
Abstract
Background:
Retention in care is a critical indicator of the quality of HIV care and a cornerstone for achieving epidemic control. Interruption in treatment (IIT) poses a significant threat to achieving the global 95-95-95 targets and leads to adverse health outcomes. This study assessed the effect of the national clinical mentorship program on retention in care and IIT among HIV clients in Nasarawa State, Nigeria.
Methodology:
In the 47 facilities where mentors worked, every client who missed an appointment was tracked immediately. A list of potential IIT clients was generated and followed through by linking those clients to trackers who ensured they were returned to care. Mentors ensured that the process of tracking in the facilities was strengthened as part of their routine mentoring activities including facilitating the release of tracking funds. Data from the Retention and Audit Determination Tool (RADET) for patients reported between November 2021 and August 2022 were extracted and imported into an Excel template. Demographic and clinical program parameters were analyzed using descriptive statistics, bi-variate, and multivariate analysis, including Chi-square and logistic regression. The parameters in the facilities where mentorship was deployed were then compared to pre-deployment parameters.
Results:
This study found that a clinical mentorship program reduced the Interruption in treatment (IIT) rate from 7% to 0.5% between 2021 and 2022. Although the 25–34 age group had the highest IIT rate, it decreased from 41.6% to 33.3% after the mentorship program. Tertiary facilities still have the highest IIT rates. Non-pregnant women were more likely to continue with treatment than pregnant women. The mentorship program successfully reduced IIT rates in Nasarawa State.
Conclusion:
Clinical mentoring can reduce IIT among HIV patients. The study found a decrease from 7% to 0.5%. Tailored mentorship programs can improve retention in HIV care and reduce IIT rates. Gender-specific barriers should be addressed, and interventions should be customized for pregnant women for better program effectiveness and health outcomes.
Introduction
Nigeria has the largest epidemic of HIV in West and Central Africa. 1 In 2020, 1.7 million people were living with HIV/AIDS, 86,000 new infections, 49,000 AIDS-related deaths, 1 and a prevalence of 1.4% in those aged 15–45 years. 2 Over 72,000 HIV/AIDS clients are on treatment in Nasarawa State, with an adult HIV prevalence of 2%. 2
Retention in care for HIV is the spectrum of the continuum of care from the moment of HIV diagnosis to receiving a comprehensive package of lifelong services. 3 Retention in care is a marker of quality of care and is most critical for attaining epidemic control. Poor retention as manifested by interruption in treatment, IIT, will hamper not just the attainment of the 95-95-95 goal but result in poor health outcomes. 3
In October 2021, the United States Centre for Disease Control and Prevention (CDC) in conjunction with the government of Nigeria through the National AIDS and STI Control Program (NASCP), introduced the clinical mentorship program in 19 states of Nigeria, Nasarawa inclusive, to achieve the 95-95-95 UNAID targets and epidemic control. 4 The 95-95-95 speaks to 95% of estimated infected persons being tested and knowing their status as the first 95, 95% of all PLHIVs elicited being retained in treatment as the second 95 with the third 95 being 955 of clients on treatment being virally suppressed. This strategy of clinical mentorship is very much in line with the World Health Organisation’s recommendation on scaling up of HIV services to achieve epidemic control. This involves the use of experienced clinicians who conduct practical teachings to facility staff offering HIV services leading to continued medical education on a regular basis based on an initial and intermittent assessment of the needs of the facility using national guidelines. 5
In a study carried out in Zambia, Boyd et al. 6 noted that sound clinical knowledge and practice with a public health approach in the background of continuous quality improvement enables program impact at facility and provincial levels.
Interruption in treatment, IIT, is used to classify PLHIVs who are no longer being seen in clinical care. 7 This is defined as no clinical contact with the client 28 days after a missed appointment. 7 This Presidents Emergency Plan for AIDS Relief (PEPFAR) definition allows for early interventions such as tracking to return the clients back to care. 8 Treatment interruption is associated with increased viral loads, reduced CD4 cell counts, opportunistic infections, and deaths. 9 The consequences of interruption in treatment will lead ultimately to the limitation of epidemic control. 8 In Ido-Ekiti Federal Medical Center, a 7-year review published in 2015 showed poor retention was 37% of clients studied and that poor retention was associated with decreasing age, baseline CD4 cell count above 400 copies/ml, stages 1 and 4 HIV/AIDS and year of diagnosis. 10
In a retrospective study carried out in 16 States of Nigeria and published in November 2021, 32% of a cohort of PLHIVs on Antiretroviral treatment (ART) were found to have interrupted treatment. 8 Another study found a burden of 30% of IIT with being a pediatric patient on first line, being on MMD3, male sex, and clients with unsuppressed viral accounting for significant risk of IIT. 11 Significant associations with treatment interruption were age, level of facility, not having documented viral load, and frequent visits to the facility to access drugs. 8 A patients prospective study carried out in South Africa amongst clients who interrupted treatment and returned showed that mobility of clients, ART-related factors, and limitation of time due to work were important in causing an interruption in treatment. 12 Reasons given for interruption in treatment from a qualitative survey in Malawi included community-level stigma, poverty, lack of family support, side effects of ART, and feeling of well-being after commencement of ART. 13
This study aims to identify the outcome of the clinical mentorship program on clients’ retention in care across facilities to which clinical mentors are deployed in Nasarawa State of Nigeria.
A study of the burden of interruption in treatment pre- and post-deployment of clinical mentors and sociodemographic characteristics of those who interrupt treatment will help in knowing the impact of mentorship program in Nasarawa state and help in preventing high attrition rate in HIV/AIDs treatment programs and contribute to attainment of epidemic control.
Conceptual framework
IIT: Interruption in treatment.

A study of the burden of interruption in treatment, sociodemographic characteristics of clients who interrupted treatment and comparative analyses of the burden pre- and post-institution of the clinical mentoring strategy will add to the body of knowledge on the outcome of clinical mentorship, which will further drive the attainment of epidemic control.
Methodology
Study area
Nasarawa state is located in North Central Nigeria with a population estimate of 2.5 million people and covers 27,117 km2. The official language is English with Hausa, Fulani, and many other local languages. The economy of the state is centered on agriculture, mining, and trade. One hundred and forty-two facilities are offering HIV services and these include two tertiary facilities. These facilities cater to the needs of over 72,000 active clients with an interruption in treatment rate of over 2%. The State has a diverse geography with plains, mountains, and hills and is the home of many ethnic groups. The State is administered democratically with the Governor being the chief accounting officer and overseeing 13 local government areas. This study area, in this operational research, represents the geographical area allotted for official work.
Recruitment of mentors and deployment
Indigenous medical doctors in Nasarawa were recruited using structured interview questions after a due advert and shortlisting process carried out jointly by the implementing partner and the State Ministry of Health. The 10 recruited mentors had onboarding training that covered the entire cascade of care and were then allocated facilities that covered the 13 local government areas. An initial deployment to 47 facilities was done after the engagement of the clinical mentors in November of 2021. These mentors provided ongoing practical training across the HIV cascade of care to clinicians and all other staff working in the HIV space in each of the 47 facilities.
Study population and settings
Data of all PLHIVs who were enrolled within the Institute of Human Virology Nigeria (IHVN) Nasarawa network into care and received ART from 2010 to 2022 from 47 Presidents Emergency Plan for AIDS Relief/Centers for Disease Control and Prevention (PEPFAR/CDC) supported public health facilities (Tertiary, Secondary, Primary) and private health facilities across 13 LGAs was used for this study. These 47 facilities, out of a total of 126, had clinical mentors deployed in December 2021. Baseline data was collected for the baseline study in November 2021, and another set of data was collected in August 2022. IHVN is a non-governmental organization that provides quality HIV care through technical assistance and support to health facilities. In the 47 facilities where mentors worked, every client who missed an appointment was tracked immediately. A list of potential IIT clients was generated and followed through by linking those clients to trackers who ensured they were returned to care. Mentors ensured that the process of tracking in the facilities was strengthened as part of their routine mentoring activities including facilitating the timely release of tracking funds from the implementing partner. Regular mentorship is provided along the lines of the recommendation by the World Health Organisation. 5
Study design and implementation
The study is a comparative retrospective cross-sectional study of clinical data on RADET of patients enrolled on ART as of November 2021 compared to that of August 2022.
Data collection/analysis
All patients reported on the Retention and Audit Determination Tool (RADET) as of November 2021 and August 2022 were extracted. The demographic and clinical program parameters of all patients will be described using frequencies and percentages. Bi-variate and multivariate analyses using Chi square and logistic regression were conducted for patients that were active or LTFU. All the p-values reported are two-sided.
Analyses
The relationship between patient retention (active vs dropped out/inactive) with age at start of ART (in years), sex, initial regime line, initial CD4 count, current CD4 count, and viral load was examined using a logistic regression. This model produces a probability function of subjects remaining active in the program or dropping out. Using step-wise backward elimination of the least significant variables, the most parsimonious statistical model was selected as the final model. To minimize the effect of multicollinearity in cases where two variables were correlated, only one of the variable pairs was used in the model, while the other variable was used in a similar alternative model.
Ethical clearance
Ethical clearance was obtained from ethics committees of Dalhatu Araf Specialist Hospital and State Ministry of Health.
Results
Year 2021
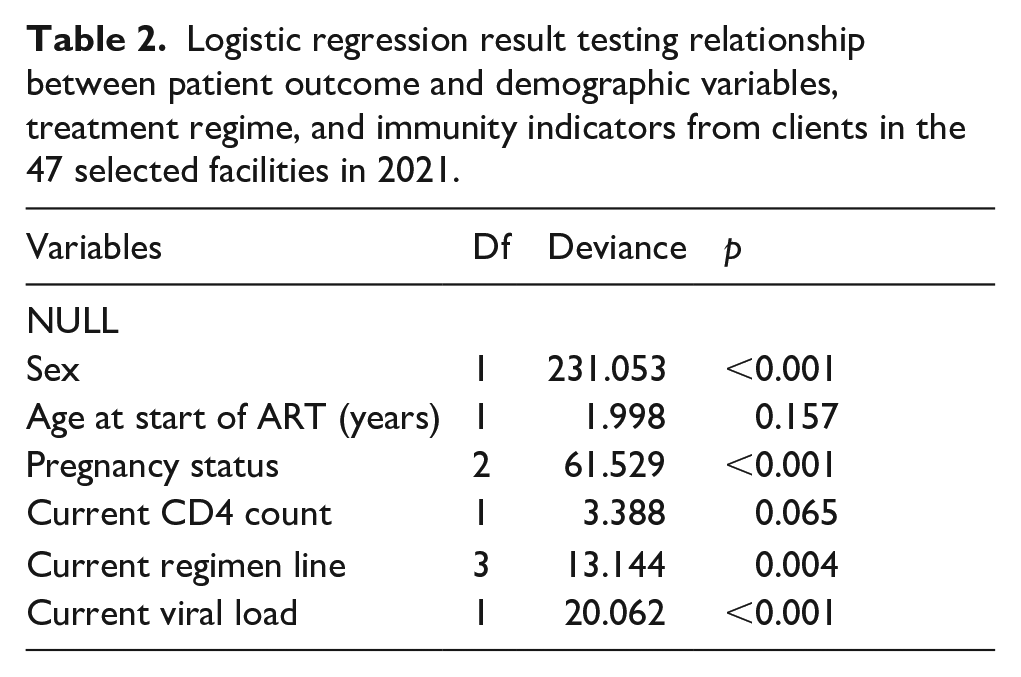
The variables that significantly predicted patient retention were sex, pregnancy status, current regimen line, and viral load (Table 2).
The probability of retention decreases with increasing viral load, with the probability of retention at about 95% at low viral load, declining as viral load increased (Figure 1).
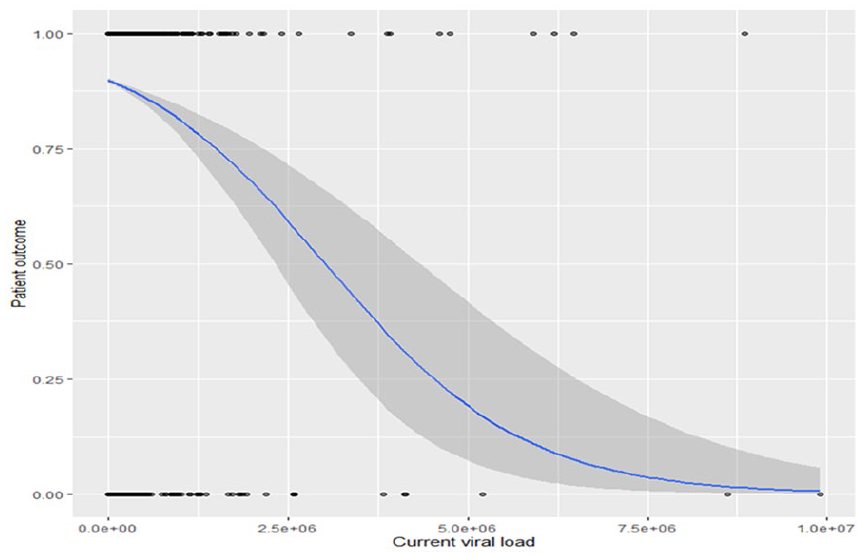
The probability of retention decreases with increasing viral load count in the 47 selected facilities from RADET of 2021 pre-deployment of mentors. Gray shading represents the 95% confidence interval.
Year 2022
The variable that significantly predicted patient retention was viral load (Table 3).
The probability of retention decreases with increasing viral load, with the probability of retention at about 88% at low viral load, declining as viral load increased (Figure 2).

The probability of retention decreases with increasing viral load count in the 47 selected facilities from 2022 RADET post-deployment of mentors.
Discussion
The IIT in these selected facilities for 2021 is 7% against 0.5% for 2022 (Table 1). Even though the IIT for 2021 was much lower than previous works documented in the country, in 2022 after 10 months of mentoring work, the IIT rate fell steeply to 0.5%, which reflects a positive outcome of the mentoring program. This achievement could be said to be the outcome of strategies already in place that yielded fruit within the year under review. However, the only new approach adopted in 2022 was bringing on board the clinical mentorship program, and thus the steep decline in IIT can be best explained by the adoption of the clinical mentorship program in the facilities under review. Further studies to compare the facilities where mentors are deployed with those facilities where mentors were not deployed will better help to resolve this and provide a causal relation or otherwise of the mentoring strategy with a reduction in facility IIT. This finding of a positive effect is comparable to the findings of similar work done in Rivers State Nigeria which found an increase in case findings and viral suppression amongst clients with the implementation of the clinical mentorship program. 14 Even though this finding is not about retention in care which this study speaks to, it addresses the impact on other thematic areas that lead to epidemic control. In Zambia, case-finding yield and viral suppression also improved post-mentoring as was found in the later study in Rivers State, Nigeria. 6
Sociodemographic characteristics of study participants (clients) from the 47 facilities in RADET.

IIT was found in this study to be related to sex (p = 0.001), pregnancy status (p = 0.004), current regimen (p = 0.001), and viral load (p = 0.001; Tables 2 and 3). Females were found in this study to be more likely to drop out of treatment, which goes against the norm where women have better health-seeking behavior. 15 A sub-optimal health-seeking behavior amongst female PLHIVs may actually be a result of lots of our women who are pregnant seeking health services outside our facilities but this certainly cannot completely explain the reversal and we need to do a deeper dive to unravel this finding. Supporting the idea that the reversal of health-seeking behavior between males versus females here is due to pregnant women seeking care outside traditional hospital facilities is the finding that non-pregnant women are more likely to remain in treatment compared to pregnant women. This can be explained by the poor utilization of antenatal services generally by our women, who prefer to deliver with traditional birth attendants even if they had a course of antenatal care in health facilities.
Logistic regression result testing relationship between patient outcome and demographic variables, treatment regime, and immunity indicators from clients in the 47 selected facilities in 2021.
Logistic regression result testing the relationship between patient outcome and demographic variables, treatment regime, and immunity indicators count in the 47 selected facilities from RADET in 2022.

Those on second-line treatment, especially in 2021, were significantly related to interruptions in treatment compared to the first-line regimen (Table 4). This is a sad reflection on the program, as it will entail that these clients will most likely fail again and will need to be switched to the third-line regimen with all the attendant challenges. However, it was good to note that with the start of the mentorship program, the IIT rate of 15% in this sub-group again crashed to 0.3%.
Type of drug regimen and frequency of dosing among study participants (clients) from the 47 facilities in the RADET.

MMD: multi-month dispensing.
High viral load was correlated with a high interruption in treatment rate, which is in keeping with the fact that these clients were not taking drugs and thus viral load was expected to rise in their bloodstream (Figures 1 and 2).
Limitation of the study
This study is limited by lack of control over the quality of original data collected and the uncontrolled variable such as the fact that the implementing partner has staff that offer similar services as the mentors. Our mentors recruitment approach of using advert placements and using structured questionnaires in the interview limited our ability for targeted recruitment of HIV specialists which would have better improved our outcomes.
Conclusion and recommendation
Clinical mentoring can reduce IIT among HIV patients. A study found a decrease from 7% to 0.5%. Tailored mentorship programs can improve retention in HIV care and reduce IIT rates. Gender-specific barriers should be addressed, and interventions should be customized for pregnant women for better program effectiveness and health outcomes.
A deep dive will need to be conducted to further unravel the dynamics at work in these sub-populations to better understand the strategies to fashion and use to mitigate the interruption of treatment.
Footnotes
Acknowledgements
The authors would like to thank the State AIDs and STI Control Program, Ministry of Health, and Dalhatu Araf Specialist Hospital for their cooperation and contribution.
Author contributions
Conceptualization of Ideas: Anthony Ajeh. Data analysis and visualization: Anthony Ajeh, Ruth Amarachi Ogbonna, Peter Attah. Writing of initial draft: Anthony Ajeh, Ruth Amarachi Ogbonna, Esther Audu. Review & editing: Ruth Amarachi Ogbonna, Toufik Abdul-Rahman, Anthony Ajeh, Adamu Alhassan Ibrahim, Ruth Amarachi Ogbonna, Peter Attah, Esther Audu, Sambo Yakubu, Oka Eze, Andrew Awuah Wireko.
Availability of data and materials
The datasets used and/or analyzed during the current study are available upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
The study received ethical approval from the Ethics Committee of the State Research and Statistics Department of Nasarawa State (NHREC Protocol No: 18/06/2017). Permission was obtained from Dalhatu Araf Specialist Hospital before data collection.