
Abstract
Background:
Medical students in Egypt are increasingly susceptible to higher levels of stress and anxiety compared to their peers. The current study aimed to assess the effect of stress management intervention in decreasing their stress and anxiety levels.
Design and methods:
A randomized controlled study was conducted on two phases survey and intervention phase using perceived stress scale to assess stress and Beck Anxiety Inventory to assess anxiety. Students with moderate/severe stress in the survey stage were stratified randomized to intervention or control group (140 in each group). The program was composed of 12 sessions for 12 weeks. Stress and anxiety were re assessed immediately after and in 3 months post intervention.
Results:
There was no significant difference between the means of perceived stress between the intervention and control groups at the baseline (25.03 ± 3.18, 24.40 ± 3.15, p = 0.098). There was a significant higher mean score of perceived stress in the control group compared to intervention group immediately post intervention (33.39 ± 9.47, 24.40 ± 3.46, p < 0.001) and 3 months later (33.03 ± 9.40, 23.76 ± 3.37, p < 0.001). While there is no significant difference between the mean score of perceived anxiety between the intervention and control groups at the baseline, post intervention and in the follow up.
Conclusions:
The stress management program was effective in decreasing perceived stress level among medical students. The widespread implementation of the study program could help medical students for coping with their stress levels.
Introduction
Stress among medical students in Egypt has a great concern.in Egypt, about 69% of medical students perceived moderate to severe stress, 1 while 73% perceived anxiety 2 and 88% having burnout. 3 Medical students are more susceptible to greater stress compared to other college students. 4 This could be explained by several factors such as higher academic load, frequent examinations, higher expectations of themselves, and higher parental expectations, lesser time for hobbies or exercise and more social isolation. 5 Stressors among medical students in Egypt are not only academic. Financial pressure, lack of leisure time and transition to clinical responsibility and social and relationship challenges strongly influence the high medical students stress and burden in the Egyptian context. 3
Medical students stress can have several negative effects on their well-being and academic performance. Some of the consequences of this stress include inefficiency and reducing their ability to effectively manage workload. 6 Furthermore, stress can also contribute to decreased academic performance, difficulty in retaining information and engaging in effective learning practices. 7 Another consequence of stress in medical students is burnout and personal detachment. 8 Moreover, the stress faced by medical students can also develop depression or trigger pre-existing depression. Medical school can be an incredibly challenging time for individuals with a history of depression or other mental health conditions. The stressors and demands of the curriculum can amplify feelings of sadness, hopelessness, despair, and even triggers suicidal ideation. 9
Medical student anxiety pertains to feelings of tension, worry, and unease that are specifically related to the academic and clinical demands of medical education. Anxiety commonly accompanies the high levels of stress experienced by medical students. 10 This can further impair their ability to focus, perform well, and maintain their overall well-being. 10 The prevalence of medical students’ anxiety is 33.8% globally compared to 42.4% in the middle east. 11
WHO revealed that college students stress increases their risk of developing mental disorders. It suggests that up to 46.9%–80% of mental disorder prevalence could be abolished if stress prevention interventions were developed among college students. 12 Stress management interventions are crucial for medical students and have been shown to reduce stress and improve coping mechanisms.13,14 To date, no Egyptian study has focused on stress management among medical students, rendering this study unique in this regard. This investigation was conducted at the Faculty of Medicine at Helwan University, a recently established institution located 30 km south of Cairo. The initial phase of this study aimed to assess the levels of stress and anxiety and identify the primary stressors experienced by these students to inform the development of a stress-management intervention tailored to address these specific stressors. In the second phase, the developed program was implemented and evaluated with the objective of enhancing the students’ capacity to effectively manage stress and anxiety throughout their academic tenure.
Design and methods
Study setting
The study was conducted at the Faculty of Medicine, Helwan University, Egypt.
Study design and sample size
The study design is a parallel two groups randomized controlled intervention study conducted on two phases:
-
-
○
- Moderate and high level of perceived stress.
- Marital status; single.
○
- History of psychiatric disease.
- Consuming psychiatric drugs within the past 6 months.
- Working students.
- Having chronic neurological disease that can affect stress and anxiety (e.g. MS).
- Having chronic medical disease that interferes with psychological state (e.g. thyroid abnormality, uncontrolled DM, renal dysfunction).
Study participants
At the survey stage, 1696 medical students (42% of total students at the time of data collection) agreed to participate in the study and fill out the online survey. Students with moderate and severe stress were 1580 (93.2%) of participants. Based on exclusion criteria mentioned before, there became 1274 students. Stratified random sampling technique was applied on the target students based on grade and gender. First, randomization was performed with respect to grade (representative quota was calculated from each grade according to its percentage). Then, block randomization was applied for each grade according to male or female gender to equally represent each gender in the final sample. For each block half were randomly assigned as intervention and half as control group. The final sample showed equal representation to avoid confounding of gender and grade. The process of randomization was performed using SPSS version 28. The final sample was 140 intervention and 140 control.
Intervention
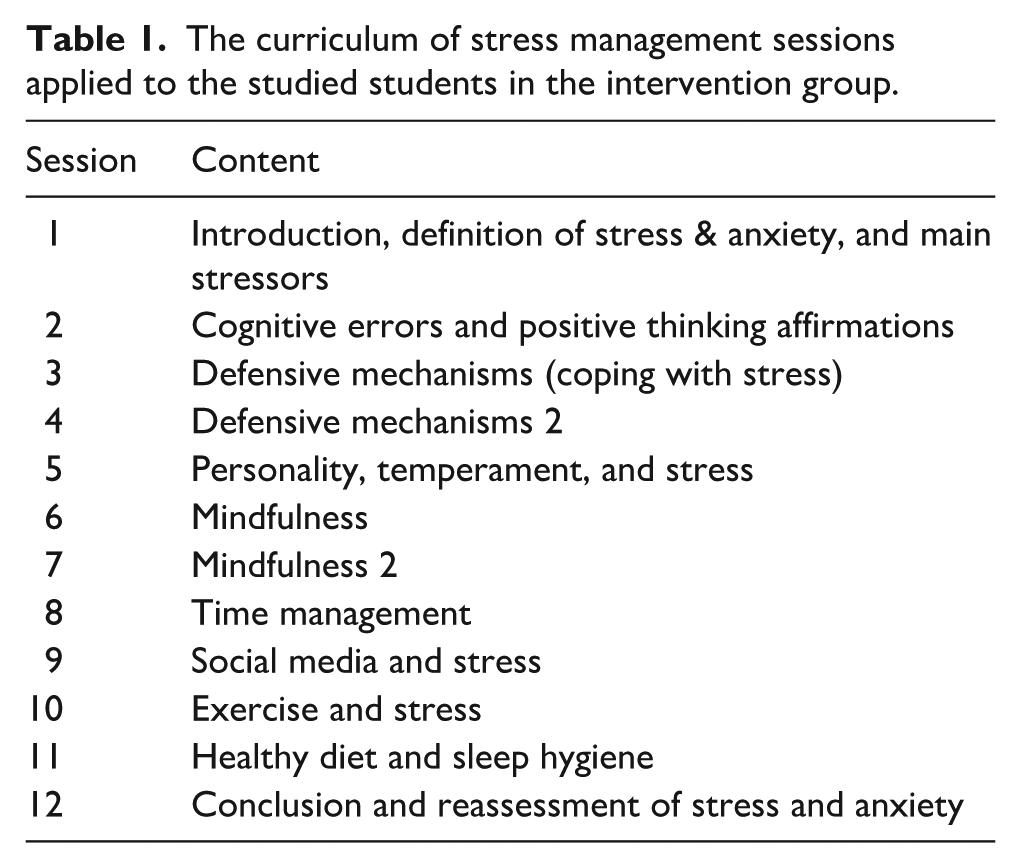
Intervention groups were divided into 14 small groups. Each group includes 8–15 students. Each small group was submitted to the stress management program which was composed of 12 sessions for 12 weeks described in Table 1. Session’s provider was trained for executing the stress management program by the psychiatric consultant (Ass. Prof. Samah Rabei). The sessions were conducted virtually via Microsoft Teams on a weekly basis from February 10, 2023, to June 25, 2023. Both stress and anxiety were assessed online immediately after the program and 3 months after, contemporary in both intervention and control groups (Figure 1). The online questionnaire was sent to students in both intervention and control groups through their e-mails. Of 280 eligible students who completed the full baseline survey, the loss of follow up was 1.78% (no. = 5) at post assessment 1 and was 6.78% (no. = 19) at post assessment 2. The following are the contents of the program:-
- Session 1 (introduction to the program):- the session included definition of stress and anxiety, main stressors among medical students, stress performance curve, scales to measure stress, anxiety, and main stressors. The session time was 25–30 min.
- Session 2 (cognitive distortion and positive thinking affirmation):- the session explained different forms of cognitive distortion (polarized thinking, personalization, overgeneralization, always being right, global labeling, should thinking, emotional reasoning, catastrophic thinking, blaming, fallacy of change, minimization, jumping to conclusions, filtering, heavens reward fallacy, and control fallacy) with examples and videos explanation. Every student was asked to record in his notebook if he had any cognitive distortion. The session then explained the ways to treat cognitive distortion (cognitive reconstruction) using thought record method in detail using video demonstration. Finally, the session discussed positive thinking affirmation and how to write personal positive thinking messages. The session time was 45–55 min.
- Session 3 (coping with stress):- the session included definition of coping with stress and the strategies used. The first strategy (problem solving) in case of solvable problems was explained to students. The second strategy (defense mechanism) is in case of unsolvable problems. The first three types of defense mechanisms (childhood, adolescent, and mature) were discussed in detail with students. The session time was 35–45 min.
- Session 4 (continuation of coping with stress): the session included the fourth type of defense mechanism (pathological defense) in detail. Then students were asked to assess their way of coping with stress using coping and stress management skills online test https://testyourself.psychtests.com/category/7. The session time was 35–40 min.
- Session 5 (Personality temperament and stress): this session discussed the different personality temperaments that mediate different responses to stress as resilience, self-confidence, optimism, self-concept and personality traits. The three personality types A, B, C were explained in detail. Every student was asked to assess whether he has type A personality or not using Type A personality test https://testyourself.psychtests.com/category/7. The session time was 40–45 min.
- Session 6 and 7 (Mindfulness):- the two sessions were mainly to practice mindfulness meditation exercises by lecturer and video demonstrations. Session 6 started with defining mindfulness and meditation and mindfulness based cognitive therapy. Then practicing mindfulness exercises (1 min mindfulness breathing, five finger breathing, grounding exercise to manage anxiety). Session 6 was 25–30 min. Session 7 included practicing five sense exercises and practicing mindfulness self-compassion. In addition, the importance of gratitude and practicing gratitude exercises (mainly gratitude journal). Session 7 duration was 25–30 min.
- Session 8 (time management):- the session discussed the definition and importance of time management. The students were asked to assess their time management skills using 20 items time management skill questionnaire. Then the five steps of time management were discussed in detail. Step 1 (time tracking practice) was explained to students using time tracker mobile application to detect how time is wasted daily. Step 2 (setting goals): the way to set SMART goal was explained to students. Step 3 (preparing task list): the way of prioritizing tasks and preparing to do list according to tasks priority, due date, estimated time needed to achieve, start date and smalls steps needed in every task were explained to students. Step 4 (making schedule): with respect to their semester calendar and their time of most productivity throughout the day. Students practiced making their weekly and daily planner using their preferred method whether simple table or mobile applications. The final step was evaluating the time plan and detecting whether procrastination was an issue. The session time was 35–45 min.
- Session 9 (social media and stress):- the different disadvantages of social media were discussed with students in detail especially on mental health and they asked to assess their drives to use social media and wasted time in social media. The vicious cycle of unhealthy social media use on stress, anxiety, depression, and loneliness was discussed with students. Finally, ways of modifying social media use to was explained by minimizing online time to maximum 30 min, being focused and changing content and finally finding other offline friends and activities. The session time was 20–30 min.
- Session 10 (exercise and stress):- the session discussed the different advantages of exercise on mental health, especially its effect in minimizing stress and anxiety. The WHO recommended physical activity for adults and the recommended steps to start exercising were explained to students. The session time was 20–25 min.
- Session 11 (healthy diet and sleep hygiene):- the session explained the healthy eating plate content, effects of healthy diet on mental health and important nutrients that decrease stress using video demonstrations. In addition, importance and stages of sleep and finally sleep hygiene. The session time was 20–30 min.
- Session 12 was the conclusion session and lasted for 30–40 min. The students completed the questionnaire immediately after intervention (post assessment 1).
The curriculum of stress management sessions applied to the studied students in the intervention group.

Flowchart illustrating the study design process.
Data collection tools
An online administered questionnaire composed of three parts: socio-demographic factors, perceived stress scale, and Beck anxiety inventory.
a. Socio-demographic factors included age, nationality, gender, marital status, residence, academic year, academic achievement in the last year, place of living during studying, whether working beside studying or not, smoking, taking drugs or alcohol, having chronic mental illness, consuming psychiatric drugs within the past 6 months, having chronic neurological illness, and having other chronic medical illness.
b. The Perceived Stress Scale (PSS) is the most widely used psychological instrument for measuring the perception of stress. 15 It was developed by Cohen et al. in 1983 and was intended to measure the degree to which situations in one’s life are stressful. The scale consists of 14 items. Each item is scored on a five-point Likert scale, ranging from 0 to 4, where 0 represents “Never” and 4 represents “Very Often.” However, for items numbered 4, 5, 6, 7, 9, 10, and 13, the Likert scale from zero to 4 is reversed, with 0 representing “Very Often” and 4 representing “Never.” The total score ranges from 0 to 56. Items were summed to determine the level of stress as follows: low level of stress ranged from (0 to 18), moderate level of stress (19–37), and high level of stress (38–56). 16 The validated Arabic version of PSS was used in the present study, 17 and Cronbach’s Alpha was 0.848.
c. Beck Anxiety Inventory (BAI) is a 21-item scale developed by Beck et al. 18 and is broadly used to assess anxiety among students. 11 The rating is done by choosing from four responses that scored respectively from 0 to 3. The total score ranges from 0 to 63. A score of 0–21 indicates low anxiety, a score of 22–35 indicates moderate anxiety, and a score of 36 and above indicates potentially concerning levels of anxiety. 18 The validated Arabic version of BAI was used in the present study, 19 and the Cronbach’s Alpha was 0.919.
Statistical analysis
Data was analyzed using SPSS version 28. First, descriptive data was presented. Quantitative data were expressed as mean and standard deviation, while frequencies and percentages were used to express the qualitative data. Descriptive statistics to compare intervention and control group were performed using the Mann–Whitney U test for continuous measures, chi-square test, and Fishers Exact test for categorical variables.
The quantitative variables (age, academic percentage, the Perceived Stress Scale, and the Beck Anxiety Inventory scale) were assessed for data normality and were not normally distributed (Shapiro-Wilk significance was less than 0.05). The Mann–Whitney U test was used to assess the difference in non-parametric quantitative variables between two independent groups. So, it was used to identify the difference in age and academic percentage between intervention and control. It was also used to assess the difference in Perceived Stress Scale, and Beck Anxiety Inventory scale between the intervention and control at the baseline, immediately post intervention, and 3 months post intervention separately.
The chi-square test and Fishers Exact test were used to compare categorical variables between two independent groups. The chi-square test was used to identify the difference between intervention and control groups regarding academic years, gender, nationality, residence, and place of living during studying. While Fishers Exact test was used to identify the difference between intervention and control groups regarding smoking and drugs/ alcohol intake where one of the cells was less than 5 in frequency.
The approach to the outcome analysis was intention to treat. Missing data were imputed using the last observation carried forward (LOCF). To assess effectiveness of the program on perceived stress and anxiety, Wilcoxon Signed Ranks test and Friedman test were used to assess the significant difference in PSS and BAI at two time and three time points respectively in each group.
The Wilcoxon Signed Ranks test was used to compare nonparametric continuous variables (PSS and BAI) in dependent sample at two time points. So, it was used to compare the difference between perceived stress and anxiety means at the baseline and immediately post intervention in the intervention group and control group separately. It was also used to compare the difference between perceived stress and anxiety means at the baseline and 3 months post intervention in each intervention group and control group separately. Mean difference (immediately post intervention- baseline) and Mean difference (3 months post intervention- baseline) were assessed using paired t-test in each group separately.
The Friedman test was used to compare nonparametric continuous variables (PSS and BAI) in dependent sample at three time points. So, it was used to assess the differences in means of stress and anxiety between baseline and immediately post intervention and 3 months post intervention in each intervention group and control group separately. 20
Results
In the survey, females were 53.2% of the sample and 80% of students were Egyptians. The students’ ages ranged from 17 to 28 years. Nearly two-thirds of the students were in first and second grade (64.9%). Most of the students were single (99.6%). The mean academic percentage (achievement) was 76.1 ± 9.7. More than two-thirds of them were urban residents (76.9%). More than half of them lived with their families during studying (54.6%). Only 7.7% were working besides studying. Most of the students were not smokers and did not take drugs or alcohol (94.2% and 99.6%). A minority of the students studied suffered from mental, neurological, or other chronic medical illnesses (2.7%, 0.9%, and 8.7%, respectively).
The mean scores of the PSS and BAI scales in the survey stage were 31.76 ± 8.63 and 24.19 ± 13.05, respectively. Medical students exposed to moderate to high levels of stress represented 93.2%, while 54.9% were exposed to moderate to high levels of anxiety, as shown in Table 2.
Levels of perceived stress and anxiety among medical students at the survey stage.

Table 3 showed the baseline characteristics of intervention and control groups. There were no statistically significant differences between the intervention and control groups regarding scientific year (p = 1.000), gender (p = 1.000), nationality (p = 0.885), residence (p = 0.408), place of living during studying (p = 0.612), smoking (p = 0.541), taking drugs or alcohols (p = 1.000), age (p = 0.744), academic percentage (p = 0.644), means of perceived stress (p = 0.098), and anxiety (p = 0.397).
Baseline characteristics of the studied intervention and control groups of medical students at Helwan University, 2023.

ºMann-Whitney test.
Chi-square test.
Fishers Exact test.
Table 4 revealed that there was no significant difference between the mean scores of perceived stress between the intervention and control groups before the intervention (25.03 ± 3.18, 24.40 ± 3.15, p = 0.098). There was a statistically significant higher mean score of perceived stress in the control group compared to intervention group immediately post intervention (33.39 ± 9.47, 24.40 ± 3.46, p < 0.001) and 3 months post intervention (33.03 ± 9.40, 23.76 ± 3.37, p < 0.001).
Comparison of the mean scores of PSS pre intervention, immediately post intervention and 3 months post intervention.

p-Valueº: Mann Whitney test.
p-Valueᵀ: Paired t-test.
p-Value1: Wilcoxon Signed Ranks test.
p-Value2: Friedman test.
For the intervention group, there was no statistically significant difference between mean score of stress immediately after intervention (24.40 ± 3.46) compared to before the intervention (25.03 ± 3.18, p = 0.184). However, 3 months post intervention, there was a significant decrease in the mean score of stress (23.76 ± 3.37) compared to before the intervention (25.03 ± 3.18, p = 0.0.004). Mean difference of perceived stress showed statistically significant reduction 3 months post intervention by 1.27 compared to baseline (p = 0.002).
Regarding control group, there was a significant increase in the mean score of perceived stress immediately post intervention (33.39 ± 9.47) compared to before the intervention (24.40 ± 3.15, p < 0.001). Similarly, there was a significant increase in the mean score of perceived stress 3 months post intervention (33.03 ± 9.40) compared to before the intervention (24.40 ± 3.15, p < 0.001). Mean difference of perceived stress showed statistically significant increase immediately post intervention and 3 months post intervention by (8.99, 8.63 respectively) compared to baseline (p < 0.001).
Friedman test showed that there is a statistically significant difference between the mean scores of perceived stress pre intervention, immediately post and 3 months post intervention in both intervention and control groups (p < 0.001and p < 0.001 respectively).
Table 5 revealed that there is no significant difference between the mean scores of perceived anxiety between the intervention and control groups before the intervention (18.44 ± 11.38, 17.36 ± 10.66, p = 397), immediately after (21.19 ± 11.07, 22.88 ± 11.87, p = 0.227) and 3 months post intervention (21.01 ± 11.03, 21.79 ± 10.87, p = 0.513).
Comparison of the mean scores of BAI pre intervention, immediately post intervention and 3 months post intervention.

p-Valueº: Mann Whitney test.
p-Valueᵀ: Paired t-test.
p-Value1: Wilcoxon Signed Ranks test.
p-Value2: Friedman test.
For the intervention group, there was a significant increase in the mean score of anxiety immediately post intervention (21.19 ± 11.07) compared to before the intervention (18.44 ± 11.38, p = 0.046). However, 3 months post intervention, there was no statistically significant difference between mean score of anxiety (21.01 ± 11.03) compared to before the intervention (18.44 ± 11.38, p = 0.063).
Regarding control group, there was a significant increase in the mean score of anxiety immediately post intervention (22.88 ± 11.87) compared to before the intervention (17.36 ± 10.66, p < 0.001). Similarly, there was a significant increase in the mean score of anxiety 3 months post intervention (21.79 ± 10.87) compared to before the intervention (17.36 ± 10.66, p = 0.002). Mean difference of anxiety showed statistically significant increase immediately post intervention and 3 months post intervention by (5.52, 4.43 respectively) compared to baseline (p < 0.001, p = 0.003).
Friedman test showed that there is a statistically significant difference between the mean scores of anxiety pre intervention, immediately post and 3 months post intervention in both intervention and control groups (p = 0.025 and p < 0.001 respectively).
Discussion
Medical studying is difficult and demanding and creates stress and anxiety for medical students. 4 The results of the current study revealed that around 93% of medical students perceived moderate to high levels of stress compared to 69% of medical students in Zagazig University. 1 The higher level of stress in our study can be attributed to several factors: (A) most students come from far places and have to live away from their families or face transportation difficulties. (B) Our newborn faculty had to accept an enlarged number of students although it has a small building and poor facilities. (C) The faculty has two separate and far buildings; the main faculty is in Helwan University while the teaching hospital is in Badr City. (D) The switching from physical to online and hybrid teaching techniques used during COVID-19 pandemic might increase the student’s stress. (E) High academic load and repeated examinations that students suffered during their learning.
Several interventions were used to manage students’ stress. 21 The current study used a comprehensive program in managing stress. The program was effective in mitigating perceived stress for the intervention group. There was a statistically significant higher mean score of perceived stress in the control group compared to intervention group immediately post intervention (33.39 ± 9.47, 24.40 ± 3.46, p < 0.001) and 3 months post intervention (33.03 ± 9.40, 23.76 ± 3.37, p < 0.001). These results can be justified by the acquired knowledge and skills developed by medical students because of the program. The program combined multiple techniques proven to be effective to manage stress such as cognitive therapy, relaxation and mindfulness meditation, and time management. In addition, the acquired knowledge of healthy diet, sleep hygiene, exercise, and modification of social media use which was needed to mitigate stress.
Comparing these results with similar stress management intervention studies. A one group pre/post-test quasi-experimental study was conducted among nursing students at Tanta University. The study used relaxation techniques, time management and cognitive techniques to manage stress. The study revealed that the mean score of the perceived stress scale decreased from 31.130 ± 7.337 pre-intervention to 26.330 ± 4.667 immediately post-intervention with a highly statistically significant difference (p = 0.001). 22 Likewise, cognitive, and behavioral stress management intervention was effective in decreasing stress of nursing students in the intervention compared to control group immediately post and 1 month post intervention compared to baseline. 23
Furthermore, mindfulness-based training programs were proven to be effective in decreasing stress and burnout of medical students. 24 An Australian study revealed that online mindfulness mediation was effective in decreasing perceived stress of medical students; PSS scores were significantly reduced at 4-month follow-up, compared to baseline by two points, CI −3.9, −0.1. 25
Among the important sources of medical students perceived stress is time related demands such as increasing academic workloads and time pressure. 26 Teaching and practicing time management rules, such as setting goals, prioritizing tasks, handling study periods, preventing procrastination, and making time for other duties, is an essential component to manage students stress. 27 Time management training program was effective in decreasing perceived stress of undergraduate students and the trainees reported less perceived stress 2 and 4 weeks after time management training compared to the pretest before training. 28
Regarding the effects of the current study program on anxiety. There was no statistically significant difference in anxiety scores between intervention and control group, neither pre- immediately post or 3 months post intervention. For the intervention group, there was no statistically significant increase in mean difference in the anxiety level immediately post intervention and 3 months post intervention compared to the baseline. While in the control group, mean difference of anxiety showed statistically significant increase immediately post intervention and 3 months post intervention by (5.52, 4.43 respectively) compared to baseline (p < 0.001, p = 0.003). This indicates that the program was effective in preventing increasing anxiety in the intervention group.
Comparing these results with other studies. A previous stress management program based on cognitive therapy and relaxation techniques was conducted among nursing students. It revealed lower means of anxiety in the intervention group compared to control group immediately after and 1 month after intervention (p = 0.001, 0.029 respectively). 23 Another online mindfulness-based intervention was in effective in decreasing anxiety of Italian medical students however it was effective in decreasing stress, overall distress and improving emotional regulation and resilience of the trained students. 29
Stress management interventions were not limited to research and were applied as a separate course in medical education. An elective course named mind body course was offered at the University of Washington School of Medicine students. The course covered theoretical and practical skills related to stress response, meditation, imagery, exercise, nutrition, genograms, and spirituality. The course was effective to decrease anxiety in the enrolled medical students compared to the comparison subjects and such decreases in anxiety were sustained 3 months after the course ended. 30
Limitations of the study
- The study has the following limitations:
(a) It was conducted in a single medical college that may decrease the generalizability of its results to all medical students across Egypt.
(b) No objective measures so liability to response bias: The study relies solely on psychometric tools, with no physiological data (e.g. cortisol levels) to validate findings.
(c) The results are limited to 3 months post-intervention, leaving long-term effects unknown.
(d) Lack of qualitative insights: While the intervention involved interactive sessions, no qualitative data was reported to complement the findings.
Conclusions and recommendations
The current study used a comprehensive stress management intervention including diverse and practical techniques targeting multiple stress dimensions in medical students. The levels of stress and anxiety were assessed using psychometric scaled (PSS and BAI respectively), immediately after and 3 months after intervention in both intervention and control groups. The program was effective in decreasing the level of stress and preventing increasing anxiety in the intervention group. Incorporating stress management programs within the courses of medical education is highly recommended. Future mixed-methods research focusing stress management among Egyptian medical students with longer follow up period is required. Incorporating qualitative data collection to complement the quantitative findings will explore the potential impacts of Egypt’s cultural, social, or economic factors on medical students’ perception of stress and anxiety.
Implications for the field of public health
Medical students stress has damaging impacts on their physical and mental health. The current study objective was to assess the effectiveness of stress management intervention on perceived stress and anxiety of medical students. The widespread implementation of the study program in medical faculties can help medical students to cope with stress and anxiety. As a result, medical students can maintain their mental health and wellbeing throughout their academic journey and future professional careers.
Footnotes
Acknowledgements
The authors gratefully thank all medical students who participated in the current study. Special thanks to the medical students Esraa Amr Mohamed Hany, Sohaila Osama Khalaf Mohamed for helping in organizing and dissemination of the stress management program online sessions.
Ethical considerations
Approval to conduct the study was obtained before starting the data collection via the Research Ethics Committee for Human and Animal Research at Helwan University, Faculty of Medicine (approval code 16-2022 date 21/2/2022). Official approval was obtained from the administrative authority of the Faculty of Medicine at Helwan University.
Consent to participate
Informed consent was obtained from the study participants themselves prior to submitting their responses to the questionnaire. Privacy and confidentiality of all data were assured by ensuring the anonymity of the questionnaire and keeping data files in a safe place. The material of the stress management program was sent online through e mails to the control group after completion of the study.
Consent for publication
Not applicable.
Author contributions
OSE contributed to the study design, collected, analyzed, interpreted the data, and prepared the main manuscript. HAS contributed to the study design, analysis, interpretation of the data, and revision of the manuscript. SR suggested the research problem and contributed to the study design, analysis, interpretation of the data, and revision of the manuscript. AAG contributed to the study design, analysis, interpretation of the data, and writing and revising the manuscript. All authors approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets that were generated and analyzed during the current study are available from the corresponding author upon reasonable request.