
Abstract
Background:
This study aimed to measure differences among informal caregivers, users, and mental healthcare workers (MHW) regarding job/organizational satisfaction and perceptions of respect for rights in the mental health services of one region of Italy.
Methods:
A sample of 100 caregivers, 240 MHW, and 200 users completed the “Well-Being at Work and Respect for Human Rights Questionnaire” (WWRR) in community mental health centers in Sardinia.
Results:
Caregivers reported higher satisfaction toward MHW on perceiving respect for human rights among users (5.2 ± 1.0 vs 5.1 ± 1.1, p < 0.0001) and health professionals (5.3 ± 0.8 vs 4.5 ± 1.3, p < 0.0001) and organization well-being (5.1 ± 1.2 vs 3.9 ± 1.3, p < 0.0001); toward users about respect of rights of MHW (5.3 ± 0.8 vs 4.9 ± 1.2, p < 0.0001) and both toward users and MHW on dissatisfaction on resources (p < 0.0001). Caregivers strongly highlighted insufficient resources for services.
Conclusion:
Despite caregiver satisfaction, resource deficiencies signal a critical juncture in Italian mental health care. Continued cuts in healthcare spending, especially in mental health, raise concerns for future outcomes.
Keywords
Introduction
The respect of human rights of people with disability by users and health workers in health care services is a crucial point especially in the facilities providing care for people with psychosocial disability. The respect of the human rights for people with disability was focalized and shared between nations thanks to the United Nations Convention on the Rights of Persons with Disabilities (UN CRPD). 1 The principles of the CRPD have been translated into the specific field of psychosocial disability by the WHO QualityRights initiative which underlined that, in mental health services there can be no quality care without respect for human rights.2–4
Perceptions of respect for users’ rights among users, caregivers, and mental health workers are crucial for organizational well-being in mental health care settings.5–7 Subsequent research has underlined that the perception of respect for users’ rights among users, caregivers, and mental health workers is a crucial point for care delivered may be of quality in a done mental health facility; but this element is also a structural factor of organizational well-being in mental health care settings, that is, the greater the respect for rights, the better the working climate and also the satisfaction of health professionals with their work.5–7
This construct was the starting point for developing the Questionnaire on Well-Being at Work and Respect of Rights (WWRR), designed to assess the relationships between the perceived respect of rights of health workers and users and satisfaction at work among in mental health professionals, and satisfaction of care received of users and informal caregivers of people with psychosocial disability. 8
The analysis of the principal components produced by the correlation of the scores at responses to the questionnaires from mental health workers in three Mediterranean countries and three Latin American ones has confirmed the construct as it had been hypothesized, that is, a strong correlation has been highlighted between satisfaction at work, the well-being organizational climate, and perception of respect for human rights of both health workers and users.9,10
The WWRR tool was used in surveys aimed at comparing levels of job/organizational satisfaction and perceptions of respect for rights in healthcare workers in three Latin American countries and four Mediterranean countries,11,12 including Italy where during the Covid pandemic the satisfaction levels of users and mental health workers were compared,8,13 furthermore in Italy the WWRR scores of users and health workers of mental health services were also compared with those of users and health workers of other than psychiatric care services.14,15 In Italy, health professionals showed higher scores than in other countries11,12 and, surprisingly, during the Covid pandemic, mental health users and professionals showed higher scores of satisfaction with care and job satisfaction than users and health workers of non-psychiatric services.8,13–15 This was linked to the fact that the mental health network, totally centered outside the hospital, thanks to being rooted in the territory, was able to better respond to treatment needs.
More recently the questionnaire was validated through the measurement of the main components in a sample of non-professional health caregivers, such as family members and volunteers. 16 The principal components analysis showed some differences compared to the factor structure found in users and health professionals. In fact item No. 6 concerning satisfaction with the resources used, was not part of a single component as for users and health workers. It should be noted, however, that this item had also received a very low score among users and health workers, which had been interpreted as the product of a critical moment for the public service in Italy. That is, despite a lack of resources perceived by both users and health workers, satisfaction continued to persist but with a lot of fear for the future if the cuts to resources continued.
In light of these results, it seemed interesting to measure the differences in the scores of informal caregivers with those of users and healthcare workers in the scores of the WWRR.
Aims
The aim of this work is to verify, through the comparison between the WWRR scores, whether informal caregivers show differences in satisfaction with the care received from their friends/relatives with psychosocial disabilities compared to the perception of the users themselves and mental health workers.
Design and Methods
Design
Cross-sectional design. A random sample of informal caregiver of users attending 4 community mental health centers in South Sardinia was compared with users and health workers. The comparison between the same sample of users and health workers was already published.8,12
This study was conducted between December 2023 and January 2024.
Sample
The final sample included 100 caregivers compared with 200 users and 240 health workers (details available in Table 1).
Socio-demographic characteristics of the study samples.

Two people didn’t indicate the educational level between caregivers.
Measures
A standardized form collected the data on Age, Gender, Education, Civil, and Occupational Status.
The WWRR (Well-Being at Work and Respect for Human Rights questionnaire) was also fulfilled by each participant. The scale is inspired by the global World Health Organization initiative Quality Rights focusing implementation of the UN CRPD in the field of psychosocial disability, (https://www.who.int/mental_health/policy/quality_rights/en/).17–20 The questionnaire consists of six core items, which are reported in Table 2, a seventh item asks what type of health professionals the interviewee believe would be useful for the mental health service to have available in addition to those who already provide services (e.g. doctors, psychologists, occupational therapists, nurses, etc.)
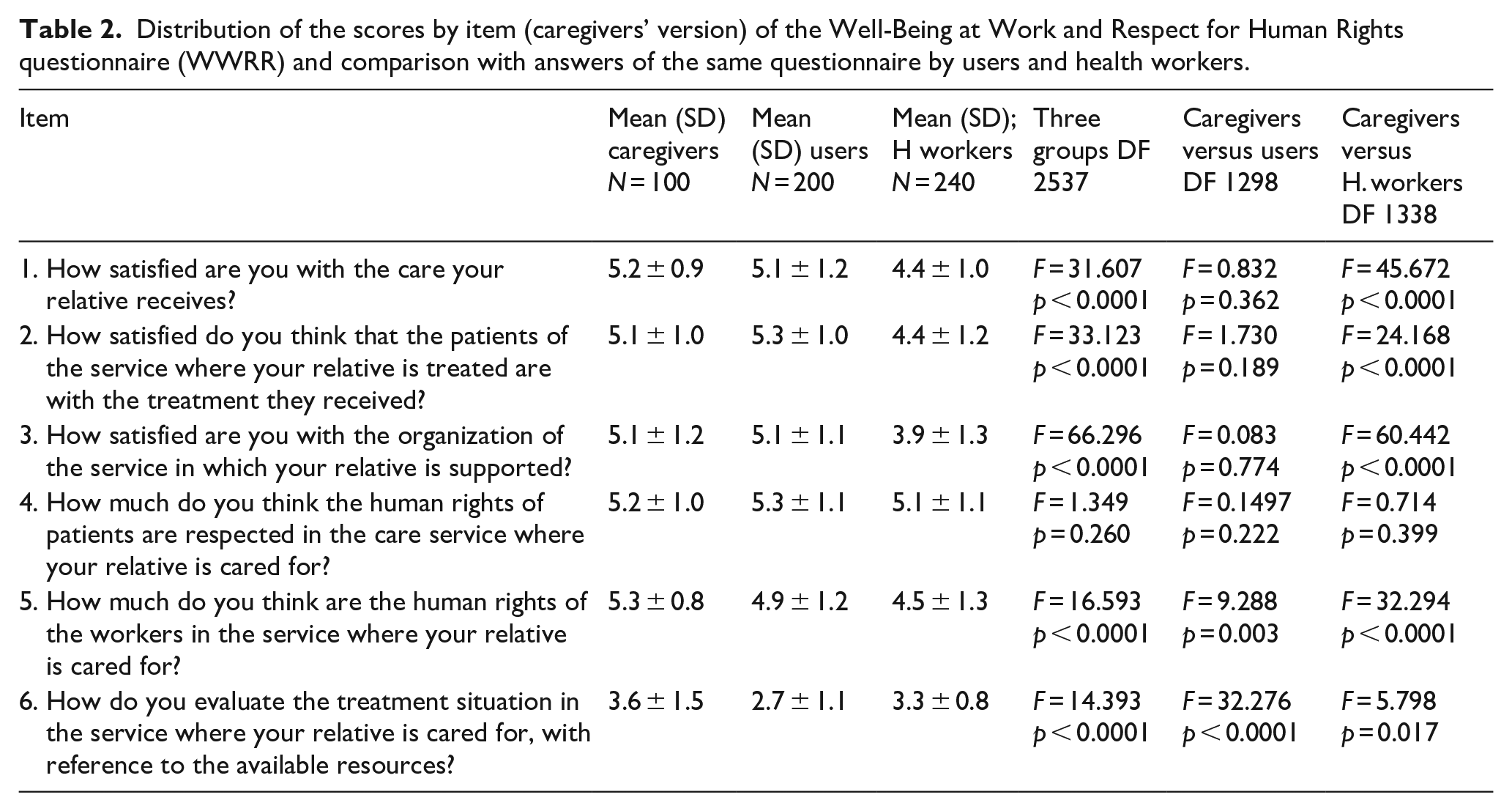
Distribution of the scores by item (caregivers’ version) of the Well-Being at Work and Respect for Human Rights questionnaire (WWRR) and comparison with answers of the same questionnaire by users and health workers.
Data analysis
The data were analyzed with the support of the Statistical Package for the Social Sciences (SPSS) version 29 (IBM Corp. Released 2021). All analyses were two-tailed, with significance set at p < 0.05. Nominal variables were shown as absolute numbers and percentages. Differences for groups for nominal variables were tested using chi square statistic. Continuous variables were presented using means and standard deviations. Differences for groups for continuous variables were tested using one-way ANOVA.
Ethics approval and consent to participate and to publication
The research was approved by the ethics committee of the Azienda Mista Ospedaliero Universitaria di Cagliari (Italy) with protocol number PG/2018/8822 and subsequent amendments. All participants provided written informed consent. All research procedures were conducted in agreement the 1975 Helsinki declaration and subsequent revisions.
Results
Table 1 shows the characteristics of sample of the caregivers in comparison with users and health worker ones. Compared to health workers, caregivers had fewer people who had obtained a degree (16% vs 53.7, Chi square = 41.126, p < 0.0001) and more people with <9 years of schooling (40% vs 11.7%, 35.417, p < 0.0001). In respect with users the caregivers are older (63% vs 35.5 with >49 years old, Chi square 30.399, p < 0.0001) and have a lower percentage of males (37% vs 60%, Chi square = 14.137, p < 0.0001).
Tables 2 and 3. Shows the distribution of the scores by item of the of the Well-Being at Work and Respect for Human Rights questionnaire (WWRR) and the comparison with answers of the same questionnaire by users and health workers. Note that the version for caregivers differs in item 1 (How satisfied are you with the care your relative receives?), in the version for health workers Item 1 investigates how satisfied the professional is with their job. Compared to users, caregivers have a higher score on item 5 (How much do you think are the human rights of workers in the service where your family member is cared for?) that is, 5.3 ± 0.8 versus 4.9 ± 1.2 (F = 9.288, p = 0.003) and item 6 (How do you evaluate the therapeutic situation in the service where your family member is assisted, with reference to the available resources?), which in this case has a reversed value, that is, the greater the lower the satisfaction score, that is, 3.6 ± 1.5 versus 2.7 ± 1.1 (F = 32.276, p < 0.0001). Compared to health workers, caregivers have a higher score on item 2 (How satisfied do you think that the patients, of the service where your relative is treated, with the treatment they received?) that is, 5.1 ± 1.0 versus 4.4 ± 1.2 (F = 24.168, p < 0.0001); item 3 (How satisfied are you with the organization of the service in which your relative is supported?), that is, 5.1 ± 1.2 versus 3.9 ± 1.3 ± (F = 60.442, p < 0.0001); Item 5 (How much do you think are the human rights of the workers in the service where your relative is cared for?) that is, 5.3 ± 0.8 versus 4.5 ± 1.3 (F = 32.294, p < 0.0001); Item 6 (How do you evaluate the treatment situation in the service where your relative is cared for, with reference to the available resources?), which in this case has a reversed value, that is, the greater the lower the satisfaction score, that is, 3.6 ± 1.5 versus 3.3 ± 0.8 (F = 32.276, F = 5.798, p = 0.017). A difference is also noted in item 1 that is, 5.2 ± 0.9 versus 4.4 ± 1.0 (F = 45.672, p < 0.0001) which however measures two different aspects, for caregivers’ satisfaction with the care the relative/friend receives, for health workers satisfaction with their job. Specifically, regarding the answer to question No. 7, although it was indicated to give only one answer, many caregivers decided to indicate multiple answers. In this way, both toward users and health workers, caregivers reported a greater number of professionals as necessary, specifically of nurses (20% vs 8.7% Health workers, Chi square = 8.424, p = 0.004 and 7.5 Users Chi square = 10.108, p = 0.001); Medical Doctors (48% vs 27.1% Health workers, Chi square = 13.818, p < 0.0001 and 13.5%Users, Chi square = 43.320, p < 0.0001); Psychologists (48% vs 26.4% Health workers, Chi square = 31.983, p < 0.0001 and 27.5% Users, Chi square = 23.230, p < 0.0001) and Social Workers (17% vs 2.9% Health workers, Chi square = 25.953, p < 0.0001 and 2.5% Users, Chi square = 6.319, p = 0.012).
Answer to the question “Needs for type of health workers in the service in which I work / I’m cared” (Item 7 WWRR).

Discussion
In our study comparing caregivers with users and health workers, the group of caregivers showed some differences relating to socio-demographic characteristics, but which are, very reasonably, the result of the difference in the reference populations. In fact, toward health workers, caregivers had fewer people who had obtained a degree and more people with less than 9 years of schooling. This is obvious because a degree is necessary to work as a doctor, nurse, psychologist, or professional educator. While as compared to the sample of users, the caregivers are older (many of them are the same parents as the users) and have a lower percentage of males. This result was also expected as European studies have underlined that women and specifically women of the family are more frequent among the closest caregivers, but only in “outside caregiving” were men and friends found in the network. 21
Caregivers show very high scores in relation to the care received from their friend and/or family member; the care received in general by all users of the mental health care services examined; the judgment on organizational well-being in the services themselves; toward the belief on respect of rights for health users and workers. In all these items there are no differences with the answers compared to the answers given by users except in relation to respect for the rights of health professionals where caregivers express higher scores (i.e. they are convinced that the rights of health workers are well respected), On the contrary, toward health workers all scores are higher except for the item of respect for users’ rights where there are no statistically significant differences. It should be noted, however, that although health workers express lower scores on average than caregivers and as has already been demonstrated also toward users, the opinions of health workers are positive, the lowest score is obtained on answer about satisfaction with the organization of health services where the average of scores is over 65% of the score. In general, the score of health professional were found higher than those of health professionals of all the countries in which similar research was conducted,11,12 the scores were even higher than those of health workers in non-mental health services in Italy. 14 Only in the item on satisfaction with the resources available in care services do the caregivers’ responses express less satisfaction with both the staff and the users, expressing strong dissatisfaction overall (responses at 40% of maximum satisfaction) in an item in which however, the responses of users and health workers also express a low level of satisfaction. The response profile of caregivers expresses, accentuating the trend, the same profile shown by users and health professionals, that is, a persistent general satisfaction with a care system that is still been able, thanks to its roots in the territory and its detachment from hospital medicine, to respond well to the needs of the population and users, particularly in the Covid-19 era. But, at the same time, a growing alarm about the loss of resources which is generally a problem of the Italian healthcare system, which is even more accentuated in terms of mental health.
The study, although it shows a positive point of view of informal caregivers about satisfaction on care and respect of human rights, seems identified a critical turned point in the history of Italian community mental health care. 22 The mental health care system in Italy even providing care of a good perceived level of quality (from the point of view of the caregivers, users, and even mental health workers), due the radical community centered model (psychiatric hospitals are closed).23,24 Nevertheless, the public health care system in Italy suffers by a progressively decreasing in public health expenditure from 2008. 25 The expenditure for health in 2017 in Italy was 15% below the per capita expenditure of the average of the European Union, while the Italian per capita income was like the European Union average per capita income. 25 But the general decrease in health spending affects mental health to a greater extent, if we consider that the percentage for mental health of the spending for health in Italy is only around 3%, while in the rest of Europe is around 10% of the total expenditure for health. In conclusion, Italy is spending a much smaller portion of its total expenditure on mental health, which is already lower than in the rest of the other countries. 22 This consideration well explained, taking in account an objective point of view, the dissonance found in health workers and users and, which higher extent, in caregivers, between the high scores in satisfaction for care and respect for human rights in mental health care services and the low scores on satisfaction for resources in the same services. It unlikely that this good satisfaction level can be maintained if spending cuts persists.
Caregivers’ strong alarm about spending cuts is reflected in responses about beliefs on staffing needed in mental health services. In fact, although a single response was required (i.e. that the most necessary professional figure in mental health services be indicated), many caregivers responded by indicating multiple figures, thus expressing their concern regarding the recent cuts and the lack of turnover for people who they have gradually retired in recent years. 26
The results of this study are quite in consistency of the results of other studies in Italy27,28 and it can support the hypothesis of the generalizability of these regional results to the overall Italian territory and of the Italian model, which, is unique in its radical community organization. Due to the limitation of this survey, future more extended studies will have to confirm the hypothesis that a model of mental health care strongly centered on community care can respect users and health workers rights and works with satisfaction of caregivers, users and health workers even in the conditions of over-stress especially in a critical period as due to the pandemic.
However, there remains a strong doubt whether the good results can continue in the future if the cuts in healthcare spending and, in particular, spending on mental health are not stopped.
Limitations
The objective limitations of this survey deals with the non-probabilistic sample conducted without randomization, and to have been carried out in only one region of the country. However, the survey can be a starting point for multicenter, trans-regional and transnational research conducted on representative samples. Additionally, an assessment of what might be a protective factor such as psychotherapy and counseling intervention, which people often use without prescription to prevent or alleviate distress, was not conducted. This avenue for future research could provide valuable insights into improving mental health care strategies.
Significance for public health
By considering caregivers’ perspectives alongside users and health workers, this study provides insights into care dynamics and organizational well-being in mental health settings. Caregivers, play a pivotal role in the care process. Their perceptions reflect high satisfaction with care quality and human rights respect but also concerns over diminishing resources and staffing shortages. This underscore systemic challenges facing the Italian mental health care system, which has experienced a progressive decrease in public health expenditure for the mental health sector. Moreover, the findings suggest that the unique community-centered model of mental health care in Italy emphasizes the importance of maintaining adequate funding to sustain its success amidst ongoing challenges. Continued research in this area is essential to validate these findings and inform policy decisions for safeguarding mental health stakeholders’ rights and well-being.
Footnotes
Acknowledgements
MA performed her activity in the framework of the PhD in Innovation Sciences and Technologies at the University of Cagliari, Italy.
Availability of data and materials
The data base is available if request after consensus of the ethical committee of reference
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project benefit of the project “QualityRights” funded by the call “Legge regionale 19 dicembre 2023, n. 17. Finanziamento anno 2023.”
Consent for publication
Written informed consent was obtained from each participant prior to the study.
Human and animal rights
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki declaration of 1975 and subsequent revisions and amendments.