
Abstract
Background:
The prevalence and characteristics of falls among community-dwelling Cantonese-speaking older adults in Southern China have not been previously investigated.
Design and methods:
The observational study enrolling 212 community-dwelling Cantonese-speaking older adults was conducted via self-administered questionnaire. Participants’ demographics, fall characteristics, and the belief and attitude score regarding falls were collected and analyzed.
Results:
The prevalence of falls was 30.66%. Poor self-care ability and the linguistic barrier during fall prevention education were associated with history of both single fall and multiple falls. Fall prevention education combining text, video, interviews, and consultation delivered in Cantonese was protective factor associated with single fall and multiple falls. Population experiencing multiple falls expressed unconcern for the fall-prone attire, fall-prone indoor environments and fall risk-increasing drugs.
Conclusion:
The community-dwelling Cantonese-speaking older adults demonstrated distinct fall characteristics and notably high fall prevalence. Linguistic barrier could be the noteworthy risk factor for falls, which should be improved with tailored fall prevention programs and thoughtful health policies.
Significance for public health
The distinguishing characteristics and prevalence of falls of Cantonese-speaking older adults were assessed for the first time in current observational study. We identified the distinct risk factors including linguistic barrier that hinder the effectiveness of falls prevention for this population. Based on current evidence, the implementation of optimized fall prevention is vital for community-dwelling Cantonese-speaking older adults in Southern China region. The dialect barrier should be further mitigated and be considered when formulating public health policies of fall prevention in older adults.
Introduction
Falls are common global public health problem among the older adults along with population aging.1,2 Based on the statistics of the World Health Organization, by 2050, the number of older adults aged 60 years and above will reach 2.1 billion, accounting for almost one quarter of the global population. With aging, falls become common incident in community-dwelling geriatric population and are the rising cause of unintentional injury that result in various degree of disability. 3 For the elderly, the falls may lead to non-fatal or fatal injuries reducing quality of life, increasing healthcare or rehabilitation costs, and elevating burden for health system, thus posing worldwide impact. 4 Moreover, falls are also the second leading cause of unintentional injuries-related death worldwide, with the elderly being the most susceptible. 5
Evidence indicated that the worldwide prevalence of falls in the older adults over 65 was 26.5%, based on the result of meta-analysis. 6 However, there is still heterogeneity of fall rate across different countries, populations, regions, culture, times, and living environments. 7 In order to further assess the determinants and the consequences of falls in the context of changing times, ongoing researches on the epidemiology of falls in each area or worldwide remain warranted.
According to the report from Chinese center for disease control, the prevalence of falls among older adults is 20.7%. 8 Previous research also revealed that the annual prevalence of multiple falls in China was 4% to 5%. 9 In addition, falls were one of the leading factors of injury-related mortality and the tremendous contributor to disability-adjusted life-years (DALYs) among the elderly in China.10,11 It was estimated that China’s elderly population aged 60 years and above will increase to about 28% of the total population by 2040. 12 Along with the growing elderly population in China, the falls inevitably remain the ongoing health issue and foreseeable burden for both older adults and public health system. 13
Numerous researches have disclosed various fall risk factors for community-dwelling older adults including the aspects of biology, behavior, socioeconomic status, and environment. For instance, the aging is one of the most significant risk factors that elevated the incidence of falls after age 70. 14 Fall-related physical factors include chronic diseases, impaired balance ability, musculoskeletal disorders, blurred vision, degenerative nerve diseases, etc. 5 Moreover, mental impairment, low social support, and unhealthy life behavior are also fall-related risk factors.15,16 Furthermore, the socioeconomic and socio-environmental factors in developing countries, such as misconception, inadequate health system, shortages of healthcare provider, and unsafe living environment also increase the fall risk for the elderly. 17
Notwithstanding the evidence for various risk factors, scarce research explored the cultural or linguistic factors that may be related to falls. A few research merely investigated the language barriers during falls prevention for people with limited English proficiency.18,19 Considering the information regarding the prevalence and the factors of falls in Cantonese population is lacking, this study aims to explore the characteristics of falls in the community-dwelling older adults who mainly speaking Cantonese in Southern China. Cantonese, best-known as “Yue dialects,” is spoken by older generation in Guangdong province, Guangxi province, and Hong Kong, which are also known as the Lingnan region. 20 According to the survey in Chinese literature, the users of Cantonese in Guangdong were approximately 40 million. In the routine community survey of our research area, we only assessed the falls among older adults who speak both Mandarin language and Cantonese, and reported the prevalence of falls among them, which was approximately 11%. However, we did not consider the possible barrier during health education or falls prevention education for the older adults primarily speaking Cantonese. Since the mainstream of falls prevention education before and during the period of this survey was conducted with Mandarin language, there was no report about how this situation hinder the efficiency of falls prevention program for Cantonese population. This could pose problematic issues for regional public health system regarding falls prevention for Cantonese population.
Therefore, we aimed to reveal the prevalence and the characteristics of falls of community-dwelling older adults, especially Cantonese speaker, in Guangdong province that has not been previously studied. We attempted to explore whether the linguistic barrier during fall prevention education was related to non-fall and falls situations in this region and disclose the difference from previous evidence. We anticipated providing tailored recommendations considering linguistic factors of falls prevention in this region in the future and further proposing implications for alike regions with various dialects.
Materials and methods
Participants
The participants of this survey were people aged 55 or above, who mainly speak Cantonese and live in Pengjiang District, Jianghai District, Xinhui District, and Jiangmen City of Guangdong Province. Based on previous census, there was a considerable amount of retired and community-dwelling adults aged 55 and above, so the inclusion criteria were extended to this age range. Simple random sampling was applied in this area, participants were selected randomly from the list of community visit of our program in the selected regions, and finally, 212 older adults were enrolled in the survey. Demographic information was acquired, and the questionnaires were administered to participants during the community assessment and on-site interviews in one session, the period of this survey was started from January 3, 2022 to March 31, 2023. The community on-site interviews were conducted face-to-face in community centers or participants’ homes. If participants could not comprehend the questionnaires or finish survey independently, interpretations or interviews were conducted. Exclusion criteria included individuals with neurodegenerative diseases, cognitive impairment, immobility, inaccessibility of medical care. Individuals with neurodegenerative diseases and cognitive impairment were identified based on diagnosis information from annual health check-up or information provided by caregiver or family member, and they were excluded from the survey due to the incapability of completing questionnaire. The written informed consents of the participants were obtained before this community investigation, which stated the anonymity was assured and the anonymous information collected by the questionnaire could only be used or be published for academic purposes.
Questionnaire and data collection
Demographic characteristics, physical state, falls history, belief and attitude regarding falls, and falls-related circumstance were included in the questionnaire, which was developed in accordance with the opinions of elderly care experts in Jiangmen region and had been previously validated and used for community survey (articles in Chinese version only). The distribution and collection of questionnaires were conducted during on-site community survey and elderly health knowledge propaganda, which were carried out by researchers, community liaison staffs, and the volunteer team that were trained at the Jiangmen Vocational College of Traditional Chinese Medicine in Guangdong Province. Executors were trained for communication skills with Cantonese to efficiently converse with older adults on account of most of the respondents were not proficient in speaking Mandarin language and had difficulty reading due to lower educational level or age-related low vision.
Variables
Demographic characteristics, including gender, age, education level, marital status, whether having chronic disease, living status, self-care status or whether needing caregivers, whether receiving fall prevention education, and the forms of received fall prevention education, were acquired via on-site interview. Falls history, including unintentional falls, but excluding falls due to acute physical status and external forces, was reported by the respondents, or their family members and the main caregivers if the respondents had difficulty communicating or could not recall the falls situation. The data with ambiguous and divergent answers from proxy respondents was excluded to avoid unauthenticity and bias. According to the falls history, the respondents were divided into the group without falls, the group with single fall, and the group with multiple fall. The belief and attitude scores regarding falls of participants with a five-point Likert scale, which was developed by public health and geriatric care experts in author’s college had been used for census in Jiangmen region to evaluate the respondent’s subjective perception of the importance of the fall-related factors (very unimportant = 1 point; not important = 2 points; average = 3 points; important = 4 points; very important = 5 points), were measured and compared among three groups. The questionnaire was partially adapted from previous articles and was simplified for the suitability and the better comprehension for the local older adults.21–23 The factors comprised eight dimensions including the importance of wearing fit clothes or not wearing loose clothes to avoid being tripped over, wearing skidproof and fit shoes (or slippers), using skidproof floor tile or other materials in the house, ensuring sufficient indoor illumination and adequate illumination at night, applying barrier-free home design including furniture and other accessories, using walking aids when walking indoors or outdoors, wearing appropriate glasses for clear vision, and being aware of fall-risk-increasing drugs such as antihypertensive, opioids, and antidepressants.
Statistical analysis
The questionnaires data was entered and sorted by two people using EpiData (version 3.1; EpiData Association, Odense, Denmark). Statistical Product and Service Solutions (SPSS; version 25.0; IBM. Corp, Armonk, NY) was used to analyze the data. The reliability and validity of self-rated belief and attitude score of falls in questionnaire was assessed via Cronbach’s alpha and KMO and Bartlett’s test, respectively. Data for descriptive statistical analysis was illustrated as the number and percentage, continuous variables were illustrated as mean and standard deviation (SD). Univariate analysis via Chi-squared test was conducted for categorical variables to assess the variables that were related to the prevalence of falls. Multiple logistic regression was applied to analyze the association among categorical variables and to distinguish the protective or risk factors for falls. The Kruskal-Wallis test with post-hoc Dunn’s test was utilized for assessing the variation of continuous variables of falls-related belief and attitude scores among groups when the normality assumption is not met. p < 0.05 was considered as statistical significance for the differences.
Results
A total of 212 older adults were enrolled in this survey. Sixty-five of participants experienced a fall (or multiple falls), with fall prevalence of 30.66%. The demographic characteristics we analyzed include gender, age, education level, marital status, health status, living status, care status, and whether receiving fall education. The participants were categorized into three situations, experiencing no fall (non-fall) (n = 147, 69.33%), experiencing single fall (single fall) (n = 30, 14.15%), and experiencing multiple falls (multiple falls) (n = 35, 16.5%). Univariate analysis was applied to assess if these categorical variables were related to the situations of falls.
Several variables were not related to the number of falls nor the prevalence of falls, including gender (p = 0.375), age (p = 0.837), educational level (p = 0.382), marital status (p = 0.745), whether participants having chronic disease or not (p = 0.184), and whether participants living alone or not (p = 0.543).
Fifteen participants with full self-care ability (15/148, 10.13%) and 15 participants requiring caregivers (15/64, 23%) reported single fall. Nineteen participants with full self-care ability (19/148, 12.83%) and 16 participants requiring caregivers (16/64, 25%) reported multiple falls. The self-care ability was related to the occurrence of falls (χ2 = 13.77, p = 0.001). Participants with full self-care ability had lower prevalence of both single fall and multiple falls. Four participants that receive no fall prevention education (4/15, 26.66%), 8 participants only receiving text- and video-based fall prevention education (8/35, 22.85%), and 18 participants receiving text- and video-based and on-site fall prevention education including interview and consultation using Cantonese (18/162, 11.11%) experienced single fall. Five participants who receive no fall prevention education (5/15, 33.33%), 5 participants only receiving text- and video-based fall prevention education (5/35, 14.28%), and 25 participants receiving text- and video-based and on-site fall prevention education (25/162, 15.43%) experienced multiple falls. Whether participants received fall prevention education and the forms of education were related to the occurrence of falls (χ2 = 9.854, p = 0.043). Participants receiving text- and video-based and on-site fall prevention education had lower both prevalence of both single fall and multiple falls (as shown in Table 1).
Demographic characteristics and univariate analysis of falls.
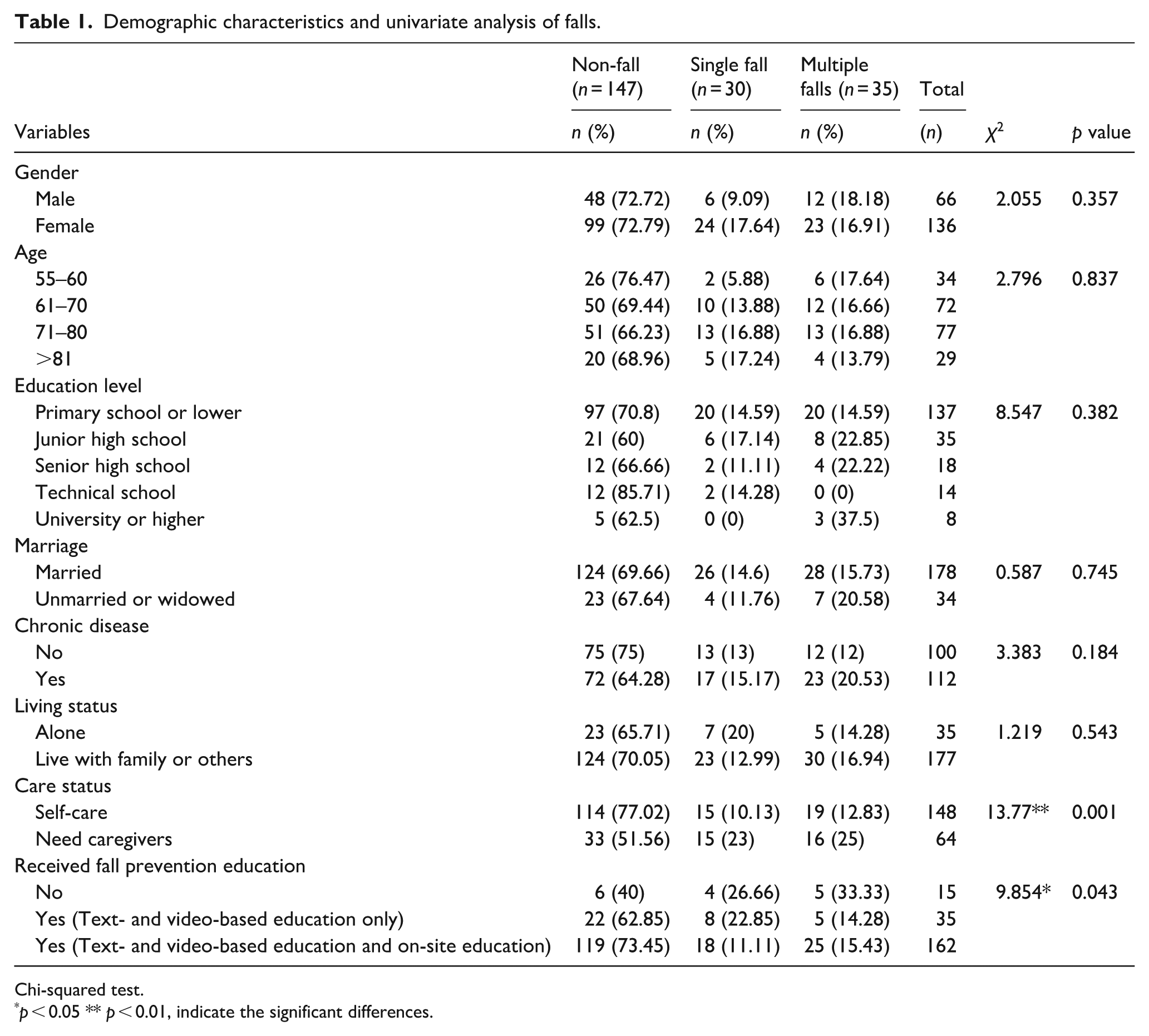
Chi-squared test.
p < 0.05 ** p < 0.01, indicate the significant differences.
The variables that were significantly related to the number of falls and the prevalence of falls, including the care status and the form of fall education, which were confirmed by univariate analysis were include in the multiple logistic regression analysis. The results revealed that the self-care ability was protective factor associated with incident of single fall (OR = 0.298, 95% C.I.: 0.128–0.653, p = 0.003) and the incident of multiple falls (OR = 0.344, 95% C.I.: 0.159–0.742, p = 0.007), using the variable of “need caregivers” as the reference. The participants with full self-care ability were associated with lower prevalence of both single fall and multiple falls. Moreover, the results indicated that receiving text- and video-based fall prevention education and on-site fall prevention education including interview and consultation using Cantonese was protective factor associated with the incidence of single fall (OR = 0.169, 95% C.I.: 0.046–0.613, p = 0.007) and the incidence of multiple falls (OR = 0.301, 95% C.I.: 0.055–0.724, p = 0.04), using the variable of “receiving no education” as the reference. In addition, receiving text- and video-based only fall prevention education was neither associated with single fall nor multiple falls. The current fall prevention education without considering linguistic barrier did not demonstrate prominent effect on the prevalence of falls in the inspected area with composition of older adults mainly speaking Cantonese (as shown in Table 2).
Multiple logistic regression analysis of falls.

Multiple logistic regression.
p < 0.05, **p < 0.01, indicate the significant differences.
The belief and attitude scores regarding falls of participants were assessed in this survey to distinguish the variations among the group with no fall, the group experienced single fall, and the group with multiple falls. The self-rated belief and attitude of falls questionnaire that we utilized had been administered for community-dwelling older adults in China. The questionnaire assesses whether the participants consider the falls-related factors important (not very important, 1 point; not important, 2 points; average, 3 points; important, 4 points; and very important, 5 points), as described above in the methods. The psychometric properties and suitability for study of the questionnaire were also validated. The results showed that the internal consistency of the self-rated belief and attitude of falls that we applied in this survey was excellent (Cronbach’s α = 0.903). The results also demonstrated that the KMO value was 0.874 and the Bartlett’s test of sphericity was significant (p < 0.001), which indicated the data was suitable for factor analysis (data was not shown in table). The scores among three groups were compared and analyzed by using Kruskal-Wallis test with post-hoc Dunn’s test because the normality assumption is not met. The results revealed that the group with multiple falls were less concerned about wearing fit clothes and not wearing loose clothes (4.14 ± 0.73 vs 4.49 ± 0.74, p = 0.013, as compared with non-fall group), and were less concerned about wearing skidproof shoes (4.28 ± 0.78 vs 4.65 ± 0.72, p = 0.004, as compared with non-fall group). Participants with multiple falls also were less concerned about barrier-free home design and furniture (4.02 ± 0.85 vs 4.41 ± 0.72, p = 0.032, as compared with non-fall group). Moreover, participants with multiple falls were less concerned about fall risk-increasing drug (4.05 ± 0.87 vs 4.44 ± 0.75, p = 0.024, as compared with non-fall group). The total belief and attitude scores of falls of group with multiple falls group were significantly lower than those in non-fall group (33.54 ± 4.20 vs 35.75 ± 4.88, p = 0.007), whereas the scores of single fall group had no significant difference, as compared with non-fall group (as shown in Table 3).
Comparative analysis of the belief and attitude score regarding falls among groups.
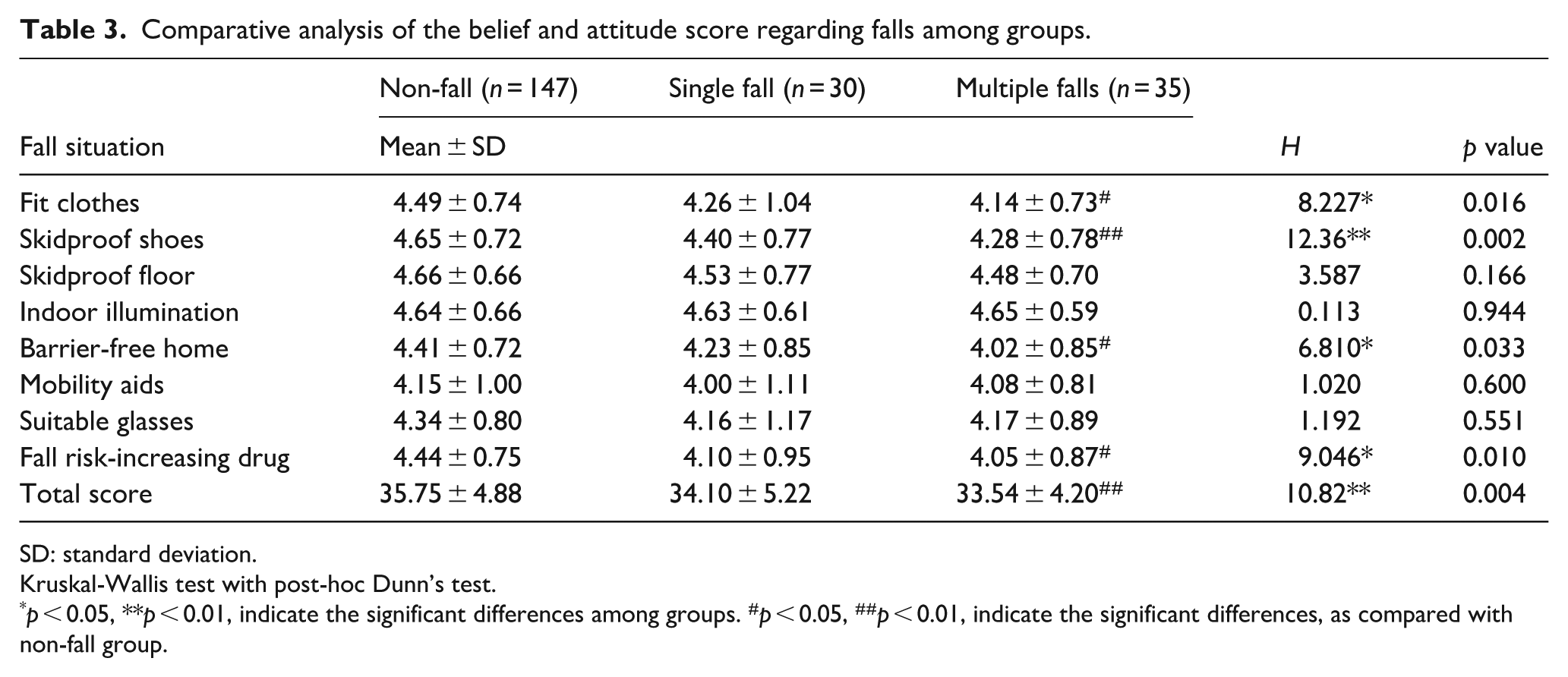
SD: standard deviation.
Kruskal-Wallis test with post-hoc Dunn’s test.
p < 0.05, **p < 0.01, indicate the significant differences among groups. #p < 0.05, ##p < 0.01, indicate the significant differences, as compared with non-fall group.
Discussion
This research indicated the prevalence and the distinct characteristics of falls among the community-dwelling older adults mainly speaking Cantonese in Southern China. The falls prevalence in this area was 30.66%, with a notably high prevalence as compared with previous documented data of Chinese older adults living in community, with a prevalence of 8.67%. 24 Furthermore, we confirmed the self-care status of older adults and the falls prevention education they received were related to both single fall and multiple falls history. We further verified the text and the video forms of falls prevention education that currently applied in this area was not related to the lower falls prevalence for Cantonese-speaking older adults, which indicated the linguistic barrier for older adults was negatively associated with the effectiveness of falls prevention. Additionally, the results revealed that the individuals with multiple falls history were unconcerned about fall risk factors including their attire, indoor environment, and the fall risk-increasing drug. The results revealed the partially atypical characteristics of falls among community-dwelling Cantonese-speaking older adults in Southern China, which can offer further suggestion to optimize the falls prevention strategies for public health system.
The falls prevalence of community-dwelling Cantonese-speaking older adults we discovered in this survey was notably high, reaching 30.66%. Based on relative research, the general prevalence of fall of older adult are 34.4% in Oceania, 27.9% in America, 25.8% in Asia, 25.4% in Africa, and 23.4% in Europe. 6 The falls prevalence obtained in this survey was relatively high, as compared with the falls prevalence in Asia. The falls prevalence of older adults in our result was also higher than the general prevalence in Guangdong, which was 11.9%, and was also higher than the prevalence in Shanghai (10.7%) and Beijing (13.1%), which had the similar socioeconomic status.5,25 These results indicated that the community-dwelling Cantonese-speaking older adults indeed suffered from higher prevalence of falls, which raised a new concern for public health system.
Regarding the results of fall risk factors, we only discovered the populations with good self-care ability and those who had received fall prevention health education were related to lower rate of falls. Both male and female populations demonstrated high incident of falls, approximately 27%, which was distinct from previous studies. 26 The age was also not a strong fall risk factor in this region, individuals aged 55 years and above had similar rates of falls, even with a notably high rate, 23%, in 55–60-year-old population, which was different from previous evidence indicating age as risk factor. 27 The result indicated the educational level was not related to falls in this region, which demonstrated individuals with higher educational level did not have lower prevalence of fall, which was dissimilar to previous evidence. 28 Although marital status was considered as better health-related factor, 29 we did not observe the relation between marital status and lower prevalence of falls. In our results, the population with chronic diseases was not related to higher prevalence of falls, which indicated chronic diseases were not the primary factors inducing the remarkably high prevalence of falls in this region, which was also different from previous evidence. 30 Whether living with family members was not related to prevalence of falls in our results, even though family provide main health support for older adults. 31 Older adults living alone had similar prevalence of falls to those living with family, which also indicated the further requirement for strengthening the healthcare ability and the fall prevention knowledge.
Population with better self-care ability was related to lower rate of both single fall and multiple falls, which was consistent with current evidence. 32 This also proposed the need to reinforce the self-care actions and behaviors of older population for the prevention of falls. Furthermore, we discovered the traditional fall prevention education did not prominently decrease the odds ratio of falls for Cantonese-speaking older adults, especially the text- and video-based fall prevention educations. In contrast, text- and video-based fall prevention education and on-site fall prevention education including speech, interview, and consultation using Cantonese were associated with lower odds ratio of single fall and multiple falls. Since the young generation in Guangdong trend to the use of Mandarin, 33 also called “Putonghua,” fewer young generation use Cantonese. Based on author’s experience, the current fall prevention education and other health education are mainly conducted with Mandarin by young generation of healthcare provider, which necessitates the social workers speaking Cantonese to communicate with older adults, which may hinder the efficiency of health education for the community-dwelling Cantonese-speaking older adults.
Based on previous research, linguistic barriers and limited language proficiency have negative effect on the healthcare delivery, health information dissemination, the satisfaction of patients, patient safety, and financial burden for healthcare system. 34 Although interpreter and mobile application can address linguistic barriers for healthcare system, there are still problematic issues including the misinterpretation by informal interpreter, impaired quality of communication, and poor accuracy.35,36 Moreover, the dialect barriers in multilingual region may cause further challenges for healthcare professionals and public health system, which requires the training for linguistic diversity. 37 The current results also indicated that the dialect barrier cause challenge for fall prevention education. The transform of health education via using Cantonese were conducting recently, which still required more time to evaluate the outcome. Therefore, our results revealed some distinct characteristics of falls among the Cantonese-speaking older adults, which provided suggestion for optimizing fall prevention strategy.
According to the belief and attitude scores regarding falls, older adults with multiple falls history in this region were unconcerned about wearing fit clothes or not wearing loose clothes, wearing anti-slip shoes, the importance of barrier-free home design and furniture, and fall risk-increasing drug, which were common fall risk factors. 38 Based on author’s experience during community visitations, most of the floor tiles in the traditional-designed home of the older adults are the original brick and stone floor, which are rough and have good anti-skid effect, whereas most of the older adults trend to wear plastic slippers, which are consistent with the results above. The traditional house characteristics and lifelong habit might influence the unconcern of wearing anti-slip shoes in the older population in this region. Besides, the division of each area in traditional style home is often unclear, which causes the obstacles resulted from the misplaced objects, furniture, and wires. These cultural habits might further worsen the lower concern about the importance of barrier-free home design. Indoor environmental modifications and age-friendly housing integrating with local culture are vital for the older adults in this region. Furthermore, older adults with multiple falls showed less concern about fall-risk-increasing drugs (FRIDs), a prominent risk factor,which had been reported that 65%–93% of older adults used FRIDs have suffered from fall injuries.39,40 FRIDs include antipsychotics, antidepressants, anxiolytics, sedatives, narcotics, antiepileptics, antihypertensives, antihistamines, opioids, and non-steroidal anti-inflammatory drugs, 41 which are fall risk factors in the older adults with polypharmacy. The situation of unconcern of FRIDs was relatively apparent in people suffered from falls in our survey, even though no significant difference in single fall group, which suggested the need to strengthen the FRIDs-related knowledge in this region. We can further improve the content of fall prevention education on the basis of these results. Furthermore, based on the demographic characteristics, the education level of most of respondents were low, which may be related to inadequate health literacy. 42 The prevalence of falls may be negatively correlated with health literacy, 43 whereas it required further survey to clarify the reason why community-dwelling Cantonese-speaking older adults disregard these falls-related factors.
Despite the fact that older adults prefer Cantonese for health education, the Cantonese pronunciation and tone vary among region even in Guangdong, which may lead to poor interpretation. There is still room for improvement for fall prevention strategy tailored to older adults in this region. Moreover, the current survey only recruited the adults mainly speaking Cantonese, which limited the generalizability and precluded the comparison of fall-related characteristics with those of adults mainly speaking Mandarin or other dialects and living in other region of China. In addition, the current cross-sectional study design cannot testify the causality and the effect of dialect barrier on fall prevention education efficacy.
Furthermore, the questionnaire applied in current survey was mainly used in Jiangmen region for census purposes and was only available in a Chinese version. Even though we have validated its psychometric properties and confirmed its suitability for study, the reference in English literature is still lacking, which could hinder the generalizability of this questionnaire. The globally used survey instruments for fall risk and fall awareness assessment were lacking, which was also the limitation for the comprehensive analysis. The self-reported falls history can also be subject to recall bias and the low accuracy and reliability, which may be further improved by health monitoring tools, such as wearable devices. In regard to sample size estimation, the actual population of older adults that only speak Cantonese was unclear, we merely randomly selected participants form our community visit pro-gram, which could be further improved by collaboration with census system to expand sample size. Additionally, the subgroup analysis may be further applied to identify whether specific groups, such as those with different physical activity or comorbidities, are associated with diverse characteristics of falls. Further surveys with more populations based on dialects and multiple regions, more compendious assessment tools, and the comparison of various fall-related indicators are required for proposing the evidence to the optimization of public health policy for fall prevention in different regions.
Conclusions
We elucidated the distinguishing characteristics and prevalence of falls among the community-dwelling Cantonese-speaking older adults in Southern China for the first time. The falls prevalence in this region is notably high along with characteristics that are distinct from those of general Chinese older adults. Linguistic barrier during fall prevention education is indeed risk factor associated with falls. The unconcern for the wearing, barrier-free indoor environment, and fall risk-increasing drug should also be ameliorated. Effort is necessitated to propose tailored fall prevention strategy for diminishing inequity and hindrance from dialects.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251388565 – Supplemental material for Distinguishing characteristics of falls among community-dwelling Cantonese-speaking older adults in Southern China: A community-based observational study
Supplemental material, sj-docx-1-phj-10.1177_22799036251388565 for Distinguishing characteristics of falls among community-dwelling Cantonese-speaking older adults in Southern China: A community-based observational study by Ying Yuan and Wei-Yi Wu in Journal of Public Health Research
Footnotes
Acknowledgements
We acknowledged the volunteers from Guangdong Jiangmen Chinese Medicine College for assisting with the survey.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Jiangmen bureau of science and technology (No. 2021YL05002).
Consent to participate
The written informed consent to participate in this research was obtained from all participants involved in the survey.
Consent for publication
The informed consent for publication was provided by the participants.
Author contributions
Conceptualization, Ying Yuan and Wei-Yi Wu; Data Curation, Ying Yuan and Wei-Yi Wu; Formal Analysis, Wei-Yi Wu; Investigation, Ying Yuan; Methodology, Ying Yuan; Project Administration, Wei-Yi Wu; Resources, Ying Yuan; Supervision, Wei-Yi Wu; Validation, Wei-Yi Wu; Visualization, Wei-Yi Wu; Writing – Original Draft Preparation, Ying Yuan; Writing – Review & Editing, Wei-Yi Wu.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are accessible on request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.