order to help reduce the complications associated with the condition.
Keywords
Introduction
Diabetes mellitus (DM) is a major worldwide healthcare concern due to its sharp increase in occurrence. DM affects people of all ages, socioeconomic backgrounds, and demographic subgroups in nearly every country on the planet. Although DM affects everyone on the earth, both its incidence and death rates are gradually rising, and its incidence is highest in Low to Middle Income Countries (LMICs).1,2 Many patients with diabetes are challenging to place into a single group, and determining a person’s type of diabetes typically depends on the conditions that were in place at that point of the diagnosis. Nonetheless, four main classifications of diabetes are generally accepted throughout a wide range of literary works, specifically: (1) Diabetes mellitus type 1 (autoimmune pancreatic β-cell destruction); (2) Type 2 diabetes mellitus (constant loss of pancreatic β-cell insulin secretion often within the framework of insulin resistance); (3) gestational diabetes mellitus, which was previously unknown and discovered during the second or third trimester of pregnancy; (4) other specific forms of diabetes, which result from different causes, including drug- or chemical-induced diabetes and monogenic diabetes syndromes, which include neonatal-diabetes and maturity-onset diabetes of the Young. 2
Type II diabetes mellitus is a chronic metabolic disease characterized by elevated levels of blood glucose usually in adults which occurs when the body becomes resistant to insulin, or doesn’t make enough insulin. T2DM reduces the body’s ability to utilize insulin leading to high glycemic levels; thus early diagnosis is important in the prevention of complications by getting regular checkups, and blood tests by health care provider.
Effective management of T2DM requires a holistic approach to lifestyle changes, including diet, physical activity, medication adherence, smoking cessation, blood pressure control, lipid management, and psychological well-being. The WHO describes a healthy lifestyle as a mode of living that reduces the risk of severe illness or early mortality.3,4 Poorly controlled T2DM may lead to significant systemic complications such as an increased risk for cardiovascular, neurological, renal, skin, muscular, and ocular-related disorders. T2DM also has a widespread impact that extends into psychological, social, and even financial wellbeing.5,6 Lifestyle changes and dietary patterns like regular physical exercise, weight management, diet control, smoking cessation are vital in management of T2DM by mitigating the long-term effects of diabetes. 7 The multidisciplinary approach to T2DM management involves an integrated plan of both medication treatment and lifestyle modification. Pharmacological therapy includes insulin treatment and oral hypoglycemic drugs such as metformin and sulfonylureas, whereas lifestyle modification includes a combination of a well-balanced diet that regulates carbohydrate intake and increased physical activity. 8
Diabetes approximately affects about 530 million adults globally with a prevalence of 10.5% among adults aged 20–79 years; with T2DM accounting for approximately 98% of patients diagnosed with diabetes although this proportion varies widely among countries. 9 In Uganda, the number of T2DM patients has been increasing over the years 10 with the central region having the highest occurrence. About 716,000 adults in Uganda had diabetes and about 89% of them are neither on medication, nor aware of their status so present to the health system with difficult complications. 11
Regular physical exercise like brisk walking, 2.5 h/week of moderate aerobic activity, or typically 30 min/day for 5 days/week help in weight loss, improves mental state of diabetic patients hence reducing complications associated with diabetes. 7 However Sedentary lifestyle like inactivity, television watching, sitting at work or social gatherings for long hours, increased mechanization, and driving have displaced physical activity. 12
Pharmacological management, diabetic self-management support and education, dietary therapy, physical exercise, counseling on smoking and alcohol cessation, and psychosocial care are crucial for diabetes management. 13 Education level, environmental factors, nature of work among others affect the lifestyle modification and practices like irregular exercise, smoking, alcoholism, and diet. 14 Lack of knowledge, negative attitude, and poor practice also affect diabetes prognosis and hasten the occurrence which is preventable with early recognition. 13
Poor adherence to lifestyle modifications is attributed to a number of factors such as poverty, diet education, dislike for recommended foods, illness, old age, bad influence from other patients among others with lack of money being the greatest contributor to the non-adherence to diet modification. 15 This leads to complications like: blindness, kidney failure, heart attack, stroke, non-traumatic lower limb amputation. 15
Diabetic Clinic of Mbale Regional Referral Hospital had over 400 adults in attendance, 70% of type II diabetes mellitus clients were either overweight or obese (HMIS Feb, Mar 2024). Some of the lifestyle modifications that were highly advocated for to the patients at the clinic included: good dietary habits, engaging in physical exercise and monitoring body weight, ceasing smoking, and alcohol intake. However, about 58% of the patients still had high blood sugar levels despite their adherence to anti diabetic medication as sampled in the months of February and March 2024. The main objective of this study was to explore factors affecting lifestyle modification among adults with type II diabetes mellitus at Mbale Regional Referral Hospital (MRRH)
Design and methods
Study design
A mixed study used in which a descriptive cross-sectional design for the quantitative component and a qualitative descriptive study was used to gain a deeper understanding of the promoters and barriers to lifestyle modification among adults with T2DM.
Study site and population
The study was carried out in MRRH, Mbale City. MRRH is located in Northern City Division, Mbale City. Mbale is about 220 km from Uganda’s capital Kampala and close to the border with Kenya. The health facility is situated in Eastern Uganda along Pallisa Road, half kilometer to Mbale city town. It serves as a major referral site for all the eastern health facilities covering districts neighboring Mbale city such as Mbale district, Budaka, Butaleja, Manafwa, Sironko, Bulambuli, and Bududa among others. The health facility has a bed capacity of approximately 300 and above in both maternity and general wards with a catchment population of about twenty-one thousand nine hundred nineteen (21,919) people. The hospital has various clinics such as outpatient, post-natal, ART clinic, maternity, outpatient departments, antenatal, maternity, general ward among others with many health workers. The study targeted adults with type II diabetes mellitus at MRRH. This area was chosen because of the increasing cases of diabetes mellitus especially type II of diabetes among adults at MRRH.
Inclusion criteria
The study recruited adults aged 18 years and above, and breastfeeding mothers with T2DM who had attended the diabetic clinic in MRRH for at least 6 months.
Exclusion Criteria
Pregnant mothers with gestational diabetes, and those who were mentally unwell and seriously ill.
Sample size calculation
The sample size was calculated basing on the Cochran’s formula, due to the large population given a desired level of precision, desired confidence level, and estimated proportion of the attribute present in the population.

Where, Z1 − α/22 is the standard normal variate (at 5% level of sig) = 1.96
n = sample size.
N = total population enrolled was 800.
P = expected proportion (prevalence) of factors affecting lifestyle modification among adults with type II diabetes mellitus in population at 0.5 The prevalence was not known so we made an assumption of 50% of factors affecting lifestyle modification among adults with DM2 which provides the largest possible sample size.
e = absolute error at 0.05.
Since the enrollment at the Diabetic clinic at MRRH was known (800) we used the formula for a finite population

Therefore, the sample size calculated was 260 respondents.
The sample size for the two focus group discussions was 24 participants.
Sampling technique
A simple random technique was used to get participants for quantitative data, and purposive sampling technique was used to get participants for focus group discussions.
Pretesting of the data collection tool
The questionnaire was distributed to 10 participants to evaluate understandability and applicability of the instrument 1 week prior to the data collection procedure. The amendments were made on the questionnaire in accordance to the participants’ responses. To ensure accuracy, completeness and consistency of data, the supervisors checked through the questionnaire. These participants involved in the pre testing with their results were not included in the final study.
One pretest focus group discussion was conducted to assess the length of the discussion. This was done 1 week prior to the data collection period.
Data collection
For quantitative data a questionnaire used which was developed by combining items from different research papers according to the objectives during literature review, it was then presented to adults with type 2 diabetes mellitus at MRRH to determine their practices to life style modification. Focus group discussions were conducted using an interview guide with open ended questions and probing statements for qualitative part. Data collected was used to determine the promoters and barriers to life style modification in adults with T2DM.
Ethical consideration
The study protocol was approved by the Busitema University Faculty of Health Sciences Research Ethics Committee, while administrative clearance to conduct the study was sought from Hospital Administration.
Written consent was obtained from study participants. Confidentiality of the information was assured, and privacy of each participant was maintained throughout data collection.
Participants were provided with written consent in English and translated copies in Luganda and English where the participant was not able write, a thumb print was provided. The consent form contained explanation of the significance of the study to the participant, description of the study procedures and details on right to refuse or withdrawal from the study at any time. Those who were willing to participate in the study were given a consent form to sign after all the above information was provided.
Data analysis and presentation
Quantitative data was analyzed in SPSS system version 25 data base and presented using descriptive and inferential statistics, while qualitative data was analyzed using the Braun and Clarkes thematic analysis which included familiarization with data, initial code generation, theme searching, review of themes, definition, and naming of the themes. Statistical significance was set at p-value of <0.05.
Results
Practices of lifestyle modification among adults with type II diabetes mellitus at MRRH.
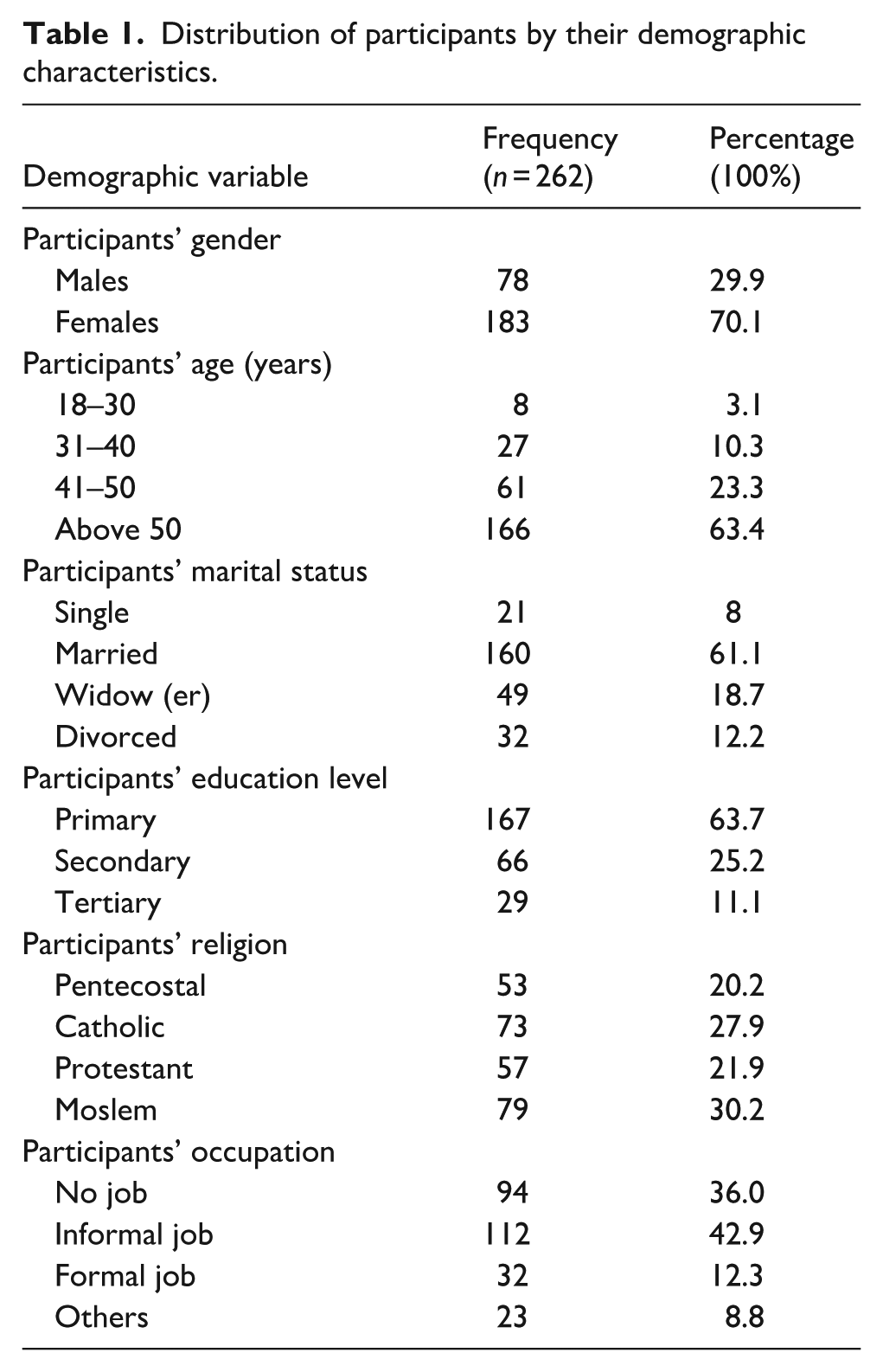
Table 1 above showed that most of the participants were females with a percentage of 70.1% and majority of the participants 63.4% were above 50 years.
Distribution of participants by their demographic characteristics.
Results in Table 2 revealed a mixed understanding of T2DM among the participants. A significant majority (75.6%) correctly identified increased blood sugar levels as the meaning of the disease.
Knowledge on type II DM.

Table 3 indicated that 77.5% of the participants had never attended a diabetic education program.
Other results on Knowledge of DM.

Based on the approximated scoring, participants knowledge was categorized as: high knowledge (12–17) points, moderate knowledge (8–11) points, and low knowledge (0–7) points, where 29.7% of participants had high knowledge, 44.7% moderate knowledge, and 25.6% low knowledge.
Table 4 indicated that most participants engaged in health practices like eating as recommended to prevent weight gain, regular physical activity, and monitoring body weight. However, fewer individuals regularly monitored their blood while attending health checkups showed even lower adherence
Analysis of practices of lifestyle modification.

Table 5 results indicated that demographic factors had a significant influence on practices among adults with type 2 diabetes mellitus, with gender, religion, occupation, physical exercise, smoking, and weight management standing out.
Relationship between demographics and practices.

Participants’ demographic data for focus group discussions
The study involved two focus group discussions of males and females separately with each group containing 8–12 participants. The focus group discussions involved out patients in the outpatient diabetic clinic in Mbale regional referral hospital. Most of the participants ranged from 40 to 60 years.
Promoters to lifestyle modification
In order to explore the promoters to lifestyle modification different aspects about lifestyle modification were asked like role of social support and health workers in lifestyle modification, how to incorporate physical exercise in the management of T2DM among others.
From Table 6, the promoters to lifestyle modification were grouped in different themes namely: social support, health education, and having a conducive environment.
showing promoters to lifestyle modification.

Theme 1: Social support
Social support is the care that one receives from other people in times of need. The availability of families, friends and support groups greatly enabled lifestyle modification among the T2DM patients.
Sub theme: Family support
Family support is very important in lifestyle modification among these patients.
The family members provide their support as listed in the codes through accompanying patients to do physical exercise, financial support by providing money for transport fares to the hospital, for buying recommended foods and machines like glucometers and blood pressure machines for regular checkups. These enabled the patients to modify and improve their life style as seen in the quotations below; They buy skipping ropes so that we skip together as they count the number of times I have skipped, some contributed some money and they opened for me a bank account where they deposited for me money so that I am able to buy food and whatever I want, Machines like glucometers that my son bought for me has helped in monitoring my health status hence enabling us to control the blood sugars,
Some participants reported that they needed to be escorted to the hospital since they lose memory and their family members know all about them as noted in the statement below; They should always bring us to hospital on the review dates since they know more about us and our illness as this disease sometimes makes us loose memory,
Subtheme: Friends’ involvement
Participants reported that their friends tell and give them recommended foods to eat, give them food in time and also listen to them effectively as stated below; My friends have helped me to manage diabetes by giving me food in time, always told me to eat a lot of green vegetables, smoked meat and boiled foods and accepted to follow my instructions as am taught by health workers about the kinds of food,
Subtheme: Support groups
Female patients were encouraged by women groups to follow health workers’ instructions and provided financial support to them as quoted in the statement below; The women groups have helped by encouraging us follow health workers instructions, taught us small businesses to enable us generate some money to help in the management of this condition. These groups have also provided some money inform of loans with little interest rates,
Theme 2: Health education
Through health education of patients, information on disease awareness, nutrition and diet and physical activity was created. This helped patients to modify their lifestyle.
Subtheme: Disease awareness
Health workers created awareness about the disease by carrying out health education sessions on some clinic days. This involved topics like complications, lifestyle modification, prevention and risk factors. The participants narrated as below: Educating me on the new lifestyle as a diabetic patient thus telling me the dos and don’ts. Educating me on how to manage other complications of diabetes and encouraging me to come to the hospital in case of any concern. Through Radios we get to be educated about diabetes and how our lives should change as diabetics,
Subtheme: Nutrition and diet
Knowledge on nutrition and diet was acquired through health educating the patients during some clinic days and this was noted from the participant’s statement below; We were educated by health workers about eating the right foods as diabetic patients like boiling food, eating a lot of vegetables and fruits and eating less energy giving foods,
Health care provider communication
Health workers provided the necessary care that they could, listened to patients’ concerns with empathy, encouraged patients and told them what health outcomes they expected. The health workers treat us well, listen to us, they tell us what to do and how our health status will be if we follow their instructions,
Subtheme: Physical activity
The patients are educated and advised to do exercise regularly and they confessed this below; Education from health workers that we should do exercise everyday like jumping around, doing house chores, even going to the garden,
Theme 3: Having a conducive environment
Some participants confessed that the availability of a conducive physical environment enabled them to do exercise hence modifying their lifestyle.
Subtheme: Safe place for physical activity
Those participants who had large compounds and those who could access to public fields were able to modify their lifestyle by doing physical activity. This was quoted in the participants’ statements below; I first run around my home very early in the morning before I go to the garden since my home has a large compound. After work in the evening, I skip my rope, Going to the field in the evening after work like cricket ground Mbale, park their cars and first do some exercises,
Table 7 showed barriers that affected lifestyle modification among adult type 11 diabetic patients in MRRH as grouped below.
Barriers to lifestyle modification.

Theme 1: Lack of social support
During analysis, lack of social support affected patients’ lifestyle modification through less family involvement.
Subtheme: Less family involvement
Some participants reported that their family members provided very little support for them and this hindered them from changing their lifestyle fully for a better life. This was mostly due to lack of money and fear of responsibilities. The participant’s statement below reflected this. Our family members and children should support us and avoid stressing us by reducing the size of the family like not bringing many grandchildren to stay with us yet we are given less support and money,
Theme 2: Religious and cultural beliefs
These beliefs have hindered lifestyle modification among diabetic patients though the following practices: fasting, dietary practices and traditional medicines.
Subtheme: Fasting
Some participants refused to stop fasting because they felt obligated to do so since they had to actively practice their religions like during the fasting periods as stated by a participant below; I am a moslem and I must fast even if I am diabetic, nothing will divert me from practicing my religion,
Subtheme: Dietary practices
Some participants have failed to follow the recommended dietary habits due to individual preferences and lack of money as confessed in the statement below; I do not have the money to buy the recommended foods, and not following health workers instructions concerning diet,
Subtheme: Traditional medicines
Use of herbal medicines was a barrier to lifestyle modification among some participants. They could only take these herbal medicines but they did not change their life accordingly and could not even come to hospital. This is seen in the participant’s statement below At first I was misled by the people who sell the herbs, I used to take a bottle of those herbs daily and I forgot the tablets not until my condition worsened that’s when I stopped using herbs and am much better now.
Discussion
The promoters to lifestyle modification were explored under the themes social support, health education and having a conducive environment.
Family support was adequate for some participants and this enabled them modify their life accordingly. The family members provided support like accompanying patients to do physical exercise, financial support, and provided recommended foods for the patients. This could be due to the positive attitude of the family members. Stanifer et al. 16 in Tanzania believed that family members helped prepare or encouraged healthy eating by changing the eating pattern of the whole family, and exercising together which resulted in a better lifestyle.
Friends were also of importance in encouraging and providing recommended foods to the patients and to supportively listen to them. This helped to overcome stigma among the patients and so enhanced lifestyle modification.
Community support groups encouraged patients to follow health workers’ instructions and provided financial support to them. This encouraged them to modify their lifestyle since they could at least afford to buy what they needed like the recommended foods. This was because through support groups patients gathered and were able to share their concerns. However contrarily, Mohamed Nor et al. 17 found out that the higher price of healthier foods affected patients’ ability in making consistent recommended dietary changes, including foods like: fruits, vegetables, unrefined rice, or bread than other foods.
Health workers played a great role in creating awareness about diabetes by carrying out health education sessions on some clinic days. This involved topics like complications of the disease, lifestyle modifications, prevention and risk factors, nutrition and diet among others hence empowering the patients with knowledge. Mohamed Nor et al. revealed that adequate knowledge is essential in the management of T2DM as it creates awareness to the patients living with the disease. Prior studies done in South Africa put it out that 56.3% of the respondents followed a controlled and planned diet and 91.3% practiced the intake of fruits and vegetables as part of their diet. 12 Nutrition education is essential in improving dietary habits and food choices, therefore conducting nutrition education increases nutrition knowledge, nutrition attitudes, and dietary habits among T2DM patients. Additionally, there is need for health workers coordinating in delivering the nutritional education to avoid fragmentation of information, as this also aligns with earlier studies about the same on building silos. 6
Participants who had large compounds and those who could access public fields had a conducive physical environment so were able to modify their lifestyle by doing physical activity at least daily. This was possible because they also allocated some time to go and do the physical exercises besides the conducive environment. However, studies have shown that there is a reduction in physical activity18–20 due to the replacement of playgrounds with buildings and over-reliance on motor transport. 18 Financial constraints also affect the rate of physical exercises as those who are well off routinely subscribe to gyms and invest in fitness equipment as opposed to those who are poor. This is in line with earlier studies which explored barriers to lifestyle modifications.2,4,5
Barriers hindering lifestyle modification in this study were grouped under two themes: lack of support, and religious and cultural beliefs. For lack of support, less family involvement was mentioned and this was due to factors like financial constraint, unshared responsibilities and inadequate household support. Participants reported that some family members were less concerned and or not involved in their wellbeing and were also burdened by their family members’ responsibilities. Furthermore, the family members provided less financial support as reported by the participants hence stressing them and leaving them with no option but not adequately adhere to lifestyle modification, like obtaining recommended foods. In support of this 20 revealed that social stress and depression, and lack of opportunities to improve health status were also identified as some of the factors contributing to the poor lifestyle modification. The marriage status and social stability of members also explains the reported barriers due to lack of autonomy in some families especially for the females. This aligns with earlier studies that explored various perceived barriers to lifestyle modifications and reported similar findings. 4 These findings are in line with earlier studies that showed that healthcare providers treating T2DM patients from unhealthy family environments may mistakenly attribute a lack of progress in dietary adherence to therapeutic failure, and therefore should instead, recognize the impact of family functionality in diabetic care and provide psychosocial support to improve dietary adherence. 21
Fasting led to poor lifestyle modification as some participants especially the men reported that they could not forego fasting because of diabetes since God is first then other things follow. This occurred mostly during the fasting periods. This was common among the Moslems who could not go through Ramadhan without fasting. This aligns with prior research where many patients believed that only God could cure diabetes mellitus and not their doctors or medicines. 22 Some participants revealed that they could not manage to live without their food preferences like spiced and sweet foods fatty foods like pork and taking alcohol. This was in line with my view where some diabetic patients were not able to have a meal without spices, sugary foods, fatty meat among others.
Participants explained that having a financial constraint hindered them from adhering to the healthy diet, and this concurred with Mohamed Nor et al. who stated in their study that the higher price of healthier foods affected patients’ ability in making consistent recommended dietary changes, including foods like: fruits, vegetables, unrefined rice, or bread than other foods. 17
Some patients were sometimes misled by herbalists who encouraged and advocated for the treatment of diabetes with herbal medicines yet this just worsened their health status. Herbalists generally gave wrong information to patients but this seemed so easy to implement than the health workers’ advice. In addition, the herbalists had a persuading language than health workers that made patients perceive it that, herbalists’ medicines and advice were far better than health workers’ advice.
Most of the participants engaged in health practices like eating healthily or as recommended to prevent weight gain. This was in line with the view that diabetic patients were always eager to know about their condition especially what they were supposed to feed on. Previous studies also mentioned that 56.3% of the respondents followed a controlled and planned diet and 91.3% practiced the intake of fruits and vegetables as part of their diet. 12 These findings resonate with earlier reports that emphasized personalized health communication during patient visits with providers being important to include in conversations about diabetes management, 5 which could explain the observed improved trends.
Most participants demonstrated good practice of lifestyle modification in terms of physical activity, weight management, not smoking, and not taking alcohol. (79%) agreed that they practiced regular physical activity and also (75.5%) spent at least 30 min on physical activity daily. This was consistent with other studies which revealed that 89.9% of the respondents engaged in some form of physical exercise, 12 and the greatest percentage (81.7%) of them had a duration of more than 30 min per session. In addition, these patients were involved in various activities and house chores throughout the day and this was generally physical activity. About 75.5% agreed to have been managing their weight, this was in line with another study which indicated that weight management is essential in glycemic control hence good outcomes, it further indicated that loss of 15% or more of bodyweight can have a disease-modifying effect in people with type 2 diabetes.
A significant portion of the participants demonstrated a poor practice to lifestyle modification in terms of blood sugar level monitoring in which only 48.1% agreed to have been checking their blood sugar regularly. This could be probably due to fear of their results since they practice less or no lifestyle modifications leading to no change in blood glucose levels. This aligned with prior research where participants felt demotivated to continue with lifestyle changes because they saw no benefit, particularly in terms of changes in blood glucose 17 as well as the challenges caused by poverty. 4 Overall, while many followed health practices related to diet and physical activity, adherence to health monitoring practices was less consistent.
The study revealed that gender, religion, and occupation significantly influenced specific lifestyle behaviors among adults with type 2 diabetes, highlighting the role of demographics in diabetes self-management.
Gender was significantly associated with spending at least 30 min on exercise (p = 0.014), indicating that men and women may have different levels of involvement in physical activity. Religion significantly correlated with regular blood sugar monitoring (p = 0.039), possibly reflected how religious beliefs impact health practices. In another study there was a misconception and popular belief reported that pricking the finger to monitor blood sugar could break the fast; hence some patients neglected to monitor their glucose levels during Ramadan. 22 There was a relationship between level of education and monitoring of the blood sugar levels (p = 0.01), this showed that participants in the study who had attained school could have high chances of monitoring their glucose levels, this was in line with a study which reported that people who had attained high levels of education had the ability to monitor their blood sugar levels. 23
Occupation status demonstrated relationship with the practices in patients with type II diabetes, this was in terms of health checks (p = 0.01), physical exercise (p = 0.041), smoking (p = 0.009), eating as recommended (p = 0.049), and weight monitoring (p = 0.009), this showed how employment affected most of the practices, this could be as a result of lack time in those employed and those not employed having some time to affect their practice in life style modification or even lack of resources in those not employed. Another study reported that self-employed men stood a risk of missing out on their out patient diabetic clinic appointments. 24 Just like it was earlier on noted in Qatar, 8 we emphasize that public health efforts should focus on reducing sedentary behaviors, while policies should improve access to physical activity opportunities for individuals with lower income and education.
Our results are in line with an earlier study by Alrasheeday et al., that reported on various barriers where, barriers to healthy eating and physical activity were perceived by 34.9% and 28% of patients, respectively. Personal and environmental barriers to healthy eating were perceived more frequently than social barriers (43.0% and 26.9%, respectively). Personal and environmental barriers to physical activity were perceived by 28.0% of patients, followed by social barriers (27.9%). The most frequently perceived barrier to healthy eating was a lack of motivation (61.6%), followed by insufficient information about healthy diets (32.2%). Regarding physical activity, a lack of motivation was the most frequently perceived personal barrier (32.0%), while a lack of a supportive work environment was the most frequently perceived social barrier (33.7%). 4
Limitations
The present study has several limitations. First, the study adopted a cross-sectional design that does not reflect the changes in perceived barriers over time. To gain a deeper understanding of these modifications, it is recommended to conduct longitudinal studies. Second, the study was health facility-based, possibly affecting the generalizability of its findings to the broader T2DM population in the community. Therefore, the study findings should be interpreted cautiously, and large-scale community-based studies are recommended. Third, the sampling strategy applied, especially for the qualitative arm, introduces the possibility of bias and may affect the representativeness of the sample. Finally, there were no participants aged below 40 years during the time of data collection for the focus group discussions, leading to missing out of information from this category of participants.
Conclusion
Generally, participants had good knowledge on the lifestyle modifications of T2DM. Gender, religion, occupation, physical exercise, smoking, and weight management significantly affected lifestyle modifications. Social support, health education, and having a conducive environment were reported as promoters to lifestyle modification, while lack of social support and religious and cultural beliefs were the main barriers. It is recommended that health care workers should continuously educate the patients on the lifestyle modifications considering their financial status, and all other limiting factors. A holistic approach to lifestyle modifications needs to be taken in order to help reduce the complications associated with the condition.
Significance for Public Health
The significance of this study is multifaceted, as it seeks to explore critical issues surrounding lifestyle modifications among patients with T2DM. The study provides valuable insights for policymakers and healthcare workers especially nurses and physicians working in diabetic clinics to be aware of the enlisted factors hence developing strategies to educate the patients based on the gaps identified. This could be at the hospital or in activities like community integrated outreaches to extend health education sessions on lifestyle modification to the patients’ vicinity. This is crucial for public health intervention that seeks to promote good well being among the specified patients group. Without this study, there would be an increasing number of complications or even death of these patients due to uncontrolled glycemic levels hence increasing cost of living, reducing the quality of life of the patients and their families at large.
Footnotes
Ethical considerations
This study was approved by Busitema university Faculty of Health science Research and Ethics Committee and REC number is BUFHS-2024-198.
Consent to participate
Participation in the study was voluntary and informed consent was got from all the participants.
Consent for publication
Not applicable.
Author contributions
This work was collaboratively carried out among all of the authors. MG, LN, RA, JE, JL, LVNS, YG, and RCN conceived, designed and supervised the study, analyzed the data and wrote the first draft of manuscript. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Raw data can be obtained from the corresponding author upon reasonable request.
Accordance statement
The authors confirm that all methods were performed in accordance with the relevant guidelines and regulations.