
Abstract
Background:
The study investigates Chinese healthcare professionals’ attitudes toward patient-initiated audio-recordings of medical consultations, a growing practice aimed at improving patient comprehension, while also presenting legal, ethical, and clinical challenges.
Design and methods:
A cross-sectional survey was conducted from March to September 2022 as a pilot study. Physicians from various specialties across China were invited to complete an anonymous online questionnaire. The survey assessed demographic data, attitudes toward patient-led recordings, and the reasons behind these attitudes. Statistical analyses, including chi-square and Fisher’s exact tests, were applied to identify significant differences, with a p-value of <0.05 considered statistically significant.
Results:
Out of 968 valid responses, 36.8% of physicians supported patient-initiated recordings, while 63.2% were opposed. Significant differences were observed based on gender, age, years of practice, and professional title, but not on education level or hospital type. Supporters cited enhanced communication and respect for patient autonomy as key reasons, while opponents expressed concerns about potential legal risks, reduced medical efficiency, and damage to trust in the doctor-patient relationship.
Conclusions:
The majority of participating physicians in our study remain cautious about patient-initiated recordings, reflecting a need for clearer regulatory frameworks and protections. This caution highlights the complexity of balancing patient engagement with the practicalities of clinical work.
Practice implications:
Establishing standardized guidelines and offering training for healthcare professionals on managing recorded consultations could alleviate concerns and foster a more collaborative doctor-patient relationship.
Keywords
Introduction
Communication between physicians and patients is vital for shared medical decision-making. Research on enhancing communication, including language use, information delivery, and emotional exchange, can improve treatment outcomes and foster trust between physicians and patients. The treatment process often requires detailed discussions about options and prognosis, which may overwhelm patients, highlighting the need for better communication during shared decision-making. Kessels RP’s research found that 40%–80% of medical information given by healthcare providers is immediately forgotten by patients, 1 with the amount forgotten increasing with age. 2 Additionally, the more information provided, the more likely patients are to forget key details, 3 leading to wasted resources and decreased treatment efficiency. Studies initiated by Butt and later conducted by Johnson and Adelstein suggest that providing patients and their families with audio recordings of consultations can enhance patient adherence and improve consultation efficiency.4–6 This is especially important in fields like emergency medicine, critical care, and oncology, where decisions often involve complex, multi-disciplinary care. 7 With the rise of smartphones, patients can now easily record their visits. As telemedicine grows, recording these conversations is crucial, especially when family members can’t attend appointments. 7 Documenting consultations also promotes efficient communication between physicians and supports evidence-based medicine by sharing decisions and evidence. 8
The implementation of a physician-led documentation process clearly enhances the effectiveness and efficiency of treatment. However, introducing a patient-led documentation process brings new complexities. With advancements in technology, particularly the widespread use of smartphones, recording devices are now more common. Among the ethical issues in doctor-patient relationships, the practice of openly or covertly recording consultations is becoming a central topic of public debate. Barr et al. were the first to examine the prevalence of patient-initiated clinical audio and video recordings in the United States, revealing that about one-third of surveyed clinicians had recorded consultations for patients’ personal use. 9 Research by Elwyn et al. found that approximately 69% of UK patients wanted to record their consultations, while 46% either preferred or had already created a confidential record. 10 In China, reports indicate that over 70% of interviewed physicians have been audio or video recorded during consultations. 11 If physicians alter their communication style due to being recorded, it could influence medical practices. A qualitative analysis by Tsulukidze et al. showed that unauthorized patient-initiated recordings can significantly affect doctor-patient communication, potentially damaging trust, causing conflict, and leading to defensive medical behavior. 4
There has been limited research on attitudes toward recording doctor-patient conversations, and regulations governing audio recordings and related practices remain incomplete. The vague definition of rights and interests weakens the effectiveness of existing regulations, and their practical application is often challenging. 12 Previous studies have largely focused on oncology,2,3,5,6 with a significant portion based on patient surveys, while few have centered on general medical professionals. Additionally, most studies related to attitudes toward recorded conversations have small sample sizes and are limited by their specific study populations. 12 Many studies are set within particular clinical contexts,11,13 limiting the generalizability of the results. Furthermore, findings from international research may not be fully applicable to local settings, and few studies have been initiated directly by clinicians or medical students.
This study addresses the attitudes of healthcare professionals toward patient-initiated recording of doctor-patient conversations from their perspective. It seeks to obtain relatively more realistic and representative findings by enlarging the sample size and to identify factors related to influences and attitudes.
Methods
Research design
This observational cross-sectional survey aimed to investigate the attitudes of medical professionals toward the recording of conversations led by patients or family members during the communication of medical conditions as a pilot study.
Research participants
Inclusion criteria for this study were (1) currently practicing physicians and (2) informed consent, understanding and willingness to cooperate with this study.
Questionnaire design
A team of emergency medicine specialists, biomedical researchers, hospital administrators, and medical ethicists conducted a literature review on doctor-patient communication. They then developed the “Survey on Medical Professionals’ Attitudes Towards Recorded Conversations” through roundtable discussions, refining the wording of the questions (Supplementary File 1). The questionnaire collected respondents’ personal information, including sex, age, education, years of medical practice, professional title, workplace location, hospital level, and department. Additionally, it gathered general information along with the medical staff’s attitudes toward recorded conversations and the reasons behind their choices. To improve the quality of the answers, 10 physicians were enrolled in a pilot study to evaluate the platform used and item comprehensibility.
Questionnaire distribution and collection
The questionnaire was completed anonymously and clearly stated the purpose of the study while providing instructions for completion. Medical professionals independently filled out the questionnaire, and the completed surveys were collected automatically by the platform. Convenience sampling and snowball sampling methods were used, and the questionnaire was distributed via social media using a link to the SoJump survey platform (https://www.wjx.cn/wjx/design/previewmobile.aspx?activity=153039827&s=1). After the questionnaire collection period, the data was exported as an Excel spreadsheet from the platform.
Sample size and statistical analysis
The sample sizes of previous similar studies varied widely from 91 to 360 participants.7,14 Discussions were held with statistical expert (HZ), and the minimum sample size for this study was formulated to be at least 10 times the number of questions. Quantitative data were described using the median and interquartile range (IQR), while categorical data were described using the count (percentage). Inter-group comparisons were performed using the chi-square test or Fisher’s exact test. Analysis was done using IBM SPSS Statistics for Windows (Version 29.0.2.0 Armonk, NY: IBM Corp). The questionnaire content was then imported into Lumivero (2023) NVivo (Version 14) and was systematically organized item by item, followed by thematic analysis and coding. The textual information was compared and analyzed to extract themes and high-frequency words. A p value of <0.05 was considered statistically significant.
Research ethics
The study was reviewed and approved by Peking University Third Hospital Institutional Review Board (IRB-2021-493). Informed consent for the study was obtained electronically and respondents agreed to participate in the survey before reading the questionnaire further.
Results
The survey was conducted from March 17, 2022, to September 13, 2022. A total of 977 questionnaires were collected, with 971 respondents agreed to participate in follow-up studies. After excluding incomplete questionnaires, a total of 968 were included in the final analysis.
Demographic information/characteristics
The respondents’ ages ranged from 22 to 86 years, with a median age of 35 (IQR 30–42) years. Of the respondents, 402 were male (41.4%) and 568 were female (58.6%). The length of work experience varied from 0.5 to 61 years, with a median of 10 (IQR 5–17) years. There were 338 residents (34.9%), 367 attendings (37.9%), and 263 senior faculties (27.2%). 647 (66.6%) had a bachelor’s degree. A total of 801 respondents (82.7%) worked in tertiary hospitals, 127 (13.1%) in secondary hospitals, and 40 (4.1%) in primary hospitals. The respondents were from 30 out of 34 provincial administrative regions (excluding Qinghai Province, Macau, Hongkong and Taiwan due to accessibility constraints), representing 88% of provincial administrative divisions.
Attitudes of medical staff toward recorded conversations
Among the 968 medical professionals surveyed, 356 (36.8%) expressed willingness to accept recorded conversations by patients or family members, while 612 (63.2%) did not. The two groups differed significantly in terms of gender, age, years of medical practice, and professional title, while there were no significant differences in education level, hospital level, average weekly working hours, department, or whether they had received training in doctor-patient communication. A description of respondent characteristics can be found in Table 1.
Sample characteristics and demographics (n = 968).
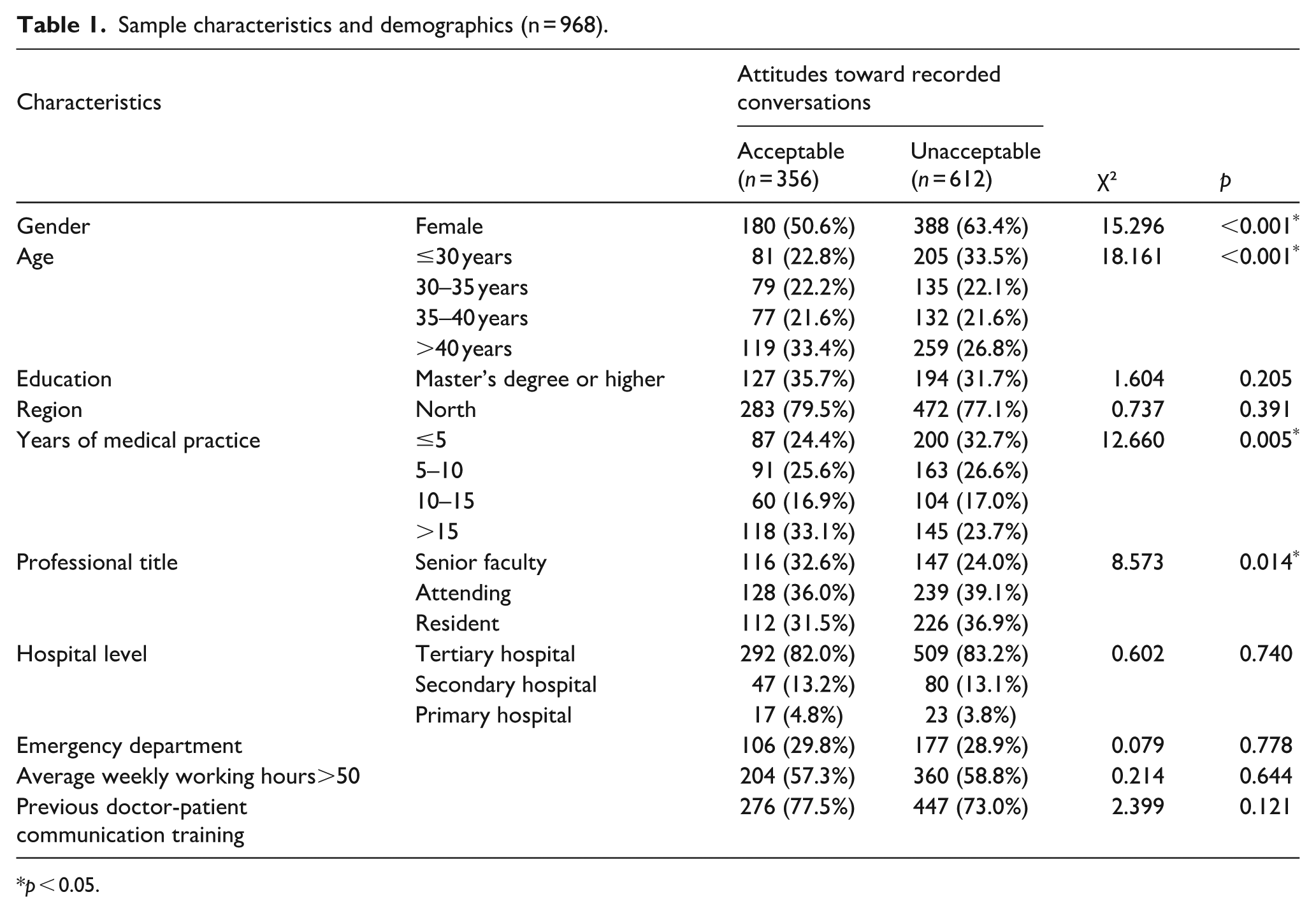
p < 0.05.
Analysis of the reasons for the different attitudes of physicians toward patient-initiated recorded conversations
Facilitates communication of medical conditions
There were 365 (36.8%) physicians receptive to the idea of recorded conversations. Their main motivations were to improve doctor-patient communication, ensure the accurate transmission of medical information, and facilitate more efficient shared decision-making. They were more attentive to the needs of patients and their families and were able to empathize with and understand any anxiety or distress they might have experienced. They hoped that the recordings could offer comfort and support to patients and their families. For more quotes, please see Supplementary File 2.
Sometimes it was challenging to immediately comprehend the doctor’s explanations. Listening to the recordings later and discussing them with other family members helped them make better judgements. (Respondent 29) Respects the family’s trust in the physician and also provides emotional stability for the family members. (Respondent 183)
Patients’ rights
Among the physicians who agreed to be recorded and provided reasons, 12.2% believed that recording is a patient’s right. They asserted that patients have the right to be informed and the freedom to record within legal limits.
Legitimate and justified claims within the bounds of the law. (Respondent 3) Patients have the right to be informed and to exercise their freedom. (Respondent 243)
Physicians’ self-perceived expertise
Some physicians were optimistic and confident in their own knowledge and doctor-patient relationship. They believed that patient-initiated recordings would not affect the medical process or outcomes, so they didn’t mind if patients or their families recorded the conversations.
I believe that doctor-patient communication should be thorough and without any gaps. (Respondent 6) My professional level can stand the test. (Respondent 674)
Physicians believed that they should be notified prior to recordings and that additional safeguards are required
Most of the physicians who agreed to being recorded and provided reasons (42.3%) suggested that certain prerequisites should be in place. These include openness and transparency, stricter safeguard measures such as mutual consent, improvements in social security systems, and the development of relevant hospital infrastructure. Some physicians who disagreed with patient-initiated recordings did so based on considerations of the current systems and environment. They maintained a conservative attitude toward patient-initiated recordings and called for the implementation of more safeguards.
Some family members cannot be present for the conversations in a timely manner. Recording or remote communication can make it more convenient to involve them, but it would be best to have a dedicated conversation space and recording facilities, with both parties retaining copies of the recordings. (Respondent 428) Recordings need to be made in designated settings and with the consent of both parties. (Respondent 696)
Impact on medical efficiency
Some physicians had different opinions on patient-initiated recordings, arguing that they are not very beneficial for doctor-patient communication or treatment. They believed that, in emergency situations, patient-initiated recordings could potentially impede physicians and hinder medical care.
It would be distracting, affecting my assessment of the medical condition, and consuming a significant amount of time to cautiously choose my words during conversations. (Respondent 103) Clinical situations are intricate, and physicians may choose to communicate less during recordings to prevent any inaccuracies. (Respondent 963)
Respect and trust issues
Among those who disagreed with patient-initiated recordings, 44.4% expressed suspicion toward the purpose of the recordings. They believed that there is tension between doctor-patient and were concerned that the recorded content could be edited or taken out of context, potentially leading to disputes and harm. “Interpret out of context” was the third most frequently used phrase. Some physicians disagreed with recordings, considering them disrespectful and indicative of mistrust. They felt that patient-initiated recordings disregarded their consent and violated their privacy, which in turn affected their emotions, psychological well-being, and decision-making to some extent.
Recording without asking permission is disrespectful to physicians. (Respondent 601) Effective communication is only possible when based on trust. Recording reflects the distrust of patients’ families. (Respondent 717) Conversations can be interpretated out of context and misleading. (Respondent 741) Given the current overwhelming and power of social media, the impact on individual physicians could be devastating. (Respondent 97)
Discussion
Recording devices are now commonly used during doctor-patient encounter and providing patients with recordings of consultations can improve consultation efficiency. With limited guidelines or regulations, unauthorized patient-led recordings can significantly affect doctor-patient communication, potentially damaging trust. This study extensively explores clinicians’ attitudes toward patient-initiated recorded conversations. Prior to this, there have been few studies on recorded conversations in China, mostly based on the perspectives of patient and their families, while few have centered on medical professionals. By using anonymous questionnaires, it gathered responses from physicians across various departments, age groups, and work situations, providing a representative reflection of clinicians’ general attitudes toward recorded conversations. As an exploratory study, it serves as a starting point for understanding the viewpoints of physicians and for beginning to define this phenomenon. Therefore, an exploratory qualitative approach was used to identify themes and categorize the viewpoints.
In this study, 63.2% of the physicians expressed caution about recorded doctor-patient conversations. A study from the United Kingdom showed that 56% of people felt uncomfortable about being recorded, and 23% would end the consultation if the patient insisted on recording. 14 Another study conducted in 2020 from the United States showed that out of the 57 participants surveyed, only 20 (35%) believed that patients had the right to record their medical conversations. A total of 36 (63%) believed that the legal risks of recording outweighed the benefits it could provide to patients. 15 A recent study investigated German oncologists’ attitudes and only 14% expressed a willingness to offer recordings, highlighting concerns over data security and legal implications. 16 The analysis in our study revealed that the acceptance of recorded conversations among physicians was related to factors such as gender, age, years of medical practice, and professional title. However, it was not significantly associated with education level, hospital level, specialty, or whether they had received training in doctor-patient communication. Magowan et al. performed an online survey of surgeons in the United Kingdom and responses varied markedly between consultants and trainees, with 46% of consultants stating they would feel comfortable, versus 20% of registrars and 15% of junior surgical trainees. 14 Jimenez et al. explored acceptance of patient-initiated audio recordings of clinic discussions by oncologists and also found an association between older physician age, and greater years in practice and higher rate of comfort with recordings. Gender, level of hospital, specialty, number of patients seen per week and personal experience with cancer was not significant. 7 Physicians who were open to recorded conversations often mentioned patients’ rights to be informed and their freedom, improved communication efficiency, respect for and understanding of family members’ wishes, and confidence in their own professionalism. On the other hand, physicians who were opposed to patient-initiated recordings frequently cited distrust between physicians and patients, feelings of disrespect caused by recordings, and the potential interference with diagnosis and treatment in certain situations. While our study did not empirically test for cultural determinants, the general attitudes of caution and opposition observed can be fruitfully discussed within the well-documented socio-cultural context of China’s healthcare environment. It is plausible that broader cultural norms, such as a traditional paternalistic model of medicine that emphasizes physician authority and a cultural preference for social harmony, may contribute to the perception of patient-initiated recordings as a potential catalyst for conflict rather than a neutral patient aid. This cultural lens could help explain the strong concerns about damage to trust and the heightened fear of litigation observed in our data. Additionally, regardless of whether they supported recordings or not, most physicians considered the existing systems and environment. They believed that even if patient-initiated recordings were permitted, there should be prerequisites, such as ensuring transparency and implementing more safeguards.
Impact on quality of care
Understanding and memorizing medical advice within a short period of time is challenging. In a systematic review conducted by Watson and McKinstry, it was found that most studies focused on the use of written and/or audio-recorded medical instructions to enhance recall of medical advice. 17 The practice and purpose of recording varied among different medical specialties. A higher proportion of oncologists and rehabilitation physicians reported sharing recordings with patients compared to other specialties, which may be due to the unique emotional impact of cancer diagnoses and the complexity of treatment plans in these fields.9,18–20 A German research team conducted questionnaire surveys to assess attitudes toward conversation recordings among cancer patients, overwhelming majority (92%) expressed a positive attitude. 21 In a literature review conducted by McClement and Hack, it was concluded that recording outpatient consultations offered numerous benefits, despite the limitations of previous studies. It was cost-effective, easy to incorporate into routine clinical practice, improved information recall, reduced the frequency of patient callback inquiries, decreased the time physicians needed to clarify information and resolve patient issues, and ultimately could reduce healthcare costs. 22 There were even studies suggesting that audio recordings could be used as a monitoring tool to improve the quality of care. 23 Additionally, sharing the recordings allowed family members who were not present to better understand the condition, which provided some relief from stress.10,24–26 Recordings involve patients’ families in the medical process, helping them understand health issues and make decisions with support. Furthermore, recordings can also motivate and inspire patients by enabling them to maintain social relationships and share their experiences with others. 25
Some physicians argue that patient-initiated recordings can impede treatment.8,27,28 On one hand, in emergency cases, it can be challenging for physicians to offer thorough and precise explanations. In this case, it would be inappropriate to make the judgment that the physician’s medical information disclosure is insufficient. This may also negatively impact the family’s willingness to pursuit progressive treatment, potentially lower the patient’s recovery rate, and heighten the chances of disputes. On the other hand, recordings can also add psychological pressure on physicians, causing them to be more cautious with their choice of words to prevent errors. It was a distraction and occasionally forced retrospective decision-making (after the recording had occurred). 12
Dynamics of the doctor-patient relationship
Studies have shown that audio-visual recordings of visits are not linked to an increase in medical malpractice claims or lawsuits. 29 However, it has been noted that patients secretly record consultations due to a lack of trust in the healthcare system. 4 The complexity of certain situations can be amplified when audio or video recordings are made during a consultation. 30 The use of recordings as evidence of medical practice can potentially harm a clinician’s professional or health service reputation. 25 Previous research has shown that physicians who are resistant to recording conversations believe that patients record to use the recordings in legal matters or to share on social media. 7 The majority of physicians in our study mentioned “trust” and “respect” as their concerns, which aligns with the findings of previous surveys.24,31 Some physicians express mistrust regarding the purpose of patient recordings, fearing potential legal issues and conflicts, leading them to adopt a defensive and resistant attitude. Additionally, some individuals perceive recordings as having an “evidentiary” purpose, which can make them feel violated. In an Australian survey, four respondents shared their experiences and reactions to being recorded by a patient on a mobile phone. Participants who had a difficult experience or were aware of adverse events were more likely to react negatively. 12 Unknown contexts, misunderstandings, invasion of privacy, and the risk of litigation are growing concerns, and there is no reliable way to address or clarify these issues. Due to concerns about future litigation or personal risks, physicians often adopt a more neutral attitude. Some physicians, fearing recording, may limit the discussion or omit unnecessary parts of the dialog to prevent manipulation. 30
Some studies conducted outside of China indicate that the majority of patients choose to actively request recordings rather than secretly recording. This is done in the hope that it will encourage physicians to conduct their consultations more diligently and conscientiously, ultimately leading to better treatment outcomes.10,24,31 When patients make a request to record consultations, physicians agreeing to this can actually help build trust. 12 It is especially important for physicians to maintain a proactive and positive attitude in order to avoid conflicts and confrontations that could worsen negative situations. 14 Although many physicians have reservations about recordings, they are starting to recognize the benefits and may even proactively offer recordings to enhance the patient experience.12,32
Legal and ethical issues
Some literature has highlighted concerns about the burdens introduced by recording, including potential compromises to personal privacy.10,28,33 Pre-existing surveys indicate that 18.7% of the population reported recording their visit with audio/video, with 2.7% recording without the clinician’s permission. 9 A total of 19.3% of respondents reported being aware of a family member or friend who had recorded a clinic visit, of whom 60.4% asked for permission and 25.7% did not. 9 Additionally, it is crucial to ensure the protection of others’ personal health information. 34 While some healthcare professionals may feel uneasy, there is little legal basis to deny a patient’s request to record clinical procedures and/or discussions with clinicians.9,14 Elwyn et al. reviewed relevant legal documents in nine countries: Australia, Brazil, Canada, France, Germany, India, Mexico, the United Kingdom and the United States and found that most jurisdictions have case law or statutes, derived from a constitutional right to privacy, or a wiretapping or eavesdropping statute, governing the recording of private conversations. Little to no guidance exists on how to translate constitutional principles and case law into advice for people seeking to record their medical encounters. 35 In 2018, the British Society of Anaesthesia issued guidance stating that consent should generally be granted if a patient or relative requests permission to record a conversation for personal use and reference, unless doing so would compromise patient safety and treatment.9,32,33,36 In a survey conducted in the United States, it was revealed that only a very small number of healthcare organizations had policies regarding patient audio recording systems. However, research conducted outside of China have revealed that most physicians believe there is either no official policy or are uncertain about the existence of a clear policy on recorded conversations. They believe that the decision regarding recording conversations lies with the healthcare organization or the individual physician. 7 There are two of our participants mentioned covert audio/video recording is not allowed per institution policy. Requirements of regulations and legal rule, hospitals policy, and other stakeholders could have significant impact on individual attitudes. 36 Furthermore, 92% of physicians believe that patients should not start recording without their physician’s consent. 70% of oncologists believe that a physician can refuse to be recorded, and 74% are in favor of a two-party consent policy for recordings (e.g. requiring the consent of both the patient and the physician). In our study, we discovered that most physicians are unfamiliar with the rights and regulations related to recorded conversations. Only 30 physicians mentioned patients’ rights to record as well as their own privacy rights. A significant number of physicians believe that recordings should have certain prerequisites. They believe that patients should actively request to record, and that it requires honesty and trust between both parties, along with more comprehensive systems and standard procedures. It would be valuable to consider implementing a formal and transparent recording process for both parties, creating two copies of the conversation recording. One copy can be provided to the patient or their family, and the other can be included in the medical records. 36 Referencing recordings in other services, such as police interviews, might add valuable technical/logistical context. All participants being present at the conversation recorded must be informed about when and where they can watch or listen to the recording. 37 The recording might have to be provided only upon a family or physician request on proper purpose (e.g. for communication training purposes) and needs approval of hospital authority to protect patient privacy. Legal advice should be sought should physicians become aware of a complaint or claim involving a covert recording. 36 The standardization and institutionalization of recordings are still in the exploratory phase, with ongoing efforts to establish guidelines, share recordings, and create a platform for doctor-patient communication.9,33
On the other hand, physicians should always practise medicine in a professional manner as the patient may record at any time. 34 The use of smartphones in the consultation room should not impact the delivery of healthcare. 7 A previous survey of oncologists found that 77% believed that documenting the visit would positively impact the patient experience. Of those surveyed, 85% “always” allowed documentation when asked, 11% “usually” allowed it, and 5% “rarely” or “never” allowed it. 7 Our study demonstrates that some physicians have an open and inclusive attitude toward recordings. This may be attributed to factors such as confidence in their professionalism, trust, and understanding of the patient. It is possible that the distribution of the study population, most of whom come from large hospitals in developed or relatively developed cities, is related to this finding. The more standard medical environment and rigorous medical background of these physicians could contribute to their confidence and composure. These attitudes could also be addressed by providing opportunities for positive experiences with consultation recordings during medical education as well as in clinical practice. Providing role models who support patient-centered care could also foster greater acceptance. 38 There has been rapid advancement in technologies that interface with medical communication, particularly the rise of AI documentation and video consultation post COVID pandemic. While our study captures attitudes at a key inflection point, the broader adoption of such technologies may influence professional perspectives on recording. For instance, if AI documentation and video consultation becomes prevalent, patient-initiated recording may be perceived differently. No large-scale studies on this specific topic in China have been published since our data collection, highlighting a need for continued research to track evolving attitudes in this dynamic landscape. Our findings thus provide a crucial baseline for future investigations.
Research limitations
This pilot qualitative study primarily distributed questionnaires in northern China, focusing on tertiary hospitals. Given the similar work environments, the data may reflect the views of this specific group and may not be applicable on a national or universal level. The questionnaire was not rigorously tested or proven but pilot tested. Additionally, due to the short completion time, most responses were brief, capturing only the initial reactions of physicians to recorded conversations. As a result, the study does not explore the underlying reasons and considerations of the physicians in depth.
Conclusions
This cross-sectional survey, conducted at multiple centers across various regions in China, with a higher concentration of participants from northern provinces, suggest a trend toward cautious engagement with recording practices, mainly due to concerns over their purpose and potential negative effects. The rapid progress of modern society has increasingly blurred the lines of personal privacy, as recordings and videos allow for the swift dissemination of personal information. While safeguarding the privacy of other patients and healthcare professionals is essential, the gradual acceptance of recorded conversations could improve medical services and reduce their negative effects on doctor-patient relationships. Clinicians no longer view recorded conversations as isolated occurrences, yet policy development in this area remains slow. There is an urgent need for policy guidance for healthcare organizations and further research into how recorded conversations affect clinical practice.
This paper highlights the need for healthcare institutions to develop standardized guidelines and provide training for medical professionals regarding patient-initiated recordings.32,34 These guidelines should emphasize transparency, mutual consent, and the implementation of safeguards that protect both parties. Such measures would help alleviate concerns related to legal risks, enhance communication, and foster trust in doctor-patient interactions. By incorporating structured communication protocols and equipping healthcare providers with strategies to handle recordings, it is possible to create a more collaborative and efficient clinical environment.2,4–6,10,17–20,24,26 This could not only improve patient engagement but also support a more positive perception of the healthcare system overall.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251381224 – Supplemental material for Cross-sectional survey of medical professionals’ attitudes toward recorded doctor-patient conversations
Supplemental material, sj-docx-1-phj-10.1177_22799036251381224 for Cross-sectional survey of medical professionals’ attitudes toward recorded doctor-patient conversations by Chuyun Ya, Peitao Suo and Shu Li in Journal of Public Health Research
Supplemental Material
sj-pdf-2-phj-10.1177_22799036251381224 – Supplemental material for Cross-sectional survey of medical professionals’ attitudes toward recorded doctor-patient conversations
Supplemental material, sj-pdf-2-phj-10.1177_22799036251381224 for Cross-sectional survey of medical professionals’ attitudes toward recorded doctor-patient conversations by Chuyun Ya, Peitao Suo and Shu Li in Journal of Public Health Research
Footnotes
Acknowledgements
We appreciated the help of experts who participated in the funding application and questionnaire modification, and all the physicians who filled out and disseminated the questionnaire.
Abbreviation
IQR, interquartile range
Ethical considerations
The study was reviewed and approved by the Peking University Third Hospital Medical Science Research Ethics Committee (IRB-2021-493).
Consent to participate
The study used electronic informed consent, requiring respondents to agree to participate before proceeding further to view the questionnaire content.
Author contributions
Chuyun Ya: Validation, Formal analysis, Data Curation, Writing—Original Draft. Peitao Suo: Validation, Formal analysis, Data Curation, Writing—Original Draft. Shu Li (Corresponding Author): Conceptualization, Methodology, Validation, Investigation, Resources, Writing—Review & Editing, Supervision, Project administration, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the China Medical Board-Open Competition Program (20-378), Peking University Third Hospital Fund for Returned Scholars (BYSYLXHG2020004) and the special fund of the National Clinical Key Specialty Construction Program, P. R. China (2022), 301-2305.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.