
Abstract
Background:
Molar Incisor Hypomineralisation (MIH) and Hypomineralised second primary molars (HSPM) are qualitative defects of enamel of systemic origin. The objectives of this study were to investigate the prevalence and clinical presentation of MIH and HSPM among Saudi primary school children in Buraydah, Saudi Arabia, to investigate the association between MIH and HSPM, and to assess the association between MIH and HSPM with possible risk factors.
Design and Methods:
This was a descriptive cross-sectional study involving 325 primary school children in Buraydah, Saudi Arabia. Data was collected via questionnaire and clinical examination that was conducted by two calibrated examiners, according to the criteria of the European Academy of Paediatric Dentistry (EAPD). Descriptive statistics, Chi-square tests/Fisher’s exact tests and odds ratio were used; the significance level was set at p-value ≤ 0.05.
Results:
The prevalence values of MIH and HSPM were 18.5% and 11.4%, respectively. There was a significant association between MIH and HSPM (OR = 8.38, 95% CI = 4.027–17.437, p < 0.05). Demarcated opacity (78.5%) was the most common clinical pattern in MIH affected teeth; atypical caries (42.4%) was the most common in cases with HSPM. MIH was significantly associated with otitis media during the first 4 years of life (OR = 3.552, 95% CI = 1.362–9.262, p < 0.05).
Conclusions:
MIH and HSPM are common conditions amongst Saudi children (18.5% and 11.4% respectively). HSPM is a risk factor for MIH. Otitis media is associated with MIH. Further research on the aetiology of these conditions is needed.
Keywords
Significance for public health
Molar incisor Hypomineralisation has a significant impact on oral health and oral health-related quality of life of children; it is related to tooth destruction, rapid caries progression, hypersensitivity and poor aesthetics. Additionally, it imposes a treatment burden since its management is very challenging. Variations and possible rise in the prevalence of MIH had been widely reported, with few studies from Saudi Arabia. Results of the current study showed a high prevalence of MIH among children in Buraydah, Saudi Arabia and identified the most common clinical presentations. Realising this might highlight the problem to health and dental authorities and help in the provision of appropriate policies and management strategies. Investigating the risk factors and the associated condition (HSPM), in the current study, is also valuable to public health since it helps in prioritising children prone to develop MIH and providing them with the appropriate early management.
Introduction
The term Molar Incisor Hypomineralisation (MIH) was first suggested by Weerheijm et al. 1 and was adopted in 2003 by the European Academy of Paediatric Dentistry (EAPD) to describe a condition defined as hypomineralisation of systemic origin of one to four permanent first molars frequently associated with affected incisors. 2 MIH is a qualitative defect of enamel caused by reduced mineralisation, characterised by normal enamel thickness with the affected areas having decreased mineral content and increased protein and water content. The clinical presentation differs between patients and between teeth in the same person.2,3
Guidelines set by the EAPD are often used to diagnose MIH. Their criteria include clearly demarcated opacity in the occlusal and buccal surfaces of the crowns, white or yellow-to-brown discolourations, MIH defects of at least 1 mm in diameter, the presence of hypersensitivity, the presence of atypical restorations and the need for extraction of permanent teeth. 2
MIH has a multifactorial aetiology with the duration, timing and severity of the aetiological factors being related to the variability in the clinical characteristics of the condition. Several potential factors and conditions may act additively or synergistically to increase the risk of MIH. These include systemic pre- and peri-natal factors, such as maternal illness, caesarean section, perinatal hypoxia, premature birth and low birth weight. Childhood events occurring in the critical period for MIH, from birth to 4 years of age, such as measles, bronchitis, otitis, pneumonia, asthma, urinary tract infection, fever, kidney diseases, gastric disorders and antibiotic use were also found to have association with MIH. The role of genetic predisposition and epigenetic effect is becoming more prominent in recent research.4,5
Furthermore, demarcated opacities affecting both primary and permanent dentitions have been reported. The condition named as Hypomineralised Second Primary Molar (HSPM) is hypothesised to increase the risk of MIH on account of the fact that formation and mineralisation of second primary molars and first permanent molars occur at the same period of time.6,7
Studies on the prevalence of MIH in different parts of the world showed considerable variations. In a recent meta-analysis, 8 the prevalence of MIH ranged between 0.48% 9 and 46.6%. 10 A meta-analysis by Mc Carra et al. 11 declared the prevalence of HSPM to range between 0% 12 and 41%. 13
Management of MIH is often very challenging to dentists due to several factors including tooth sensitivity, difficulty achieving adequate local anaesthesia, complicated dental restorations and aesthetic concerns. Different treatment modalities are usually needed; these include options such as desensitisation and remineralisation, resin infiltration, sealants, micro-abrasion, composites, veneers, crowns and even extraction of teeth. 4
We chose to conduct the current study because the rise in prevalence of MIH 8 and its impact on oral health-related quality of life, 4 as well as the multiplicity of potential associated risk factors and the scarcity of MIH and HSPM studies in Saudi Arabia, should receive greater consideration from dentists and healthcare policy makers. Thus, the primary objective of the current study was to investigate the prevalence and clinical presentation of MIH among 8–10 years old Saudi primary school children in Buraydah City at Al-Qassim, Saudi Arabia. The secondary objectives were to investigate the prevalence and clinical presentation of HSPM in the same population, to assess the association between MIH and HSPM, and to assess the association between MIH and HSPM with some possible risk factors.
Design and methods
Study design and population
This study was a descriptive cross-sectional study conducted between 2022 and 2023 among Saudi primary school children in the city of Buraydah. Buraydah is the capital city of Al-Qassim Province in the central region of Saudi Arabia. It is a growing city with a moderate development index and a population estimated as 741,000 inhabitants of which more than 62,000 are primary school children. Approval was obtained from the Committee of Research Ethics of Qassim University, Saudi Arabia.
The sample size was calculated based on a previous study in Riyadh, Saudi Arabia 14 with a 15.2% prevalence of MIH. For a margin of error of 4%, a confidence level of 95%, the minimum sample size required was 310. Considering a potential loss or non-response of 20%, the desired sample size was calculated as 388 children.
A stratified random sampling technique was used. Six primary schools were selected randomly from the list of schools from the Ministry of Education; then students were randomly selected from the appropriate grades. With the help of school authorities, a form consisting of the written informed consent and the questionnaire were sent to the children’s parents.
Participants of this study included Saudi primary school children in the age range of 8–10 years who had the informed consent been signed by the parent. Excluded were children whose parents did not sign the consent, those with orthodontic appliances, children with Special Health Care Needs and children who did not assent to examination.
Diagnostic criteria
Diagnosis for MIH and HSPM was carried out according to the criteria designated initially by the European Academy of Paediatric Dentistry (EAPD) 3 (Table 1). Sixteen index teeth, the first permanent molars, permanent incisors and second primary molars, were scored using the charting method (short form) developed by Ghanim et al. 15 This charting format consists of two main sections: one considering the visual clinical status criteria of enamel lesions and a second considering the lesion extension criteria (Table 1). To identify a child as having MIH, at least one first permanent molar should be diagnosed with MIH (scores 2–6 in the clinical status criteria of the EAPD). For HSPM, at least one second primary molar should be diagnosed with HSPM (scores 2–6 in the clinical status criteria of the EAPD). The tooth had to have at least one-third of its clinical crown visible to be scored.
EAPD criteria for diagnosis of MIH and HSPM.

Training and calibration
Data was collected by two investigators, one of whom was an experienced paediatric dentist (the second author) who directed the training and calibration process. The first stage was the training phase, which was completed at the College of Dentistry, Qassim University. Both photographic images and actual examination of children were used to illustrate and discus the different clinical patterns and lesion extensions of MIH and HSPM according to the EAPD criteria and Ghanim et al. short charting form. 15 Images of cases that should not be included, such as fluorosis and amelogenesis imperfecta, were also discussed. Then, the two investigators examined 30 children, who were not part of the study participants, in a school setting to test the inter-examiner reliability. The two investigators repeated the examination of the same children after 2 weeks to test the intra-examiner reliability. The results were tested using Cohen Kappa coefficient. Kappa values for the inter-examiner reliability of MIH and HSPM diagnosis were 0.87 and 1 respectively. For the intra-examiner reliability, Kappa values for the diagnosis of MIH and HSPM were 0.87 and 0.84 for the first investigator, 0.93 and 1 for the second investigator. All the results indicated perfect agreement.
Data collection
Data collection was done in two steps, a questionnaire and clinical examination. The questionnaire was used to identify some possible risk factors of MIH and HSPM. It included:
● Personal information
● Duration of pregnancy
● Method of delivery
● Weight of the child at birth
● Duration of breast feeding
● Maternal diseases during pregnancy (gestational hypertension and gestational diabetes)
● Childhood diseases during the first 4 years of life (asthma, otitis media, frequent antibiotics intake, chicken pox, gastrointestinal problems, jaundice, eczema, urinary tract infections, frequent tonsillitis).
The clinical oral examination was done inside the schools’ settings. Each child was examined while sitting in an up-right position on an ordinary chair; a portable headlight was used. The examiners used sterile mirrors, dental probes, tweezers, cotton rolls, examination gloves and face masks. The probe was initially used to gently remove dental plaque and food remnants from the tooth surfaces if needed. Cotton rolls were used to clean the teeth surfaces. The examination was performed on wet and clean teeth.
Statistical analysis
The data were analysed using the IBM SPSS Statistics for Windows, Version 26. All study variables were categorical. Descriptive statistics (frequencies and percentages) were used to describe the variables -prevalence of MIH and HSPM, the clinical patterns (demarcated opacities, PEB, atypical restoration, atypical caries, missing due to MIH/HSPM) and the lesion extensions (I, II, and III) of both conditions. Pearson’s Chi-square test (or Fisher’s exact test) and odds ratio (OR) were used to test the association between two dependent variables (MIH and HSPM) and the independent variables (gender and the risk factors listed in the questionnaire). The Chi-square test was used to determine the statistical significance between the variables. However, when expected cell counts were notably low, Fisher’s exact test was applied. Statistical significance was set at p-value ≤ 0.05.
Results
Response rate
With the help of the schools’ authorities, 400 leaflets, each containing the informed consent form and the questionnaire, were sent to the children’s parents. Among these, 341 consented to participate in this study, yielding a response rate of 85.3%. Sixteen children were excluded, three with orthodontic appliances (space maintainers), five were uncooperative and did not assent to participate and eight with incomplete answers to the questionnaire. No replacement was made for the non-consenting or excluded participants. Thus, the final sample consisted of 325 primary school children, of whom 156 (48.0%) were girls and 169 were boys (52.0%).
Prevalence of MIH and HSPM
The prevalence of MIH and HSPM among the total sample was 18.5% (n = 60) and 11.4% (n = 37) children consecutively. As shown in Table 2, there was no significant difference between girls and boys regarding the prevalence of both MIH and HSPM (p > 0.05).
Distribution of MIH and HSPM between girls and boys.
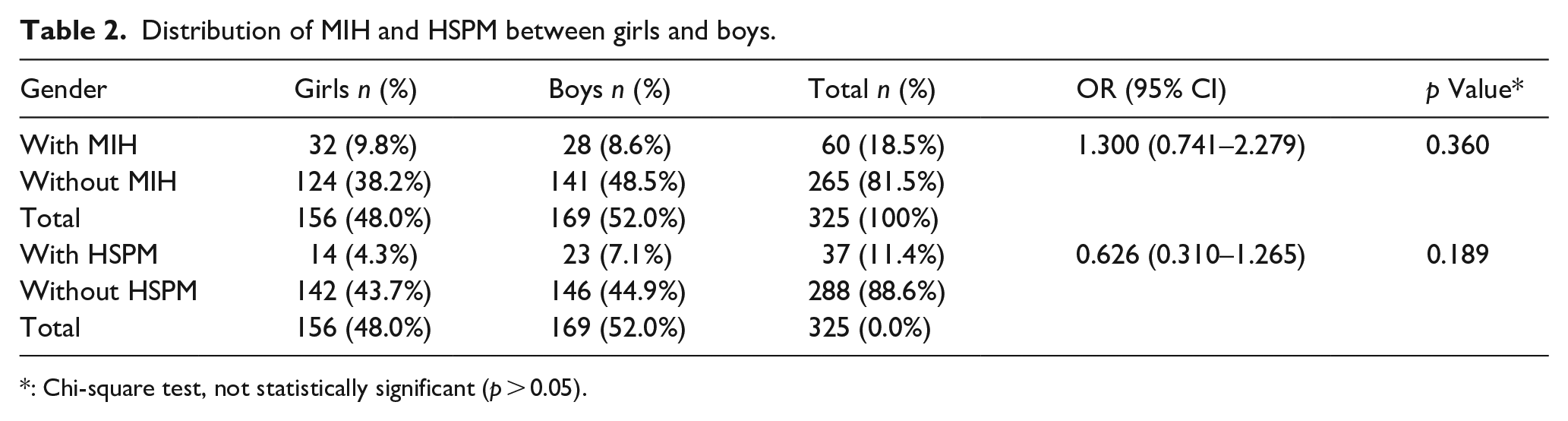
: Chi-square test, not statistically significant (p > 0.05).
Association of MIH and HSPM
As Table 3 displays, there was a significant association between MIH and HSPM (p < 0.05). Children with HSPM had odds ratio for having MIH 8.38 times higher children without HSPM (95% confidence interval [CI] = 4.027–17.437).
Association between children with MIH and children with HSPM.

CI: confidence interval; *: Chi-square test; **: p < 0.05 is significant.
Clinical Pattern and lesion extension
Figure 1 shows the distribution of clinical patterns in teeth affected with MIH and HSPM. Regarding children with MIH, 191 teeth were affected. Amongst these, the most common clinical pattern was the demarcated opacity (n = 150, 78.5%). As for HSPM, 85 teeth were affected and the most common clinical pattern was the atypical caries (n = 36, 42.4%).

Distribution of the clinical patterns of MIH and HSPM defects.
Figure 2 shows the extension of the lesion in teeth affected with MIH and HSPM. Of the 191 teeth affected with MIH, the most prevalent was type I extension (n = 113, 59.2%). As for the 85 second primary molars affected with HSPM, the most prevalent was type III extension (n = 45, 52.9%).

Extension of the lesion in teeth affected with MIH and teeth affected with HSPM.
Risk factors
The association of both MIH and HSPM with possible risk factors are shown in Tables 4 and 5 consecutively.
Association between MIH and possible risk factors.

: Chi-square test/Fisher’s exact test; **: p < 0.05 is significant.
Association between HSPM and possible risk factors.

: Chi-square test/Fisher’s exact test; **: p < 0.05 is significant.
As shown in Table 4, the results of the current study showed a statistically significant association (p < 0.05, OR = 3.552, 95% CI = 1.362–9.262) between MIH and having otitis media during the first few years of life. All the other health risk factors investigated were not significantly associated with MIH (p > 0.05).
As for HSPM, our results showed that it was statistically significantly associated (p < 0.05) with the occurrence of some childhood diseases during the first 4 years of life namely otitis media, frequent antibiotics intake and GIT problems. Other investigated possible risk factors did not show statistically significant associations with HSPM (Table 5).
Discussion
A substantial body of epidemiological research on the prevalence of MIH has been published worldwide. Hence, significant concerns have been expressed about a probable rise in the prevalence of MIH. 8 This is a very crucial issue since evaluating regional and global burden of MIH and trends in its prevalence is essential for decision makers and dental care providers so as to best address the treatment needs regarding MIH. Thus, this study was conducted to investigate the prevalence of MIH (primarily) and HSPM (secondarily) and their associated factors. The sample size (325 children) fitted the recommendations by Elfrink et al. 16 that a minimum of 300 children should be included for prevalence studies of MIH. Similarly, the age of the current study participants was 8–10 years is compatible with the recommendation that the favourable examination age for MIH is 8 years since, at this age, most children have erupting first permanent molars.2,16
This study showed the prevalence of MIH among Saudi primary school children in Buraydah, in the Central Region of Saudi Arabia, to be 18.5%. It is worth mentioning that the relatively high response rate (85.3%) is a considerable advantage in our sample. Our result is comparable to the weighted mean prevalence of 12.8% calculated in a meta-analysis by Sluka et al. 8 Reports from different countries have shown variable prevalence results such as Spain (28.63%), 17 Norway (28.2%), 18 Sudan (20.1%) 19 and the United Arab Emirates (38.9%). 20 Comparing our finding with other studies from Saudi Arabia displays some variations. MIH prevalence was reported to be 15.2% 14 in Riyadh, 8.6% in Jeddah 21 and 25.1% in Qassim. 22 These variations could be attributed to factors such as differences in methodologies, population criteria, the ages of participants, samples and sampling techniques. However, it is noteworthy that all the studies used the EAPD criteria.
The prevalence of HSPM in the current study was 11.4%. This is higher than the overall pooled prevalence of 6.80% reported in a recent meta-analysis by McCarra et al. 23 However, the same meta-analysis showed a very wide range in the prevalence of HSPM, from 0.0% in West Bengal 12 to 41.0% in Syria. 13 Interestingly, the subgroup analysis from the same article, displayed that the pooled prevalence in the studies that used the EAPD criteria was slightly higher (7.54%). 23 Studies from Saudi Arabia showed lower prevalence of 9.4% in Riyadh 14 and 5.4% in Southern Saudi Arabia. 24
Our finding that there was no gender predilection of MIH is consistent with the results of a meta- analysis by Lopes et al. 25 However, some studies reported significant differences between girls and boys. 17 HSPM, as well, showed no gender differences in the current study; which is in agreement with to some earlier reports.13,26
In accordance with many previous studies, we found a significant association between MIH and HSPM (OR = 8.38, p < 0.05). Although some researchers did not find a significant association between MIH and hypomineralisation in primary molars,27,28 a recent meta-analysis by Zhang et al. 29 demonstrated a definite correlation between HSPM and MIH indicating that HSPM may act as a predictor for the occurrence of MIH. It is noteworthy that many authors have stated that not all cases of MIH are preceded by HSPM.6,29 The obvious explanation for the association between these two conditions is that second primary molars and first permanent molars share the same timing of amelogenesis and mineralisation. 7 This finding has important implications; identifying patients expected to develop MIH would help in managing this condition at an early age and hence reduce the problems associated with these enamel defects.
In this study, we found that demarcated opacity, which is the mildest form, constituted the most frequent clinical pattern amongst teeth affected with MIH (n = 150, 78.5%) followed by post-eruptive enamel breakdown (PEB; n = 15, 7.9%) and atypical restorations (n = 15, 7.9%); this was consistent with many previous studies.14,19,22,28 As for HSPM, our results showed that atypical caries followed by atypical restorations are the most prevalent patterns (n = 36, 42.4% and n = 30, 35.3% respectively). However, this finding differs from many other published studies that showed demarcated opacity to be the most prevalent in cases of HSPM.23,24,28 On the other hand, our finding was similar to a study in Saudi Arabia by Almuallem et al. 14 which reported that the most common clinical patterns of HSPM were atypical caries (38.68%) followed by atypical restorations (30.50%).
Regarding the extension of the lesions on teeth surfaces, in agreement with previous reports,14,17 the current study showed that type I (less than 1/3 of the crown affected) was the most prevalent type (n = 113, 59.2%) in teeth affected with MIH. As for HSPM, our results showed the most prevalent to be type III (more than 2/3 of the tooth affected) which accounted for 52.9% (n = 45) of cases. This result disagrees with an earlier finding from Canada 28 which showed the most prevalent to be type I (less than 1/3 of the crown affected). However, Almuallem et al. 14 in agreement with our findings, conveyed that type III (more than 2/3 of the tooth affected) is the most common in Saudi Arabia.
The results of the current study clearly indicate that the mildest forms of MIH, in terms of both the clinical pattern and the lesion extension, are the most prevalent. This may be attributed to the fact that we studied the age group of 8–10 years, as 8 years is the age recommended by the EAPD for MIH prevalence studies.2,16 At this age, the index permanent teeth are newly erupting and presumably still intact. The more destructed clinical patterns are most likely seen in older children.17,18 Regarding HSPM, the recommended age for diagnosis and prevalence studies is 5 years. 16 This was not the case in our study since it was designed to fit the primary objective of assessing MIH, with HSPM being a secondary objective. This may possibly explain our current results, as the older age at examination time means that affected teeth had been present in the oral cavity for longer periods of time and were thus prone to exhibit more destruction resulting from the presence of the enamel defects. It may also be the reason for the more severe degrees of HSPM compared to MIH observed in the present study.
The current study investigated the association between MIH, HSPM and various risk factors. Otitis media was significantly associated with MIH (p < 0.05). Interestingly, the same finding was reported in two other studies from Saudi Arabia.14,21 Parallel to this, otitis media was one of the aetiological factors identified as significant in a meta-analysis by Garot et al. 5 In general, the literature regarding factors associated with MIH shows substantial variations. In our study, all other risk factors investigated (prenatal, perinatal and postnatal) were not significant (p > 0.05). In contrast to our results, the meta-analysis by Garot et al. showed MIH to be associated with caesarean delivery, asthma, frequent antibiotics intake, GIT disorders, UTI and tonsillitis. 5 Nevertheless, they agreed that weight of the child at birth, duration of breast-feeding, maternal diabetes, maternal hypertension, chickenpox, and jaundice were not associated with MIH (p > 0.05). 5 On the other hand, another meta- analysis by Juárez-López et al. 30 determined antibiotic use and weight of the child at birth to be significantly associated with MIH. This wide variation supports the scientific consensus about the multifactorial aetiology of MIH. It may also indicate that some aetiological factors have greater effects than others. Furthermore, the duration, strength and timing of event may account for the different clinical presentations of the defect4,5
The current study showed that childhood conditions -otitis media, frequent antibiotics intake and GIT problems- were significantly associated with HSPM (p < 0.05). Amongst these factors, only otitis media was also significantly associated with MIH (p < 0.05). This discrepancy in the risk factors between MIH and HSPM was surprising since first permanent molars and second primary molars develop and mineralise over the same period of time. 7 Hence, it was expected that they would share the same risk factors. However, our results should be interpreted with caution due to some limitations which include the cross-sectional study design and the recall bias, in addition to the relatively small number of children affected by HSPM in this study (37 children). One meta-analysis by Lima et al. 31 had proved significant association between HSPM and maternal hypertension, maternal smoking, prematurity, low birth weight, complications of delivery, need for an incubator, no breastfeeding, child antibiotic use, childhood asthma and fever.
When interpreting our results, it is important to acknowledge that this study has some limitations. The sample is only representative of this part of Saudi Arabia; therefore, the results may not be generalised. Another limitation is the potential recall bias since the data about medical history was collected via questionnaire. Moreover, the cross-sectional design used in the current research does not provide robust evidence that a specific risk factor has a causative role in the development of a disease. It rather implies an association between the risk factor and the disease.
MIH remains a complex condition that demands extensive research efforts. More epidemiological research, regarding both MIH and HSPM, with larger sample sizes covering wider populations is still needed. In order to obtain more valid results on the aetiology, future research should be based on documented medical records rather than self-reported questionnaires. Case-control and longitudinal studies are more suitable designs for establishing causal relationships. Also, more research about interactions between genetic and environmental factors in the aetiology of MIH and HSPM is needed.
The results of the present study have important implications for dental care services, providing a reference to ensure that appropriate strategies and efficient management are provided for children with MIH. Children with HSPM should be given special attention, as this may help with early diagnosis of MIH and thus assist in providing early treatment and decreasing prospective complications. Despite its limitations, our results may provide additional evidence supporting our understanding of the complex nature of the aetiology of MIH and HSPM.
Conclusion
The current study showed the prevalence of MIH and HSPM among 8–10-year-old primary school children in Buraydah, Saudi Arabia to be 18.5% and 11.4%, respectively, with no gender differences. The most common clinical pattern in teeth affected with MIH was demarcated opacity (n = 150, 78.5%), and the most common in teeth with HSPM was atypical caries (n = 36, 42.4%). Regarding the extent of the defects, 59.2% (n = 113) of MIH-affected teeth showed type I extension, while 52.9% (n = 45) of HSPMs showed type III extension. Children with HSPM have an 8.38 times higher odds ratio for having MIH than children without HSPM. Among the possible risk factors investigated, otitis media during the first 4 years of life was significantly associated with MIH.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki. Approval was obtained from the Committee of Research Ethics of Qassim University, Saudi Arabia under the registration No. 21-14-06.
Consent to participate
Written informed consent to participate in this study was provided by the participants’ legal guardians
Author contributions
Conceptualization: R.M.F.I. and H.A.A.H.; methodology, R.M.F.I. and H.A.A.H.; software, H.A.A.H. and R.M.F.I.; validation, R.M.F.I. and H.A.A.H.; formal analysis, R.M.F.I. and H.A.A.H.; investigation, H.A.A.H. and R.M.F.I.; resources, H.A.A.H. and R.M.F.I.; data curation, R.M.F.I. and H.A.A.H.; writing—original draft preparation, R.M.F.I. and H.A.A.H.; writing—review and editing, R.M.F.I. and H.A.A.H.; visualisation, R.M.F.I.; supervision, R.M.F.I.; project administration, H.A.A.H.
All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.