
Abstract
Background:
The digitalisation of healthcare has introduced virtual consultations as a means of improving accessibility and efficiency. However, the adoption of this technology among hospital doctors remains slow due to concerns about patient safety, quality of care, usability, and medico-legal implications.
Aim:
This study examines hospital doctors’ perceptions of digital virtual consultations, identifying key factors influencing their acceptance and implementation.
Design and methods:
A structured survey based on the Technology Acceptance Model 3 (TAM3) was distributed to 886 hospital doctors in a tertiary hospital in Malta. A total of 133 responses were received (15% response rate), with 67% of respondents completing the full questionnaire. The survey measured key variables such as perceived usefulness, perceived ease of use, job relevance and behavioural intention. Statistical analyses included Fisher’s exact test, Friedman’s test and ANOVA to explore significant relationships among variables.
Results:
The findings suggest that while doctors acknowledge virtual consultations as beneficial adjuncts to face-to-face consultations, concerns persist regarding technological infrastructure, usability and cost-effectiveness. Job relevance (p = 0.028) and perceived external control were significant predictors of perceived usefulness and ease of use. Behavioural intention was most strongly influenced by perceived usefulness (p < 0.001). Despite the insights offered, the 15% response rate may introduce non-response bias, limiting the generalisability of findings across the wider population of hospital doctors.
Conclusions:
To enhance adoption, healthcare systems must invest in infrastructure, training, and policy frameworks. Conducting feasibility and cost-effectiveness studies, coupled with stakeholder engagement, will be essential for successful implementation.
Background
Worldwide, countries and their health care systems are facing challenges brought about by the changing demography, increasingly ageing populations, geographical barriers, and rising costs of health care provision.
1
These pressures contribute to waiting times, generating concern in patients regarding access to care and leading to a weakening of the doctor
The World Health Organisation (WHO) defines ‘telemedicine’ as the utilisation of information and communication technology (ICT) by health care professionals for the purpose of health care delivery where physical distance is a barrier. 9 The terms ‘telemedicine’ and ‘telehealth’ tend to be used interchangeably. However, the term ‘telemedicine’ tends to restrict the use of digital health technologies to the medical professions while ‘telehealth’ is the use of these technologies by various other health professionals. 9 Telemedicine includes synchronous (real-time video consultations) and asynchronous (store-and-forward data sharing) applications. Studies have demonstrated that telemedicine reduces waiting times, facilitates chronic disease management and optimises healthcare resources.10–12 Despite the benefits, telemedicine adoption remains slow due to medico-legal concerns and resistance from healthcare professionals.13,14
By leveraging ICT, digital virtual consultations can overcome geographical barriers, extending the reach that medical professionals have beyond their physical workplace, enabling telemedicine to offer an alternative way of building capacity. 15 Telemedicine empowers patients to be actively involved in their medical care, ushering in a paradigm shift in patient involvement and person-centred care. 16
Digital health care has been adopted in numerous Economic Co-operation and Development (OECD) countries. 15 For example, Poland started introducing telemedicine in the early 20th century while in 2013, Korea sought to permit digital consultation use between patients and the medical workforce.15,17 Furthermore, investments in telemedicine are also being spurred by the rapid evolution of ICT, fast internet connectivity and adoption of electronic patient records (EPRs). 18
Telemedicine can be stratified according to the complexity of the technology and infrastructure utilised, its temporality in terms of use, and the ease of access for the patient. 19 Depending on the technology and utilisation, telemedicine can either be ‘synchronous’, that is, occur in real time as exemplified by video consultations or ‘asynchronous’, as in the case of electronic consultations where the data are stored and then addressed later.2,20
The literature shows that digital virtual consultations provide benefits beyond facilitating access to care and addressing workforce shortages.20–23 They reduce waiting times through appropriate triaging, reduce congestion in waiting rooms and allow doctors to focus on complex cases, positively impacting their work-life balance.24,25 Digital virtual consultations, as adjuncts to traditional medical practice, facilitate the follow-up of patients who suffer from chronic disease and the hospitalised and are a source of education for both medical professionals and patients through the exchange of evidence-based information.26,27
During the COVID-19 pandemic, digital virtual consultations played a crucial role in triaging and maintaining access to care while limiting workforce exposure and reducing costs related to resource utilisation. 28 Post-pandemic, the barriers to implementation have diminished, and digital consultations are increasingly being recognised as central to healthcare provision, presenting a window of opportunity for widespread adoption.29,30
Digital innovations for health care delivery have been shown to be cost-effective. 31 Cost-analysis studies have shown that, in terms of the technology used, the training required, and the costs incurred in terms of patient transportation and missed workdays, telemedicine is cheaper than traditional methods of consultation.32,33 Additionally, digital virtual consultations reduce the overall number of hospital visits, further lowering costs and improving efficiency.21,22
Telemedicine is feasible, effective, and safe in providing care. 34 The technology has been found to be consistent, appropriate, and effective in achieving patient outcomes in different scenarios ranging from acute care to follow-up of patients with chronic illness.35–37
Research has attempted to explore individuals’ inclination to use IT applications such as electronic patient records, telemedicine platforms and digital consultation systems. 38 From an organisational point of view, it is crucial for administrations to make the appropriate decisions on interventions which will lead to enhanced acceptance of IT applications. 39 Identification of factors that could impact the uptake and utilisation of new IT applications can help in decision making and shape implementation strategies. 39
The literature discussed in this section shows that, while numerous studies have explored telemedicine globally, there is limited empirical research on hospital doctors’ adoption of virtual consultations in small, digitally evolving healthcare systems such as Malta. These contexts present unique challenges related to systemic infrastructure and policy adaptation. Against this background, this study examines doctors’ perceptions regarding the adoption, implementation, and utilisation of digital virtual consultations in a tertiary hospital in Malta. Answers to the following research questions were sought: (i) What are the perceptions of doctors working in a secondary- and tertiary-level hospital in Malta, regarding the adoption, implementation and utilisation of video consultations in their work practice?; and (ii) Which are the best predictors of behavioural intention, perceived usefulness and perceived ease of use of video consultations from among the five predictors image, job relevance, perceived ease of use, result demonstrability and subjective norm?
By aligning the research focus with the identified gaps, this study provides insights into the factors influencing digital virtual consultation adoption, helping policymakers and healthcare administrators implement effective digital health strategies.
Based on existing literature and the study objectives, we hypothesise that:
H1: Doctors perceive digital virtual consultations as a beneficial supplement to in-person consultations.
H2: The willingness of doctors to adopt virtual consultations depends on the availability of adequate infrastructure and technology.
H3: Adoption barriers, including policy and training gaps, impact the feasibility of implementing virtual consultations in Malta.
Theoretical framework
This study draws on the Technology Acceptance Model 3 (TAM3), 40 an evolution of the original TAM 41 and its extension, TAM2. 42 TAM posits that an individual’s intention to use an IT application is shaped by their attitude towards it, which is driven by perceived usefulness (PU) and perceived ease of use (PEOU). 41 These perceptions are further influenced by external variables such as user demographics, organisational context and technological features.42,43
TAM3 builds on this foundation by identifying specific determinants of PU and PEOU, offering a more robust framework for analysing technology adoption. 42 PU reflects the extent to which a user believes the technology enhances task performance, while PEOU relates to the effort required to use it. 44 Venkatesh and Bala’s TAM2 45 expanded these concepts, culminating in the development of TAM3, from which this study’s instrument is adapted.
In this research, TAM3 is applied to assess hospital doctors’ intentions to adopt virtual consultations in Malta. The model guides analysis of:
Determinants of behavioural intention (Figure 1), including PU, PEOU and subjective norm;
Influences on PU (Figure 2), such as job relevance, result demonstrability, subjective norm and image;
Drivers of PEOU (Figure 3), including computer self-efficacy, external control perceptions and computer anxiety.
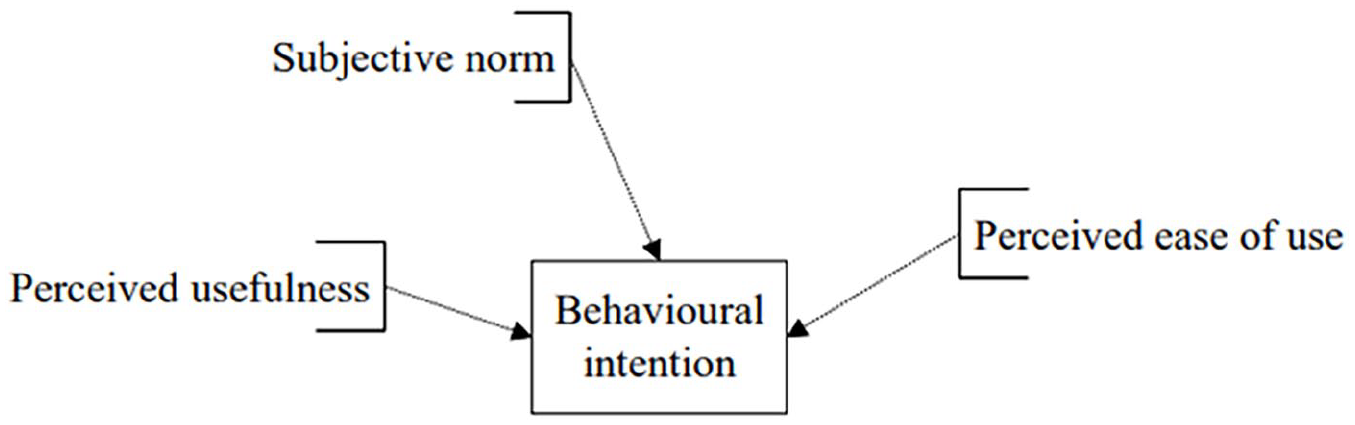
The determinants of behavioural intention.
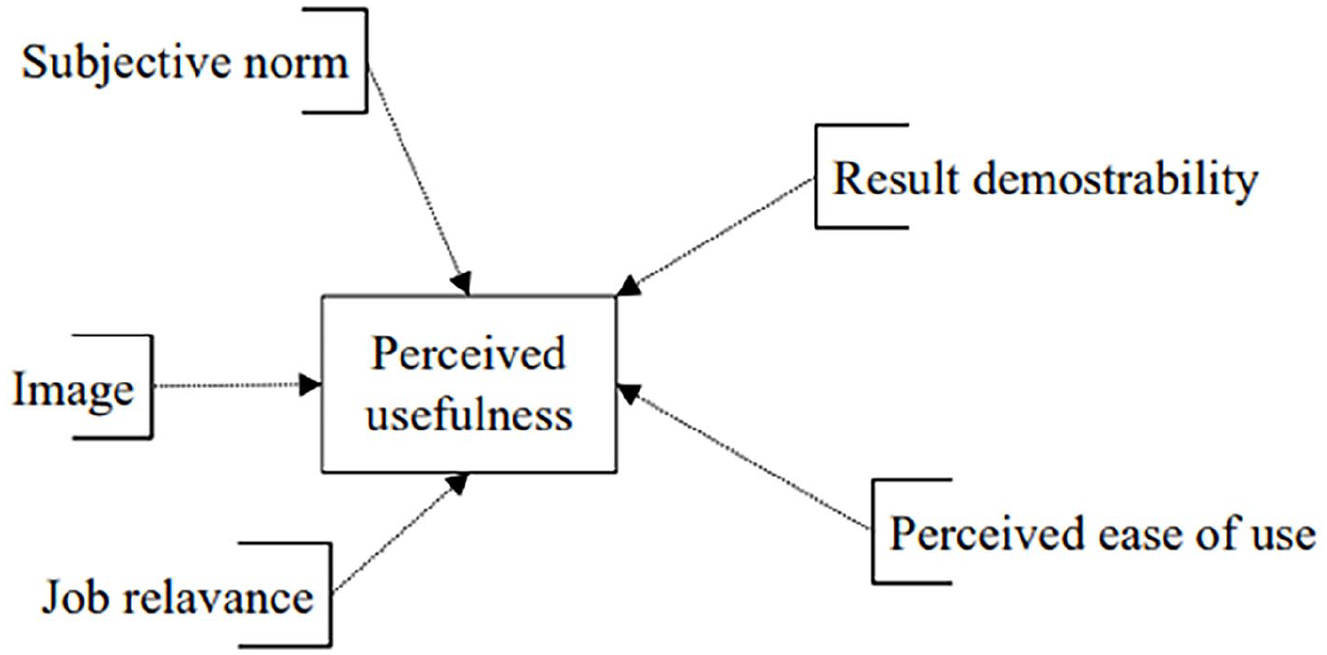
The determinants of perceived usefulness.

The determinants of perceived ease of use.
Constructs like perceived enjoyment, object usability and output quality were excluded, as virtual consultations had not yet been implemented at the study site. Without hands-on experience or performance data, these factors were not measurable. Prior research suggests such variables become more relevant post-adoption, once users interact directly with the technology. 42
For the purpose of this research, the following relationships were studied:
The determinants of behavioural intention (Figure 1)
The determinants of perceived usefulness (Figure 2)
The determinants of perceived ease of use (Figure 3)
The determinants of behavioural intention
Figure 1 illustrates the determinants of behavioural intention, highlighting that PU exerts the strongest influence on a doctor’s decision to adopt virtual consultations. This aligns with findings in the literature, which suggest that perceived benefits in efficiency and effectiveness drive adoption in medical practice.40,41
The determinants of perceived usefulness
Figure 2 outlines the predictors of PU, demonstrating that job relevance is a key factor. In a hospital environment, physicians are more likely to adopt digital virtual consultations if they perceive them as enhancing their workflow and patient interactions. This study’s findings confirm that job relevance significantly predicts PU (p = 0.028), reinforcing the importance of aligning new technologies with healthcare professionals’ practical needs.
The determinants of perceived ease of use
Figure 3 presents the determinants of PEOU, emphasising that perceptions of external control, such as availability of IT support and infrastructure, play a crucial role in shaping ease of use perceptions. The study results indicate that perceptions of external control were the strongest predictor of PEOU (p = 0.001), underscoring the necessity for adequate institutional support in technology adoption efforts.
The constructs of perceived enjoyment, object usability and output quality were not included in the adaptation of the research tool as, at the time of the study, digital virtual consultations were not yet in place at the analysed hospital. The last aspect of the behavioural intention construct was removed as there was not yet a timeline for implementation of digital virtual consultations. The construct of computer playfulness was removed as it was deemed not significant for the purposes of this research. The use construct was used to explore any previous experience that the respondents had using the software or platforms that support digital virtual consultations.
Contextual adaptation to Malta’s healthcare system
The Maltese healthcare system presents unique challenges that influence the adoption of digital virtual consultations, including workforce constraints, high patient loads and infrastructural limitations. Unlike larger healthcare systems with extensive digital integration, Malta is in the early stages of implementing virtual consultations. Therefore, this study applies TAM3 within a setting where digital health adoption is nascent, emphasising the role of organisational readiness and policy frameworks. By focusing on a tertiary hospital in Malta, this research highlights the specific enablers and barriers to digital virtual consultation adoption in a small island nation. Investment in digital infrastructure, training and administrative support is essential for fostering a positive perception of usability and usefulness among hospital doctors. Furthermore, stakeholder engagement, including policymakers and healthcare administrators, will be critical to ensuring a smooth transition to digital consultation services.
The theoretical framework adapted in this study provides a robust foundation for analysing hospital doctors’ attitudes towards digital virtual consultations. By integrating TAM3 with contextual considerations specific to Malta’s healthcare environment, this study offers valuable insights into technology acceptance in resource-constrained medical settings.
Methodology
Study design
This study employed a cross-sectional mixed methods design within the philosophical paradigm of pragmatism. The quantitative survey assessed the hospital doctors’ attitudes towards digital virtual consultations. The survey also included a minor qualitative component with questions that allowed open-end responses which provided deeper insights into the statistical findings. Pragmatism shaped this approach by prioritising practical, real-world problem-solving rather than rigid adherence to either positivist or interpretivist methodologies. This paradigm allowed the study to integrate numerical data with subjective perspectives, ensuring a more comprehensive understanding of factors influencing technology adoption.46,47 The choice was made with the aim to provide practical insights rather than being purely theoretical.
Participant selection
The sample population included doctors at houseman (junior doctors in their first year of supervised clinical practice), basic specialist trainee, higher specialist trainee, registrar and consultant level, in medical specialities including cardiology and neurophysiology, and in surgical specialities including ophthalmology, otorhinolaryngology and orthopaedics, as well as in obstetrics and gynaecology. Doctors not included in this research were specialities that do not perform out-patient sessions. The sample size amounted to 886 individuals.
A combination of convenience and purposive sampling was used. Convenience sampling was chosen due to the accessibility of hospital doctors within the targeted tertiary hospital in Malta, ensuring an adequate sample size within the study timeframe. This method was supplemented with purposive sampling to include doctors across various specialisations, ensuring representation of different medical disciplines. However, convenience sampling may introduce selection bias, as participants who are more technologically inclined or interested in digital consultations may have been more likely to respond. To mitigate this, email invitations were sent to the entire eligible doctor population to maximise inclusivity and representativeness. Eligible participants were hospital doctors currently employed in the public health system with a minimum of 6 months’ clinical experience. Of the 886 invited, 133 responded (15% response rate).
In sum, two sampling methods were adopted in selection of the sample population: convenience and purposive sampling. 48 Both approaches were used to identify potential respondents and send the email invitation to the sample population. 49 This method was chosen because of the digital nature of the study. 50
Data collection
Quantitative data collection was conducted through administration of an online cross-sectional questionnaire. Permission for utilisation of TAM 3 constructs was obtained from the authors and publisher, who were contacted via email and permission was obtained via reply to the same email.
The research tool was organised into 13 constructs that explored demographics, current use of video consultations and perceived usefulness, perceived ease of use, computer self-efficacy, perceptions of external control, computer anxiety, subjective norm, voluntariness of use, image, job relevance, result demonstrability, and behavioural intention. The questionnaire included a comment box at the end, inviting the participants to share opinions and comments. 21 free-text comments were received from respondents. The constructs apart from demographics and current use were addressed through statements which the respondents rated on a 5-point Likert scale ranging from 1 that is ‘strongly agree’ to 5 that is ‘strongly disagree’.
The questionnaire was constructed on SurveyMonkey.com, an online platform for the creation and distribution of web-based questionnaires, chosen because its interface is comprehensible and customisable and the data collected can be exported to formats compatible with data analysis software. 51 The final version of the questionnaire and the method of distribution was reviewed and approved by the Data Protection Office at the analysed hospital. A research intermediary was appointed, who had access to the sampling frame, filtered potential participants by specialty and grade and emailed the web-based questionnaire to participants. The data collection method was chosen to ensure anonymity.
The questionnaire was accompanied by an approved invitation email and information letter that explained the objectives of the study, the method of data collection, the storage of data, the availability of support if required and consent giving. Respondents were assured that the survey would take less than 15 min to complete. The questionnaire was sent to 886 individuals between September and November 2021. Reminders on a fortnightly basis were sent out until no new responses were registered. These were sent via email every 2 weeks until responses plateaued. Regarding questionnaire validation and reliability, the questionnaire was adapted from TAM3, a validated model, ensuring construct validity. Before data collection, it underwent internal review by the research team to confirm relevance and clarity. Additionally, a pilot test was conducted with a small group of doctors (n = 15) to assess comprehension and refine ambiguous questions. Reliability was examined using Cronbach’s alpha, confirming internal consistency across constructs such as perceived usefulness, perceived ease of use and behavioural intention. Constructs with alpha values above 0.7 were considered reliable.
The survey included TAM3-based items, with core constructs (e.g. PU, PEOU, BI) adapted from validated instruments. Some items were modified for context relevance, and a few were newly developed. Cronbach’s alpha values were PU = 0.84, PEOU = 0.81, BI = 0.86.
Data analysis
The data collected from the questionnaires was transferred from SurveyMonkey.com to Statistical Package for the Social Sciences (SPSS), version 28 (IBM Corporation, Armonk, NY, USA), which was then used to analyse the data. Statistical tests included Fisher’s exact test, Friedman’s test, one-way analysis of variance (ANOVA) and multiple linear regression.
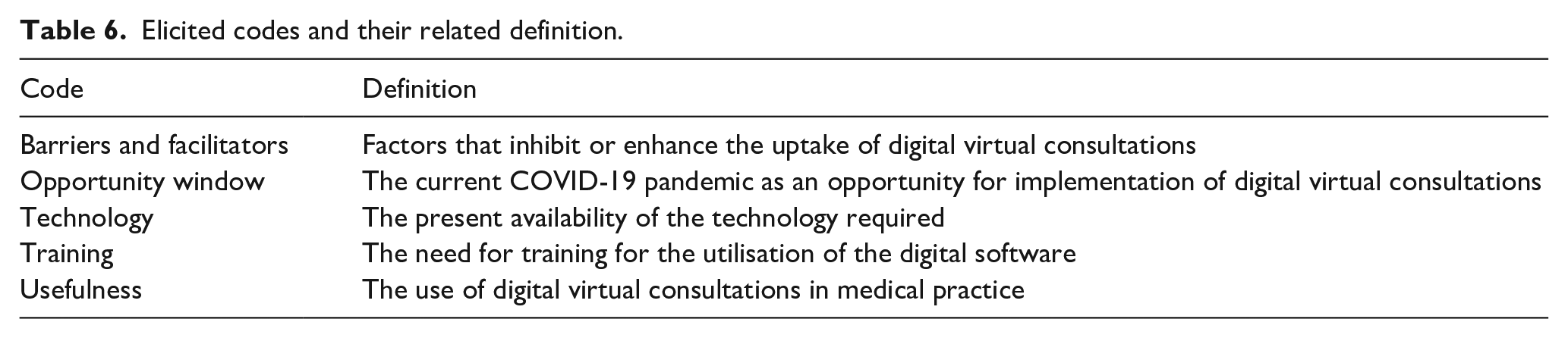
Fisher’s Exact Test was chosen for categorical variable analysis due to the small sample size in certain subgroups, ensuring accuracy in evaluating associations between demographic factors and virtual consultation experience. ANOVA (Analysis of Variance) was applied to compare mean differences across multiple groups (e.g. specialisation levels, gender, and age groups) regarding perceived usefulness and ease of use. In addition, multiple regression analysis was used to determine the predictive power of TAM3 constructs on behavioural intention, ensuring a robust evaluation of the model’s applicability. With a 15% response rate, non-response bias was a potential limitation. To assess and mitigate its impact, the below actions were conducted: First, a comparison of early and late respondents was conducted, as late responders often resemble non-respondents; and no significant differences were found in key variables. Second, the demographic representativeness was evaluated against hospital workforce statistics to ensure the sample aligned with the broader population of hospital doctors. And third, weighting adjustments were considered but deemed unnecessary as subgroup distributions closely matched workforce demographics. Nevertheless, despite these measures, generalisability remains a limitation, thus the need for caution when extrapolating findings beyond the studied hospital context. Regarding the analysis of the minor qualitative component of this study, thematic analysis was employed to analyse the free-text responses of the survey. The following themes were extracted: barriers and facilitators; opportunity window; technology; training; and usefulness.
Ethical considerations
The ethical principles of freedom from harm, the right to autonomy, anonymity, confidentiality and privacy were followed throughout the study.
Ethical approval was obtained from the University Research Ethics Committee (UREC) at the University of Malta (Ref. No. V_150620205465) prior to piloting and data collection. The review process took approximately 4 weeks. Permission was also obtained from the Data Protection Office, the Chief Executive Officer and the Chief Clinical Chairperson at the included hospital. The necessary permissions were also obtained from the relevant heads of departments of the hospital.
Data collection was anonymous and the digital platform SurveyMonkey.com was set up so as not to keep the internet service provider (ISP) addresses of the participants. Data were collected and handled only by the researchers and stored on a secure, password-protected device.
Results
A total of 886 email invitations were sent to potential participants between September and November 2021. Reminders were sent every second week until no further responses were elicited. A total of 133 responses were obtained, giving a response rate of 15%. Altogether 67% of the respondents fully completed the questionnaire, ensuring data completeness for analysis. The 15% refers to the overall response rate, while 67% represents the proportion of respondents who fully completed the questionnaire.
Seventy-one respondents were female and 62 were male, with the majority of those who responded being junior doctors at foundation level (postgraduate trainees in early stages of their medical career). Respondents’ demographics are presented in Table 1. Table 2 gives the respondents’ experience with virtual consultations.
Demographic data of respondents.

Foundation Doctor: A recently graduated medical doctor undergoing the initial two-year Foundation Programme, aimed at building core clinical competencies across multiple specialities. Basic Specialist Trainee (BST): A doctor who has completed foundation training and is undertaking early-stage specialty training, typically leading towards specialisation. Higher Specialist Trainee (HST): A doctor in the advanced stages of specialty training, working towards consultant-level responsibilities and accreditation. Resident Specialist: A fully qualified specialist who has completed all necessary training and exams, and works under a consultant, often within a fixed hospital position. Consultant: The most senior medical specialist responsible for leading clinical teams, making high-level decisions and overseeing training of junior doctors.
Current experience and utilisation of digital virtual consultations (VCs).

Fisher’s exact test showed an association between gender (p = 0.046), age (p = 0.035) and level of specialisation (p = 0.05) and experience with digital virtual consultations.
The Friedman test was used to compare the mean rating scores for the items in each construct. The mean scores indicate respondents’ agreement that digital virtual consultations can be used in conjunction with face-to-face consultations and are a means of communication between professionals and a way to enhance quality of care. Respondents perceived video consultations as easy to use and as relevant to their medical practice and stated that they would be able to perform a digital consultation in an adequate, supportive environment.
One-way ANOVA was used to compare mean construct scores between several groups of respondents clustered by gender, age and level of specialisation. With a p-value of 0.028, female participants scored significantly higher on job relevance and there was a statistically significant difference (p = 0.024) between the age groups regarding perceived usefulness and subjective norm. Similarly, there was a statistically significant difference (p = 0.010) in the mean scores between levels of specialisation for computer self-efficacy.
Multiple regression analysis was applied to evaluate the relationships between perceived usefulness, perceived ease of use and behavioural intention, and their determinants.
The model relating perceived usefulness to the five predictors subjective norm, image, job relevance, result demonstrability and perceived ease of use explained 54.8% of the total variability of perceived usefulness. Job relevance was the strongest predictor of perceived usefulness because it has the lowest p-value and the highest t-value (see Table 3).
Model relating perceived usefulness to five predictors.
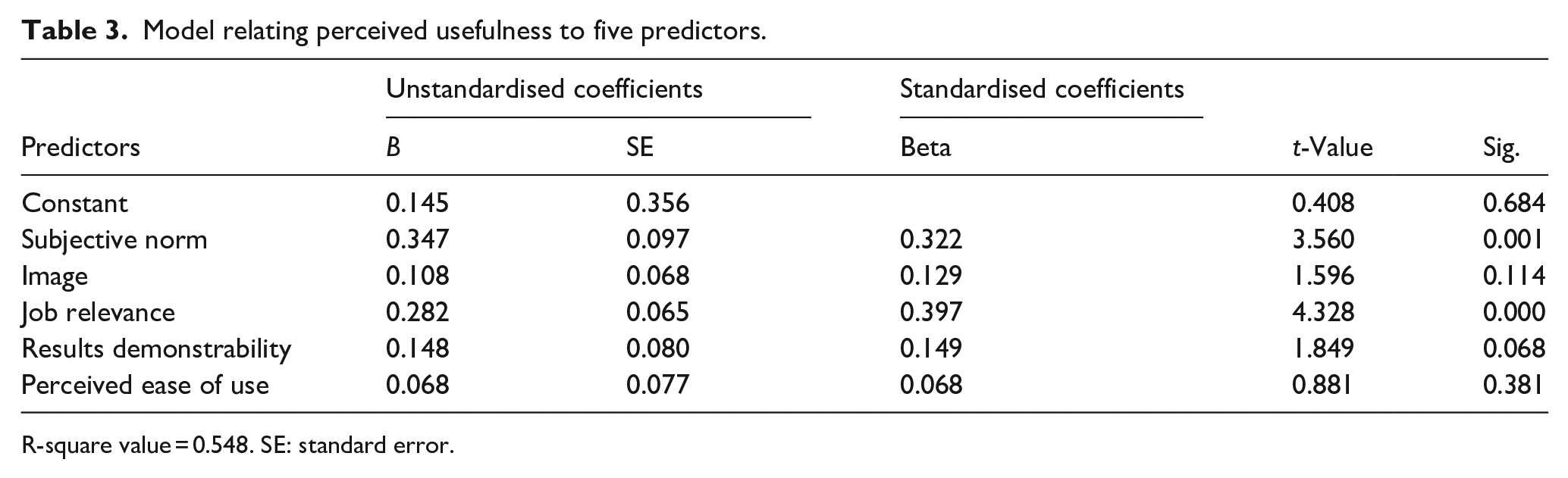
R-square value = 0.548. SE: standard error.
The model relating perceived ease of use to the three predictors computer self-efficacy, perceptions of external control and computer anxiety explained 43.2% of the total variability of perceived ease of use. Perceptions of external control was the best predictor of perceived ease of use as it had the lowest p-value (Table 4).
Model relating perceived ease of use to three predictors.

R-square value = 0.432. SE: standard error.
The model relating behavioural intention to the three predictors perceived usefulness, perceived ease of use and subjective norm explained 51.1% of the total variability of behavioural intention. Perceived usefulness was the best predictor of behavioural intention because it has the lowest p-value (Table 5).
Model relating behavioural intention to three predictors.

R-square value = 0.511. SE: standard error.
The last question of the survey invited the participants to share any thoughts and ideas on the topic being researched, namely the adoption, implementation and utilisation of digital virtual consultations in their practice. A total of 21 participants shared their views through this question. Two researchers read through the comments and assigned codes to the text. The following codes were elicited, barriers and facilitators, opportunity window, technology, training and usefulness. Table 6, Figure 4 and Table 7 illustrate the codes and their definition, the number of references in the text and quote examples.
Elicited codes and their related definition.

Codes elicited and number of references in text.
Examples of quotations for the codes elicited.
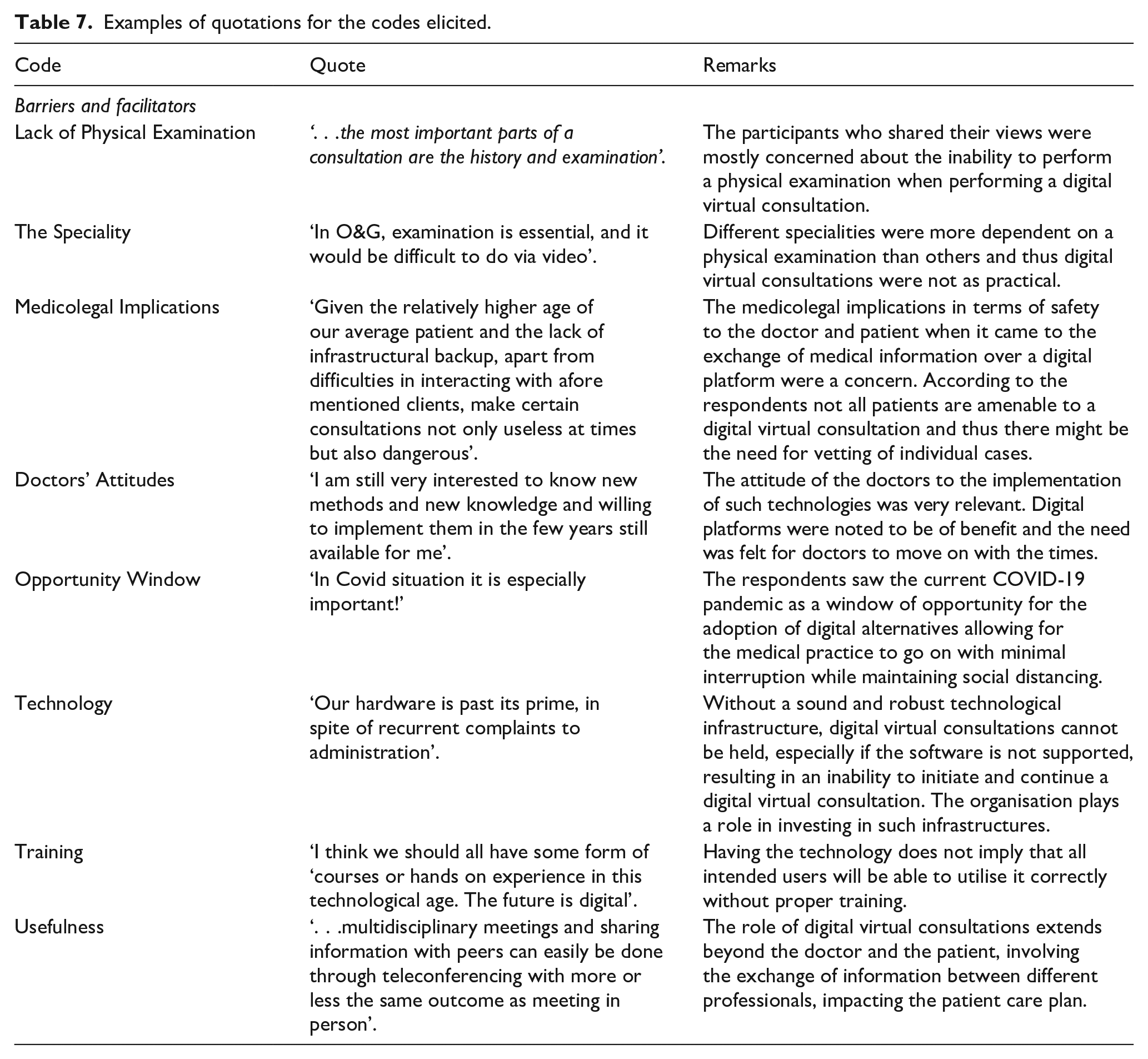
The results obtained from the analysis of the quantitative data informed the qualitative data collection as the researcher sought to develop further on the perceptions of doctors as regards the ease of use of digital virtual consultations, their usefulness in the current medical practice and their role within the context of a small island state, the impact of video consultations on the relationships between doctors and patients as well as between the professionals themselves and ultimately provide further insight into those factors which enhance or inhibit the uptake of these technologies.
Discussion
Summary of results
This study explored hospital doctors’ attitudes towards the adoption and utilisation of digital virtual consultations in a Maltese tertiary hospital. The findings align with previous research highlighting both the benefits and challenges of digital health adoption. Doctors acknowledged the convenience and efficiency of digital virtual consultations, consistent with studies that report improved accessibility, reduced waiting times and better resource utilisation.20,21 However, concerns regarding technological infrastructure, usability, and medico-legal implications mirror those found in other studies where digital health adoption has been met with similar scepticism 30
A significant finding of this study is that job relevance and perceived external control were among the strongest predictors of perceived usefulness and ease of use, supporting the Technology Acceptance Model (TAM3) framework. 41 This suggests that if healthcare organisations provide sufficient technical and administrative support, doctors may be more inclined to adopt digital virtual consultations. These results align with research emphasising the role of institutional readiness in digital health implementation. 31
Digital virtual consultations have a role in supporting the balance between health care resource utilisation, access and provision of care.52,53 Some of the respondents in this study thought that video consultations would be useful to them in their jobs. The mean score of 2.6 indicated agreement on the relevance of digital virtual consultations in the local medical practice. Female respondents tended to perceive video consultations as more relevant to their job than their male counterparts (p = 0.28). However, the respondents did not feel that video consultations were appropriate as first point of contact with patients, and there was strong disagreement regarding the question whether digital virtual consultations are superior to traditional face-to-face consultations (mean score 3.7). With mean scores of less than 3, respondents did perceive digital virtual consultations as adjuncts to face-to-face consultations with a particular role in the follow-up of patients. The implementation of the new technology will invariably lead to changes in work practices. Doctors will need to adapt to change while understanding what will be required of them to initiate and complete a digital virtual consultation. 54
There was agreement on the construct of perceived ease of use. With a mean score of 2.32, respondents perceived digital virtual consultation software as easy to use and with mean scores of less than 3 there was agreement that operating the software would be easy and understandable and would not require much mental effort. The respondents did not feel that working with technological devices such as computers made them feel anxious or uneasy. The notion of digital virtual consultations might still be new in the health care system; however, these technologies were already being used informally to initiate communications and some of the respondents stated that they already used digital virtual consultations in their practice. The respondents expressed neutrality (mean score of 3.04) regarding the availability of resources required to initiate digital virtual consultations; however, there was agreement as to the ease of use of the technology if the resources and knowledge are present.
An improvement in workload, in terms of increased productivity and effectiveness, as discussed by Ref.,
55
was not perceived by the respondents in this study. With mean scores of around 3, the respondents were neutral to the perception that video consultations would improve doctors’ performance, productivity and effectiveness, as well perceptions regarding their impact on doctors’ working hours and work
There is the need for health care organisations to guarantee the availability and accessibility of the infrastructure coupled with proper project management and coordination to enhance sustainability of initiatives such as the one discussed here.56,57 With a mean score of 2.46, respondents perceived it to be easy to operate the software if the resources, opportunities and knowledge are available. They perceived the organisation they worked for as supportive in the utilisation of these digital alternatives, allowing for voluntary use of the technology.
The mean scores obtained on behavioural intention indicate that if the respondents had access to the software, they would, based on their predictions, initiate digital virtual consultations. The respondents thought that the utilisation of such technologies would be on a voluntary basis, and they would not find it difficult to communicate the advantages and disadvantages of such alternatives to colleagues.
Lack of acceptance by users was identified by Refs.54,58 as a major barrier to adoption and implementation of innovative technologies. As postulated by Davis, intention of use is influenced by perceived usefulness, perceived ease of use, and the subjective norm. 43 These constructs are in turn influenced by their determinants.
Multiple regression analysis performed for the model evaluating the determinants of perceived usefulness found an association between perceived usefulness and its five predictors. The analysis indicates that the way in which the respondents perceived digital virtual consultations as relevant to their practice, followed by the perception that management would be supportive in the utilisation of the technologies, had more impact on the perceived usefulness of these consultations than the ability to communicate the pros and cons of utilisation, the influence of utilisation on the individual’s status within the organisation and the ease of use of the technology.
Regression analysis showed an association between perceived ease of use and three predictors. The extent to which the respondents perceived the necessary resources as being present was the strongest predictor, followed by the extent to which the respondents felt comfortable working with technical infrastructure and the extent to which they believed they were able to initiate digital virtual consultations with or without assistance.
Behavioural intention was likewise associated with its three predictors. Of these, perceived usefulness was the strongest predictor, followed by perceived ease of use and, finally, subjective norm.
The findings of this study therefore indicate that targeting these predictors will strengthen the intention to use the technology in the local context. Identifying the factors or determinants that impact intent to use is crucial for the development of implementation strategies. 59
Factors that facilitate the uptake of modern technologies need to be identified. Also, there should be an understanding of those factors which are perceived as critical by the workforce, and which should therefore be addressed in the implementation process. There is a need for proper evaluation of the technologies to be adopted, coupled with a feasibility analysis to understand the need and the demand to ensure project sustainability. 60
In conclusion, our findings confirm that doctors perceive digital virtual consultations as a beneficial supplement to traditional consultations (H1). However, the feasibility of adoption depends on infrastructure availability (H2), while policy and training barriers must also be addressed (H3).
Barriers and facilitators to adoption
The study identified several barriers and facilitators that influence the adoption of digital virtual consultations.
Infrastructure and Technological Support: Doctors expressed concerns about outdated hardware, unreliable connectivity and lack of seamless integration with existing electronic health records (EHRs). Similar barriers have been reported in studies where poor infrastructure significantly hindered telehealth adoption. 17 Adequate investment in digital infrastructure is necessary for successful implementation.
Organisational Support: The study revealed that doctors perceive management support as a key facilitator. Organisational policies that provide clear guidelines and standard operating procedures (SOPs) for virtual consultations could increase adoption rates. Prior studies emphasise that top-down leadership support and incentives can drive successful digital transformation in healthcare. 25
Training and Digital Literacy: While doctors found video consultations easy to use, concerns about a lack of formal training were raised. Research suggests that structured training programmes and workshops enhance user confidence in adopting new digital tools. 60
Patient Readiness: The study highlighted concerns regarding older patients’ ability to engage with digital platforms. Similar findings in telemedicine research emphasise the need for patient-centred interventions, such as user-friendly applications and caregiver assistance. 56
By linking these findings with the TAM3 framework, it is evident that perceived external control (institutional support) and computer self-efficacy (training) play a crucial role in shaping doctors’ willingness to adopt virtual consultations. Addressing these barriers systematically could improve adoption rates and streamline integration.
Practical implications
Although the concept of digital virtual consultations is relatively new to doctors working in the main hospital on the island of Malta, it was acknowledged that they have a role in the current medical practice. There is a need to understand the role of digital virtual consultations in the follow-up of patients once initial rapport has been established between the doctor and the patient during a traditional consultation, which is still seen as the gold standard for the patient
Improved access and enhanced communication between specialists and patients result in enhanced quality of care. Digital virtual consultations are channels of communication fostering the sharing of medical knowledge and information, leading to a higher level of health care provision in and outside the practice and therefore to better patient management.
Digital virtual consultations are of particular importance in the small island state of Malta. The literature highlights the role of digital consultations in overcoming distance barriers; however, it does not address the challenges faced by small countries that have limited resources and are isolated by geography. The small size of Malta limits exposure and may lead to loss of skill over time, while the island’s isolation leads to seeking specialised patient care overseas. Virtual consultations can help reduce these barriers by lessening the need for patients to go abroad while supporting the delivery of specialised care. Though video consultations can transcend geographic boundaries, jurisdictional policies may still restrict patient registration to specific catchment areas. Future models may need to account for cross-border virtual care.
In analogy to findings in the literature, this study has identified the need for investment in appropriate technological infrastructure that is simple to use, easily accessible and robust so as to support virtual consultations. The new technologies should fit with the way local doctors practise. They should also be easily integrated into existing digital infrastructure, with the appropriate level of technical support made available.
Apart from making the initial investment, the health care organisation was seen as having an essential role in the sustainability of the initiative. There is a need for investment in technical support and training, which would heighten the intention of use of the new technologies and maintain their utilisation as the workforce becomes familiar with the new practices.
The literature has shown that the uptake of digital virtual consultations is influenced by the understanding that users have of its benefits. As postulated in the TAM, 43 individuals’ intention to use technology is influenced by the usefulness and relevance of the technology, as well as by how easy and effortless the technology is to use. This research study has shown that the participants’ perception of the technology’s usefulness and ease of use did have an association with their intention of use, and that, with the appropriate resources and access to the technology, the respondents would make use of these alternatives to traditional methods.
The integration of digital virtual consultations into healthcare systems requires a multifaceted approach that combines investment, policy development and training. Enhancing technological infrastructure should be a priority, as reliable internet connectivity and secure telehealth platforms are fundamental to the seamless operation of digital virtual consultations. This includes ensuring compatibility with electronic health records (EHRs) to facilitate continuity of care. Beyond infrastructure, developing comprehensive policies and guidelines is crucial to establishing medico-legal frameworks that clarify responsibilities, patient confidentiality protocols, and reimbursement structures. Without clear policies, healthcare professionals may be hesitant to adopt virtual consultations due to uncertainty around liability and procedural standards.
Training programmes tailored for healthcare professionals can improve digital literacy and reduce apprehension towards digital virtual consultations. Structured training sessions, including simulations and peer learning, could foster confidence in using telehealth technologies. Moreover, change management strategies should emphasise stakeholder engagement, as early involvement of doctors in decision-making processes can enhance acceptance and trust in new systems. Finally, healthcare organisations should expand pilot programmes before rolling out virtual consultations at large scale. Implementing these models in specific hospital departments can help identify operational challenges and refine best practices before broader adoption. By ensuring a phased approach, healthcare institutions can mitigate risks and increase the likelihood of long-term success.
Significance for public health
As population demographics change, individuals become more knowledgeable, increasingly demanding, and progressively dependent on technology. As individuals seek innovative approaches to treatment, health care systems seek innovative ways of providing care. In this respect, digital virtual consultations have a significant impact on public health, offering numerous advantages such as accessibility and continuity of care, equity, more efficient resource utilisation and patient management, improved quality of care. Digital virtual consultations may enhance care quality through timely access, continuity of care and reduced travel-related burden for patients. Furthermore, in line with the Sustainable Development Goals (SDGs) of the United Nations (UN), digital health has been widely recognised as a means of improving the sustainability of the healthcare sector. 61 Specifically, the use of ICT and digital technology in healthcare organisations can help achieve universal health coverage (SDG 3).
Digital virtual consultations align with Sustainable Development Goal 3 (SDG 3) by promoting universal health coverage and improving access to care, particularly in geographically constrained settings like Malta. Telehealth initiatives in small island nations, such as Iceland and Singapore, have successfully demonstrated how digital health can address workforce shortages and improve patient management. 62 Incorporating lessons from these contexts can inform Malta’s strategy for digital virtual consultations. Additionally, digital virtual consultations reduce carbon emissions associated with patient travel, contributing to SDG 13 (Climate Action) by minimising the environmental impact of healthcare delivery.
Strengths and limitations
This study has both strengths and limitations. The main strength of this study is that it is the first of its kind in the Maltese islands to provide important insights regarding hospital doctors’ attitudes to the adoption, implementation and utilisation of digital virtual consultations. In addition, the study used a cross-sectional mixed-method design. However, the study is not without limitations. First, the sampling process may have introduced biases such as lack of representativeness of all doctors working in the hospital as well as potential overestimation of the general acceptance of virtual consultations by doctors who were already inclined to adopt technology. However, the digital nature of the study allowed for easier access to the population of interest in the context of the COVID pandemic even if findings need to be interpreted with caution. Second, the study had a low response rate (15%) which might have influenced the observed findings as doctors with strong opinions (positive or negative) may have been more likely to participate in the study. But the comparison of early and late respondents mitigated the effects of the response rate to an extent, and again warranting caution when extrapolating the study results. Third, given that the study took place in a single tertiary hospital, findings may not fully represent the perspectives of doctors in other healthcare settings of Malta or other countries with different digital health infrastructures. Overall although the limitations above, the study results still provide greater insights that are needed by policy makers in the areas of public health and health care in the context of Malta. Nevertheless, there is a need of future studies using randomly selected samples.
Conclusions
This study aimed to explore the attitudes of doctors towards the adoption, implementation and utilisation of digital virtual consultations in a tertiary hospital in Malta. The findings indicate that while doctors view digital virtual consultations as valuable supplements to in-person visits—helping to overcome barriers related to distance and time—their successful adoption depends on the availability of appropriate infrastructure and technology. Infrastructure and technological readiness emerged as the most significant factors influencing adoption, with 72% of participants indicating these as essential for successful implementation of virtual consultations.
To facilitate implementation, healthcare institutions must invest in robust digital infrastructure, provide comprehensive training for medical staff, and establish clear policies and guidelines. Additionally, feasibility and cost-effectiveness studies should be conducted to evaluate the long-term sustainability of digital virtual consultations, alongside a stakeholder analysis to ensure all key actors are engaged in the transition process.
Hospital doctors in Malta acknowledge the potential of digital virtual consultations to enhance healthcare delivery, but adoption barriers—including technological, infrastructural and policy-related challenges—must be addressed through targeted interventions. Future research should build on these findings by incorporating a larger and more diverse sample while employing a mixed-methods approach to gain deeper insights into the practical aspects of implementation.
The next phase of this research will focus on expanding the respondent pool and integrating both qualitative and quantitative methodologies to provide a more comprehensive understanding of how digital virtual consultations can be effectively integrated into Malta’s healthcare system. Moreover, while this study focused on hospital doctors, future research could explore parallel perceptions among other clinical roles involved in virtual care delivery.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251361425 – Supplemental material for Hospital doctors’ attitudes to the adoption, implementation and utilisation of digital virtual consultations
Supplemental material, sj-docx-1-phj-10.1177_22799036251361425 for Hospital doctors’ attitudes to the adoption, implementation and utilisation of digital virtual consultations by Dorothy Zammit, Gianpaolo Tomaselli, Lalit Garg, Sandra C. Buttigieg and Gloria Macassa in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251361425 – Supplemental material for Hospital doctors’ attitudes to the adoption, implementation and utilisation of digital virtual consultations
Supplemental material, sj-docx-2-phj-10.1177_22799036251361425 for Hospital doctors’ attitudes to the adoption, implementation and utilisation of digital virtual consultations by Dorothy Zammit, Gianpaolo Tomaselli, Lalit Garg, Sandra C. Buttigieg and Gloria Macassa in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to acknowledge the support received from the Department of Social Work, Criminology and Public Health Sciences at the University of Gävle, Gävle, Sweden.
Author contributions
Conceptualisation, D.Z.; methodology, D.Z.; investigation, D.Z.; research supervision, G.T. and S.C.B.; writing—original draft preparation, D.Z. and G.T.; writing—review and editing, D.Z., G.T., S.C.B., L.G. and G.M. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.