
Abstract
Background:
Tuberculosis (TB) remains the leading cause of communicable disease-related mortality worldwide. The present study aimed to determine the prevalence of pulmonary tuberculosis (PTB), rifampicin resistance pattern, and to identify the major explanatory risk factors among suspected patients visiting Durbete Primary Hospital (DPH).
Design and methods:
A cross-sectional study was conducted among patients suspected with PTB at DPH from February to June 2022. All eligible suspected PTB patients aged ≥18 years were included in the study. Data on risk factors were collected using questionnaire. Two spot sputum specimens were collected from each enrolled patient according to WHO guidelines. Sputum was examined by GeneXpert and Ziehl-Neelsen microscopy. Logistic regression models were used to determine the strength of association between dependent variable and risk factors and to identify the major explanatory risk factors.
Results:
Of the total of 180 PTB suspected patients who participated in the study, 17 (9.44%, overall prevalence) were identified as having PTB. Participants who had an unknown history of hypertension (AOR = 8.483; 95% CI 1.059–67.935) and who had contact with known PTB cases (AOR = 16.108; 95% CI 1.983–130.844) were significantly associated with the prevalence of PTB (p < 0.05). One (6.25%; 1/16) specimen that was detected as positive by the GeneXpert was found to be resistant to rifampicin.
Conclusion:
This study showed a relatively high prevalence of PTB among suspected patients. Periodic surveillance of PTB and educating the local community about major risk factors, such as contact with known PTB cases, are necessary to reduce the prevalence of PTB.
Introduction
Tuberculosis (TB) remains the leading cause of communicable disease-related mortality worldwide, with approximately 10 million infected and 1.4 million deaths in 2019.1,2 Ethiopia faces a significant burden of TB and multi-drug resistant TB (MDR-TB), with an incidence of 132 per 100,000 populations and an estimated 5800 MDR-TB cases annually.3,4 Pulmonary TB primarily affects the lungs, presenting symptoms such as cough, chest pain, and weight loss.2,5 The disease often carries stigma and marginalization, exacerbated by factors like poverty, undernutrition, and HIV infection. Educational status, history of TB contact, and malnourishment significantly correlate with TB infection risk.6,7 Regular surveillance and assessment of these factors are crucial for timely interventions to reduce TB’s community burden.
Rapid identification of M. tuberculosis is essential for effective diagnosis and treatment, as TB can spread easily. 8 Studies indicate that a significant portion of TB transmission occurs among those who test negative for Acid Fast Bacteria (AFB) smear microscopy. 9 Drug-resistant TB poses a continuing public health threat, with nearly half a million new cases of rifampicin-resistant TB globally in 2019. The WHO advocates for rapid molecular testing alongside conventional methods to detect drug resistance. 2 Understanding the genetic mutations in M. tuberculosis responsible for drug resistance is vital for improving treatment outcomes.10,11 Despite advancements in TB control, updated prevalence data on PTB, rifampicin resistance, and associated risk factors are needed, especially in areas like Durbete Primary Hospital in northwest Ethiopia, where such information remains undocumented.
Method
Study setting
A hospital-based cross-sectional study was conducted in Durbete Primary Hospital located in South Achefer District, West Gojjam Zone of the Amhara Regional State, northwest Ethiopia (Figure 1). It borders with Agew Awi Zone to the South and West, North Achefer District in the North, and North Mecha District in the East. Geographically, the district lies within 11°04′00″−11°05′00″N latitude and 36°52′00−36°54′00″E longitude at a distance of 498 km far from Addis Ababa and 59 km from Bahir Dar city. The altitude of the district ranges from 1500 to 2500 m above sea level with an annual rainfall range of 1450–1594 mm per year. The average annual temperature of South Achefer District is 26.8°C.

Map of Ethiopia, Amhara Region, and the study district.
According to the Amhara Regional State Bureau of Finance and Economic Development population projections, the total population of the district is about 148,974. The rural population is 134,447 or 90.2%, whereas the number of people living in urban areas is 14,528, which accounts for only 10.8% of the total population of the district. 12 Durbete Primary Hospital is the only government primary hospital in South Achefer District, Amhara National Regional State. It lies on about 5000 m 2 of surface area. The hospital has 48 beds and 202 health workers offering different services. DPH provides health care services for outpatient and in-patient services including TB diagnosis services for more than 170,297 populations in its catchments.
Study population
The source of the population for this study was all suspected PTB patients visiting DPH from February 2022 to June 2022. The study participant was selected when suspected PTB patient exhibited clinical symptoms of one or more of the following: persistent cough for more than 2 weeks, coughing up blood, chest pain, unexplained weight loss, fatigue, night sweats, and fever.
Inclusion criteria
All eligible PTB suspected patient participants whose age was ≥18 years during the study period were included in the study until the required sample size, 184, was reached.
Exclusion criteria
Study participants who were unable to give samples and socio-demographic information at the time of data collection were excluded. Critically ill patients, participants whose age was <18 years, individuals who had taken anti-tuberculosis drugs, and sample referrals were also excluded.
Sample size determination
The sample size was determined using a single population proportion formula for cross-sectional surveys.

, Where n is the sample size; Z1−∝/2 is the standard normal distribution value at 95% confidence interval (CI), which is 1.96; P = 11.2% (0.112) is the expected PTB prevalence from a previous similar study from Central Ethiopia, 13 and d is the margin error or precision taken as 5% (0.05).
Therefore, with the data provided above, the final sample size including a 20% non-response rate was 184 suspected PTB patients enrolled in the study. However, due to various kinds of errors on the GeneXpert MTB/RIF assay, four (2.2%) specimens did not give results; therefore these four specimens were not included in the final analysis.
Data on socio-demographic characteristics and risk factors were collected using a structured questionnaire. STROBE checklist for cross-sectional study was followed in this study 14 (see Supplemental File, S1). Two spot sputum specimens (in the spot-spot sample collection approach) were collected simultaneously (immediately after the provision of the first sputum) from each enrolled patient using coded and two clean plastic containers (50 ml Falcon tubes) by laboratory personnel as per WHO guidelines on the sputum collection procedure. 15 The minimum acceptable volume of sputum in each collection tube was 3 ml. Each study participant was requested to provide two samples in an hour interval in the same day. An early morning sputum was collected using one cup and then the second sputum sample was collected using another cup from the same study participant. One sample was tested directly by ZN microscopic examination and the other sputum sample was used for GeneXpert MTB/RIF assay. Every day, manual checks were made to acquire data and ensure its accuracy and consistency. To assure the reliability and validity of test results, standard operational procedures were employed for specimen collection and correct labeling. In addition to this, the sample sputum was discarded if it contained food particles.
Socio-demographic and risk factor data collection
After the study participants had given their informed consent, socio-demographic and risk factor data were collected using a structured questionnaire. A risk factor is operationally defined as any characteristic, condition, or behavior that increases an individual’s likelihood of acquiring or developing TB infection or progressing from latent TB infection to active TB disease. A structured questionnaire was developed with modifications based on known and possible risk factors from previous literature 6 (See Supplemental File, S2) and data were then collected using an original questionnaire prepared in English and translated into the local language, Amharic. The questionnaires were answered by study participants through interviews conducted by nurses.
Laboratory methods
Ziehl-Neelsen microscopy
The thick purulent part of the sputum samples was formed into direct smears, which were then air-dried, heat-fixed, and stained using the ZN staining technique. The smears were examined with oil immersion 100× objective lenses and graded as scanty (1–9/100 fields), +1(10–99/100 fields), +2(1–10/field, and +3 (>10/field) as per Ethiopian national TB guidelines. 4
GeneXpert MTB/RIF assay
Sputum samples or decontaminated sputum pellets were treated with NaOH and isopropanol-containing sample reagent. The sample reagent was added at a 2:1 ratio to the sputum sample or sputum pellet and incubated for 15 min at room temperature. The treated sample was transferred into the cartridge; the cartridge was loaded into the Xpert instrument, and an automatic process completed the remaining steps of the assay. 16
Statistical analysis
The data collected through the questionnaire and laboratory investigation were coded in an Excel spreadsheet and then exported to SPSS software version 26 (Chicago, IL, USA) for analysis. Descriptive statistics were used to characterize the study participants. The prevalence of PTB was calculated with its 95% CI. Univariate logistic regression was used to determine the strength of association between dependent variables and possible risk factors. Variables that showed significance at a p-value of less than 0.25 during univariate logistic regression analysis were selected for multivariable logistic regression analysis. 17 The strength of association was measured by using odds ratio values and then variables with p-value of less than 0.05 in the final model of multivariate logistic regression were considered statistically significant explanatory risk factors for PTB.
Results
Socio-demographic and economic characteristics of study participants
In the current study, a total of 184 suspected PTB individuals were invited to participate. However, the overall response rate was 97.8%. Five sputa with a GeneXpert MTB/RIF assay final result of “No result” were excluded from this analysis. Only 180 sputum samples had an interpretable result for the GeneXpert MTB/RIF assay. Out of the 180 study participants, 92 (51.1%) were males and 88 (48.9%) were females. Most of the participants, 38 (21.1%) were in the age group of 28–37 years whereas the least participants 24 (13.3% each) were in the age groups of 58–67 years and ≥68 years. The age of study participants ranged from 18 to 82 years with a mean age of 45.72 ± 17.19 years. One hundred seventy-eight (98.9%) were Orthodox Christians whereas two (1.1%) were Muslims. The majority (120; 66.7%) of the study participants were married, rural residents (113; 62.8%), unable to read and write (77; 42.28%) and farmers (110; 61.1%). The houses of majority (104; 57.8%) of study participants had inadequate ventilation and 120 (66.7%) of the participants used firewood for cooking their food (Table 1).
Socio-demographic and economic characteristics of PTB suspected patients in DPH, northwest Ethiopia, 2022 (N = 180).

Clinical presentations and co-morbidity-related factors of the study participants
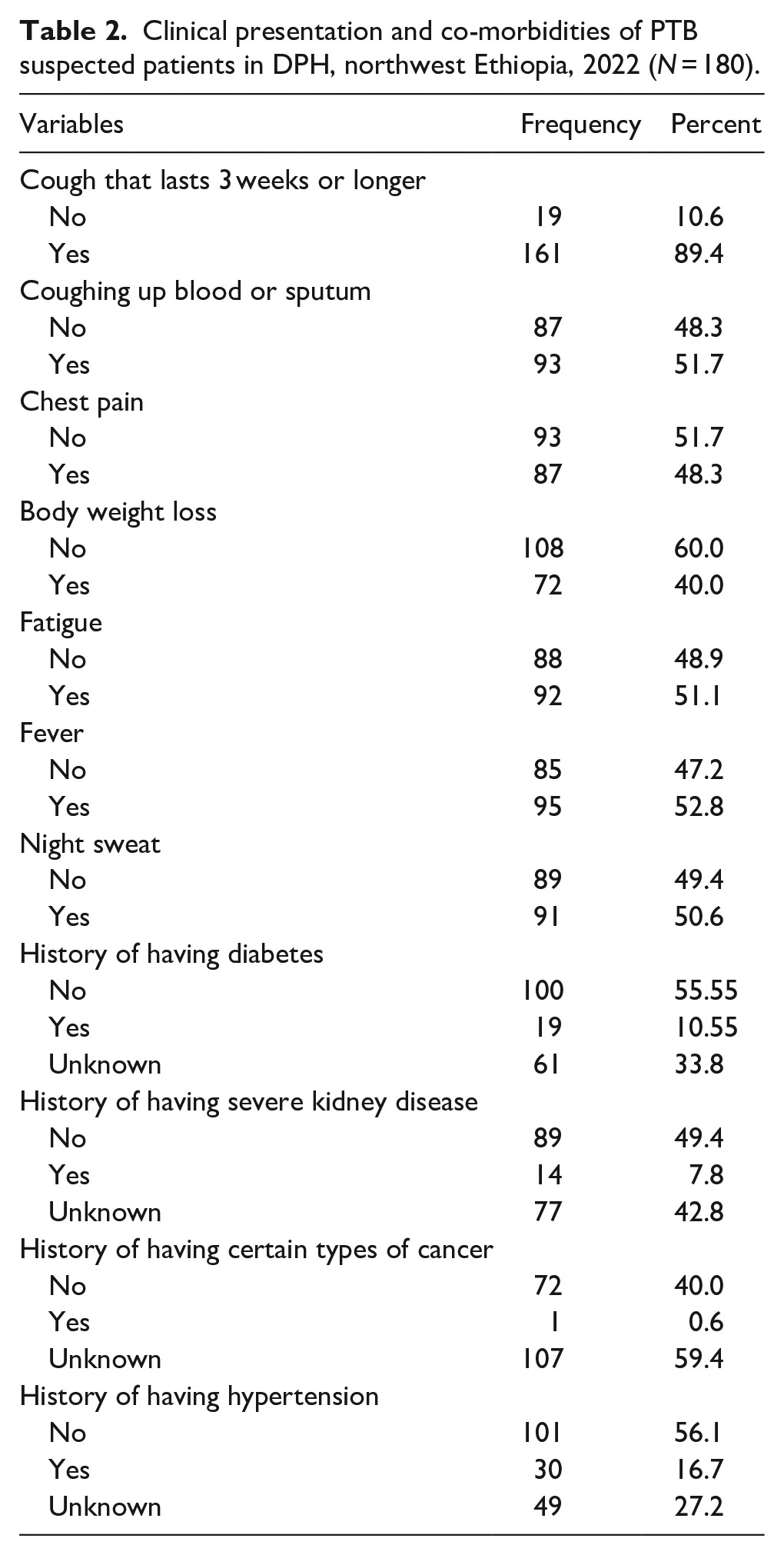
Signs and symptoms, as well as co-morbidity (self-reported by the patient, not confirmed) related factors, were assessed in the study. Of all the participants, 161 (89.4%) had a cough that lasted 3 weeks or longer, 93 (51.7%) coughed up blood or sputum, 87 (48.3%) had chest pain, 72 (40.0%) had body weight loss, 92 (51.1%) had fatigue, 95 (52.8%) had a fever, and 91 (50.6%) had night sweats. Among co-morbidities reported, 19 (10.6%), 14 (7.8%), 1 (0.6%), and 30 (16.7%) of study participants had a history of diabetes, severe kidney disease, certain types of cancer, and hypertension, respectively (Table 2).
Clinical presentation and co-morbidities of PTB suspected patients in DPH, northwest Ethiopia, 2022 (N = 180).
Behavioral and practice-related characteristics
Out of the total study participants, 31 (17.2%) and 29 (16.1%) had a history of contact with known PTB cases and a habit of sharing a cup and/or spoon, respectively. Six (3.3%), 15 (6.7%), and 78 (43.3%) participants had a history of cigarette smoking, khat chewing, and alcohol consumption, respectively (Table 3).
Behavioral and practice-related characteristics of PTB suspected patients in DPH, northwest Ethiopia, 2022 (N = 180).

Prevalence of PTB
Among 180 participants, 17 (9.44%) tested positive for PTB by at least one of the two diagnostic methods (GeneXpert MTB/RIF assay or ZN microscopy).
Risk factors associated with PTB infection
In the univariate analysis of socio-demographic and economic characteristics of the study participants, the Crude Odds Ratio (COR) values were greater than one, except for the variables of income, residential area, and family size. The odds of M. tuberculosis infection were about four times (COR = 3.785; 95% CI: 1.048–13.677, p = 0.042) higher in study participants who had inadequate ventilation compared to those who had adequate ventilation in their houses.
In the univariate analysis of clinical presentations and co-morbidity-related characteristics, study participants who coughed up blood or sputum were about five times (COR = 4.962; 95% CI: 1.374–17.922, p = 0.014) at higher risk of contracting PTB compared to those who did not cough up blood or sputum. Similarly, the odds of M. tuberculosis infection were about five times (COR = 4.850; 95% CI: 1.212–19.401, p = 0.026) and five times (COR = 4.732; 95% CI: 1.350–16.590, p = 0.015) higher in study participants who had a history of hypertension and an unknown history of hypertension, respectively, compared to those who had no history of hypertension (Table 4).
Univariate and multivariate analyses that shows the strength of association between risk factors and PTB in DPH, northwest Ethiopia, 2022.

TB: tuberculosis; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Statistically significant.
In the univariate analysis of behavioral and practice-related characteristics, study participants who had a contact history with known PTB cases were about five times more at higher risk of contracting PTB compared to those who had no history of contact with known PTB cases (COR = 5.411; 95% CI: 1.894–15.454, p = 0.002). Similarly, those who had a history of khat chewing were four times (COR = 4.252; 95% CI: 1.186–15.244, p = 0.026) more likely to contract M. tuberculosis infection compared to those who did not have a history of khat chewing (Table 4).
All socio-demographic, clinical presentation and co-morbidity, and behavioral and practice-related characteristics that showed a p-value of less than 0.25 in the univariate analysis were selected and entered into the multivariate logistic regression analysis to identify the most explanatory risk factors of PTB. In the final model of multivariate logistic regression, family size, night sweats, history of hypertension, and contact with known PTB cases were found to be independent explanatory risk factors for M. tuberculosis infection in suspected patients in the study area. The patients who had an unknown history of hypertension and contact with known PTB cases were about 8 times (AOR = 8.483; 95% CI: 1.059–67.935, p = 0.044) and 16 times (AOR = 16.108; 95% CI: 1.983–130.844, p = 0.009), respectively, at higher risk of acquiring the disease compared with those without a history of hypertension or without any contact with known PTB cases (Table 4).
GeneXpert MTB/RIF assay rifampicin resistance profile
GeneXpert is an automated machine that utilizes a real-time nucleic acid amplification technique to simultaneously detect M. tuberculosis and rifampicin (RIF) resistance in a closed system. It is important for the diagnosis of multidrug-resistant M. tuberculosis. One of the objectives of this study was to investigate whether M. tuberculosis bacteria in sputum were sensitive or resistant to the antibiotic drug, rifampicin. So, out of 16 specimens that were found to be positive by the GeneXpert, 14 (87.5%) specimens were RIF-sensitive, 1 (6.25%) specimen was RIF-resistant, and 1 (6.25%) specimen was indeterminate based on the Xpert RIF sensitivity test (Table 5). An indeterminate result shows that the test was unable to accurately determine whether the bacteria were resistant to RIF.
Rifampicin sensitivity test by GeneXpert MTB/RIF assay.

Discussion
The present study aimed to determine the prevalence of pulmonary tuberculosis (PTB) at DPH and assess rifampicin resistance patterns and major risk factors for M. tuberculosis infection among suspected patients. The findings will provide current information for TB prevention programs in Durbete town and the South Achefer District.
The overall prevalence of PTB among suspected patients was 9.44%, consistent with a study at Ataye District Hospital, northeast Ethiopia (8.98%). 18 In contrast, higher rates were reported in Nigeria (22.9%), 19 Adare General Hospital, Southern Ethiopia (30.5%), 20 Addis Ababa (15.11%), 21 Gambella Regional State (20%), 22 University of Gondar Hospital (24.6%), 23 Karamara Hospital, Jigjiga (25.5%), 24 and Debre Markos (23.2%). 25 Discrepancies may arise from variations in population, risk factors, settings, and study designs. Conversely, lower prevalence rates of PTB were reported in other Ethiopian studies: 2.6%, 26 2.9%, 27 6.5%, 28 and 5.73%, 8 possibly due to differences in population and diagnostic methods.
Most socio-demographic and economic factors did not show a significant association with PTB presence. However, studies at Ataye District Hospital, 18 Jabi Tehnan District, 29 Debre Markos Referral Hospital, 7 and in the Philippines 30 found significant associations with older age groups. Sex, residence, marital status, education, and smoking habits were not significantly associated with PTB occurrence, contradicting earlier Ethiopian findings, 6 likely due to differences in study design and participant characteristics.
M. tuberculosis was detected across all family sizes, with lower prevalence in families of 4–6 and >6 compared to those with 1–3. This differs from previous northeast Ethiopian studies, 18 where family size was not significantly associated with PTB, potentially due to increased exposure from social interactions in the current study area.
Key clinical symptoms included coughing for over 2 weeks, sputum production, weight loss, and chest pain. In univariate analysis, significant features included hemoptysis, chest pain, weight loss, fatigue, fever, and night sweats; however, only night sweats remained significant in the multivariate model.
Among co-morbidity factors, individuals with an unknown history of hypertension were 8.4 times more likely to acquire M. tuberculosis than those without. This finding contrasts with a study among smear-negative PTB patients in Addis Ababa, 27 potentially due to differences in population selection.
Logistic regression revealed that individuals with a history of contact with known PTB cases were 16 times more likely to contract M. tuberculosis than those without contact, consistent with findings from other Ethiopian studies.7,18
Rifampicin-resistant TB (RR-TB) is a significant concern globally. In this study, RR-PTB isolates identified by the Xpert assay (1/16; 6.25%) were lower than in similar Ethiopian studies (186/1876; 9.9%) 21 and Nigeria (15/102; 14.7%), 19 indicating a public health issue. Comparable rates were reported at Ataye District Hospital (2/38; 5.3%) 18 and in Gambella (9/185; 4.86%), 22 while other studies reported no RR-PTB cases.26,27,31 Variations in RR-PTB prevalence may stem from differences in methodology, sample size, treatment adherence, and geographical factors.
Of 16 GeneXpert MTB/RIF assay positive specimens, 14 (87.5%) were RIF-sensitive, 1 (6.25%) was RIF-resistant, and 1 was RIF-indeterminate. These results align with studies in northern Ethiopia (94.7% RIF-sensitive) 18 and others (90.9% RIF-sensitive), 32 but differ from findings at the University of Gondar Hospital (84.2% RIF-sensitive), 23 likely due to their larger sample size and retrospective design.
Limitations of the study
A hospital-based study among PTB-suspected patients might have increased the present prevalence of M. tuberculosis. GeneXpert might detect smear-negative TB cases and also report potential false-negative results which might affect the present findings. Home-to-home visits are one of the strategies for active detection of TB in countries like Ethiopia; therefore, employing this strategy could reveal the actual prevalence of the disease in Durbete District.
Conclusion
The overall prevalence of pulmonary tuberculosis (PTB) among suspected patients using ZN microscopy and Xpert was 9.44%. Among the 16 PTB-confirmed patients identified by the GeneXpert MTB/RIF assay, one (6.25%) was resistant to rifampicin. This indicates a significant prevalence of PTB in the study area. Family size, night sweats, history of hypertension, and contact with known PTB cases were significantly associated with PTB. These results highlight that PTB and rifampicin-resistant PTB remain public health concerns, necessitating periodic surveillance and identification of key risk factors for effective prevention and control. Integrating TB services into primary health care is essential to ensure that TB prevention and treatment are part of Ethiopia’s broader health system.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251373008 – Supplemental material for Prevalence of pulmonary tuberculosis and its associated risk factors among suspected patients visiting Durbete Primary Hospital, northwest Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036251373008 for Prevalence of pulmonary tuberculosis and its associated risk factors among suspected patients visiting Durbete Primary Hospital, northwest Ethiopia: A cross-sectional study by Maritu Demelash, Endalkachew Nibret, Zebasil Minichil and Daniel Mekonnen in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251373008 – Supplemental material for Prevalence of pulmonary tuberculosis and its associated risk factors among suspected patients visiting Durbete Primary Hospital, northwest Ethiopia: A cross-sectional study
Supplemental material, sj-docx-2-phj-10.1177_22799036251373008 for Prevalence of pulmonary tuberculosis and its associated risk factors among suspected patients visiting Durbete Primary Hospital, northwest Ethiopia: A cross-sectional study by Maritu Demelash, Endalkachew Nibret, Zebasil Minichil and Daniel Mekonnen in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to thank all the participants of the study who volunteered to take part. We would also like to express our gratitude to the staff of Durbete Primary Hospital for their cooperation during the study.
Ethical considerations
Ethical approval was obtained from the Ethical Clearance Committee of Science College, Bahir Dar University (Ref. No: PRCSVD/285/2014). All experimental protocols were also approved by the same Committee. The study was conducted in accordance with Declaration of Helsinki and Good Clinical Practice.
Consent to participate
Written informed consent was obtained from all study participants. Those study participants who could not read and write were considered as illiterates and informed consent was obtained from their legal representatives.
Author contributions
MD and ZM were involved in the design, data collection, processing, and interpretation of the findings and drafting of the manuscript. EN and DM were involved in the conception of the idea, reviewing and editing the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.