
Abstract
Context:
While it is well-known that age and race/ethnicity have been associated with poor COVID-19-related outcomes, it is less clear if vulnerable populations consistently experienced higher rates of poor outcomes over time.
Objective:
Considering this, our study compared COVID-19-related outcomes by age group and racial/ethnic group across variant-dominant periods to assess how poor outcomes were experienced over time in Oklahoma County.
Design and methods:
In this retrospective observational study, we used health department surveillance data to compare COVID-19-related average daily case, hospitalization, and case fatality rates across three time periods–each dominated by different SARS-CoV-2 variants in Oklahoma County, Oklahoma, US.
Results:
When comparing across variant-dominant time periods, with respect to age, we observed that people age 65+ years consistently had the highest average daily rates of COVID-19-related hospitalization and death. With respect to race/ethnicity, we observed that American Indian/Alaska Natives consistently experienced the highest case rate, that Black people experienced high rates of hospitalization during the pre-Delta- and Delta-dominant time periods, and White people consistently experienced the highest rate of death. Hispanic people experienced the first surge of cases in the pandemic and subsequently had relatively low rates of COVID-19-related outcomes. Asian/Pacific Islanders had relatively low rates of COVID-19-related outcomes except a relatively high rate of death late in the Omicron-dominant period.
Conclusion:
There is little evidence to suggest that once a segment of the population experiences high rates of COVID-19-related outcomes that they will benefit from lower rates of outcomes in subsequent variant-dominant time periods.

Introduction
Oklahoma County, the most populous county in the State of Oklahoma, encompasses the Oklahoma City metropolis and nearly mirrors the racial/ethnic distribution of the United States (US). 1 In Oklahoma County, the first reported case of COVID-19 was on March 12, 2020 with cases reported in every county in the state since. During the COVID-19 pandemic study period (March 12, 2020–Feb 28, 2022), 194,928 cases, 7043 hospitalizations and 2428 deaths associated with COVID-19 have been reported in Oklahoma County. SARS-CoV-2, the virus that causes COVID-19, has genetically drifted during the pandemic resulting in the emergence and persistence of multiple variants. Largely because of their varying transmissibility and severity, the variants that emerged over the course of pandemic have not been of equal risk and concern. The original Alpha variant, Delta variant, and Omicron variant have been found to be the most dominating variants in the US and are largely responsible for the major surges at different time intervals over the course of pandemic. 2 In Oklahoma County, the Alpha variant was responsible for a surge December 2020–January 2021 while the Delta variant surge occurred August-November 2021 and the Omicron variant surge occurred December 2021–February 2022.
Numerous studies in the US and elsewhere have reported inequitable impacts and outcomes of COVID-19 within and among communities. The demonstrated pattern largely depicts disproportionate impacts on racial/ethnic minority populations.3–5 COVID-19 outcomes have also been shown to be related to age with increased disease severity in older populations. 6 Race/ethnicity and age were selected as factors to examine because they are linked to systemic inequalities and presence of comorbidities, making them a key starting point for understanding disparities. Examining how outcomes vary by race/ethnicity and age over time enables identification of disparities and understanding of their progression. Given the unique composition and history of each community in the US, along with varying geographic, demographic, and political settings, decoding and understanding these patterns at a finer geographic and temporal scale provides more insight into the relationship between the COVID-19 pandemic and different demographic strata of community and their manifested outcomes.7–9
Our earlier research on racial/ethnic-specific outcomes found that the effects of COVID-19 have been unevenly distributed and unequal within and among different communities in Oklahoma County. We observed that the Hispanic population was the first to surge in cases and hospitalizations, and non-Hispanic Black people experienced the highest hospitalization and death rates in Oklahoma County in the winter of 2020. 1 However, there is a lack of comparative evaluation and understanding of COVID-19-associated cases, hospitalizations, and deaths due to variants that emerged and dominated during different time periods. Understanding the inequitable impact of variant-driven surges at a finer scale aids in effective preparedness, educated policy formulation, and efficient resource allocation to attain equitable health outcomes in the community. With these understandings in mind, this study aimed to explore and synthesize the impacts of COVID-19 in Oklahoma County during different time periods propelled by SARS-CoV-2 variant dominance. In particular, the study compares COVID-19 daily average case, hospitalization, and case fatality rates by age group and racial/ethnic group across variant-dominant periods to assess how poor outcomes were experienced over time.
Design and methods
In this retrospective observational study, the source population includes people living within the jurisdiction of Oklahoma County, Oklahoma, US. Surveillance data—reported to the Oklahoma State Department of Health (OSDH)—of COVID-19 cases residing in Oklahoma County were included in this analysis. Cases were obtained through several reporting sources including labs and healthcare facilities. Any cases with unknown and/or non-reported race/ethnicity were excluded from analyses involving racial/ethnic groups. Race/ethnicity was categorized as non-Hispanic American Indian/Alaska Native, non-Hispanic Asian/Pacific Islander, non-Hispanic Black, non-Hispanic White, (hereinafter referred to as American Indian/Alaska Native, Asian/Pacific Islander, Black, and White) and any person with Hispanic origin. Age was categorized into groups of <18, 18–35, 36–49, 50–64, and 65 years and older. Using OSDH variant reports, 10 we categorized the COVID-19 pandemic into three periods: pre-Delta-dominant period (March 12, 2020–May 31, 2021; 445 days), Delta-dominant period (June 1, 2021–Nov 30, 2021; 182 days), and Omicron-dominant period (Dec 1, 2021–Feb 28, 2022; 89 days). While the pre-Delta-dominant period includes the time period with dominance of the Alpha variant and any other variants leading up to Delta dominance, Delta- and Omicron-dominant periods include the time periods when at least 50% of the sequenced isolates were the Delta variant (B.1.617.2) and Omicron variant (B.1.1.529), respectively, in the study area. Although the Omicron variant accounted for over 50% of sequenced isolates well past February 28, 2022, the study period ended due to a substantial increase in people using in-home testing which likely changed trends in surveillance data reporting.
We calculated daily average case, hospitalization, and case fatality rates by age group and racial/ethnic group for each of the three variant-dominant periods and compared them. Addressing the population at risk, we calculated case rates by taking the number of COVID-19 cases divided by population size of each demographic group as the denominator using estimates from the US Census Bureau. 11 We calculated hospitalization and case fatality rates using the number of hospitalizations and deaths, respectively, divided by the number of COVID-19 cases in each demographic group as the denominator. COVID-19 contributing cause deaths used in case fatality rate estimates were determined using OSHD coding on patient death from the disease, primarily from direct reporting from healthcare facilities. One-way ANOVA, a statistical test used to analyze differences between the means of groups, was performed to compare the daily average rates between the three periods. Comparisons were conducted collectively by racial/ethnic and age groups to examine disparities within and across time periods. We also performed Tukey’s HSD test for multiple comparisons. A type I error rate of 0.05 was used to test for statistical significance. Statistical analyses were conducted in the R Project for Statistical Computing. 12
Results
A total of 194,928 COVID-19 cases were reported during three variant-dominant periods in Oklahoma County. The daily average case rate of 101.05 cases/day (95% CI = 78.79–123.32) during the Omicron-dominant period was significantly higher than that of the pre-Delta-dominant-period at 24.13 cases/day (95% CI = 21.66–26.59) and Delta-dominant period at 24.97 cases/day (95% CI = 21.99–27.95; F(2,716) = 118.9, p < 0.001)
A total of 7043 COVID-19-associated hospitalizations were reported during the three different periods in Oklahoma County. The daily average hospitalization rate of 15.95 hospitalizations/day (95% CI = 13.84–18.07) during the Delta period was significantly higher than during the pre-Delta-dominant period at 7.67 hospitalizations/day (95% CI = 7.06–8.28) and Omicron-dominant period at 11.07 hospitalizations/day (95% CI = 9.68–12.46; F(2,716) = 52.47, p < 0.001).
There were 2428 COVID-19-associated deaths reported during the study period. The daily average case fatality rate was significantly higher during the Delta-dominant period at 6.78 deaths/day (95% CI = 5.77–7.79) and Omicron-dominant period at 6.97 deaths/day (95% CI = 5.88–8.05) than during the pre-Delta-dominant period with 4.00 deaths/day (95% CI = 3.57–4.43; F(2,716) = 23.58, p < 0.001). However, the daily average case fatality rates during the Delta- and Omicron-dominant periods were not significantly different from each other. The daily average case fatality rate was highest during the Omicron-dominant period, yet, the total number of deaths was greatest during the pre-Delta-dominant period (1530 deaths; Figure 1).
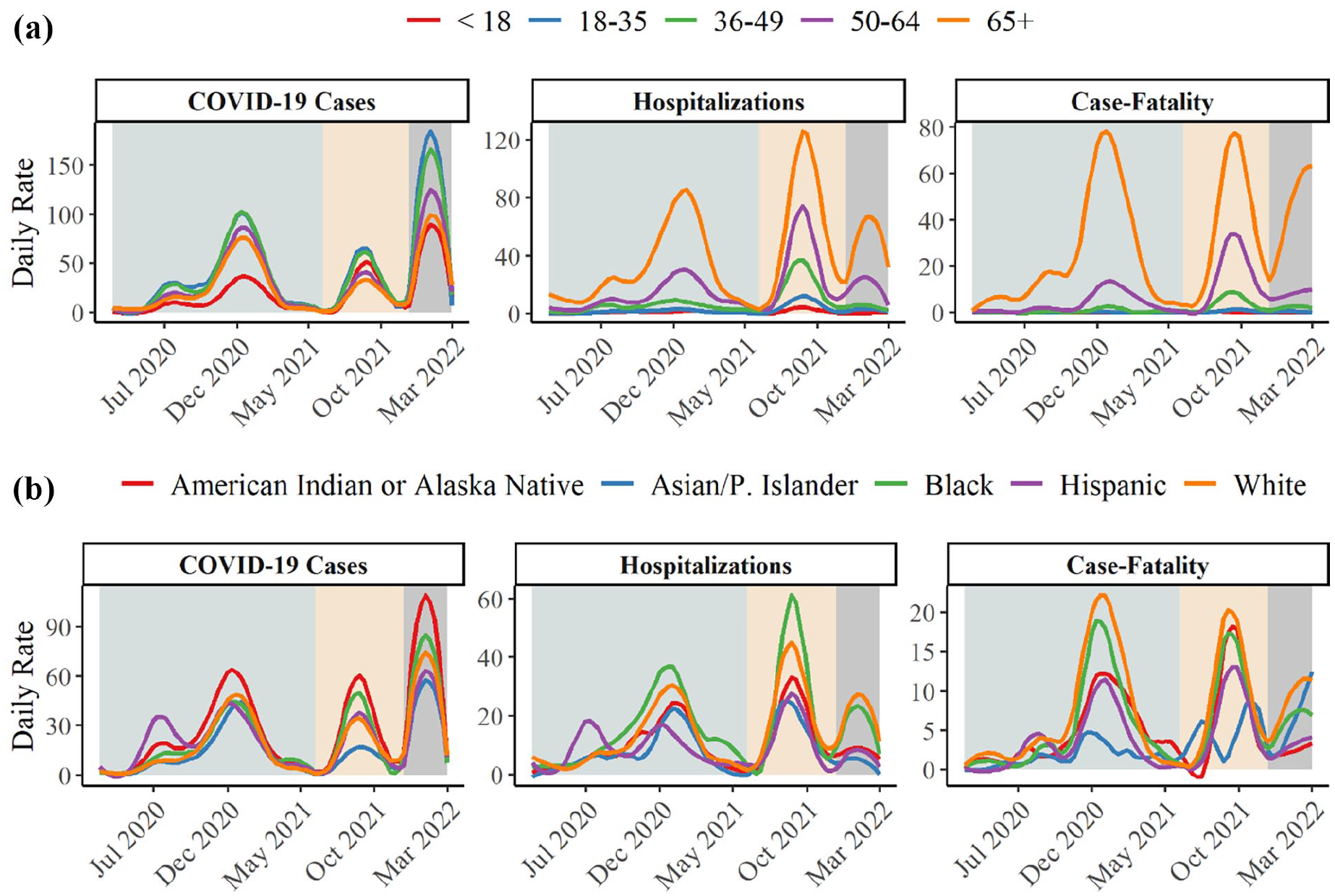
Daily case*, hospitalization, and case fatality rate** smoothed trend lines during three variant-dominant periods in Oklahoma County, March 12, 2020–February 28, 2022. (a) Daily rate by age group. (b) Daily rate by race/ethnicity.
Daily rates by age group
COVID-19 cases
Age groups saw a decline in daily average case rates from the pre-Delta-dominant period to the Delta-dominant period followed by a drastic increase during the Omicron-dominant period. The 18–35 years age group had the highest daily average case rates during all three variant-dominant periods compared to other age groups.
COVID-19 hospitalization
The oldest population (65+ years) had the highest daily average hospitalization rate during all three variant-dominant periods. The daily average hospitalization rates for all age groups dropped during the Omicron-dominant period compared to the Delta-dominant period. For example, the daily average hospitalization rate for those 50–64 years and those 65+ years decreased from the Delta-dominant period with 30.78 hospitalizations/day (95% CI = 26.35–35.20) and 60.69 hospitalizations/day (95% CI = 53.82–67.57), respectively, to 19.25 hospitalizations/day (95% CI = 17.17–21.34) and 57.13 hospitalizations/day (95% CI = 49.95–64.31), respectively, during the Omicron-dominant period. Further, a gradient was seen where hospitalization rate increased as age increased across all three variant-dominant periods.
COVID-19 case fatality
Similar to the observed hospitalization rates, those age 65+ years had the highest daily average case fatality rate during all three periods (pre-Delta: mean = 23.79 deaths/day, 95% CI = 21.44–26.15, Delta: mean = 37.54 deaths/day, 95% CI = 33.05–42.02, Omicron: mean = 47.01 deaths/day, 95% CI = 40.50–53.51). Like with hospitalization, case fatality rates increased as age increased (Table 1).
Daily average rates (95% confidence interval) by age group across variant-dominant periods in Oklahoma County, March 12, 2020–February 28, 2022.

Number of COVID-19 cases per 100,000 population. Number of COVID-19-associated-hospitalizations and deaths per 100,000 COVID-19 cases. Data were reported to the Oklahoma State Department of Health.
Daily rates by race/ethnicity
COVID-19 cases
The daily average case rate was higher for American Indian/Alaska Native people than for all other racial/ethnic groups during the three variant-dominant periods (pre-Delta: mean = 21.42 cases/day, 95% CI = 19.28–23.56; Delta: mean = 27.82 cases/day, 95% CI = 24.12–31.52; Omicron: mean = 81.48 cases/day, 95% CI = 61.70–101.25) while Asian/Pacific Islander people experienced the lowest case rates. Among Hispanic people, cases peaked earlier (at 53.18 cases/day) in the pre-Delta-dominant period than other racial/ethnic groups.
COVID-19 hospitalization
Black people experienced consistently high daily average hospitalization rates across all three variant-dominant periods with the highest hospitalization rates during the pre-Delta- and Delta-dominant periods, and second highest hospitalization rate, after White people, during the Omicron-dominant period. Hispanic people experienced the first peak of hospitalization rates and reached a maximum rate of 25.00 hospitalizations/day per 100,000 population during the early phase of the pre-Delta-dominant period. After the initial peak, hospitalization rates stayed relatively low for Hispanic people. Hospitalization rates remained lowest in Asian/Pacific Islander people throughout all variant-dominate periods.
COVID-19 case fatality
The daily average case fatality rates were highest in White people across all variant-dominant periods (pre-Delta: mean = 6.58 deaths/day, 95% CI = 5.90–7.26, Delta: mean = 9.26 deaths/day, 95% CI = 8.05–10.48, Omicron: mean = 9.37 deaths/day, 95% CI = 8.19–10.55) closely followed by Black people (pre-Delta: mean = 5.07 deaths/day, 95% CI = 4.49–5.66, Delta: mean = 7.60 deaths/day, 95% CI = 6.45–8.75, Omicron: mean = 6.47 deaths/day, 95% CI = 5.45–7.48). Although Black people experienced the highest hospitalization rates, the case fatality rates were not as stark of a trend. Conversely, White people had the highest rate of deaths after only seeing moderate case and hospitalization rates. American Indian/Alaska Native people had the highest case rates throughout, yet it did not translate into high hospitalization or case fatality rates. The earliest peak in COVID-19-related-deaths was experienced by Hispanic people and reached a maximum rate of 11.88 deaths/day per 100,000 population beginning in August 2020. The second peak (still characterized as the pre-Delta-dominant period), third peak (Delta-dominant period), and fourth peak (Omicron-dominant period) were most experienced by White and Black people. Asian/Pacific Islander people experienced low case fatality rates aside from a relatively high case fatality rate late in the Omicron-dominant period (Table 2).
Daily average rates (95% confidence interval) by race/ethnicity group across variant-dominant periods in Oklahoma County, March 12, 2020–February 28, 2022.

Number of COVID-19 cases per 100,000 population. Number of COVID-19-associated-hospitalizations and deaths per 100,000 COVID-19 cases. Data were reported to the Oklahoma State Department of Health.
Discussion
The results from this descriptive epidemiological study of COVID-19 by variant-dominant periods (or casually referred to as waves), reveal both important differences and stark patterns by age group and race/ethnicity. First, a high age- or racial/ethnic-specific COVID-19 case rate did not necessarily correspond to a high COVID-19-related hospitalization or case fatality rate. Second, experiencing a high case/hospitalization/case fatality rate during an early phase of the pandemic did not predict protection during later phases of the pandemic as rates varied by each variant-dominant period without a clear pattern of decline as the pandemic went on. These results are meaningful because they shed light on the limits of the expected accruement of population immunity within population segments over time. Further, they highlight that health disparities persist by age and race/ethnicity across variant-dominant periods and demonstrate the need to consistently prevent disease transmission in each population segment.
The results show that both case and hospitalization rates remained relatively low during the pre-Delta-dominant period. Safer at Home orders were issued during this time from March 24 to May 6, 2020 in Oklahoma. Our results fall in line with studies that have found higher hospitalization rates during the Delta-dominant period.13,14 High virulence and waning immunity from the primary vaccine doses were contributing factors to the heightened hospitalization rates before the first booster was made available in September 2021. We observed disproportionality in hospitalization and case fatality rates compared to case rates during the Omicron-dominant period. The high case rates during the Omicron-dominant period could be attributed to the enhanced infectivity of the variant15,16 and its increased transmissibility with a higher reproduction number compared to previous variants. 17 Although case rates were drastically higher during the Omicron-dominant period compared to the pre-Delta- and Delta-dominant periods, hospitalization and case fatality rates during the Omicron-dominant period stayed relatively low.13,14
There was hope that the combination of infection-induced and vaccine-induced immunity would build sufficient population-level immunity to reduce the risk of COVID-19-related outcomes, particularly among those at greatest risk of severe outcomes. 18 Unfortunately, we observed a consistently high, concentrated and skewed severity largely toward the older population throughout the COVID-19 pandemic. Their daily hospitalization and case fatality rates were high during all periods with significant disparity between each variant-dominance. The disproportionate impact on the older population (65+ years) is likely associated with weakened immune systems and underlying comorbidities19,20 that potentially increased their susceptibility. Those age 65 years and older were the first age group to become COVID-19 vaccine eligible in Oklahoma County and elsewhere in the US. Acquired immunity from vaccination is potentially the reason this age group had decreased daily average case rates of COVID-19 during the Delta-dominant period compared to the pre-Delta-dominant period.21,22 By the end of the pre-Delta-dominant period (May 31, 2021), fully-vaccinated status by age groups was: 72.3% of those age 65+ years, 54.5% of those age 50–64 years, 43.8% age 36–49 years, 31.1% of those age 18–35 years, and 2% of those age < 18 years in Oklahoma County. Age groups 12–15 years, 5–11 years and 6 months–5 years became vaccine eligible in the study area in May 2021, November 2021 and June 2022, respectively. Resurgence of severity with increased daily average case and case fatality rates during the Omicron-dominant period is possibly due to waning/incomplete immunity and low proportions of boosted population with additional doses of vaccine. 23 Additionally, age groups 18–35 and 36–49 years had the highest daily average case rate during all the three variant-dominant periods. While they did not experience the significant burden of hospitalization and death, they appear to be the major potential spreader during all the three periods. These age groups were often more engaged in public activities, driven by a perception of lower vulnerability to COVID-19 and desire to maintain a sense of normalcy after pandemic fatigue.24,25
The impact of COVID-19 on race/ethnicity across variant dominant periods is also noteworthy. The daily case, hospitalization, and case fatality rates among Hispanic people surged much earlier than other groups and even before the pre-Delta peak. 1 Black people, on the other hand, had the highest daily average hospitalization rates during the pre-Delta- and Delta-dominant periods. They also had the second highest daily average case fatality rates during all three variant-dominant periods with the highest occurring in White people. This could be due to age-related factors and pre-existing conditions observed in White populations in the state. Nationwide, Black and Latino communities have faced disproportionately high rates of mortality associated with COVID-19. American Indian/Alaska Native people had the highest reported daily average case rate during all three variant-dominant periods. Such a temporal disparity in COVID-19 outcomes is probably a reflection of disparity in vaccination coverage, and inequitable distribution of stressors that potentially affect a wide spectrum of health outcomes, in turn increasing the severity of COVID-19.26–29 Oklahoma is a relatively strong vaccine-hesitant south-central state in the US. The COVID-19 vaccine hesitancy for Oklahoma County has been estimated at 17% by the CDC 30 while another survey found unwillingness to be vaccinated as high as 32% in Oklahoma. 31 We observe a significant disparity in vaccine uptake among racial/ethnic groups within these already high vaccine-hesitant populations. By the end of the pre-Delta-dominant period, 18.4% of Black people, 22% of Hispanic people, 26.4% of American Indian/Alaska Native people and 33.1% of White people were fully vaccinated in Oklahoma County. By the end of the Delta-dominant period, 30.5% of Black people, 39.8% of Hispanic people, 37.6% of American Indian/Alaska Native people, and 43.2% of White people were fully vaccinated. Asian/Pacific Islander people remained the leading racial/ethnic group for vaccine uptake (43.6% vaccinated by the end of pre-Delta and 57.8% vaccinated by the end of Delta dominance) and also bore a low burden of COVID-19 morbidity and mortality during all three variant-dominant periods. Furthermore, we observe a significant disparity in socio-economic factors between different racial/ethnic groups. For example, in the United States, the median household income for Black, Hispanic, and White people is $48,297, $57,981, and $77,999, respectively. 32 The home ownership rate in Black people is 44.2% compared to 48.4% in Hispanic people and 74.1% in White people. 33 Health disparities and structural racism are complex issues that have been shown to induce long-term impacts on the health of vulnerable populations. 1 Social, environmental, and economic stressors have contributed to poor health and caused health disparities between communities. 29 Social stressors, such as discrimination in healthcare, and environmental stressors, such as disproportionate exposure to air pollution, have been linked to asthma, obesity, cardiovascular disease, and high blood pressure in minority populations. The disproportionately high prevalence of comorbidities in these populations also likely contributed to the adverse outcomes experienced during the pandemic. 26 Additionally, socioeconomic status and access to care often intersect and shape health outcomes across all racial groups, including White populations. It is important to note that the comparisons by age and race/ethnicity were descriptive in nature and our analyses did not account for potential confounding variables.
Most diseases have a subset of a population and/or a community that are disproportionately more susceptible to disease and are thus more vulnerable compared to others. 34 While part of this is determined by behavior of a pathogen and innate immunity of the individuals to resist that pathogen, it is also largely determined by synergistic effects of social, environmental, and economical stressors and their differential distribution in the communities. 29 Because of unique characteristics driven by a distinct composition of demographic, social, economic, behavioral, political, and cultural factors, each community responds differently and uniquely to a public health crisis, both spatially and temporally. So, it is important to identify the most vulnerable populations/communities to direct the resources and increase attention for better response. Analyzing the impacts of a pandemic and/or disease at a finer scale not only helps to better understand the disease but also provides information for effective and efficient planning for similar crises in the future. 35 While there are many studies that have reported inequitable impacts of COVID-19 in US communities and elsewhere,35–37 this is among the few studies, as per our knowledge, to synthesize and compare the epidemiologic disparity between the time periods driven by different variants that emerged, endured and exacerbated the public health crisis along the course of the pandemic. 38
This study is subject to certain limitations and challenges. Public health surveillance data were used. While public health agencies attempt to use a standardized approach to data collection, certain factors can affect data quality, including patient volume, availability of testing sites, availability and type of tests, access to health care, and requirements for testing at hospital admission. Data could have been misclassified due to variations across reporting sources and potential differing death determinations. There were societal factors changing over time as well, including masking policies. Despite these challenges, there were not any specific changes that affected people by age, race, or ethnicity that would be expected to invalidate the study results. We compared rates of COVID-19-related outcomes by variant-dominant period; however, the length of these periods were unequal and hence daily rates were the primary measure of disease incidence. Interpreting disease incidence at the daily level may detract from appreciating the magnitude of the disease burden.
Conclusions
Our study found heterogeneous patterns in age and racial/ethnic strata such that public health and policy leaders cannot rely on previous COVID-19 peaks to confer protection against subsequent peaks caused by new variants of COVID-19. Ongoing resources need to be directed at reducing COVID-19-related hospitalization and death among vulnerable populations. Across three variant-dominant periods in Oklahoma County, the oldest people remained highly susceptible to morbidity and mortality throughout the COVID-19 pandemic and young and middle-aged adults experienced high rates of infection that contributed to viral transmission. Additionally, minoritized populations were the early target of the pandemic though the impact borne by each community varied across different variants. The results demonstrate differential COVID-19 outcomes likely influenced by response efforts, vaccination coverage, and inequitable distribution of stressors.
Significance for public health
Results highlight that health disparities persist by age and race/ethnicity across variant-dominant periods and demonstrate the need to consistently prevent disease transmission in each population segment. Continued resources are needed to reduce COVID-19-related hospitalization and death, especially among vulnerable populations.
Footnotes
Acknowledgements
We would like to extend our appreciation to our colleagues at the Oklahoma City-County Health Department, including Astrian Horsburgh for her key contributions and Phil Maytubby for his leadership.
Consent to participate
The informed consent statement clarifies that IRB approval was exempted due to the retrospective nature of the study, and the study was approved by the University of Oklahoma Institutional Review Board (IRB #14281).
Author contributions
Conceptualization, J.B., K.K. (Kapil Khadka), M.C., K.A., K.K. (Katrin Kuhn), and A.W.; methodology, J.B., K.K. (Kapil Khadka), M.C., K.A., K.K. (Katrin Kuhn), and A.W.; software, J.B. and K.K. (Kapil Khadka); validation, J.B. and A.W.; formal analysis/investigation/data curation, K.K. (Kapil Khadka); writing—original draft, J.B., K.K. (Kapil Khadka), and A.W.; writing—review and editing, J.B., K.K. (Kapil Khadka), M.C., K.A., K.K. (Katrin Kuhn), and A.W.; supervision, K.K. (Katrin Kuhn) and A.W. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available because we are treating them consistently with all other public health disease surveillance data managed by the Oklahoma City County Health Department.
Human participant compliance statement
Not applicable. With the use of de-identified, aggregate data, an Institutional Review Board review was not required.