
Abstract
Background:
Oral health significantly affects the overall well-being of the elderly, influencing nutrition, communication, and quality of life. Poor oral hygiene can cause infections and dental issues. In Thailand, promoting oral hygiene among the aging population remains a pressing and ongoing public health challenge.
Design and methods:
This study explores the factors influencing oral health care behaviors among elderly individuals at the Phitsanulok Health Center (Buddhachinaraj Hospital) as a case study of lower Northern Thailand. A total of 365 elderly participants were surveyed using a structured questionnaire.
Results:
Multiple regression analysis showed that general employment (β = −0.227, p < 0.001), business (β = −0.300, p < 0.001), and government service (β = −0.205, p < 0.001) were negative predictors of oral health care behaviors. In contrast, enabling factors (β = 0.204, p < 0.001), average monthly income (β = 0.200, p < 0.001), and supporting factors (β = 0.142, p = 0.005) had positive effects. These factors together explained 20.02% of the variation in behaviors (p < 0.001), with enabling factors having the strongest influence.
Conclusions:
This study emphasizes the importance of financial security, access to dental care, and social support in maintaining oral health among the elderly. Enhancing affordable dental services is crucial for low-income seniors. The findings suggest further research into factors influencing elderly oral health and strategies to improve care access. Recommendations include reducing dental costs, creating family-centered health initiatives, involving families in oral hygiene, and enacting policies to support low-income elderly individuals.
Introduction
Thailand is currently undergoing a profound demographic transformation, marked by a steady rise in its elderly population aged 60 and above. This shift has made Thailand the country with the second-largest elderly population in the ASEAN region, trailing only Singapore. Notably, in 2019, for the first time, the proportion of older adults surpassed that of children under 15 years, with seniors constituting 18% of the total population compared to 15.9% for children. 1 Projections suggested that by 2022, Thailand would enter the phase of a “complete aging society,” wherein over 20% of the total population would be elderly. This demographic transition is largely driven by advancements in public health, nutrition, science, and medical care, all of which have contributed to increasing the life expectancy of Thai citizens. 2
In response to this demographic change, the Thai government implemented a 20-year national strategy (2017–2036) focused on strengthening public health across the nation. The strategic plan is anchored in four main pillars: health promotion and disease prevention, the development of efficient public health services, the training of high-quality healthcare personnel, and the establishment of effective governance systems. 3 A core element of this strategy is ensuring that elderly individuals receive comprehensive healthcare services, with a particular emphasis on oral health. Maintaining oral health is considered critical for sustaining quality of life and independence in aging populations. 4
Oral diseases, particularly among the elderly, are categorized as non-communicable diseases (NCDs) and are associated with a host of physical and psychological challenges. These conditions can cause pain, inflammation, and infection, which in turn compromise an individual’s ability to chew, eat, and maintain a balanced diet. A lack of proper nutrition can further diminish overall health and heighten the risk of other illnesses. Moreover, inflammation from oral infections has been linked to exacerbating chronic systemic diseases such as diabetes and cardiovascular issues. 5
Tooth loss is another prevalent concern that impacts elderly individuals both functionally and socially. It can lead to altered facial structure, slurred speech, and diminished self-esteem, all of which can reduce social engagement and contribute to mental health issues. In extreme cases, poor oral health may hinder daily functioning and reduce the capacity for self-care. Therefore, consistent oral health monitoring and timely dental interventions are crucial. 6 Despite these challenges, oral health among Thailand’s elderly population remains suboptimal. The eighth National Oral Health Survey Report (2017) revealed that only 56.1% of elderly individuals aged 60–74 retained at least 20 functional teeth, with an average of 18.6 teeth per person. This figure dropped drastically for those aged 80–85, with only 22.4% retaining 20 or more teeth and an average of just 10 teeth per person. 7
Phitsanulok Province in northern Thailand had 167,865 elderly residents in 2021, representing 19.76% of its population and indicating its transition to a complete aging society by 2022. 8 Data from Health Zone 2 showed increasing dental service use among the elderly from 2020 to 2022, though disparities remain in the Mueang Phitsanulok district.9,10 The Phitsanulok Community Health Center reported 3232 elderly dental patients in 2020, rising to 4111 in 2022. Key reasons for visits included having fewer than 20 natural teeth (75%), fewer than four pairs of back teeth (34%), and complete tooth loss (33%). Moreover, 59% required dentures, while 31% recognized their need. 11 Oral health issues significantly impacted quality of life, especially in eating (58%), denture hygiene (17%), and self-confidence when smiling (11%), highlighting the importance of denture access and oral care for elderly well-being.
Several factors influence oral health behavior among the elderly, including personal health beliefs, knowledge, attitudes, access to services, dental care tools, health information, and social support. To investigate these variables, the study applied the PRECEDE model, a health promotion planning framework that categorizes influencing factors into three groups: predisposing, enabling, and reinforcing factors. This model highlights that health behavior is shaped by both internal and external influences, and effective health programs must consider all three dimensions. 12
This study explored oral health care behaviors among elderly individuals at the Phitsanulok City Health Center (Buddhachinaraj Hospital) as a case study of lower Northern Thailand. It aimed to identify the factors influencing these behaviors, laying the groundwork for targeted interventions and educational programs. By promoting proper oral health practices, the study seeks to improve health outcomes and enhance the quality of life for Thailand’s growing elderly population.
Design and methods
Study design
This study employs a survey research design. The target population comprises elderly dental patients, including both general patients and those with systemic diseases, who receive services at the Phitsanulok City Health Center (Buddhachinaraj Phitsanulok Hospital). Over the past four fiscal years (2020–2023), an average of 3868 elderly individuals have received dental services annually, as reported by the Office of the Permanent Secretary, Ministry of Public Health. 13
Sample size
The sample for this study includes 365 elderly dental patients from the Phitsanulok City Health Center. The sample size was calculated using Daniel’s 14 formula, resulting in a total of 365 participants. A specific sampling method was employed based on the inclusion and exclusion criteria outlined below to collect data on factors related to the oral health care behaviors of the elderly.
Inclusion and exclusion criteria
The sample group for this study was selected based on specific inclusion and exclusion criteria. Eligible participants included individuals aged between 60 and 75 years at the time of the study, who are Thai nationals registered in the household registration of Phitsanulok Province. Participants were required to be in good health, free from uncontrollable chronic diseases, and possess full consciousness and cognitive ability to engage in the study. Additionally, they must have received dental services at the Phitsanulok City Health Center at least once and provided their consent to participate. Conversely, individuals who were not dependents or who did not consent or were unwilling to participate were excluded from the study.
Instruments used in the research
This study employed a structured survey research design using a questionnaire adapted from previous studies and validated through intra-class correlation to ensure reliability. The questionnaire comprised five sections, each addressing key dimensions of elderly participants’ oral health and related behaviors.
The first section, General Information and Health Status, included seven items collecting demographic and health-related data such as gender, age, marital status, occupation, education, monthly income, existing medical conditions, and living arrangements. These variables provided essential context for interpreting oral health behavior.
The second section explored predisposing factors, including oral health knowledge and attitudes. Knowledge was assessed through 10 multiple-choice questions, scored from 0 to 10. Based on Bloom’s 15 classification, a score of six or more indicated high knowledge. Attitudes were measured using 10 items rated on a five-point scale and categorized using Best’s 16 criteria into five levels ranging from very low to very good.
The third section evaluated enabling factors, particularly access to dental cleaning equipment and services. It included 10 items rated on a three-level scale: regularly, sometimes, and never. The scores, ranging from 1.00 to 3.00, were classified into low (1.00–1.66), moderate (1.67–2.33), and high (2.34–3.00) access levels according to Best’s 16 standards.
The fourth section examined supporting factors, focusing on personal and informational support received regarding oral health. This section had 10 items rated on a five-point scale, with mean scores categorized as very low (1.00–1.80), low (1.81–2.60), moderate (2.61–3.40), or good (3.41–4.20) support, again based on Best’s 16 interpretation.
The fifth and final section assessed oral health care behavior through 20 items rated on a five-point frequency scale (from regularly to never). The resulting mean scores, ranging from 1.00 to 5.00, were categorized into very low (1.00–1.80), low (1.81–2.60), moderate (2.61–3.40), good (3.41–4.20), and very good (4.21–5.00) behavior levels, consistent with Best’s 16 framework.
Overall, the study’s comprehensive and statistically grounded design allowed for an in-depth analysis of multiple factors influencing elderly oral health care behaviors. This approach supports the development of more targeted interventions and policies aimed at improving oral health outcomes in aging populations.
Quality of instrument
To ensure research quality, validity and reliability were rigorously assessed. Validity was evaluated using the Index of Item-Objective Congruence (IOC), achieving a mean value of 0.96 from three experienced dentists. Reliability was measured with a pilot group of 30 Thai nationals aged 60–75, yielding a Cronbach’s alpha coefficient of 0.899. This thorough evaluation ensures accurate data on the oral health care behaviors of the elderly population in Phitsanulok.
Data collection
The research team met with eligible participants, explaining the study’s purpose and their rights, including the option to withdraw at any time. After obtaining consent, participants completed questionnaires independently, returning them to research assistants or a designated box to ensure confidentiality. For those needing assistance, research assistants read the questions aloud. This approach respected participants’ dignity while gathering valuable insights into the oral health care behaviors of the elderly, prioritizing ethical considerations throughout the process.
Data analysis
The data analysis for this study employed both descriptive and inferential statistical methods. Descriptive statistics, including frequency counts, percentages, means, standard deviations, and minimum and maximum values, were used to summarize the demographic characteristics and oral health care behaviors of elderly participants. Inferential statistics explored factors influencing oral health care behaviors. Correlation coefficients assessed relationships between quantitative variables, such as age, monthly income, and various predisposing, enabling, and reinforcing factors. Phi and Cramér’s V tested relationships between categorical variables, including sex, marital status, occupation, education, living arrangements, and medical conditions. Pearson’s correlation examined the connections between quantitative variables, including predisposing factors and income. After ensuring the data met preliminary assumptions and normal distribution, multiple regression analysis identified factors affecting oral health behavior, such as income, reinforcing factors, enabling factors, and occupation types, using stepwise variable selection. The Durbin-Watson statistic was applied to test for autocorrelation in the residuals. These methods facilitated identifying key patterns to inform interventions.
Ethical consideration
The Ethics Review Committee at PSRU approved our interviews (Approval No. 2024/020) on June 24, 2024. Respondents provided written informed consent, with their signatures, before the interviews commenced.
Results
Demographic characteristics of participants
Descriptive statistics revealed that the majority of elderly participants were female (54.79%). The most common age group was 60–65 years, comprising 50.14% of the sample (
Demographic factors in the elderly (n = 365).

Scores and levels of factors influencing oral health care behavior in the elderly
Predisposing factors included oral health knowledge. The average score was 6.24 ± 1.04, with 83.29% of participants demonstrating high knowledge. Many participants understood key concepts, such as sugar causes tooth decay (Item 1, 96.16%) and gingivitis causes bad breath (Item 4, 90.96%). However, knowledge was lower on certain items, like early-stage tooth decay typically having no symptoms (Item 3, 21.46%) and fluoride toothpaste helps strengthen teeth (Item 5, 41.37%). Additionally, only 49.86% knew plaque couldn’t be removed by mouthwash alone (Item 8), and just 15.07% knew brushing for at least 1-min helps prevent cavities (Item 10; Table 2).
Oral health knowledge in the elderly (n = 365).

The overall mean attitude score was 3.94, indicating generally positive views on oral health care. Most items were rated as very good or good. For example, participants agreed on proper brushing to remove food and plaque (Item one,
Levels attitudes and beliefs regarding oral health care, and enabling factors among older adults (n = 365).
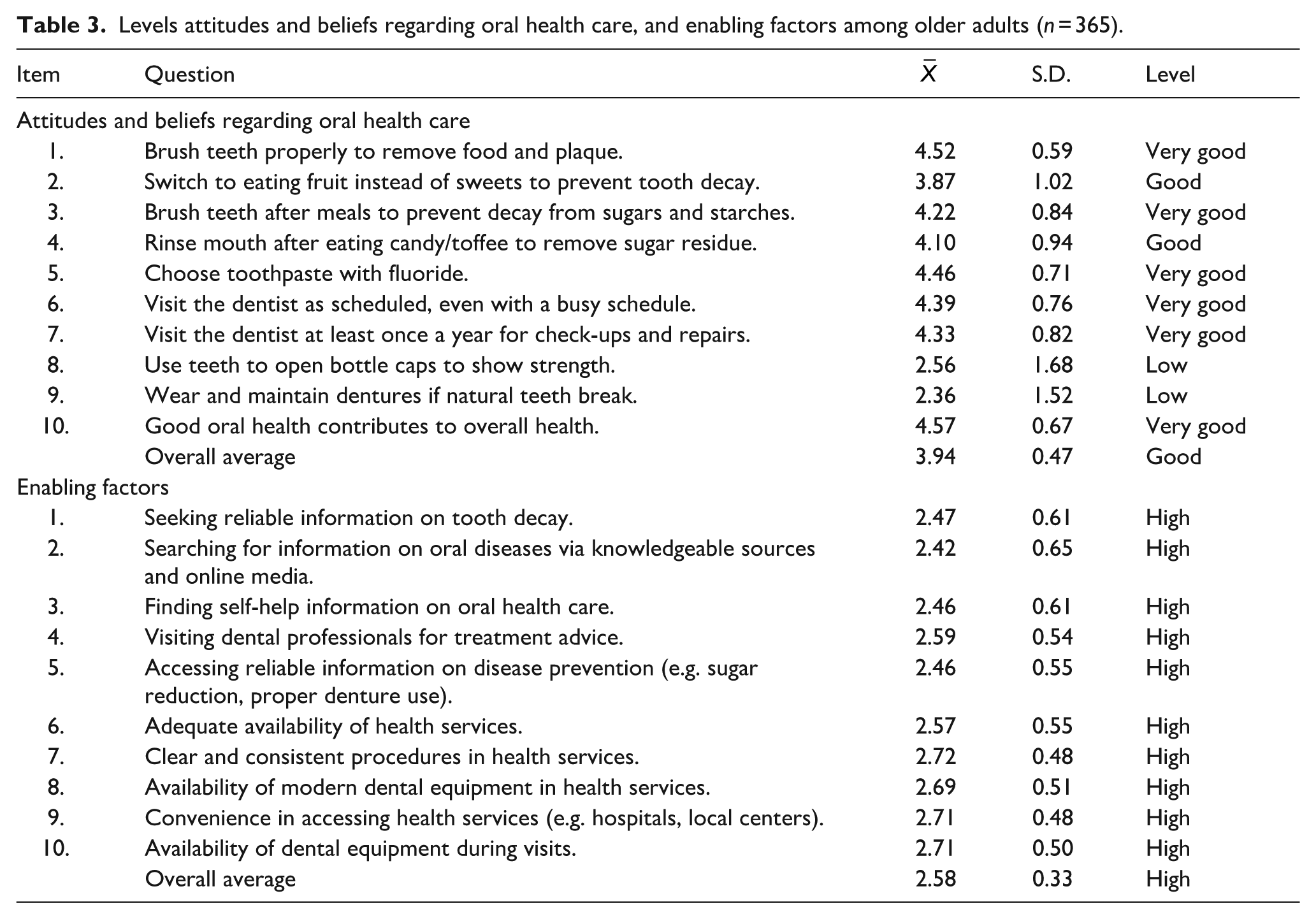
The overall mean score for enabling factors was 2.58, indicating a high level of access to resources and services among elderly participants. All items in this section were rated high, showing that participants actively sought reliable information about oral health. For instance, they frequently searched for details about tooth decay (Item 1,
For supporting factors, the overall mean score was 3.87, indicating a good level of social and informational support. All 10 items were rated at a good level. Participants noted that family members listened to their oral health concerns (Item 1,
Levels of supporting factors and oral health care behaviors in the elderly (n = 365).

The mean score for oral health care behavior was 3.65, reflecting good practices. Participants brushed for at least 2 min (Item 1,
Factors associated with oral health care behaviors of the elderly
The Phi and Cramer’s V analysis revealed significant relationships between oral health care behaviors and occupation (0.435), education level (0.506), and Pearson correlations for enabling factors (0.269), supporting factors (0.178), and monthly income (0.197), all with p-values ≤0.001. However, sex, marital status, living arrangements, and medical conditions showed no significant associations (Table 5).
The relationship between general information, health status, and oral health care behaviors in the elderly.

The relationship is significantly different at the 0.05 level, based on data from 365 participants.
Factors predicting oral health care behaviors of the elderly
Multiple regression analysis using the stepwise method revealed that total enabling factors, average monthly income, and total supporting factors significantly and positively influenced oral health care behavior (p < 0.05). In contrast, general employment, business, and government occupations had a statistically significant negative impact (p < 0.001). Together, these variables explained 20.02% of the variance in behavior. Notably, enabling factors contributed positively (20.40%), while business occupation had the strongest negative effect (30.00%), both with statistical significance (p < 0.001; Table 6).
Predictive factors of oral health care behavior in the elderly.

Note. The sample size was 365 participants. The Durbin-Watson statistic was 1.942, with an R² of 0.202 and an Adjusted R² of 0.189. In the analysis, B represents the unstandardized regression coefficients, SE is the standard error, β denotes the standardized coefficients, t is the t-test, and a p-value of less than 0.05 was considered statistically significant. Collinearity statistics showed acceptable levels (VIF < 1.7), indicating no serious multicollinearity among the predictors.
Discussion
This study explored factors influencing oral health care behaviors among the elderly in Thailand. Results from the multiple regression analysis indicated that employment and business occupations had a statistically significant negative impact on oral health care behavior (p < 0.05). Conversely, average monthly income, total enabling factors, and total supporting factors showed a significant positive association (p < 0.05). These variables collectively explained 20.02% of the variance in oral health care behavior. Among them, enabling factors had the most substantial positive influence (20.40%), while business occupation had the highest negative effect (30.00%). These findings are consistent with earlier studies that identified occupation, income,17,18 enabling resources, 19 and support systems 20 as key determinants of healthcare behavior. No significant associations were found between sex, age, marital status, education, living arrangements, or medical conditions in the Indonesian study. 21
Occupation strongly influenced oral health care behavior, particularly due to its connection with welfare benefits and healthcare access. Elderly individuals employed in the formal sector often receive dental benefits, while retirees or the unemployed face financial limitations. These results align with previous studies,17,18 reinforcing occupation as a determinant of oral health behavior. This highlights occupation as a key factor influencing oral health behavior. Consistent findings across studies support government efforts to address socioeconomic disparities in oral health care for the elderly, emphasizing the importance of income and employment-related welfare in promoting health equity.
Enabling factors, including access to dental services and equipment, had a substantial impact on oral health care behavior. When dental care is easily accessible to the elderly, they are more likely to practice good hygiene, attend check-ups, and follow professional recommendations. The importance of accessible and well-equipped health facilities in improving oral health outcomes is particularly crucial for the elderly, who may face mobility challenges that limit clinic attendance. This finding aligns with previous research demonstrating that enabling resources, such as access to dental care, predict oral health outcomes in adults. While social structures did not directly influence tooth decay or dental service utilization, they had an indirect impact on oral health. 20 These results highlight the critical role of dental care access in improving oral health, especially for the elderly, and underscore the need for policies that address oral health disparities and expand access to dental services.
Monthly income was also a significant predictor of oral health care behavior. Higher income levels were linked to better oral hygiene practices and more frequent dental visits, whereas lower income was associated with unmet dental needs. Previous research has similarly shown that financial status influences dental care utilization, with low-income elderly individuals facing higher risks of tooth loss and untreated dental conditions. 20 These results underscore the need for targeted preventive measures for elderly individuals from lower socioeconomic backgrounds. Factors such as manual labor occupations and lower income levels are also connected to broader health outcomes, highlighting the importance of addressing socioeconomic disparities in healthcare access.
The study emphasizes the vital role of family support in influencing oral health behaviors among the elderly. Elderly individuals who receive assistance and reminders from family members are more likely to maintain good oral hygiene and attend dental appointments. Family members, especially those knowledgeable about oral health, help with tasks like brushing and ensuring access to care, which is crucial for those with physical or cognitive challenges. Married or single elderly individuals generally exhibit better oral care attitudes due to family support, whereas divorced or separated individuals often have poorer oral care habits due to a lack of support.20,22 Family involvement is positively associated with better oral health and increased use of dental services. Strained relationships or lack of family support can negatively impact oral health behaviors by lowering social support and self-awareness. 23 In cultures valuing family cohesion, such as the Chinese community, family support plays a critical role in maintaining oral health. 24 These findings underscore the importance of including family support in public health initiatives to improve elderly oral health outcomes.
Interestingly, this study found no significant association between education level and oral health care behavior, despite previous literature linking education with health literacy.25,26 One explanation may be that financial barriers, limited access to care, or physical impairments outweigh the benefits of education in this demographic. While education can raise awareness, it does not guarantee behavior change when structural barriers remain. Therefore, policy efforts should prioritize improving access and affordability rather than focusing solely on educational interventions.
Conclusions
This study revealed that most elderly participants were female and primarily aged between 60 and 65. They demonstrated moderate knowledge and generally positive attitudes toward oral health care, particularly in areas related to food and gum disease. Many participants reported high levels of oral health behaviors, especially in avoiding smoking and alcohol. Socio-demographic factors, such as occupation and income, were significant predictors of behavior, while enabling factors like access to dental services and equipment supported better oral practices. Family support emerged as a critical component of oral health behavior among the elderly, although challenges such as inconsistent service access remained.
Future research should explore psychological, environmental, and social factors influencing elderly oral health. Mental health, social isolation, and neighborhood conditions may impact oral care and warrant deeper investigation. Additionally, studies should assess how technology, including telemedicine and mobile dental clinics, can enhance service access, particularly in underserved areas. Long-term research on family involvement could further clarify its influence on oral health behaviors over time.
Practically, improving elderly oral health requires more than education. Policy reforms are needed to expand affordable dental care for low-income seniors. Healthcare providers and community organizations should promote family-centered care models, encouraging active caregiver involvement and public campaigns that support sustained oral health practices.
Significance for public health
This study examines factors influencing oral health care behaviors among elderly individuals in lower Northern Thailand, focusing on a case study at the Phitsanulok City Health Center (Buddhachinaraj Hospital). Using data from 365 participants surveyed with a structured questionnaire, the research identified employment status, income, access to dental services, and family support as significant determinants. Business occupations were linked to poorer oral health behaviors, while higher income levels and better service access were associated with improved hygiene and more frequent dental visits. Family involvement, including reminders and assistance with daily care, emerged as a key factor, particularly for those with limited mobility. Notably, education level showed no significant impact, indicating that financial and structural barriers may be more influential than knowledge alone. These findings underscore the importance of developing targeted public health strategies that promote affordable, accessible dental care and strengthen family-centered approaches to support the aging population’s oral health.
Footnotes
Acknowledgements
The authors would like to thank the technicians at Pibulsongkram Rajabhat University for their invaluable support in completing this research. Additionally, we extend our gratitude to the elderly participants who contributed to this study.
Author contributions
Conceptualization, methodology, software, validation, formal analysis, investigation, resources and data curation, writing—original draft preparation, W.S., S.Y., J.T., P.Y., and T.J.; writing—review and editing, W.S., P.Y., and T.J. visualization, supervision and project administration and funding acquisition, W.S. and T.J. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research and Development Institute of Pibulsongkram Rajabhat University, grant no. RDI-2-67-14, fiscal year 2024.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.