
Abstract
Background:
The Breastfeeding Enabling Environment Conceptual Framework underscores the pivotal role of structural, individual, and setting-level factors, including the mother’s occupation in the practice of breastfeeding. This study aimed to investigate the pattern and practice of breastfeeding among mothers of different occupations in Ekiti State, a southwestern region of Nigeria.
Design:
A cross-sectional descriptive survey was conducted involving 191 working mothers selected from different occupational groups in Ekiti State, Nigeria.
Methods:
A pre-tested adapted questionnaire was used to collect data. Descriptive statistics and Chi-square analysis were used for data analysis at a significance level of p < 0.05.
Results:
The mean age of the respondents was 32.4 ± 2.1 years, with approximately 70.2% having tertiary education. Among the respondents, 66% were in professional (white-collar) roles, while 34.0% were artisans (non-professional roles). Sixty-one percent of the respondents reported breastfeeding their babies within 1 h after birth, and a majority (71.2%) practiced exclusive breastfeeding (EBF) for the first 6 months. Approximately 61% of the respondents reported having workplace support for breastfeeding, although only 52.4% had breastfeeding breaks. Mothers in white-collar jobs demonstrated higher rates of EBF (61.0%) and good infant feeding practices (74.8%) compared to self-employed mothers. Bivariate analysis revealed a statistically significant association between the practice of EBF and maternal occupation (p < 0.05).
Conclusions:
Mothers in white-collar and professional occupations exhibited more appropriate breastfeeding practices compared to self-employed mothers. It is crucial for healthcare professionals, including nurses, midwives, and other stakeholders, to prioritize support systems and interventions that facilitate breastfeeding among self-employed mothers.
Introduction
The World Health Organization (WHO) recommends exclusive breastfeeding for infants up to 6 months of life. Breastmilk is safe, and clean and contains antibodies that help protect against many common childhood illnesses. 1 In a bid to raise awareness of the health benefits of breastfeeding and highlight its importance for maternal and child health. The Nigerian government launched the National Guidelines on the Baby Friendly Hospital Initiative (BFHI) in 1992, the National Breastfeeding Policy in 1998, the National Policy on Food and Nutrition in 2001, and the National Policy on Infant and Young Child Feeding (IYCF) in Nigeria in 2005 in an effort to meet the targets of the 1990 Innocenti Declaration. These policies were designed to offer guidance to national and local levels of government, as well as to health practitioners and other stakeholders, on a variety of issues related to the promotion of breastfeeding, and supplemental feeding efforts. 2 Additionally, the Federal Ministry of Health places a strong focus on starting breastfeeding as soon as possible—within an hour of delivery, exclusively (EBF) during the first semester of life, continuing for at least 2 years, and starting appropriate supplemental foods at 6 months of age. Unfortunately, these initiatives haven’t resulted in a significant advancement in the country’s adoption of the exclusive breastfeeding practice because the majority of policy documents were only accessible at the federal level, and nutrition-related policies, reports, and resources were infrequently available at the state and local levels, even within the State Ministry of Health (SMOH), 3 Furthermore, breastfeeding practices in Nigeria show low rates of exclusive breastfeeding, with only 29% of infants under 6 months being exclusively breastfed, according to the National Demographic and Health Survey (NDHS) 2018 study. 4
In our study we decided to focus on exclusive breastfeeding up to 6 months of life because in Nigeria, the rates of early initiation of breastfeeding have improved. According to the latest data available, 42% of infants were breastfed within 1 h after birth and 82% were breastfed within 1 day after delivery, an improvement of 9% and 17% respectively. 1 However, the percent of exclusive breastfed infants in the first 6 months has not improved. This might contribute to high rates of infant mortality and malnutrition observed in the country.5,6 Even though exclusive breastfeeding is associated with a number of advantages that should be enough to encourage mothers to choose this practice, many mothers chose not to breastfeed their children for a variety of socio-cultural reasons. 4 noted that some nursing mothers in Nigeria were discouraged from breastfeeding because they believed that if they breastfed their babies exclusively, their breasts would sag and make them less beautiful to their husbands. The attitudes and behaviors of society provide a substantial additional obstacle to exclusive breastfeeding. According to several writers, the custom of giving newborns water to relieve their thirst and evaluating the bitterness of breast milk before giving it to the infant are detrimental elements that hinder mothers’ practice of exclusively nursing in sub-Saharan Africa.8,9
The Breastfeeding Enabling Environment Conceptual Framework5,6 highlights the importance of structural, individual, and environmental factors. A mother’s occupation, for instance, plays a pivotal role in her breastfeeding practices, 7 which can affect their ability to continue breastfeeding. Studies from different countries, including the United States and Pakistan, have shown that returning to work is a common reason for early discontinuation of breastfeeding.8 –10 In Nigeria, returning to work has been identified as a major barrier to exclusive breastfeeding among female resident doctors 11 and in a mixed-methods study conducted in three locations in Nigeria. 12
In Nigeria, women’s participation in the labor market is predominantly informal, and according to the Nigeria Labor Force Statistics Report, in 2023, approximately 79% of women participated in the labor force. Of those, approximately 95% of women employed work in the informal sector, which includes self-employment and unregistered enterprises. This is largely due to institutional and cultural barriers that limit access to formal employment, despite a significant interest in formal work among women. The sectors where women are most active include subsistence agriculture, which accounts for 8% of the working-age population. Additionally, women are increasingly involved in sectors like beauty and lifestyle, tourism, hospitality, entertainment, and performing arts, where they leverage digital platforms to enhance visibility and business opportunities. On the other hand, the proportion of women who are housewives or not participating in the labor force is not precisely quantified in recent reports, but the high engagement in the informal sector suggests a significant number of women are balancing domestic roles with informal work, which might affect their ability to breastfeed.
Recognizing the challenges faced by working women who want to breastfeed, World Breastfeeding Week 2015 focused on the theme “Breastfeeding and work: let’s make it work.” 13 This emphasized the need to support women in the workplace to successfully combine work and breastfeeding. Exclusive breastfeeding, providing only breast milk to the baby for the first 6 months, is recommended for optimal nutrition. As socio-cultural and economic conditions change, and women increasingly participate in income-generating activities, and the educational and professional status of mothers becomes a significant factor in determining the time available to take care of children. 14 Despite all the advantages of exclusive breastfeeding, there is a lack of information on how workplace-related factors and different occupational settings impact it among Nigerian mothers.
Objectives
The objectives of this study were as follows:
To investigate the pattern and practice of breastfeeding among mothers of different occupational groups in Ekiti State.
To compare the breastfeeding patterns and practices between mothers in white-collar jobs (nurses, bankers and lecturers) and those who are self-employed (artisans like hairdressers and tailors).
Methodology
A descriptive cross-sectional survey was conducted to assess the pattern and practice of breastfeeding among mothers of different occupational groups in three locations within Ekiti State, which is in the southwestern region of Nigeria. It shares borders with Ondo State to the east and south, Kwara and Kogi States to the south, and Osun State to the east. The capital of Ekiti State is Ado-Ekiti. The state is divided into 16 Local Government Areas, 15 and the estimated population for 2016, as published by the National Bureau of Statistics, was 3,270,798 people.16,17
The survey was conducted in three main locations within Ekiti State: Afe Babalola University Ado-Ekiti (ABUAD), Ekiti State University Teaching Hospital (EKSUTH) in Ado-Ekiti, and Ado-Ekiti Metropolis (ADM). These study locations were chosen as targets because they represent a larger percentage when compared to other health facilities. The study population consisted of mothers from different occupational backgrounds, including nurses, bankers, lecturers, hairdressers, and tailors, selected from these three locations. The sample size for the study was determined using the formula for comparative studies, 18 resulting in a sample size of 222.
A non-probability sampling technique (purposive) was employed and only those who met the inclusion criteria were recruited for the study. A total of 222 study participants were sampled, however, only 191 surveys were returned and those were included in the study.
Inclusion criteria
Women who were breastfeeding mothers
Mothers who were either nurses, bankers, hairdressers, or tailors
Breastfeeding mothers who agreed to participate willingly in the study.
Exclusion criteria
Non-breastfeeding mothers
Mothers who were not Nurses, bankers, hairdressers, or tailors
Breastfeeding mothers who were not willing to participate in the study
Instrument for data collection
A pre-tested, self-administered, semi-structured questionnaire was used to collect data from women of different occupational groups. The authors adapted the questionnaires from previous validated studies2,3,14 with modifications made to suit the specific needs of this research. Permission were obtained from the respective copyright holders. The instrument consisted of four sections (A–D). Section A collected information on respondents’ socio-demographic characteristics, including age, marital status, education level, ethnicity, religion, occupation, and professional background. Section B addressed questions regarding the pattern of breastfeeding. Section C focused on the influence of employment status on breastfeeding, Section D assessed respondents’ awareness of the benefits of exclusive breastfeeding, and Section E explored factors influencing exclusive breastfeeding practices among mothers of different occupational groups.
Validity and reliability of the instrument
The questionnaire underwent face and content validity. The face and content validity of the questionnaire was assessed by experts in the College of Medicine and Health Sciences of the University, and experts in the nursing field to determine its scope, relevance, and content. All their suggestions were used to revise the instrument before the questionnaire was administered. A pre-test was also conducted amongst 10% of the sample size, to further ascertain the validity of the instrument. To assess the reliability of the instrument, a test-retest method was employed. The questionnaire was administered to 22 women (representing 10% of the sample size) who shared the same characteristics as the intended study participants. These women completed the questionnaire twice, with a 2-week interval between administrations. The reliability coefficient was calculated to determine the instrument’s dependability and internal consistency of responses. The items showed a high intra-class correlation coefficient of 0.84, indicating the questionnaire’s validity.
Data collection procedure
Data collection took place over 12 weeks, with participants self-administering the questionnaires. The researchers approached the participants at their respective workplaces. Both verbal and written informed consent were obtained from all respondents before data collection.
Data management and statistical analysis
After data collection, the questionnaires were carefully reviewed for completeness. The manually entered data was analyzed using IBM Statistical Product and Service Solutions (SPSS) version 23. The results were summarized using frequency tables, percentages, charts, and descriptive statistics such as mean and standard deviation. The relationship between variables was assessed using the chi-square (χ2) test. A one-tailed p-value of 0.05 was considered statistically significant for all inferential analyses.
Ethical considerations
Ethical clearance was obtained from the Ethics and Research Committee of Afe Babalola University (AB/EC/21/02/158). Informed consent was obtained from all study participants, and the study was conducted following the principles outlined in the Declaration of Helsinki. The researchers ensured the privacy and confidentiality rights of the participants, and respondents were assured that their data would be used solely for research purposes.
Results
A total of 222 questionnaires were distributed, with 191 retrieved and analyzed, yielding an 86% response rate.
Socio-demographic characteristics of respondents
Baseline socio-demographic information is presented in Table 1 and Figures 1 and 2. The mean age of respondents was 32.4 ± 2.1 years. A majority (84.8%) were married, and nearly three-quarters (70.2%) had tertiary education. The predominant ethnic group was Yoruba (78.5%), and Christianity was the most common religion (84.3%). Occupational distribution revealed that 65% of respondents were professionals (white-collar job): nurses (27.8%), bankers (21.0%), and lecturers (16.2%), while 35.0% were non-professional (artisans): hairdressers (18.5%), and tailors (16.2%).
Socio-demographic characteristics of respondents.

Mean age of respondent
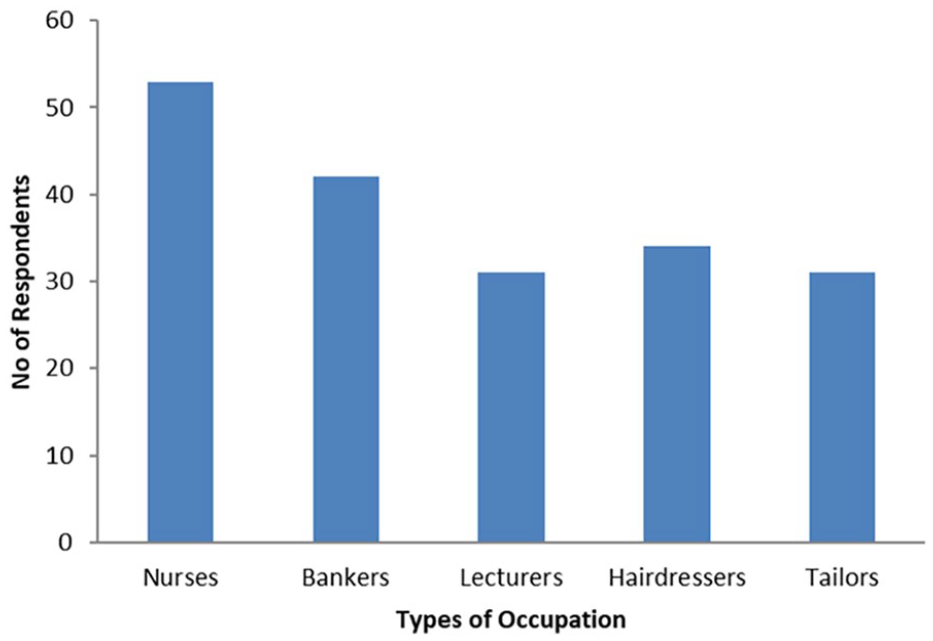
Respondents by occupation.

Classification of respondents based on professional background.
Patterns of breastfeeding among respondents
Breastfeeding patterns are detailed in Table 2 and Figures 3 to 6. A majority (61.3%) breastfed within an hour after birth, about a third (34.0%) breastfed after an hour, and a few (4.2%) breastfed after 24 h or more. The majority (71.2%) practiced exclusive breastfeeding (EBF) for the first 6 months. Reasons for not practicing EBF included the nature of the job (16.2%), insufficient breast milk production (5.8%), and stress (3.7%). Other reasons cited were concerns about weight gain, sagging breasts, soreness, lack of sleep, and tiredness. The most convenient feeding methods reported at work were breastfeeding (56.0%), formula feeding (39.8%), and other methods (4.2%).
Pattern of breastfeeding among respondents.


Respondents who exclusively breastfeed their babies for the first 6 months.
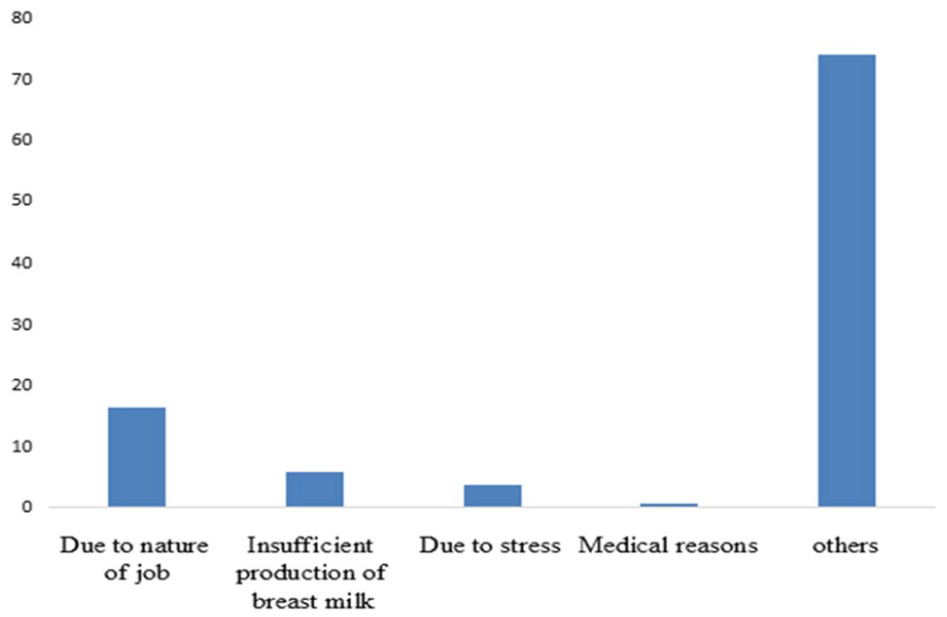
Reasons for not exclusively breastfeeding babies for the first 6 months.

Age when babies were introduced to other food/milk/water.
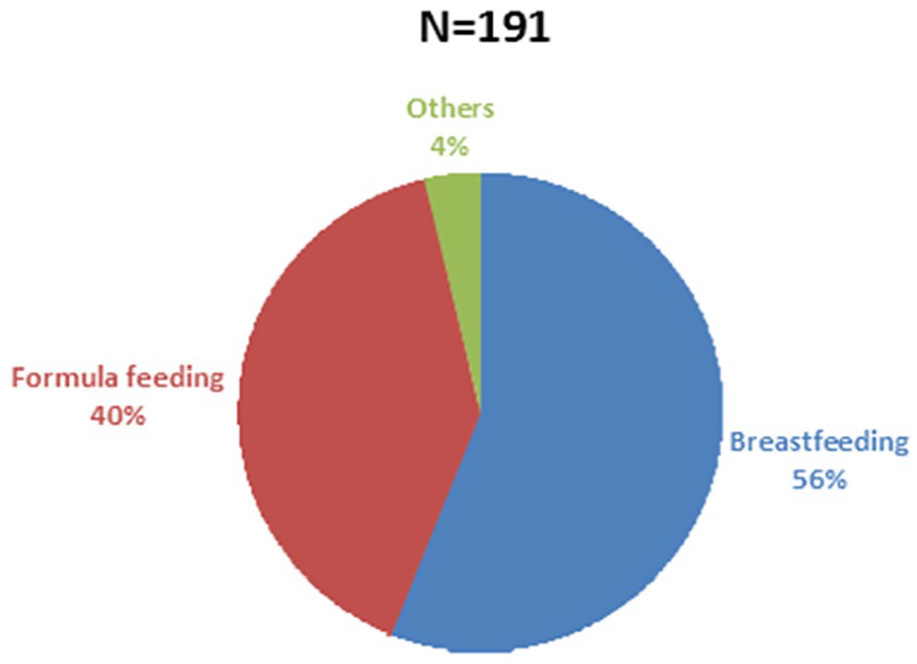
Most convenient feeding method while at work.
Influence of employment status on breastfeeding
Around half (55.0%) reported not being allowed to keep babies at work, while 52.4% said they had special break time to breastfeed. Only 60.7% said their workplace supports breastfeeding post-maternity. Babies were kept during working hours in crèches (55.5%), with the mother (25.7%), and with a maid (13.6%), as shown in Table 3.
Influence of employment status on breastfeeding.

Knowledge on benefits of breastfeeding among respondents
Table 4 highlights respondents’ knowledge of breastfeeding benefits. Most knew about colostrum (86.9%) and its role in boosting immunity (89.5%). A majority (91.1%) were aware that babies should be exclusively breastfed for the first 6 months, with such babies being healthier (85.3%). Knowledge of other benefits included mother-child bond (97.9%), disease prevention (97.4%), and diarrhea prevention (90.6%). A majority (84.3%) were well-informed about breastfeeding benefits, with a few (15.7%) having poor knowledge, as shown in Figure 7.
Respondents’ knowledge on benefits of breast feeding (n = 191).


Knowledge level of respondents on benefits of breastfeeding.
Factors influencing breastfeeding among respondents
Factors promoting breastfeeding included spousal support (69.1%), information from health workers (75.9%), encouragement from friends (37.7%), and support from relatives (52.9%). Barriers included lack of proper place to breastfeed (32.5%), insufficient milk production (32.5%), maternal health challenges (29.3%), inadequate workplace support (30.9%), and lack of time (45.0%; Table 5).
Factors that influence breastfeeding among mothers of different professional groups.

Relationship in the time of initiation of breastfeeding between white collar jobs mothers and self-employed mothers
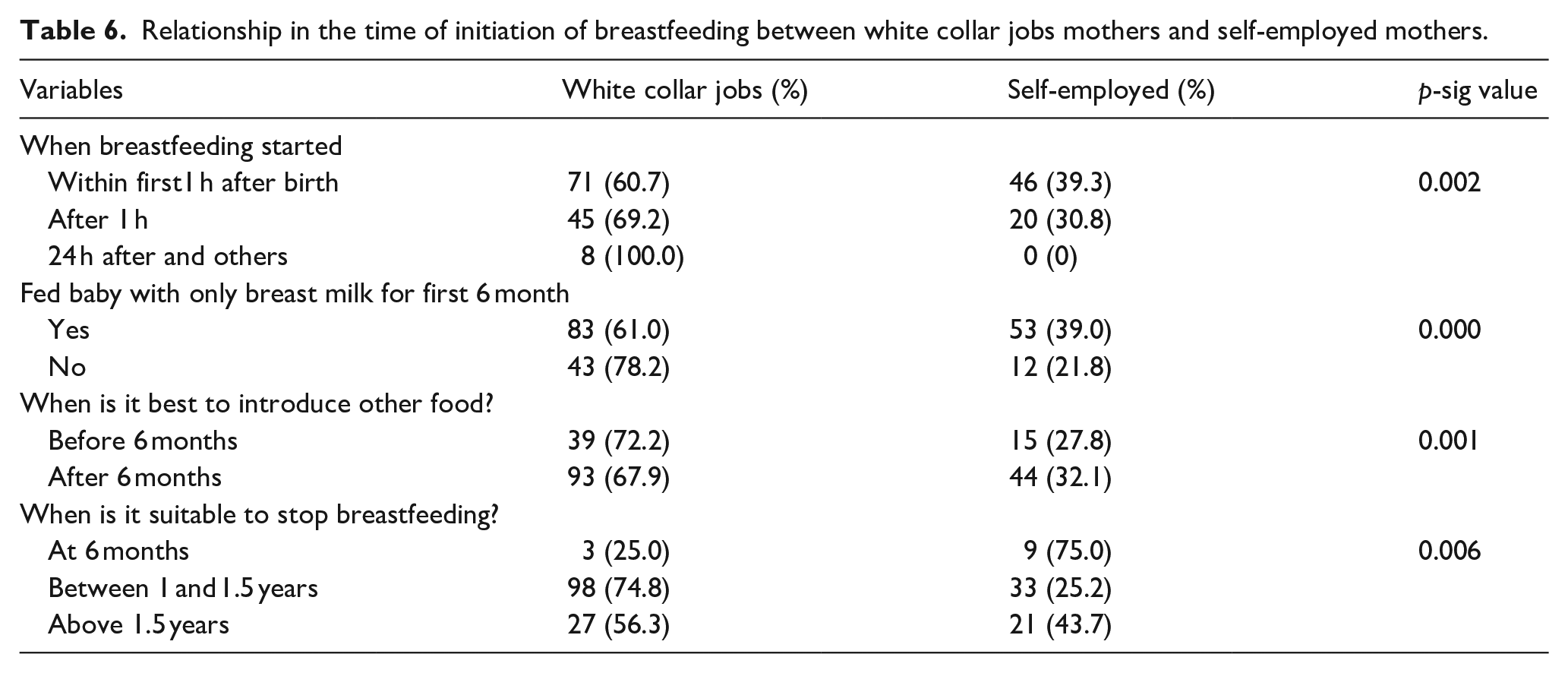
Table 6 reveals a higher proportion of white-collar job mothers (60.7%) breastfeeding within the first hour compared to self-employed mothers (39.3%). Similarly, more professional job mothers (61.0%) practiced exclusive breastfeeding compared to non-professional job mothers (39.0%) which is measured and defined as good feeding practice. Additionally, a greater proportion of professional job mothers (74.8%) believed the appropriate time to stop breastfeeding is between 1 and 1.5 years compared to non-professional job mothers (25.2%). These findings demonstrate a statistical relationship between breastfeeding patterns and mothers’ occupations.
Relationship in the time of initiation of breastfeeding between white collar jobs mothers and self-employed mothers.
Relationship between educational status and breastfeeding practice
Table 7 indicates that most mothers practicing exclusive breastfeeding (65.4%) had tertiary education. A statistically significant association was found between educational level and exclusive breastfeeding practice (p = 0.049).
Relationship between education level and practice of exclusive breastfeeding among mothers.

Discussion
In our study, most of the respondents demonstrated good infant feeding practices and engaged in exclusive breastfeeding (EBF) for the first 6 months postnatally. This positive practice seems to be linked to a higher proportion of participants engaged in white-collar work, most at the university level, which presumes a higher level of education among them. Such a connection between education and infant feeding practices has been observed in different regions. 19
The study’s findings indicate a significant relationship between breastfeeding patterns and maternal occupation, as well as a correlation between maternal education and exclusive breastfeeding. Mothers with professional jobs were more likely to practice exclusive breastfeeding than those who were without professional jobs. This could be attributed to higher educational levels among white-collar job mothers, leading to better awareness of EBF benefits.20 –24 This finding is supported by studies showing that formal employment often provides better conditions for breastfeeding, such as designated lactation rooms and paid time off. 25 This finding corrugated with those in another study conducted by, 26 which concluded that creating adequate conditions for breastfeeding mothers which are mostly likely provided by professional workers fosters the continuity of exclusive breastfeeding, and workplace lactation programs increased duration and exclusive breastfeeding.
Effectiveness of workplace lactation interventions on breastfeeding outcomes in the United States: an updated systematic review. 26 The financial pressures faced by non-professional or informal workers might contribute to shorter breastfeeding periods due to early returns to work. 27 Contrary to some prior claims, the study’s results oppose the idea that professionally employed mothers are less likely to breastfeed for an extended period.28,29 The variation in these findings could stem from factors such as job demands, workplace stress, and other barriers. This is also congruent with the findings from another study conducted in South Africa by, 30 which suggests that breastfeeding mothers especially in low-income settings like South Africa are bound to socio-cultural attitudes and consider exclusive breastfeeding as a taboo, while others are unaware of the benefits they are bound to enjoy as breastfeeding mothers.
Also, these cross-national variations in breastfeeding practices may be partially explained by the various social policies in place. Maternity leave regulations differ substantially across the European Region: countries like Sweden, Finland, and Portugal, which offer lengthy and well-compensated maternity leave and have greater uptake, flexibility, and division of leave between parents, show better breastfeeding outcomes in terms of initiation and duration. 31
While most respondents in this study were knowledgeable about the benefits of breastfeeding, some cited job nature, limited milk supply, sagging breasts, stress, and medical reasons as reasons for not exclusively breastfeeding. Similar studies have reported concerns about sagging breasts affecting physical appearance4,8,32 and a lack of breast milk 33 as factors influencing mothers’ choice to not exclusively breastfeed. This is also in line with another study conducted by, 34 where breastfeeding mothers admitted to not practicing exclusive breastfeeding because of concerns about their sagging breasts impacting their physical appearances.
In terms of workplace support, most respondents reported having breastfeeding support. This aligns with previous research highlighting the importance of workplace support for exclusive breastfeeding. The study also brings out the significance of spousal and family support, which can play a crucial role in sustaining breastfeeding practices. 35
This study underscores the importance of maternal education, workplace support, and familial encouragement in promoting breastfeeding practices. It highlights the complex interplay of factors like occupation and education in shaping breastfeeding behaviors. Such insights are valuable for tailoring interventions to promote exclusive breastfeeding practices among different occupational and educational groups. In line with the findings from this study, policies that allow for breastfeeding breaks not just in formal sectors but also in informal settings should be put in place to ensure good breastfeeding practices, thereby contributing positively to public health policy.
Limitations
Despite achieving a commendable response rate, this survey is not without its limitations. The cross-sectional nature of the study design restricts our ability to draw definitive conclusions about the causal relationships between maternal education, occupation, and breastfeeding behaviors. Longitudinal research would be better suited to establish causal links over time. Additionally, there was an uneven distribution of professionals and non-professionals in the sample, which could have influenced the statistical associations observed between variables. The inclusion of other regions in Nigeria as well as occupations could go a long way in enhancing the transparency of the study.
Furthermore, the population studied does not reflect the Nigerian population labor distribution due to the sample being chosen from higher education institutions and from a major population center.
Consequently, care should be exercised when extrapolating the study findings to other Nigerian states or regions.
Furthermore, reliance on self-reported data may introduce recall or social desirability bias, which could impact responses, especially concerning breastfeeding practices.
Conclusion
Our study showed mothers in white-collar and professional occupations exhibited more appropriate breastfeeding practices compared to self-employed mothers. In addition, a significant relationship was also found between exclusive breastfeeding practice and maternal education. Mothers engaged in white-collar and professional occupations tend to exhibit better breastfeeding practices compared to self-employed mothers.
Our results underscore the necessity for nurses, midwives, and other stakeholders as well as policymakers to prioritize self-employed mothers, particularly those in artisan occupations, and offer support systems to enhance their breastfeeding practices. Self-employed mothers represent a substantial portion of the female population in emerging economies. Therefore, there is a call for more workplace support for breastfeeding mothers, especially those who are in informal sectors
Footnotes
Acknowledgements
The authors extend their gratitude to all the participants who generously contributed to this study. Their cooperation and involvement have been invaluable to our research.
Author contributions
DTE: conceptualization, project design, data analysis, project administration, paper writing. AAS: data analysis paper writing and revising the manuscript. OEA: data collection and literature searches. AO: review and editing. TAA: Data analysis and literature searches. CGR: writing original draft, reviewing and editing, revising the manuscript. All authors read and approve the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset is available from the corresponding author on reasonable request.