
Abstract
Objectives:
The study investigated the knowledge, prevalence of hypertension and associated factors among poor urban community dwellers in Ibadan, Nigeria.
Methods:
This was a cross-sectional study that explored non-communicable diseases using the modified World Health Organisation STEPwise approach to noncommunicable disease risk factor surveillance. Data was collected from 500 eligible participants aged 18–65 years from two urban communities in Ibadan, Nigeria. Knowledge was scored on 28-point score with ≤9 classified as poor, 10–19 as fair, and 20–28 as good. Data were analysed using Chi-square statistics and binary logistics regression at p < 0.05 level of significance.
Results:
Mean age of the respondents was 35.3 ± 12.2 years, most, (67.9%) of the male respondents were currently married, while most female were self-employed (72.8%) with secondary education (53.1%). Almost two-fifth, (16.2%) had good knowledge of hypertension which was associated with Christianity religion, earning more than #20,000 ($49) monthly and a history of obesity (p = 0.001). Hypertension prevalence was 18.6%, and only 8.4% were aware of their hypertensive status before the survey. Obesity was 14.6% among females and 3.0% among males. The majority of the females (87.0%) and 55.8% of males were physically inactive. More males (64.9%) than females (42.3%) consume alcohol. The logistic regression shows no significant association with the covariates.
Conclusion:
The study population has a low level of knowledge, high risky practices and a high prevalence of hypertension. There is a need for concerted health promotion interventions geared towards improving the knowledge and changing the behavioural practices of poor urban community members in southwestern Nigeria.
Introduction
Hypertension, a condition characterised by elevated blood pressure is a global health problem1,2 affecting an estimated 1 billion people globally and a little less than one third, (31%) of whom reside in sub-Saharan Africa. 3 This includes over 20 million in Nigeria 4 —the seventh most populous nation globally and the most populated in Africa.2,5 Several challenges to effective hypertension control efforts exist at policy, population and health systems levels in Africa including Nigeria.
Population-level factors such as low awareness rates, the widespread misconception about hypertension, poor care-seeking habits 6 and heavy reliance on traditional medicine or local concoctions. 7 In addition, many households are burdened with huge out-of-pocket health expenditure with only 5% of Nigerians covered by health care insurance. 8
Health systems factors such as poor translation of clinical guidelines into practice, 9 and a suboptimal number of skilled physicians 7 and dilapidated Primary Health Care infrastructure and outbreak of covid-19 further limiting access to quality care services including prompt hypertension screening for preventive, diagnostic and appropriate treatments, especially in poor urban and rural community settings. The condition contributes about 5278.4 per 100,000 age-standardised disability-adjusted life years (DALYs).6,10 Currently, in Africa, about 38% of adults are living with hypertension with 39.2% prevalence in urban and 37.5% in rural, 10 and only 12.5% of these cases are controlled. 10 A systematic review of studies in Nigeria showed that the crude prevalence of hypertension among adults was 30.6% in 2021 6 ; rising to 8.6%% in 1995 (4.3 million cases) to 32.5% (27.5 million people) in 2020. Furthermore, a study has shown that the annual cost of hypertension management per patient in Nigeria is N145,086.12($354.73) per hypertensive patient in Nigeria. 11 This reflects the urgent need for cost-effective interventions such as the mass implementation of a campaign on preventive strategies such as routine health screening, healthy diet, physical activity and alcohol smoking limitation and medication adherence to address the silent burden. Emphasis should also be placed on disease control measures such as encouraging prompt diagnosis and hypertension therapeutic compliance while genuine political will are needed to subsidise health expenditure through the provision of universal health insurance for Nigerians to address the financial burden.
Studies have shown that only 27.0% 6 and 29.0% 12 of hypertensives in Africa and Nigeria respectively are aware of their hypertension status which may predispose them to increased risk of complications, other diseases such as cardiovascular disorders including stroke, ischaemic heart disease, heart attack10,12 and death. 12
Studies have also shown that lifestyle (tobacco use, physical inactivity, alcohol intake, poor dietary habits) and living location (rural or urban settings) are modifiable risk factors for hypertension 13 while the genetic factors (parental genetic makeup) and sex of a person are the non-modifiable risks for the development of hypertensive conditions. 14
In Nigeria, only 2.8% of the reported 30.6% hypertensive had the ideal blood pressure in Nigeria. 9 Furthermore, the Nigerian health systems remain grossly under-staffed and ill-equipped to adequately address hypertension burden thus making it a critical threat to the productive age group in Nigeria.
Most interventions and services for hypertension are health facility-based rather than at the community level where preventive care can be a game-changer. Unsurprisingly, the prevention and management of hypertension in poor urban areas have not received sufficient attention 15 Thus, the need for the current study.
Many urban Nigerian studies usually fail to include a sizable proportion of poor urban neighbourhoods; this study focuses mainly on these underexplored settings.
It is hoped that the results presented will deepen understanding of the knowledge, practices, burden of hypertension and associated factors in poor urban community settings in South-western Nigeria.
Methods: Study setting and design
This was a cross-sectional study nested into a larger study that explored the knowledge, risk factors and preventive practices on non-communicable diseases (breast and cervical cancer, hypertension and diabetes) in selected communities. A community-based study was carried out among residents of two poor urban communities in Ibadan North Local Government Area, Oyo State, Nigeria between 14 November and 3 December 2018 at Aba Apata (Agbowo) and Inu Koko (Ashi) communities in Ibadan. Ibadan North Local Government consists of 12 political wards and the governance is based on the 1999 Nigerian constitution of governance. The LGA has a population of 856,988 people with 50.5% and 49.5% males and females who are mainly from the Yoruba ethnic group. The main occupation of the community is farming and trading and low-level government or self-employed workers. 16
Sampling size and sampling technique
The sample size for the study was calculated using the Leslie Kish sample size formula for cross-sectional studies 17 and a 42.1% prevalence of hypertension from a previous study in southwestern Nigeria, 2 at a 95% confidence level, 5% margin of error and a design effect of 1.5. Consequently, the final sample size was determined to be 374 and increased to 500 respondents to adjust for non-response, and to increase the precision and generalisation of the research. The participants consisted of 500 community members aged 18–65 years who were randomly selected from the total community population. A simple random sampling technique was used to select households. From each of the selected households, one participant was selected by ballot method.
Data collection instrument and measurement
Data were collected using the modified version of the WHO STEPS instrument and this has three sections: the socio-demographic profile, behavioural characteristics and physical measurements. The modified instrument was translated into the local language—Yoruba and back-translated into the English language by an expert to ensure accurate reporting of findings without loss of meaning. Validated (pretested) questionnaires were used to collect data through an electronic data capture tool (ODK Collect) which was interviewer-administered.
Blood pressure measurement was taken with the aid of an OMRON M2 (Model: HEM-7116-E; Company: Omron Corporation, Kyoto Head Office, Shiokoji Horikawa, Shimogyo-ku, Kyoto 600-8530; Country: Japan) automated Sphygmomanometer. The respondents were made to sit in a relaxed position for 5–10 min before the readings were taken. The appropriate cuff was placed on the left upper arm of the respondents depending on their body sizes. Three readings were taken from each respondent to ascertain the presence or absence of elevated blood pressure using the WHO standardised scale for Systolic blood pressure ≥140 mmHg and diastolic Blood pressure scale of ≥90 mmHg.
The height was measured using a graduated plastic heightometer (in metres to the nearest 0.5 cm). Height was measured in an upright position with the participant’s heel, shoulder and buttock touching the vertical board of the heightometer. The measurement value was recorded to the nearest centimetre. Weight was measured using a calibrated weight scale and participants wore light clothes without shoes and the reading was taken to the nearest 0.1 kg. Waist and hip circumference measurements were taken by making the respondents stand upright with their arms spread while the research data collector pull up a tape rule to measure the waist and hip ratio of the respondents the waist circumference was taken in between the iliac crest and lower rib while the hip ratio was taken at the intertrochanteric level.
Three (3) supervisors and eight trained doctoral students (research data collectors) were trained for 2 days in line with research ethics, data collection procedures and the contents of the instrument to increase the quality of our data. The data collection procedure and tools were pretested prior to actual data collection. Supportive supervision was carried out by the supervisors daily during the data collection period.
The knowledge of hypertension was calculated by assigning one mark to each correct response while a negative response was a zero score. The study made use of a 24-item questionnaire to assess, awareness, and knowledge of hypertension risk factors and preventive practices. The overall score was determined using a 28-point score with ≤9 classified as poor, 10–19 as fair and 20–28 as good knowledge of hypertension. Physical activity level was determined using the physical activity guidelines of the World Health Organisation (WHO) for adults specifying 150 min of vigorous intensity physical activity or 300 min per week of moderate intensity aerobic physical activity. 18 This was categorised as a dichotomous variable with two responses “active” and “in-active.” Other practices assessed were consumption of an alcoholic drink in the past 12 months (“Yes” or “No”), current tobacco and alcohol use (“Yes” or “No”).
Hypertension was classified as a systolic/diastolic blood pressure of ≥140/90 mmHg. Stage 1: SBP = 140–159 mmHg; Diastolic BP = 90–99 mmHg; Stage 2: SBP ≥ 160 mmHg; Diastolic B > 100 mmHg, 19 the body mass index was measured by calculating the weight divided by the height in metres m2 (weight (kg)/(height (m) × height (m)). Waist-to-hip ratio (WHR) was calculated as waist (cm) divided by the hip in centimetre. 20
Data analysis techniques
The collected data was exported to SPSS version 21.0 for analysis. Association between socio-demographic factors and hypertension was determined using the chi-square tests statistics and binary regression models at p = 0.05 level of significance.
Ethical consideration
Ethical approval was sought from the University of Ibadan/University College Hospital Ethical Review Committee; Nigeria and the reference number is UI/EC/17/0410. Written consents were obtained from all the participants after they had been thoroughly informed on the study including the consent to publish the findings.
Results
Demographic profile of the respondents
The mean age of the respondent was 35.3 ± 12.2 years. More than half, (55.8%) of the females and half, (50.3%) of the males fall within the adult age group distribution. More than two third, (62.6%) of the females’ respondents were currently married compared to the males (67.3%).
Almost an equal proportion of both the male and female respondents were self-employed (72.5%) and 72.8% respectively. Almost half, (45.0%) and (45.6%) of the female and male respondents respectively completed secondary education as the highest educational qualification.
The ethnicity of the respondent showed that more than four-fifth or, (88.7%) of the females and (89.1%) of males were of the Yoruba ethnic group (See Table 1 for details).
Socio-demographic characteristics of study participants.

Mean Years risiding in community = 11.4 ± 11.6, Median = 7.0 years, Minimum = 0, Maximum = 65 years. Mean income = 19,714 ± 22.975 ($48.2 ± 0.2), Median = #10,000 ($24.5), Minimum = #0, Maximum = #200,000 or ($484.99). Mean Household size = 4.0 ± 1.8, Median = 4 people, Minimum = 1, Maximum = 10 people.
Others = Akwa = 3 (0.6%), Benue 1 (0.2%), Cross rivers 6 (1.2%), Delta 2 (0.4%), Edo7 (1.4%), Ibibio 1 (0.2%), Kogi 3 (0.6%), non-Nigerian 1 (0.4%), Tapa 1 (0.2%).
Socioeconomic characteristics of the respondents
The mean household size was 4.0 people. The average year of residence in the community is 11.4 ± 11.6, with a median = 7.0 years and a range of 0–65 years.
More than two-third, (68.3%) of the female and a little above half, (59.9%) of the male respondents have lived in the community for less than 10 years. A little above one-tenth, (14.2%) of the female respondents and almost two-fifth, (17.0%) of the male respondents have lived in the community between 11 and 20 years.
The proportion of female respondents found to be earning #20,000 ($49) or less per month was higher than male population with 73.7% of females compared to 51.7% of males. The mean monthly income was 19,714 ± 22,975, or ($48.2 ± 56.2) a median of #10,000 ($24.5; See Table 1 for details).
Knowledge of hypertension causative factors
Less than one-third, (31.4%) of the respondents knew that a family history of cardiovascular disorder and being over 40 years (36.4%) increased the risk for hypertension. Other risk factors identified include; being overweight (39.0%), eating salty food (40.2%), overeating (32.0%) old age, (35.2%), stress (75.4%), lack of exercise 36.6%), smoking (52.0%) and alcohol use (52.2%; See Table 2 for details).
Knowledge of hypertension causative factors.
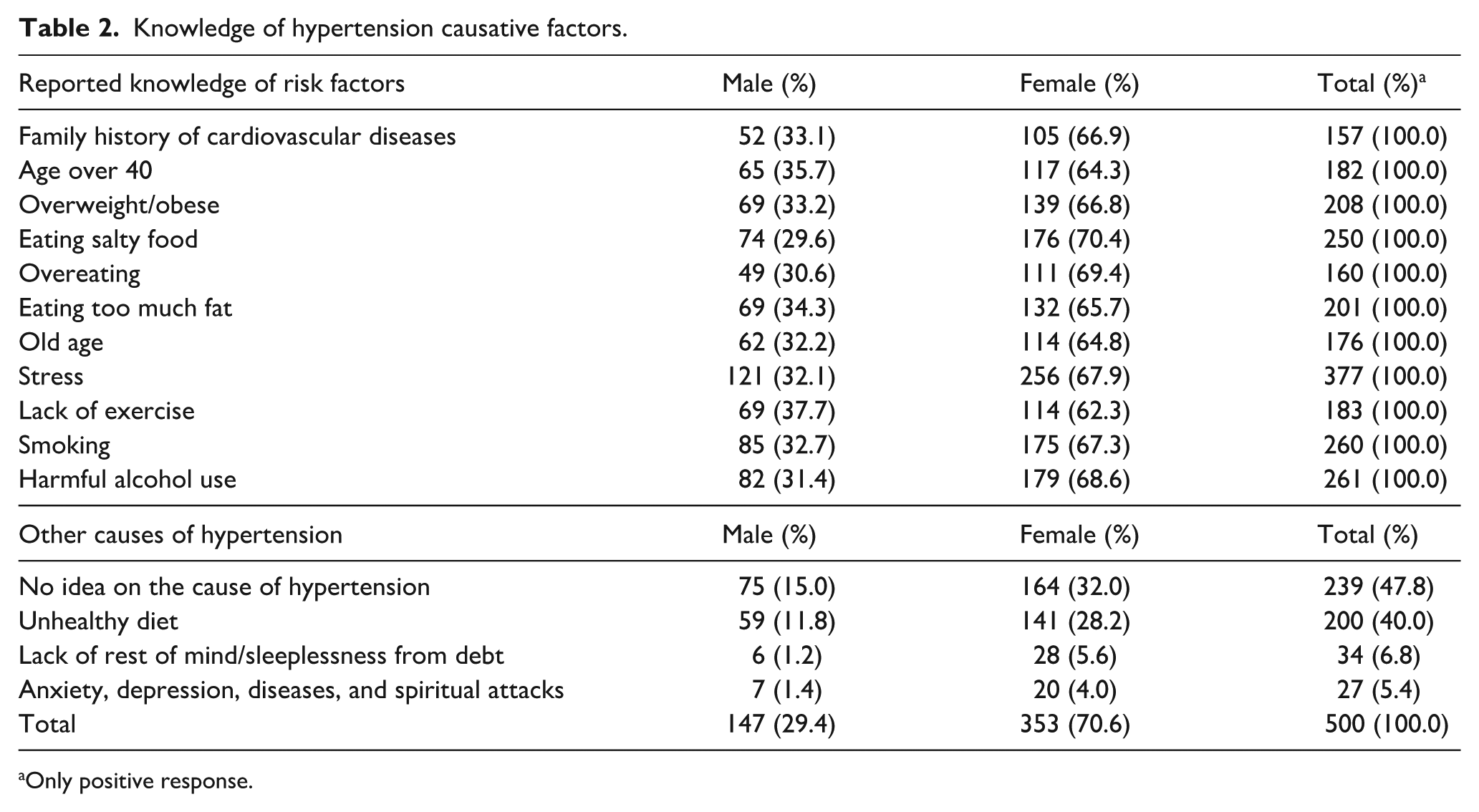
Only positive response.
Responses from open-ended questions on the risk factors for hypertension include, an unhealthy diet (40.0%), lack of rest/sleeplessness (6.8%) and a few (5.4%) attributed it to spiritual attacks (See Table 2 for details).
The mean knowledge score of hypertension among the respondent was 13.0 ± 6.5 with a median of 14.0 and a range of 2–14 points. More than half (51.4%) of the respondent had fair knowledge some, 32.4% had poor knowledge while only a few, 16.2% had good knowledge of hypertension (See Figure 1 for details).

Overall knowledge of hypertension among the respondents.
Respondents’ lifestyle practices, anthropometric and blood pressure measurements
In respect of levels of physical activity, more females (87.0%) than males (55.8%) were physically inactive (See Table 3 for details). Overall, 45.6% of female respondents reportedly consumed alcohol 12 months prior to the survey which was lower than the male population of whom 75.3% reported alcohol consumption. More than half (51.7%) of male respondents compared to none of the females consumed tobacco products, while more 64.9% of the males compared with 42.6% of females reported current alcohol intake (See Table 3 for details).
Respondents’ lifestyle practices, anthropometric and blood pressure measurements.

Positive response.
The BMI showed that among the females, more than two-third, (63.8%) fall within the normal BMI range (≤25), (27.3%) were overweight while few, (14.6%) were obese. In comparison, more than two-thirds of males or 79.1% were within normal range BMI range (≤25), 27.3% were overweight, and 3.0% obese. Nearly equal proportions of females (56.7%) and males (55.8%) were non-obese. The outcome of blood pressure measurement revealed that more than four-fifth (85.6%) and (86.4%) of the female and male respondents respectively had normal systolic blood pressure while over one-tenth, (10.8%) each had stage 1 systolic hypertension and 4.0% and 2.7% had stage II systolic hypertension respectively.
Furthermore, on diastolic blood pressure, more than four-fifth of females (83.0%) and male (86.8%) had a normal diastolic blood pressure; 11.0% and 6.9% had stage 1 diastolic hypertension, and 6.1% and 6.3% had stage 2 diastolic hypertension respectively (See Table 3 for details).
Hypertension related management
Almost one-tenth (8.4%) of the respondents were aware of their hypertension status, (71.4%) were diagnosed in the past 12 months (see Figure 2).
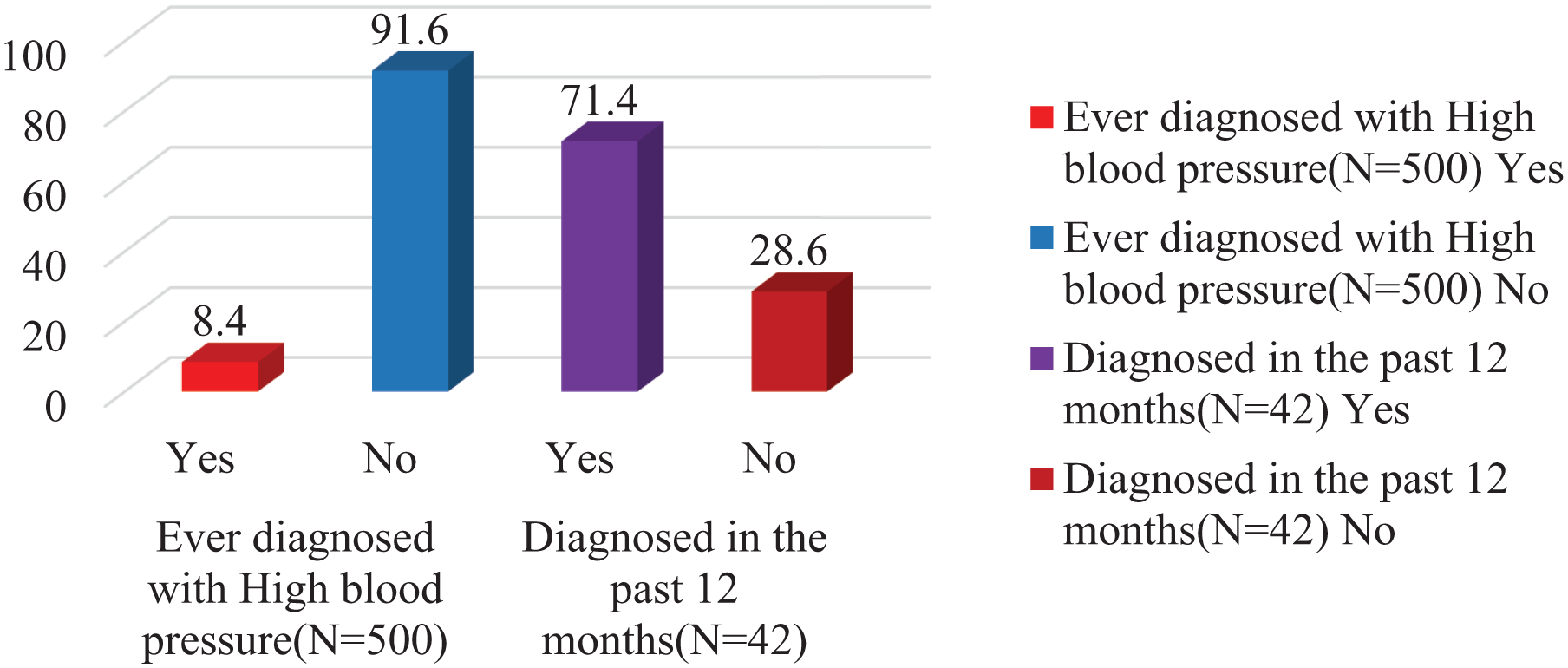
Hypertension status among respondents.
The adopted hypertension management technique by those aware of their hypertensive status includes, compliance with prescribed medicine (99.9%), controlling weight (33.3%), cutting down salt (33.3%), exercising to lower blood pressure (16.7%) and self-blood pressure measurement (6.6%). However, none of the respondents stated that they reducing consumption could help limit hypertension risks (100.0; See Table 4 for details).
Reported hypertension management technique.

Blood pressure (BP; mmHg) Mean systolic Blood pressure (SD) = 121 ± 18.1, Median = 119. Mean diastolic Blood pressure (SD) = 78 ± 12.9, Median = 76.
Mean BMI = 24.2 ± 5.4, Median = 23, Minimum = 14, Maximum = 58.
Test of association of hypertension knowledge and sociodemographic profiles
More than two third, (60.5%) of the respondents who fall within the adult age group had good knowledge of hypertension compared to few, (18.5%) of the respondents who are youths. The association between the knowledge and age of the respondents was found to be statistically insignificant [p > 0.001] (See Table 5 for details).
Categorisation of respondent’s knowledge by sociodemographic characteristics.

Significant at (p = 0.05) chi-square test statistics were used.
The association between the knowledge and the sex of the respondents was found to be statistically insignificant [p > 0.001] (See Table 5 for details). The association between knowledge and educational level of the respondents was found to be statistically significant that is, [p < 0.001] as (37.0% of the respondents with a college education had good knowledge of hypertension compared with those without formal schooling (8.6%) See Table 5 for details.
Regarding ethnicity, 86.4% of the respondents who were of the Yoruba ethnic group had good knowledge of hypertension compared to 6.2% of those who were of the other ethnic groups. The association between the knowledge and the ethnicity of the respondents was found to be statistically insignificant that is, [p > 0.01].
More than half, (54.3%) of the respondents who are of the Christian faith had good knowledge of hypertension compared to less than half, (45.7%) of the respondent who were Muslims. The association between the knowledge and religion of the respondents was found to be statistically significant, p < 0.001 (See Table 5 for details).
Nearly two-third, (63.0%) of the respondents who had lived within the community for less than 10 years had good knowledge of hypertension prevention compared to a few, (4.9%) of the respondents who had lived for more than 30 years in the communities. The association between the knowledge and years of residence among the respondents was found to be statistically insignificant [p > 0.001] (See Table 5 for details).
More than half, (51.9%) of the respondents, who earn #20,000 or less had good knowledge of hypertension and only few, (2.5%) of those who earn no income at all had good knowledge. The association between the knowledge and the income level of the respondents was found to be statistically significant [p < 0.001] (See Table 5 for details).
More than half or, (57.5%) of the respondents with a BMI of less than 25 had good knowledge of hypertension compared to the few or, 13.7% of the respondents who had a BMI of more than 30. The association between the knowledge and the BMI levels of the respondents was found to be statistically insignificant [p > 0.001] (See Table 5 for details).
An equal proportion, or 50.0% of the respondents who went for a blood pressure check-up in the past 12 months and those who had not had their blood pressure checked in the past 12 months had good knowledge. The association between the knowledge and the blood pressure assessments among the respondents was found to be statistically insignificant [p > 0.001] (See Table 5 for details).
Test of association of respondents’ awareness of previous hypertension status by socio demographic characteristics
Middle-aged respondents had the highest proportion of those with hypertension 64.3% being. Adults and adolescents had much lower proportions with 33.3% and 2.4% respectively. The association between prior awareness of hypertension status and age of the respondents was found to be statistically significant [p < 0.001] See Table 6 for details.
Categorisation of respondents’ awareness of previous status with hypertension by socio-demographic characteristics.
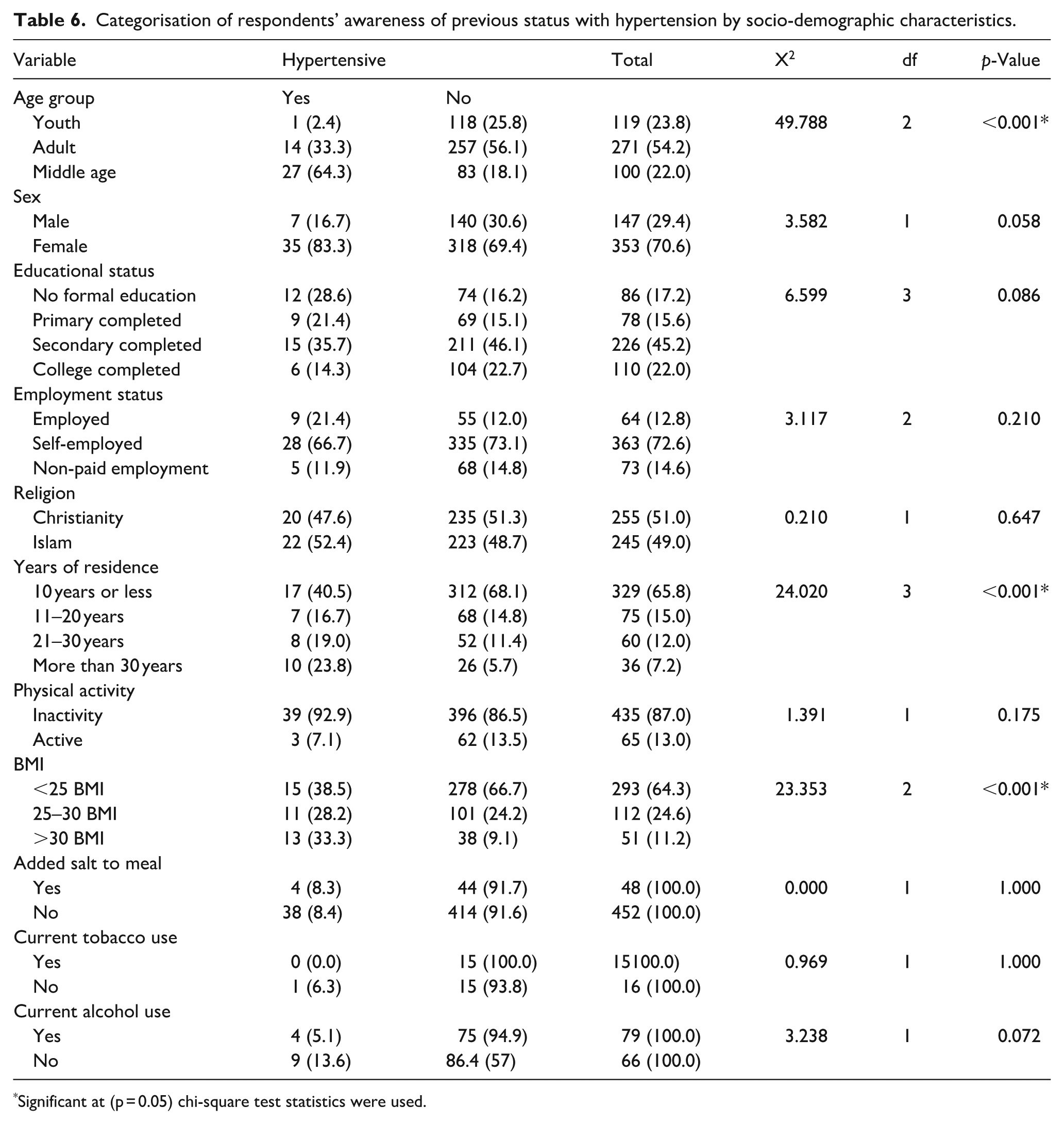
Significant at (p = 0.05) chi-square test statistics were used.
More than four-fifth, (83.3%) of the females compared to few, (16.7%) of the male respondents have been previously diagnosed with hypertension. The association between awareness of hypertension status and sex of respondents was found to be statistically insignificant [p > 0.001] (See Table 6 for details).
A little more than one third, (35.7%) of those who completed secondary education, few (28.6%) with no formal education, (21.4%) of who completed primary education and (14.3%) who completed college education respectively had prior knowledge of their hypertension status. The association between the prior awareness of hypertension status and educational status of the respondents was found to be statistically insignificant [p > 0.001] (See Table 6 for details).
Roughly two third, (66.7%) of self-employed, less than one third, (21.4%) of the respondents in paid sectors and (11.9%) un-employed respondents respectively had been previously diagnosed with hypertension. The association between the prior awareness of hypertension status and respondents’ employment status was found to be statistically insignificant [p > 0.001] (See Table 6 for details).
More than half or52.4%—Muslim and 47.6% Christian respondents had been previously diagnosed with hypertension. The association between the prior awareness of hypertension status and religion of the respondents was found to be statistically insignificant [p > 0.001] See Table 6 for details.
More, (40.5%) of the respondents who had resided in the community for about 10 years or less, 23.8% who had resided in the community for over 30 years, some, (19.0%) who had resided in the community for 21–30 years and (16.7%) who had resided in the community for 11–20 years respectively are aware of their hypertension status. The association between the prior hypertension status and years of residence in the community was found to be statistically significant [p < 0.001] (See Table 6 for details).
Almost all or 92.9% of the respondents who are physically inactive compared to few, (7.1%) of those who are physically active were aware of their hypertension status The association between the prior knowledge of hypertension status and level of physical activity was found to be statistically insignificant [p > 0.001] (See Table 6 for details).
More, (38.5%) of the respondents who had normal BMI (18.5–24.9 BMI), 33.3% of obese (>30 BMI) and 28.2% of overweight (25–29.5 BMI). About (6.2%) of the respondents who are self-employed. The association between prior awareness of hypertension status and the obesity levels among the respondents was found to be statistically significant [p < 0.001] (See Table 6 for details).
Less than one-tenth, (8.3%) of those who added salt to their meal have prior awareness of their hypertension status. The association between the prior awareness of hypertension and addition of salt while at the table was found to be statistically insignificant [p > 0.001].
Few, (5.1%) of those who currently use alcohol were aware of their hypertension status prior to the study. The association between the prior awareness of hypertension and current alcohol use was found to be statistically insignificant [p > 0.001] (See Table 6 for details).
Table 7 shows the logistic regression analysis used to determine the magnitude of the relationship between the respondent’s demographic profile and hypertension status. The model showed that hypertension status was not associated with age, as respondents who are aged 26–45 years and those aged 46–65 years were more likely to have been diagnosed with hypertension (OR = 5895.5; CI = 219.02–18,203, p > 0.05) and (OR = 1.023; CI = 0.827–2.286, p > 0.05) or [p > 0.001] respectively compared to those aged 18–25 years.
Binary logistic regression of the relationship between Hypertension and covariates factors.

Reference category.
p < 0.05 (Binary logistic analysis was used).
The model showed that obesity was not a predictor of hypertension status though overweight and obese respondents were more likely to be diagnosed with hypertension (OR = 0.949; CI = 1.398–4.048, p > 0.05) and OR = 1.014; CI = 1.287–9.917, p > 0.05) or [p > 0.001] respectively compared to respondents with a normal body mass index. The model showed that years of residence in the community were a predictor of hypertension status. Respondents who had resided in the community for 11–20 years (OR = 2.949; CI = 1.144–3.140, p < 0.05) were likely to be hypertensive. Intake of an alcoholic drink in the past 12 months was also not significantly associated with hypertension (OR = 1.148; CI = 1.236–5.459, p > 0.05) or [p > 0.001] (See Table 7 for details).
Discussion
In this study, less than one-tenth has ever conducted blood pressure self-assessment before the study. Hence, possession of digital blood pressure assessment tool coupled with timely training on usage is recommended to increase awareness and health seeking behaviour. This finding suggests that, low level of awareness on hypertension screening, testing and prompt management may be a key factor driving the disease prevalence among the urban population.
Most Nigerian population do not have access to behavioural change communication material such as leaflets and posters on warning signs of hypertension, and this is compounded with low self-efficacy on conducting blood pressure self-examination. 21 The mean income of the respondent was #19.714 ± 22.975 ($48.2 ± 0.2), which is similar to that of the study conducted in Nigeria where most participants were low-income earners. 22
The prevalence of hypertension in this study was 18.6% which is similar to that of a study conducted among urban residents in Nigeria 10 but lower than that reported in the general population 6 thus indicating the worrisome trajectory of hypertension among urban population groups. Studies have shown that, unhealthy dietary habits, sedentary behaviour and increased environmental life stressor in urban community settings further predisposed the population to cardiovascular diseases. 6
The study identified moderate stage 1 systolic hypertension among the respondents (10.8%), which is lower than the value seen in national surveys, 2 hence, this could provide a unique opportunity for management and reduced blood pressure using appropriate community-directed lifestyle intervention. 23
All of the respondent wrongly stated that limiting alcohol use could not prevent hypertension hence, the need for timely behavioural change communication intervention in print, radio and televised jingles on hypertension risk factors and correct the misconceptions. This findings points to the urgency for a comprehensive national alcohol control policy with enhanced awareness on the consumption health risks.24,25
The study showed that only two-fifth (16.2%) have good knowledge, thus pointing to a poor understanding of the causative risk factors, wrong attribution of hypertension to spiritual attack and sleeplessness due to huge debts. These findings point to the need for tailoring hypertension related information to the most accessible communication medium available to the urban-poor dwellers towards attaining optimal hypertension control.
The above finding is similar but lower in value to that of a study conducted in urban area of Kogi State, Nigeria where only 23.6% had good knowledge of hypertension Almost half of the respondent’s suggested prayer as a preventive strategy, 23 where many of the respondents believed the disease is caused by a spiritual attack 2 and could be cured by native drugs and spiritual prayers. 26 These findings suggest a huge knowledge deficit among some of the respondents who sometimes wrongly interpret the signs, symptoms and preventive factors for hypertension thus requiring immediate intervention in other to address the growing burden of the silent killer disease in the country.
In this study, over two-fifth of the respondents were obese, most were physically inactive and currently consume alcoholic drinks which are risk factors for hypertension development. These findings are in congruence to that of a Nigerian study 27 conducted in similar settings hence, pointing to poor lifestyle behaviour as significant risk factor for hypertension development. Furthermore, most urban community members are more likely to be physically inactive due to increased motorisation of several activities hence the likelihood of being obese. 27
Significant factors associated with hypertension were; advanced age, being overweight/obese, and residents more than 30 years in the community. This is similar to that of another Nigerian study. 4 This finding could be because hypertension increases with advanced age, increased consumption of junks and unhealthy meals which are very prevalent in urban settings where processed foods with high salt and lipid content consumption are associated with affluence.
In this study, more male had hypertension compared to females which could be attributed to the higher prevalence of lifestyle risk factors such as smoking, binge alcohol consumption among men. Furthermore, most men have poorer health seeking behaviour compared to their female counterparts.28,29 Alcohol consumption reduction interventions such as “sin taxation” and discouraging intake in younger adults while promoting healthy lifestyle behaviours may prove very vital to reducing the incidence and prevalence of hypertension in Nigerian urban settings.
This study revealed a deep routed misconception in spiritual causes of hypertension hence the need to campaign on medication compliance to reduce the endless search for local and traditional treatments for hypertension. Such efforts should be complimented with increased recruitment and posting of skilled cardiovascular experts to poor urban communities, co-opting traditional leaders in hypertension mobilisation and awareness creation campaigns including provision of policy framework for expanded health insurance coverage to mitigate the economic stress of hypertension and encourage positive health seeking behaviour. There is an urgent need for renewed political will for community mobilisation on dietary and nutritional education and risk minimisation approach such as alcohol limitation and physical exercise to serve as a key preventive measure
Furthermore, there is a need for a routine community training with support from philanthropists and government agencies in funding such programmes at the community levels.
Limitation of the study
The study is limited by the close-ended nature of the majority of the questions hence our ability to fully investigate factors influencing their knowledge and lifestyle factors could have been limited. Secondly, the findings of this study does not points to the entire urban poor communities in the entire Nigeria but represent a state in a south-western geopolitical zone. Future studies should look at adopting qualitative approach and larger geo-political state representation to deepen understanding of the socio-cultural and environmental context and how these influence their lifestyle, However, the study points to the rising burden of hypertension among poor urban dwellers in Ibadan which may be a reflection of the situation in the nation.
Conclusion
In conclusion, there is a high prevalence of hypertension among urban poor dwellers in Ibadan with about 1 in every 20 hypertensives, hence, an affordable health-care package should be designed towards reducing the disease burden among marginalised population withlimited access to affordable care. The government, civil society organisation and philanthropist should invest in cost-effective innovation that addresses the hypertension risk factors, promote periodic community testing and encourage self-testing to stem the burden of hypertension in Ibadan, Nigeria.
Furthermore, there is a need to strengthen the primary health care settings for hypertension surveillance, timely diagnosis, prevention and control measures. The primary health care centres are within the reach of 85% of the Nigerian population hence, vital to sustain any non-communicable disease prevention initiative in Nigeria. There is a need to encourage adopting healthy behaviour such as exercise, smoking cessation, alcohol reduction and healthy food consumption to reverse the growing unhealthy lifestyle among the poor urban dwellers in southwestern Nigeria. Finally, in the phase of diminishing resources and global intervention funding fatigue, investing in early hypertension detection, prevention and control efforts including cost-saving lifestyle modification approaches remain central to addressing non-communicable disease burden in Nigeria.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251395255 – Supplemental material for Knowledge, practices and prevalence of hypertension among poor urban community dwellers in Ibadan, South-Western Nigeria
Supplemental material, sj-docx-1-phj-10.1177_22799036251395255 for Knowledge, practices and prevalence of hypertension among poor urban community dwellers in Ibadan, South-Western Nigeria by Segun Emmanuel Ibitoye, Mojisola Oluwasanu, Yetunde John-Akinola and Oladimeji Oladepo in Journal of Public Health Research
Footnotes
Acknowledgements
We appreciate the research assistants and participants who participated in the study.
Ethical considerations
Ethical approval was obtained from the University of Ibadan/University College Hospital Ethical Review Committee; Nigeria and the reference number is UI/EC/17/0410.
Consent to participate
Written consents were obtained from all the participants after they had been thoroughly informed on the study including the consent to publish the findings.
Author contributions
Oladimeji Oladepo, Mojisola Morenike Oluwasanu and author Yetunde John Akinola conceptualised the research and study protocol. Ibitoye Segun Emmanuel analysed the data, interpreted and led the developed of the manuscript with review by all authors. All authors read and approved the final manuscript for submission to the journal. OO is the principal investigator and study tool design, data collection; supervision and management processes were anchored by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Authors declare that, this research was supported by a planning grant awarded by the U.S. National Institutes of Health, Fogarty International Centre, “Addressing NCDs In Nigeria Through Enhanced International Partnership and Interdisciplinary Research Training,” award number 1D71TW010876-01. The funding body had no role in the design of the study, collection of data, analysis, interpretation of data and manuscript writing.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors are knowledgeable about and conform with the Conflict of Interest Policy of the Journal and they all declare they have no competing interest.
Supplemental material
Attached questionnaire document.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.