
Abstract
Introduction:
The COVID-19 pandemic has impacted all age groups, with older individuals experiencing health effects and lifestyle changes. This study explored factors associated with quality of life (QoL) among older adults and examined how a history of COVID-19 infection and quarantine varied across these factors in the post-pandemic period.
Methods:
A cross-sectional survey was conducted among older adults attending a primary care clinic between November 2023 and January 2024. Sociodemographic data and information on patients’ history of COVID-19 infection and quarantine were collected. The WHOQOL-BREF-THAI was used to assess QoL. Bivariate and multiple logistic regression analyses identified factors associated with a history of COVID-19 and QoL.
Results:
The study received 195 survey responses. Most participants had moderate to poor QoL, were female (69.74%), and had a mean age of 67.07 years (SD = ±5.69). Marital and living status were associated with individual’s COVID-19 infection history, with living with family linked to higher infection risk. The presence of underlying disease and social media use were significantly associated with quarantine history. QoL was associated with education, income, and physical and social activities, but not with COVID-19 history.
Conclusions:
Household health precautions should be emphasized. Chronic conditions and social media use were linked to quarantine, possibly due to challenges in maintaining in-person contact. Enhancing social and physical activities may improve QoL among older adults. These findings provide valuable insights for healthcare providers and policymakers to better support older adults in future health crises, including promoting social and physical engagement and addressing sociodemographic factors.
Significance for public health
This study examines the impact of COVID-19 on the quality of life (QoL) of urban older adults, with significant public health implications. Living with family members can increase infection risk, emphasizing the need for household health precautions. Those with chronic conditions and frequent social media use were more likely to be quarantined, which posed challenges in maintaining social connections and adhering to stay-at-home measures. Conversely, increased social activity and physical exercise were found to enhance QoL, regardless of COVID-19′s effects. The study also highlights the importance of early support in income and education to prevent QoL decline as the population ages. The experiences of older adults during the pandemic offer valuable insights for healthcare providers and policymakers, aiding in better preparedness for future health crises. These findings stress the importance of tailored interventions and proactive public health strategies to improve the well-being of older adults in post-pandemic societies.
Introduction
The coronavirus (COVID-19) pandemic, stemming from the SARS-CoV-2 virus, has had a lasting impact across all age groups. However, its effects have been particularly severe among older adults due to their increased vulnerability to infection and related complications.1 –3 From its initial detection in China in December 2019, the virus rapidly evolved into a global health crisis, alerting the World Health Organization (WHO) to declare it a Public Health Emergency of International Concern (PHEIC) in January 2020, followed by its classification as a pandemic in March 2020. 4 In Thailand, the first confirmed case was detected in early January 2020. The number of new cases increased rapidly, leading the government to classify COVID-19 as a dangerous communicable disease by late February. 5
The vulnerability of older individuals to severe infections has become a significant concern, 1 with the aftermath of recovery often marked by persistent symptoms known as “long COVID.” The condition could result in persistent symptoms such as fatigue, myalgia, breathlessness, chest tightness, and cognitive impairments like memory loss and difficulty concentrating.3,6 These ongoing effects highlight the long-term physical and mental health consequences of COVID-19, particularly for aging populations.
In addition to direct health impacts, the pandemic disrupted daily routines, reduced physical activity, and increased sedentary behavior.7,8 These lifestyle changes may pose substantial health risks, such as the development of chronic diseases, obesity, and mental health issues. 8 In May 2023, the WHO reclassified COVID-19 from a public health emergency to an ongoing health concern emphasizing the need for long-term strategies that address not only infection control but also post-pandemic health outcomes. 9
Quality of life (QoL) is defined by the WHO as “an individual’s perception of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.” It encompasses the relationships among physical health, psychological state, level of independence, social relationships, and the environment. 10 Multiple pre-pandemic studies identified factors such as sex, marital status, educational background, occupation, income, underlying health conditions, and physical activity as significant determinants of QoL in older adults.11 –13 However, the pandemic introduced new stressors. Social isolation, economic uncertainty, and family illness have been linked to reduced QoL.14,15 Although some studies assessed QoL following COVID-19 recovery, findings have varied across different QoL domains, indicating a lack of consensus.16,17
As Thailand undergoes rapid aging, transitioning into a “superaged society,” 18 aging presents a complex landscape and does not always represent a better QoL. 19 The WHO’s definition of healthy aging, emphasizing the maintenance of functional ability for well-being, has become increasingly important. 20 The overarching goal of promoting healthy aging is to enhance the QoL for the older adult population. 21 Aging, especially in urban areas, presents complex challenges that can adversely affect both physical, and psychological well-being. 22 Despite these issues, few studies have comprehensively examined the QoL of older adults in the post-COVID-19 period, particularly regarding the effects of infection and quarantine measures.
In the face of these considerations, this study investigates factors associated with QoL among older Thai adults after the pandemic, with particular emphasis on the impact of COVID-19 infection and quarantine history. By shedding light on the unique challenges faced by older individuals, this study aims to guide policymakers in formulating targeted strategies that can significantly contribute to the well-being and optimized quality of life of older adults.
Methods
Respondents and study design
This study presents a cross-sectional analysis of data collected from November 2023 to January 2024. The reporting of this study conforms to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement 23 (see Supplemental File 1). Older adult patients who visited a primary care clinic at the Faculty of Medicine, Vajira Hospital during the study period were invited to participate in the study. The inclusion criteria for respondents were as follows: (1) 60 years old or older, (2) able to speak and understand Thai language, and (3) absence of cognitive impairments. Ethical approval for the study was obtained from the Human Research Ethics Committee of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand. (COA 180/2566). All respondents agreed and signed an informed consent form prior to study participation.
Sample size calculations
The sample size was calculated based on the difference between two proportions using G*Power. Data from a previous study on the QoL of older adults were used as a reference. 24 Among the reported proportions of participants with good and poor QoL across various factors, the one that yielded the largest required sample size was selected to ensure adequate power. At a 5% significance level and 80% power, a sample size of 160 was calculated. After accounting for a 10% incomplete response rate, a total sample size of 178 was needed.
Data collection
The data collection involved face-to-face interactions, during which respondents were presented with an information sheet and requested to provide written informed consent. The respondents were given instructions to complete the questionnaire. For older adults facing challenges in reading and writing, proficient research staff read all the questionnaire items aloud in a clear, monotonal voice while maintaining a neutral facial expression. Subsequently, the staff recorded the respondents’ responses on their behalf. The questionnaire comprised three parts: (1) demographic section of factors associated with QoL, specifically designed based on a literature review (see Supplemental File 2); (2) history of COVID-19 infection and quarantine (see Supplemental File 2); and (3) QoL assessment using the 26-item WHOQOL-BREF-THAI. Missing data were identified post-collection and omitted from the final analysis without participant follow-up.
Independent variables
The independent variables primarily included sociodemographic factors,1,2,15,24 –34 which were investigated for their association with QoL and, in some cases, with a history of COVID-19 infection, and quarantine. The collected data included: Sex (Male/Female), age (in years), marital status (Single/Divorced/Widowed/Married), education background (Under bachelor’s degree/Bachelor’s degree or higher), occupation (employed/unemployed/retired), income (Insufficient /Sufficient), living status (Alone/With family/With others), health coverage (Civil Servant Medical Benefit Scheme (CSMBS)/Social Security Scheme (SSS)/Universal Coverage (UC)/Others), presence of underlying diseases (None/At least one underlying disease), amount of exercise (Less than 150 min/week/At least 150 min/week), social activity (None/Membership in at least one group), alcohol consumption history (Yes/No), smoking history (Yes/No), social media ability (Able to use/Unable).
Dependent variables
The study investigated two main areas as dependent variables: Quality of Life (QoL) and, in certain analyses, history of COVID-19 infection and quarantine:
Quality of Life (QoL): Assessed using the 26-item WHOQOL-BREF-THAI, which contains information on overall QoL and general health (2 items), physical health (7 items), psychological health (6 items), social relationships (3 items), and the environment (8 items). 35 The instrument demonstrated satisfactory internal consistency, with Cronbach’s alpha values of 0.94 for overall QoL, 0.73 for physical domain, 0.82 for psychological domain, 0.72 for social domain, and 0.84 for environmental domain. 36 Each item was evaluated using a five-point Likert scale. Values were transformed into scores ranging from 26 to 130 according to the WHO guidelines and were interpreted into three categories: low QoL (26–60 points), moderate QoL (61–95 points), and high QoL (96–130 points).10,35 This study classified QoL into binary variables: poor QoL (low to moderate QoL) and good QoL (high QoL). The dichotomization could provide a distinct difference between individuals with good QoL and those whose QoL is affected, which coincides with the goal of prevention.
History of COVID-19 infection and quarantine: This variable was treated as a dependent variable when examining its associations with sociodemographic factors. The collected data included: Self-history of COVID-19 infection, family history of COVID-19 infection, self-history of quarantine due to COVID-19, and family history of quarantine due to COVID-19. The four data were collected as Yes or No.
Data analysis
Statistical analysis was performed with STATA version 18.0 at the 5% significance level. Kolmogorov-Smirnov test was conducted to determine the normality of the data along with consideration of the data’s standard distribution and skewness. Demographic data were analyzed and reported using descriptive statistics. Pearson’s chi-square test was conducted to assess the association between sociodemographic factors and history of COVID-19 infection and quarantine.
A total of nine multiple binary logistic regression analyses were conducted to explore various associations. Five separate models were run to identify sociodemographic factors associated with QoL. Each model used a different QoL outcome as dependent variable: overall QoL, physical QoL, psychological QoL, social QoL, and environmental QoL. For all five models, all sociodemographic factors were simultaneously included as independent variables. Four additional binary logistic regression models were performed to specifically explore the association between history of COVID-19 infection and quarantine with overall QoL, modeled separately by self-history of infection, family history of infection, self-history of quarantine, and family history of quarantine. These four models were adjusted for the sociodemographic factors that were found to be significantly associated with any QoL domain in the initial five regression analyses.
Results
Sociodemographic characteristics of the study respondents
A total of 195 individuals participated in this study. The sociodemographic and clinical characteristics of the respondents are presented in Table 1. The majority of participants were female, with a mean age of 67.07 years (SD ±5.69). Most respondents were married, retired, and living with their families. A significant proportion reported having sufficient income and the ability to use social media, with over half also engaged in at least one social organization. In terms of health status, almost all respondents had at least one underlying disease, with dyslipidemia, hypertension, and diabetes mellitus being the most common. Additionally, about two-fifths of participants engaged in recommended levels of physical activity, while a smaller proportion reported histories of alcohol consumption or smoking.
Baseline characteristics of the respondents (n = 195).

CSMBS: civil servant medical benefit scheme; SSS: social security scheme; UC: universal coverage; UD: underlying diseases.
Associations between history of COVID-19 and sociodemographic characteristics
Table 2 presents the distribution of sociodemographic characteristics by history of COVID-19 infection and quarantine. Significant associations identified using Pearson’s chi-square test are indicated with asterisks. Marital status and living with family members were significantly associated with respondents’ history of COVID-19 infection. Additionally, having at least one underlying medical condition was significantly associated with a family history of quarantine. Lastly, the ability to use social media platforms was significantly associated with both having family members infected with COVID-19 and having a history of quarantine.
Distribution of sociodemographic characteristics by history of COVID-19 infection and quarantine.

Significant association at p < 0.05.
Factors associated with quality of life (QoL)
Most respondents reported moderate to poor overall quality of life (QoL). Table 3 presents the sociodemographic factors that were significantly associated with at least one QoL domain, as identified through multiple binary logistic regression analyses. Higher levels of education, sufficient income, regular physical activity, and participation in social activities were associated with better overall QoL.
Associations between sociodemographic data and all domains of quality of life (QoL).
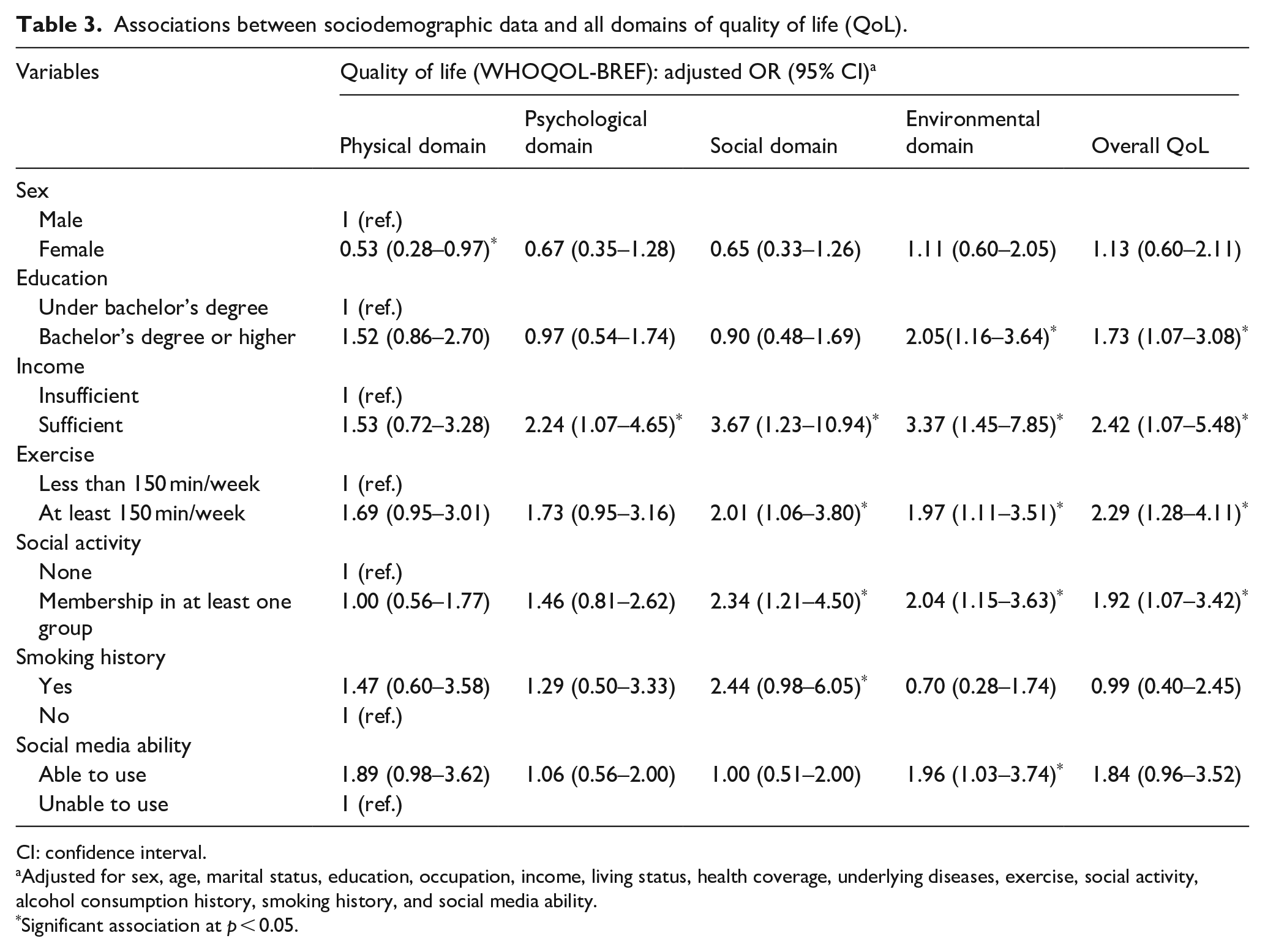
CI: confidence interval.
Adjusted for sex, age, marital status, education, occupation, income, living status, health coverage, underlying diseases, exercise, social activity, alcohol consumption history, smoking history, and social media ability.
Significant association at p < 0.05.
Sex was significantly associated with QoL in the physical domain, with men reporting better outcomes. In the psychological domain, sufficient income was linked to higher QoL. In the social domain, moderate to poor QoL was more common among non-smokers, while individuals who were socially and physically active reported significantly better outcomes.
In the environmental domain, lower education levels, insufficient income, and inability to use social media were associated with moderate to poor QoL. Conversely, individuals who engaged in at least 150 min of physical activity per week and those participating in social activities reported better QoL in this domain.
Despite the associations with various sociodemographic factors, an association between QoL and history of COVID-19 was not found, as depicted in Table 4.
Association between COVID-19 history and overall QoL.
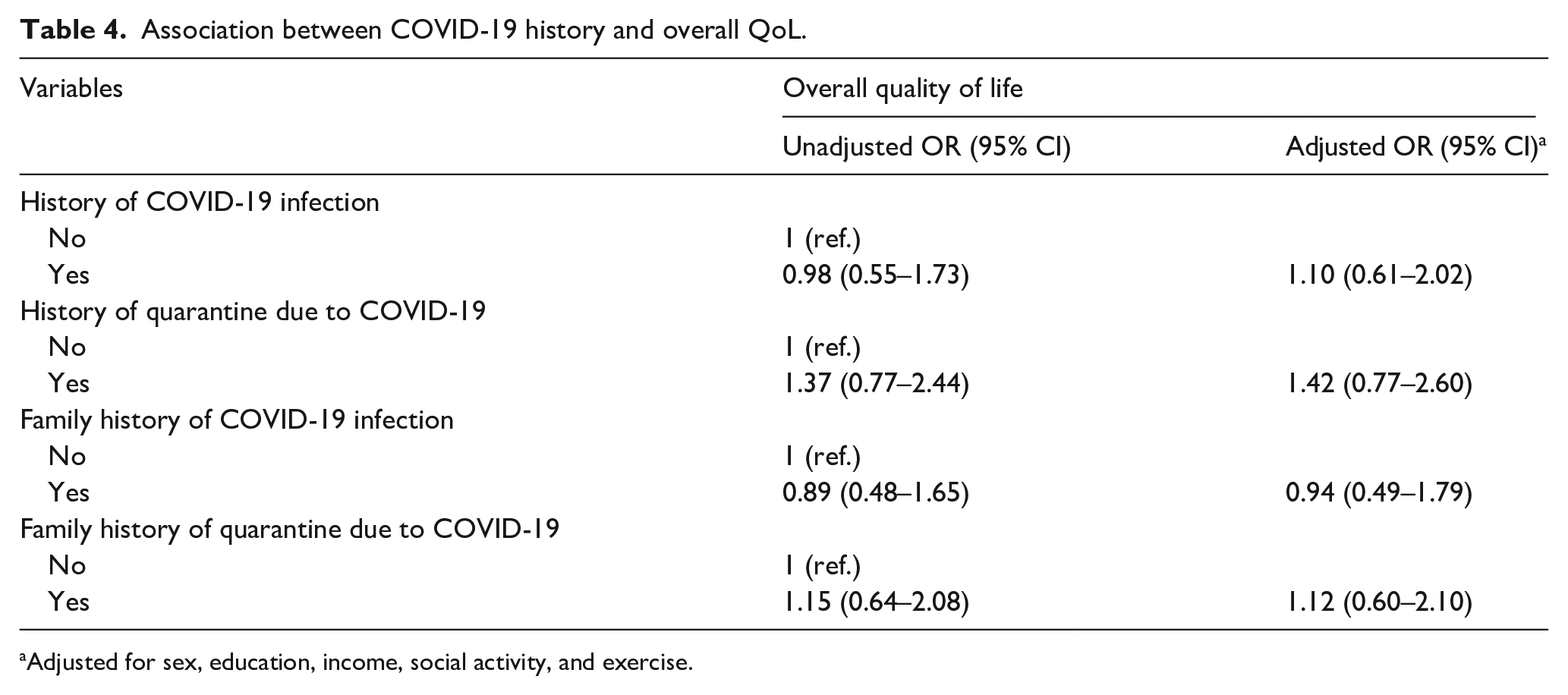
Adjusted for sex, education, income, social activity, and exercise.
Discussion
To the best of our knowledge, this is the first study to comprehensively assess the QoL of older adults in Thailand during the post-COVID-19 era, utilizing the WHOQOL-BREF, and simultaneously exploring associations with COVID-19 infection and quarantine history alongside various sociodemographic factors. Our findings offer valuable insights into the multifaceted well-being of this vulnerable population.
Associations with COVID-19 infection and quarantine history
Being married and living with family members were found to be associated with the risk of infection. Close contact with other residents is related to the transmission of COVID-19, either through droplets or direct contact. 37 The results suggest that having other members in the household could increase the likelihood of transmission and the risk of infection among household members. Our findings align with previous results from China and India,38,39 which suggested that close household contact increases the risk of SARS-CoV-2 transmission among family members and the frequency of contact. This underscores the critical need for enhanced health-protective behaviors within households, not only during pandemics but also for preventing other infectious diseases.
Furthermore, the presence of at least one underlying medical condition was significantly linked to a family history of being quarantined. This may reflect a heightened awareness among family members of the potential severity of COVID-19 in older adults 2 with comorbidities, leading to more stringent self-isolation measures to protect vulnerable household members.40,41 Furthermore, this study revealed a significant association between a family history of quarantine and older adults who had the ability to use social media platforms. During the pandemic, social activities often shifted online, leading to increased social media use, especially among older adults during quarantine.7,42 However, increased social media use can lead to reduced physical activity and sedentary lifestyles.43,44 Our findings suggest that quarantine measures may inadvertently promote sedentary behaviors, highlighting the importance of primary care interventions to encourage physical activity, particularly for older adults with chronic diseases.
Factors associated with quality of life
Most respondents reported moderate to poor overall QoL, and multivariable analyses identified several key sociodemographic factors significantly associated with overall QoL and its specific domains.
Sufficient income was significantly associated with better overall QoL, as well as psychological and environmental domains. This observation was consistent across various economic development settings,45 –48 highlights how higher income facilitates access to better living conditions, services, and healthcare, thereby positively influencing well-being. Moreover, a higher level of education was significantly associated with good QoL, especially in the environmental domain. This aligns with research suggesting that better education can lead to improved health awareness, access to healthcare, and enhanced living standards.27,47,49 These findings emphasize the long-term importance of socioeconomic support, especially given the pandemic’s impact on education and income.48,49
Engaging in regular exercise was associated with good QoL across multiple domains, including overall QoL, social, and environmental domain. This reinforces well-established benefits of exercise on mental health, physical function, and cognitive function.26,50 Previous findings also suggest that regular exercise could also connects isolated individuals, leading to increased socialization and improvement in overall QoL. 31 This study suggests that primary care providers should not only advise regular physical activity but also collaborate with the government to promote outdoor and virtual classes to prepare for the next pandemic or for individuals who may find it difficult to engage in exercise outside of their homes.
Similarly with exercise, participation in social activities was significantly associated with better overall QoL, social, and environmental domain. This supports the activity theory of aging, where maintaining social engagements contributes to personal identity, self-esteem, healthy behaviors, and ultimately QoL.51,52 Better access to green or public spaces could be a factor that encourages individuals to participate in social activities, therefore improving health. 53 Our study suggested that older adults should have membership in at least one organization, group, or association to improve overall QoL. Policymakers should consider developing accessible public spaces that encourage physical and social activities to improve overall well-being in aging populations.
Associations between a history of COVID-19, both infection and quarantine, and QoL were not found in this study. Concurrently, a study also reported similar QoL between recovered COVID-19 patients and the general population after a period of recovery, 33 while the other found an improvement in QoL upon recovery. The severity of COVID-19 infection was found to have a significantly negative impact on QoL. 17 The overall moderate to poor QoL could be due to lock downs and other prevention measures which affect every individual, regardless of their infection history. This suggests that support for QoL enhancement should be universally provided to all individuals, irrespective of their COVID-19 history, particularly within vulnerable populations.
Strengths and limitations
This study’s strengths include its focus on older adults in the post-COVID-19 era, use of the standardized WHOQOL-BREF-THAI, and the comprehensive assessment of various sociodemographic factors with both COVID-19 history and QoL.
This study has several limitations. First, its cross-sectional design limits the establishment of causal relationships between the variables and the QoL of older adults. Second, the study’s inclusion criteria, limited to older adults attending a specific primary care clinic, may restrict the generalizability of findings to those with limited healthcare accessibility or different socioeconomic backgrounds. Lastly, although logistic regression was used in the final analysis, the sample size was not originally calculated based on a regression model framework. Instead, a more conservative sample size estimate was employed to maximize statistical power and account for potential incomplete responses. Ultimately, the number of participants exceeded the minimum required for regression analysis. Further studies could involve multiple centers, adopt a community-based approach, and utilize a cohort design to provide better insight into the matter.
Implications for public health and clinical practice
To summarize, this study highlights the fact that the COVID-19 pandemic and infection control policies could have long-term consequences for everyone, especially vulnerable populations such as older adults and those with comorbidities. Lessons learned from the COVID-19 pandemic could be applied in primary care clinics, such as routinely providing recommendations for understanding contact and standard precautions at home. Since primary care clinics are often the first point of contact for infected individuals, during their visit at the clinic could be a good opportunity to provide essential information. Additionally, our study emphasizes the role of healthcare providers in encouraging older adults to be more active, such as by engaging in social activities and exercise. This not only improves physical and psychological health but also enhances overall QoL and promotes comprehensive geriatric care. Although not every province has a geriatric clinic, this intervention may help prevent functional decline in older adults, especially those with underlying diseases who are at risk of decline, and may face increased quarantine measures. Policymakers play a crucial role in providing adequate social activity and exercise opportunities, as well as addressing education and income sufficiency to prepare for future pandemics, not limited to addressing infection control measures alone.
Conclusions
In conclusion, this study examined factors influencing QoL among the aging population post-COVID-19. Sociodemographic factors such as education, income, physical activity, and social engagement significantly affect QoL. Those living with family members face greater COVID-19 infection risks, emphasizing the need for health-protective behaviors within households. Individuals with chronic conditions and social media usage were more likely to be in quarantine, potentially facing challenges in maintaining in-person contact and adhering to stay-at-home measures due to the pandemic. Promoting social activities and regular exercise is crucial for overall QoL improvement. While no direct link was found between COVID-19 history and QoL, this study highlights the importance of comprehensive geriatric care and proactive measures. Policymakers, healthcare providers, and researchers must prioritize targeted strategies to promote healthy aging and enhance QoL, particularly among vulnerable older adults in urban areas post-pandemic and future health crises.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251373005 – Supplemental material for Quality of life and influencing factors among older adults in the end of COVID-19 era: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036251373005 for Quality of life and influencing factors among older adults in the end of COVID-19 era: A cross-sectional study by Witchaya Sitthisasithorn and Sivarat Ratthanasathian in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251373005 – Supplemental material for Quality of life and influencing factors among older adults in the end of COVID-19 era: A cross-sectional study
Supplemental material, sj-docx-2-phj-10.1177_22799036251373005 for Quality of life and influencing factors among older adults in the end of COVID-19 era: A cross-sectional study by Witchaya Sitthisasithorn and Sivarat Ratthanasathian in Journal of Public Health Research
Footnotes
Acknowledgements
The authors express their gratitude to all respondents in this study.
Ethical consideration
The study was performed in accordance with the Declaration of Helsinki and was approved by the Human Research Ethics Committee of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand (COA 180/2566).
Consent to participate
All respondents agreed and signed an informed consent form prior to study participation.
Consent for publication
Consent for publication was received from respondents prior to data collection.
Author contributions
All authors read and approved the final manuscript. WS contributed substantially to the conception, study design, execution, data acquisition, analysis, interpretation, and drafting of the manuscript. SR contributed substantially to the conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting and revising the manuscript; and gave final approval of the version to be published. All authors agreed on the journal of submission and accept responsibility for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. However, the article processing charge (APC) was financially supported by Navamindradhiraj University.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The dataset generated during the current study is available upon request from the corresponding authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.