
Abstract
This study planned to assess the prevalence and associated factor of perceived stigma among caregiver of patient with mental illness in Ethiopia. The Design of this study is a systematic review and meta-analysis. We searched from database PubMed, Google Scholar, and CINAHL and studies available from inception to August 2024. The quality of eligible studies was assessed using Newcastle-Ottawa Scale (NOS). A DerSimonian-Laird random-effects meta-analysis was used to estimate the pooled effect size of the outcome measures with their 95% CI. Stata version 14.0 (StataCorp, College Station, Texas, USA) was used for statistical analysis. A total of five studies reported the prevalence of perceived stigma among caregivers of patients with mental illness. The pooled prevalence of perceived stigma was 65% (95% CI: 41%–88%), with high heterogeneity (I² = 99.6%, p < 0.001). Longer caregiving duration (2.08, 95% CI: 0.87–3.29), and poor social support (4.20, 95% CI: 2.30–6.11) were associated with perceived stigma. Perceived stigma among caregivers of patient with mental illness is high in Ethiopia. The prevalence of perceived stigma prevalence varies across regions. Addressing perceived stigma among caregivers of individuals with mental illness in Ethiopia should be a priority for mental health services and policy makers.
Introduction
Mental illness is one of the most difficult life problems today. A wide range of mental disorders including schizophrenia, depressive disorders, anxiety disorders, bipolar disorder, autism spectrum disorder, conduct disorder, attention deficit hyperactivity disorder (ADHD), eating disorders, idiopathic developmental intellectual disorders, and other residual categories are recognized as a global burden of disease. 1 These conditions contribute heavily to the global disease burden, particularly in developing countries. 2 Similarly, the prevalence of mental illness in Ethiopia is notably high. 3 Mental illness is a lifelong condition that often necessitates continuous family caregiving. This caregiving can take many forms informational, practical, and emotional and is beneficial both to individuals with mental illness and to their caregivers. 4 In this context, caregivers play a pivotal role, providing essential support that fosters recovery and helps navigate everyday challenges. 5
One common challenge in providing care for any illness is stigma. However, stigma surrounding mental illness is particularly severe and affects not only the individuals living with mental illness but also those around them or their caregivers.6–8 In particular, caregivers often experience perceived stigma. 8 Perceived stigma refers to their sense of how others view them due to their association with mental illness. 9 Caregivers often experience feelings of rejection from the community when they have a family member living with mental illness. 10 This type of stigma is pervasive across societies and cultures worldwide. 9 In China, for example, high levels of perceived stigma among caregivers have been documented, 11 while nearly half of respondents in Nepal report experiencing significant stigma. 12 In countries such as India,9,13 Africa like Egypt and notably in Ethiopia 14 caregivers of individuals with mental illness encounter high levels of stigma. 15
Caregivers of individuals with mental illness often face more intense societal stigma compared to those caring for individuals with chronic dermatological conditions. 11 This stigma extends beyond the patients themselves it deeply affects the caregivers as well. The psychological burden associated with perceived stigma can lead to emotional distress 16 and is strongly linked to declines in caregivers’ physical, psychological, and environmental quality of life. 17 The connection between perceived stigma and caregiver distress is significant, often contributing to increased psychological morbidity. 18 Furthermore, stigma serves as a barrier to timely treatment, hinders adherence to care plans, and elevates the risk of relapse among individuals with mental illness.8,19,20
Several factors contribute to the perceived stigma experienced by caregivers of individuals with mental illness. A lack of understanding about mental health conditions and fear surrounding societal judgment play a significant role in perpetuating stigma. 8 It also differ based on caregivers’ demographic characteristics, with higher levels observed among those who are illiterate compared to those who are literate.21,22 Perceived stigma was associated with being a married caregiver, 21 lack of formal education,13,23 and lack of social support and the sex of the caregiver, 21 especially being female was linked to perceived stigma. 14 In addition caregiver with low income and elder caregivers of mental illness experience high level of perceived stigma. 13 Caregivers of individuals with mental illness who attributing schizophrenia to hereditary causes, caregivers who have daily contact with the patient and burden scores are associated with higher stigma. 22
In addition, caregiving burden, 24 social support and avoidance coping associated with perceived stigma of caregivers. 25 Additionally, caregivers may feel rejected by their community due to their association with mentally ill patients and this perceived stigma influences various aspects, including healthcare facility usage and support for mentally ill relatives. 10
Research conducted in Ethiopia highlights a significant prevalence of perceived stigma among caregivers of individuals with mental illness. For instance, studies revealed that perceived stigma rates reach 89.3% in Bahir Dar, 14 54.7% in Jimma, 26 38.5% in Addis Ababa, 27 and 42.5% in the Harari Region. 23
The significant occurrence of perceived stigma among caregivers of individuals with mental illness underscores the urgency of implementing targeted interventions and support services to address the perceived stigma of this vulnerable group. Gaining insights into the pooled prevalence and associated factors of perceived stigma among caregivers is essential for designing effective strategies to enhance their mental well-being and elevate the overall quality of care provided to individuals with mental illness. Although, some individual studies in Ethiopia showed the prevalence of perceived stigma and its associated factors among caregivers of patient with mental illness, to date, their findings were not reported in comprehensive way. Based on this consideration, this meta-analysis and systematic review assesses the pooled prevalence the perceived stigma and associated factor of caregivers of patient with mental illness in Ethiopia.
Objectives
This study assesses the pooled prevalence and associated factor of perceived stigma among caregiver of patient with mental illness in Ethiopia.
Materials and methods
Protocol registration
This study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020) checklists. It has been registered with Prospero (ID: CRD42024581201).
Search strategy
We searched databases including PubMed, Google Scholar, and CINAHL published from inception to August 2024. Systematic searches were conducted by combining every possible predefined search term determined by Medical Subject Headings (MeSH) and keywords. To make the search effective, we used keywords such as “magnitude,” “epidemiology,” “prevalence,” “perceived stigma,” “associated factor,” “risk factors,” “determinant,” “predictor,” “caregivers,” “informal caregiver,” “mental illness” and “Ethiopia.” We used Boolean operators AND and OR. The full search strategies are presented in Supplemental Table 1. The duplicates from the searched results were removed by using endnote reference manager. Four researchers were screened the studies by title and abstract and the discrepancy were solved by discussion.
Eligibility criteria
Inclusion criteria
This study exclusively included observational research that explored the prevalence and contributing factors of perceived stigma among caregivers of individuals living with mental illness in Ethiopia. To simplify the searching strategy and organization of search terms, this study is employed following the condition, context and population (CoCoPop) framework.
Exclusion criteria
Randomized controlled trail, systematic review and meta-analysis, studies without full access, studies that do not have statistical data which is suitable for meta-analysis, studies conducted on other caregivers (caregivers of physical disease) were excluded.
Outcome measures
This study has two outcomes. The primary outcome was the pooled prevalence of perceived stigma among caregivers of patient with mental illness in Ethiopia. The second outcome of the study is factors associated with perceived stigma among caregivers of patient with mental illness in Ethiopia.
Selection of studies
Two researchers (GEM and ADW) evaluated the studies based on eligibility criteria. Initially, they assessed the titles and abstracts of the studies from the searched databases. Full-text screening was then conducted to review the complete texts. The disagreement was solved by discussion with the third party. Besides, we have a rationale for inclusion and exclusion of studies in the PRISMA diagram. Finally, the final list of studies for data extraction for systematic review and meta-analysis was arranged for the analysis.
Data extraction
The data extraction was independently extracted by two researchers individually (GEM and ADW) using the data extraction format of Microsoft Excel. Double check was made by other two authors (ECT and AAH). Disagreements were handled by discussion. The data extraction contain the author’s last name, year of publication, region, and study design, number of cases, sample size, sampling design, instrument, study population, relation with care recipient, care recipient age and prevalence and associated factors with their odds ratio.
Quality appraisal
Newcastle-Ottawa Scale (NOS) quality appraisal was adapted to assess the methodological quality of included studies. 28 According to this method the quality score is less than 5, it is considered low quality; if the quality score ranges from 5 to 7, it has moderate quality; and more than 7 scores indicate high quality and moderate and above quality studies were included in this meta-analysis and systematic review. Two independent authors conducted the quality assessment (ADW and GEM). Three additional authors (AAS, AAH and ECT) confirmed it.
Data synthesis
The data was extracted in Microsoft Excel were imported to Stata version 14.0 (StataCorp, College Station, Texas, USA) to analysis the whole meta- analysis. DerSimonian-Laird random-effects meta-analysis was used to estimate the pooled prevalence along with 95% confidence interval. 29 Assessment of heterogeneity was checked by I2 and Cochran’s Q-statistics30,31 Subgroup analyses were performed by regions, year of publication and sampling methods used in individual studies to decide the source of heterogeneity. Publication bias was checked by DOI plot and Luis Furuya Kanamori (LFK) and Egger’s test. The DOI plot and the LFK index tools were used to determine asymmetry of studies, with small number of studies.32,33 According to the LFK index, a value outside the interval -1 and 1 is considered as asymmetry (i.e. publication bias). 33 To assess the small study effects the leave one out sensitivity analysis is used.
Results
A PRISMA chart addressing the means of data search and refining process for the concentrate on prevalence and associated factor for perceived stigma among caregivers of patients with mental illness in Ethiopia displayed in Figure 1. From databases search, initially 246 studies were identified. Due to duplication, 43 studies were removed. Fifty-one studies were screened and full text studies were examined. 46 studies excluded by their title and abstract. Finally, we recognized five studies appropriate to this systematic review and meta-analysis.

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart.
Study characteristics
In this systematic review and meta-analysis, we included five cross-sectional studies with a total of 2119 participants. The following studies were included.14,23,27,34,35 Specifically, two studies were conducted in Addis Ababa27,36, one in Harari, 23 one in Amhara 14 and one in Oromia. 35 The summarized data on key characteristics from the included studies is presented in Table 1.
Study characteristics and quality of the included studies for prevalence and associated factors of perceived stigma among caregivers of patients with mental illness in Ethiopia.

FIS: family interview schedule; FQ: family questionnaire; n: sample size.
Risk of bias assessment
The risk of bias of eligible study was assessed by using Newcastle Ottawa scale (NOS), which is appropriate for cross-sectional studies quality assessment showed in Table 1. We considered moderate quality, and high quality studies for this review.
Publication bias
Publication bias was assessed by the DOI plot, a tool used to visualize asymmetry and by the LFK index, 33 a tool used to detect and quantify asymmetry of study effects. As showed in Figure 2, there is no asymmetry’ (LFK index = 0.12). In addition the insignificant value of egger test (p = 0.095) indicate that there is no publication bias is observed.

Assessment of publication bias of included studies.
Sensitivity analysis
In this study leave one out sensitivity analysis is used. It is a method used to evaluate the impact of omitting one data point on the overall results of a statistical analysis. As shown in Figure 3, the leave one out meta-analysis there is no outshining pooled estimate after removing one out, indicates that there is no small study effects in the meta-analysis. This can provide confidence in the reliability of the analysis results findings and no potential sources of bias or error in the data.
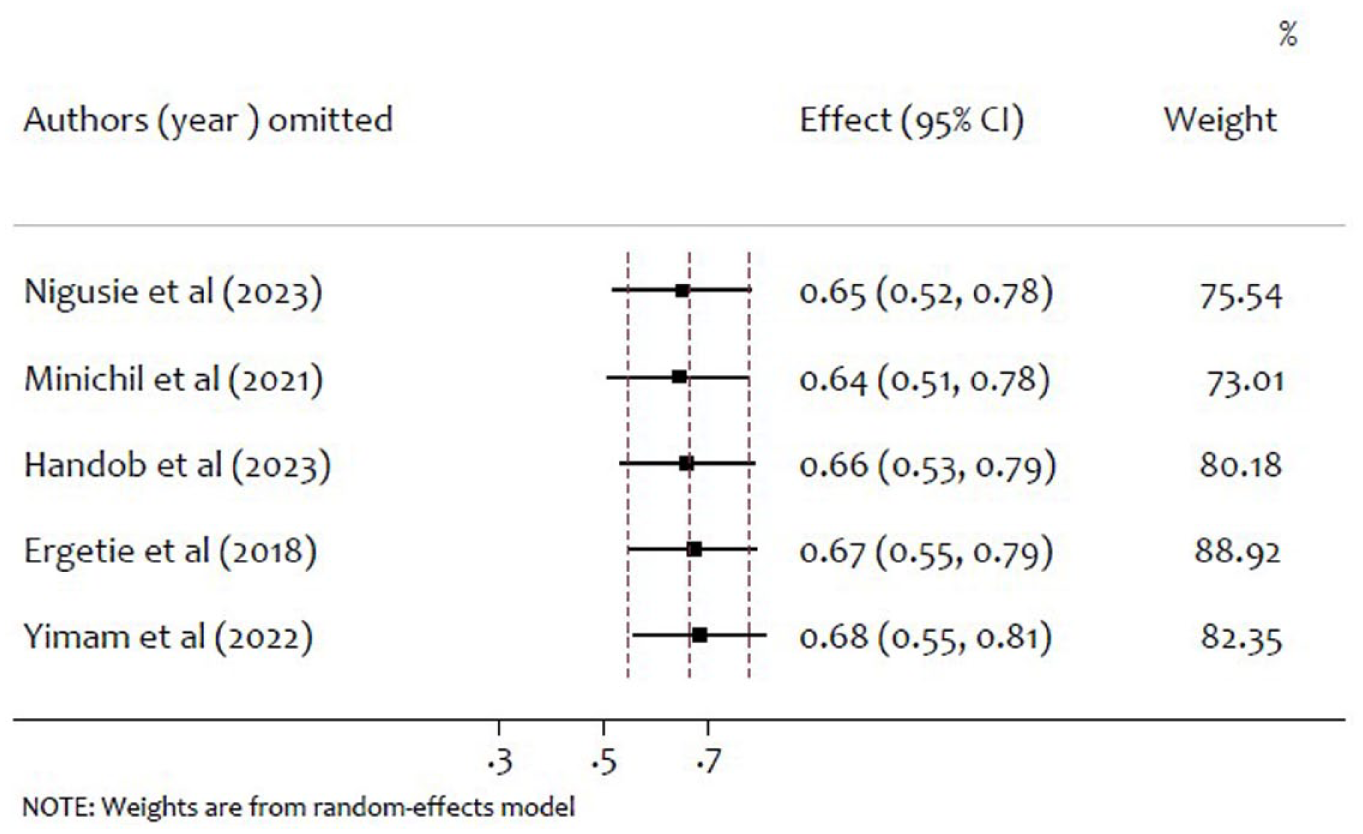
Leave-one-out sensitivity analysis.
Pooled prevalence of perceived stigma among caregiver of patient with mental illness
A total of five studies include reported the prevalence of perceived stigma, and the pooled prevalence of perceived was 65% (0.41, 0.88), I2 = 99.6%, p < 0.001; Figure 4). Therefore there is a substantial heterogeneity among study prevalence of prevalence of perceived stigma.

Forest plot for the prevalence of perceived stigma among caregivers of patients with mental illness.
Subgroup analysis of perceived stigma by region
Since high level of heterogeneity found in our included studies, a sub group analysis was conducted based on region, sampling method, tool or instrument and year of publication (Table 2). The prevalence of perceived stigma in Ethiopia is not homogeneous across regions (Q = 487.89, df = 3, p < 0.001). The prevalence of perceived stigma in Harari was 43% (0.38, 0.47), Addis Ababa 47% (0.31, 0.63), Amhara 89% (0.87, 0.92) and Oromia 97% (0.96, 0.99). The highest levels of perceived stigma were observed in Oromia, followed by Amhara and Harari, while Addis Ababa reported the lowest prevalence.
Subgroup analysis of perceived stigma and assessment of heterogeneity among subgroups.

df: degree of freedom; FIS: family interview schedule.
Subgroup analysis of perceived stigma by publication year
From the subgroup analysis by publication year (Table 2), the prevalence of perceived stigma among caregivers of patients with mental illness was 89%, 39%, 97%, and 49% in the years of 2018, 2021, 2022, and 2023, respectively. The heterogeneity test result among the groups (Q = 711.91, df = 3, p < 0.001).This indicates that there is heterogeneity in years of publication on the prevalence of perceived stigma.
Subgroup analysis of perceived stigma by sampling methods
The subgroup analysis using sampling method used (Table 2) the pooled prevalence of perceived stigma in study using sampling methods: systematic sampling was 57% (29%, 84%), consecutive sampling 0.97 (0.96, 0.99). The heterogeneity test among group (Q = 8.38, df = 1, p < 0.05) and therefore it indicated that there is statistically significant heterogeneity among sampling methods.
Subgroup analysis of perceived stigma by tool or instrument
The subgroup analysis based on tools, the pooled prevalence among caregivers as measured by FIS tool, Devaluation of Consumer Families Scale, Family stigma scale and family questionnaires was 66%, 39%, 55% and 97% respectively. The heterogeneity test among group indicated that there is a significant heterogeneity among tools or instrument
Associated factors of perceived stigma and pooled effect size
This study also report factors associated with perceived stigma among caregivers of patient with mental illness in Ethiopia Table 3. Specifically, longer duration of caregiving, admission history, and poor social support were linked to higher levels of perceived stigma. In our included studies reported that individuals with poor social support,14,23,27 and long caregiving duration23,26 were more likely to develop perceived stigma. The odds of experiencing perceived stigma were 2.08 times higher for those with longer caregiving duration compared to the short duration. Conversely, caregivers with poor social support had a 4.20 times higher likelihood of developing perceived stigma. Moreover, due to a lack of studies to assess pooled effect size, we summarized the factors that affect perceived stigma (Table 4).
Pooled AOR for associated factors of perceived stigma among caregivers of patient with mental illness in Ethiopia.

AOR: adjusted odds ratio; CI: confidence interval.
Summary review of significant associated factors of perceived stigma among caregivers of patient with mental illness in Ethiopia.

AOR: adjusted odds ratio; CI: confidence interval.
Discussion
To the best of our knowledge, this systematic review and meta-analysis is the first of its kind to assess the pooled prevalence and associated factors of perceived stigma among caregivers of patients with mental illness in Ethiopia. A total of 5 studies involving 2119 caregivers of individuals with mental illness were included. The pooled prevalence of perceived stigma was found to be 65%. Our finding is notably higher compared to other studies for instance, one reported a prevalence of 25.65% 38 and, another presented a medium level of perceived stigma with a mean score of 15.8 ± 2.8, 33 and yet another described mild to moderate level 39 and It also exceeds the findings of a study that reported 57% of caregivers experiencing stigma. 40 The prevalence is also considerably higher than rates found in research conducted in Nepal. 12 The level of perceived stigma in Ethiopia is notably higher compared to other middle-income countries. For example, a study conducted in India reported that approximately 44% of respondents experienced high stigma, while 36% reported low stigma levels. 6 In contrast, Agrasuta and Pitanupong 41 found that the majority of caregivers in their study 62% reported low perceived stigma, with only 0.6% experiencing high levels. These variations may indeed stem from cultural differences, sample sizes, or measurement approaches. 41
Subgroup analysis indicated that the prevalence of perceived stigma among caregivers was 43% in Harari, 47% in Addis Ababa, 89% in Amhara, and 97% in Oromia. The highest prevalence was observed in Oromia. This elevated rate of perceived stigma may be attributed to inadequate awareness and limited understanding of mental illness within the region. 42 Additionally, the lack of specialized mental health hospitals outside Addis Ababa may contribute to this heightened stigma. Cultural differences and demographic factors also likely contribute to regional variations in stigma levels. Age is another influential factor individual between the ages of 26 and 33 report higher levels of perceived stigma. Moreover, married caregivers tend to experience greater stigma compared to their unmarried or single counterparts. These findings align with previous research showing that individuals aged 34 and younger tend to report higher levels of perceived stigma. 13
Among the associated factors, longer durations of caregiving (OR = 2.08; 95% CI: 0.87–3.29) and lack of adequate social support (OR = 4.20; 95% CI: 2.30–6.11) were significantly linked to increased stigma. Consistent with the findings of the present study, Perlick et al. 25 found that social support and avoidance coping explained 63% of the relationship between caregiver stigma levels. Caregivers who provide long-term care are 2.08 times more likely to experience stigma compared to those with shorter caregiving durations. Similarly, a study from India found that caregivers who had been providing care for extended periods exhibited higher levels of perceived stigma. 6 Additionally, our study found that individuals without formal education exhibited a stronger association with perceived stigma compared to those with college-level education or higher. This finding aligns with previous research, which similarly reported elevated stigma levels among illiterate caregivers. 22 The consistency across studies may be attributed to the role of education in shaping awareness, understanding, and attitudes toward mental illness—higher educational attainment among caregivers appears to be linked to reduced stigma scores. 13 Moreover, caregivers who did not hold supernatural beliefs about mental illness were less likely to experience stigma than those who did a finding consistent with the study by Farah et al. 22 findings. This may be attributed to limited understanding and negative attitudes commonly associated with supernatural explanations.
When considering residential differences, caregivers from rural areas reported higher levels of perceived stigma compared to those living in urban settings, aligning with findings from an Indian study. 13 Limited access to mental health information through media and public awareness campaigns in rural regions may contribute to this disparity. Additionally, caregivers providing care for their spouses were found to experience particularly high levels of perceived stigma. 6
Female caregivers consistently reported higher levels of perceived stigma compared to their male counterparts,21,43 a pattern that may be influenced by culturally embedded gender roles and societal expectations. 21 In addition, individuals who rejected supernatural beliefs about mental illness exhibited lower levels of stigma than those who endorsed such explanations. 20 This finding is supported by findings from Kumar et al., who identified a significant positive correlation between strong supernatural beliefs and heightened stigma levels. Furthermore, caregivers residing in rural areas were more likely to experience high levels of perceived stigma relative to those in urban settings, indicating that geographic location and cultural context may play a substantial role in shaping stigma perceptions.
Clinical and practical implications
This national systematic review and meta-analysis reveals a high prevalence of perceived stigma among caregivers of individuals living with mental illness in Ethiopia. The findings underscore the urgent need for targeted interventions within clinical and community settings.
Conclusion
Caregivers of individuals with mental illness in Ethiopia experience a significant level of perceived stigma. Factors such as lack of social support, poor knowledge about mental illness, and internalized stigma contribute to the perceived stigma experienced by caregivers. Addressing perceived stigma among caregivers of individuals with mental illness in Ethiopia should be a priority for mental health services and policy makers.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251385275 – Supplemental material for Prevalence and associated factors for perceived stigma among caregivers of patients with mental illness in Ethiopia: A national based systematic review and meta-analysis
Supplemental material, sj-docx-1-phj-10.1177_22799036251385275 for Prevalence and associated factors for perceived stigma among caregivers of patients with mental illness in Ethiopia: A national based systematic review and meta-analysis by Asalfew Damtew Wolde, Gezahegn Eshetu Mamed, Abubeker Alebachew Seid, Eshetu Chekole Tadesse and Aragaw Asfaw Hasen in Journal of Public Health Research
Footnotes
Acknowledgements
We acknowledge authors of studies included in this systematic review and meta-analysis.
Abbreviations
Author Contributions
ADW was involved in systematic searching, selection of studies, quality assessment, and review of articles, data analysis and approval of the final draft. GEM contributed to systematic searching, selection of studies, quality assessment of the included studies, and review of articles. ECT was involved in the approval of the final draft, quality assessment and confirmation, and study selection. AAS took part in systematic searching, selection of studies, quality assessment and confirmation, and review of articles. AAH participated in systematic searching, selection of studies, quality assessment and review of articles, data collection, data analysis and the approval of the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.