
Abstract
Dissemination and implementation science (D&I) can help bridge the gap between research and practice by addressing how to facilitate and maintain pre-existing evidence-based interventions (EBIs) in various contexts within different fields, including that of breast cancer screening and treatment. Yet, despite the availability of D&I frameworks and strategies, there is a lack of studies exploring knowledge transfer dissemination and implementation models, strategies, and frameworks in the setting of breast cancer care. There is a need for studies that create guidelines and roadmaps built on theoretical foundations of D&I research to scale up successful D&I of strategies, frameworks, and protocols proven to cater to the needs of all breast cancer patients when seeking screening and treatment services. The Arksey and O’Malley (2005) York methodology was used as guidance for this review: (1) identifying research questions; (2) searching for relevant studies; (3) selecting studies relevant to the research questions; (4) charting the data; (5) collating, summarizing, and reporting results. Most cited barriers (n = 46) sorted into the category of “Recruitment, Measurement, and Delivery Challenges.” The predominant ERIC strategy, featured in a noteworthy 84% of studies, was “Tailor strategies” (#16), which belongs to the “Adapt and tailor to context: culture, language, data analysis, collection” domain. This study can guide researchers, physicians, and community workers in improving accessibility, affordability, and quality of breast cancer screening and adequate follow-up opportunities through D&I strategies and models improving the reach and sustainability of evidence-based programs in at-risk female populations.
Significance for public health
Dissemination and implementation science (D&I) can help bridge the gap between research and practice by addressing how to facilitate and maintain pre-existing evidence-based interventions (EBIs) in various contexts, including that of breast cancer screening. Currently, there is a lack of research exploring D&I strategies and frameworks are lacking for breast cancer screening in the setting of breast cancer care. There is a need for studies that create guidelines and roadmaps to scale up successful D&I of strategies, frameworks, and protocols proven to cater to the needs of all breast cancer patients when seeking screening and treatment services. The purpose of this scoping review was to identify common barriers and effective mitigating D&I models and strategies to successfully disseminate and implement evidence-based breast cancer screening and treatment programs for at-risk U.S. women aged ≥40 years. Most cited D&I barriers sorted into the category of “Recruitment, Measurement, and Delivery Challenges.” Most cited ERIC strategy was #16 “Tailor strategies,” with the primary reason being perceived relevance of screening. Lessons learned from barriers and challenges to the successful D&I of evidence-based breast cancer screening and treatment programs and/or protocols were also highlighted. This paper will contribute to informing and guiding future D&I initiatives aimed at reducing breast cancer health disparities in this population.
Background
In the United States, approximately one in eight women are estimated to develop invasive breast cancer during their lifetime, and 3% of women will die from the disease. 1 In fact, in 2022, the most common cancer amongst women in the US was breast cancer, with the estimated prevalence set at four million women across the country. 2 With such a high prevalence of breast cancer, the importance and value of mammograms in early detection has been emphasized and the benefits of early screening are well-publicized. 3 Despite screening awareness efforts, nearly one-third of women aged 40 and above in the US reported having no recent mammogram. 4 A report of a recent mammogram was more common among women aged 50–79, married women, women with higher educational attainment or income, and those with health insurance and a regular source of recent health care. 5 Accessibility to mammograms was a main barrier hindering annual adherence to screening.5–7 Studies have shown that a lack of an adequate number of X-ray machines can create longer screening appointment wait times. 5 Increased wait times have been noted as a barrier with not only screening but cancer treatment as well, resulting in treatment delays. 6 Another access-related barrier includes a shortage of staff, particularly radiologists, and technologists. 7
Women also face barriers to breast cancer screening beyond the facility.8,9 A recent study found that transportation and a lack of paid time off were the most significant barriers overall to seeking a mammography amongst women aged 40 and above, regardless of whether their care was at an inner-city safety or a suburban county one. 8 Lack of childcare services was also a prominent barrier across income quartiles and, for women specifically at the inner-city safety net hospital, fear of the procedure and/or the results understanding was noted as the most prohibitive barrier to abnormal screening work-up. 8 Findings remained disparate across city versus county patients, highlighting the place of residence as a possible contributor to health care access and, in turn, ultimately to breast cancer screening and treatment. 8
In oncology, especially, there is a general trend of emphasizing treatment over prevention. 10 Yet, more than half of cancers today are preventable by pre-existing knowledge, emphasizing the need for improved methods of dissemination and implementation of this information. 10 This knowledge base includes recommendations such as increasing physical activity, consuming a healthier diet, and limiting alcohol consumption, but many of these concepts are embedded within contextual issues such as policy, food insecurity, and structural inequities that recommendations often do not address with enough specificity. 11 The National Comprehensive Cancer Network and the Breast Health Global Initiative have even developed resource-stratified, evidence-based guidelines for breast cancer control and management; however, the publication of such recommendations does not translate to their use and to meeting breast cancer control needs. 12 Dissemination and implementation science (D&I) can help bridge this gap between research and practice by addressing how to facilitate and maintain pre-existing evidence-based interventions (EBIs) in various contexts within different fields, including that of breast cancer screening and treatment. 13
D&I science is the scientific study of methods, frameworks, and strategies that promote the uptake and application of evidence-based practices and interventions into real-world contexts to prevent disease and improve the quality and efficacy of services in healthcare. 12 As this field grows, studies have begun using D&I frameworks to examine the implementation of different breast cancer EBIs, such as the Peace of Mind Program (PMP)—an EBI to increase mammography appointment attendance.13,14 Another study used the Dynamic Adaptation Process (DAP) and Exploration, Preparation, Implementation, Sustainment (EPIS) frameworks to assess the implementation and application of Project ADAPT, an adaptation of the Ending Metastatic Breast Cancer for Everyone (EMBRACE) program, to the St. Louis region. 15 Despite the utility and availability of such frameworks, limitations of their application remain, along with concerns regarding strategies and frameworks themselves, including inconsistency with terminology and lack of sufficient detail for real-world replication.14–16
To address these limitations, groups of strategies have been clarified and created to help facilitate the adoption, use, and eventual sustainability of EBIs. One such taxonomy consists of the Expert Recommendations for Implementing Change (ERIC). 16 ERIC is a compilation of 73 implementation strategies organized into nine thematic clusters that cover areas including but not limited to financial strategies, infrastructure changes, developing stakeholder relationships, and consumer engagement.17,18 As these strategies continue to be studied and adapted to achieve their maximal value, they already demonstrate their utility in two key features: (1) they provide conceptual clarity and consensus among implementation strategies and terminology and (2) they use recommendations from multiple stakeholders to develop implementation strategies that are context-sensitive. 19 Yet, despite the availability of these strategies, there is a lack of studies exploring knowledge transfer dissemination and implementation models, strategies, and frameworks in the setting of breast cancer care.20,21 There is a need for studies that create guidelines and roadmaps built on theoretical foundations of D&I research to scale up successful D&I of strategies, frameworks, and protocols proven to cater to the needs of all breast cancer patients when seeking screening and treatment services. 12
The purpose of this scoping review was to identify common barriers and effective mitigating D&I models and strategies to successfully disseminate and implement evidence-based breast cancer screening and treatment programs for at-risk U.S. women aged ≥40 years. It will also explore lessons learned from barriers and challenges to the successful D&I of evidence-based breast cancer screening and treatment programs and/or protocols. This paper may further contribute to informing and guiding future D&I initiatives aimed at reducing breast cancer health disparities in this population.
Methods
The PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping reviews) was used as a reference checklist for this review. 22 This scoping review was guided by Arksey and O’Malley’s (2005) York Methodology. 23 This framework methodology is composed of five steps: (1) identify research questions; (2) search for relevant studies); (3) select studies relevant to the research questions; (4) chart the data; and (5) collate, summarize, and report results.
Step 1: Identify research questions
Four guiding research questions for this scoping review were: (1) Which theories, models, and/or frameworks have been used to promote the dissemination and implementation of breast cancer screening and prevention evidence-based programs for at-risk U.S. women aged ≥40?; (2) What are the main barriers encountered in the D&I of breast cancer screening and prevention evidence-based programs for at-risk U.S. women aged ≥40?; (3) What implementation strategies have been used for evidence-based breast cancer screening and prevention program and intervention adoption, implementation and/or maintenance in at-risk U.S. women aged ≥40?; (4) What are the major limitations encountered when establishing sufficient follow-up opportunities for U.S. women aged ≥40 who are at-risk of or have developed breast cancer?
Step 2: Search for relevant studies
Acronyms were developed (Supplementary File 1) with the involvement of a research librarian (MK) who has expertise in writing scoping reviews and developing the protocol relevant for this study. Search terms included: dissemination science; implementation science; frameworks; strategies; theoretical frameworks; health promotion theories; breast cancer; mammography; screening/prevention; follow-up; doctor visits; women/female; United States. The review of the literature was completed over a period of 4 months, beginning in January 2023 and ending in April 2023. Screening of the articles was carried out by the senior author (LS) and co-authors (MR, SB, YZ, AM, SD, GO, DL, VJ).
Inclusion criteria
Included were peer-reviewed studies, published in English between 2000 and 2020 that (1) described the use of D&I models, frameworks, and theories to increase the dissemination, implementation, or maintenance of evidence-based or evidence-informed breast cancer screening and prevention programs, (2) were conducted in the U.S., and (3) addressed women aged ≥40 years.
Exclusion criteria
Excluded were studies that targeted women outside the age range (not ≥40 years of age) or not located in the U.S., studies focusing solely on improved behavioral or health outcomes with no reference to the D&I field, and studies that only reported general recruitment strategies, or that focused solely on ethical issues related to the implementation of these programs. Narrative, scoping, and systematic reviews were excluded as well.
Step 3: Selection of studies for the research questions
The senior author (LS) reviewed all tabulated data to resolve any discrepancies. All co-authors (MR, SB, YZ, AM, SD, GO, DL, VJ) extracted and summarized data. Summary tables included 1 evidence table describing characteristics (Table 1). Table 2 included a list of barriers that were first classified based on the Socio-Ecological Model and then further stratified based on emerging barrier themes that were common across studies retained for analysis. D&J models were identified using the ‘Dissemination and Implementation Models in Health Research and Practice Webtool’. Table 3 consisted of the D&I strategies that were categorized and coded based on ERIC strategies. These strategies both help to clarify concepts and provide consensus on implementation strategies and terminology, as well as to develop context-sensitive implementation strategies using stakeholder recommendations. 19
Study characteristics.

Dissemination and implementation barriers classified based on the socio-ecological model and barrier category themes.

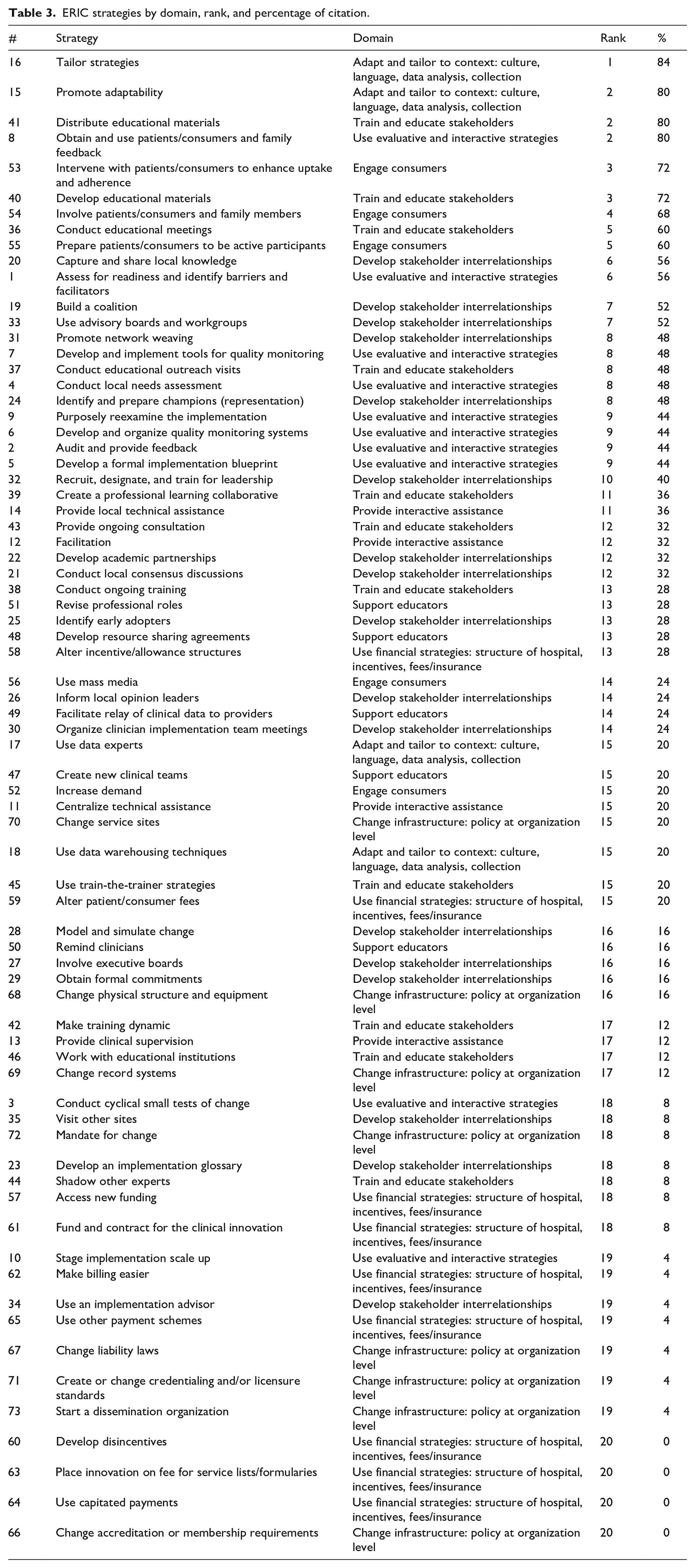
ERIC strategies by domain, rank, and percentage of citation.
Step 4 and 5: Data charting and collation, summarization, and reporting of results
Study characteristics were tabulated for primary author/year, study design, sample size, priority population, study purpose, setting, stakeholders, D&I theory/framework (Table 1). Twelve barrier theme categories were identified based on recurrence across studies (Table 2). D&I strategies were matched with the ERIC strategies and ranked by frequency of occurrence, as well as ranked by most cited strategies within each domain (Table 3).
Results
The initial study extraction resulted in 886 articles from PubMed (n = 281), EMBASE (n = 538), Web of Science (n = 50), and Cochrane (n = 17) (Figure 1). Studies were excluded due to targeting women outside the age range (n = 222), not being located in the U.S. (n = 213), focusing solely on improved behavioral or health outcomes with no reference to the D&I field (n = 188), only reporting general recruitment strategies or focusing solely on ethical issues related to the implementation of these programs (n = 167), or for being narrative, scoping, or systematic reviews (n = 11). Duplicate studies were removed (n = 25 from PubMed; n = 16 from EMBASE, n = 7 from Web of Science, and n = 2 from Cochrane). Sixty studies met the inclusion criteria from PubMed (n = 34), EMBASE (n = 22), and Web of Science (n = 4). An additional 35 studies were excluded after completing a full study review due to (1) being abstracts only and not full text (n = 27) and (2) having no relation to D&I (n = 8). A total of 25 eligible studies were retained for analysis.

Flow selection of the study process.
The 25 retained studies were published between 2002 and 2022 (Table 1). About one-third of studies (8/25, 32%) were published in 2018 or later (n = 8). Study designs included qualitative studies (n = 6); quasi-experimental studies (n = 3); randomized control trial studies (n = 7); descriptive studies (n = 3); mixed-methods studies (n = 3); case study (n = 1); cross-sectional study (n = 1); and repeated measures survey methodology (n = 1). Sample size ranged from n = 1 patient navigator in an urban underserved community to n = 1974 un- and under-insured racially and ethnically diverse urban women. Studies for this review occurred in various settings including health and medical centers (n = 9); state and national registries (n = 7); primary care practices, FQHCs, and community clinics (n = 4); religious settings and community centers (n = 3); virtual via Zoom (n = 1); and national foundations (n = 1).
Priority populations and key stakeholders
Priority adult female populations included women from diverse racial and ethnic backgrounds residing in rural and/or underserved communities experiencing accessibility, affordability, and quality issues when it comes to breast cancer screening. Key stakeholders included patients, investigators, research teams, medical centers, medical staff, and providers (Table 1).
D&I models
D&I models included the Consolidated framework for implementation research (n = 2); Ajzen’s Theory of Planned Behavior (n = 1); Health Belief Model (n = 1); Health Disparities Framework by Warneke et al. (n = 1); CDC Social Ecological Model of Health Promotion (n = 1); Precede-Proceed Model (n = 1) (Table 1).
D&I barriers
One hundred and eighty four barriers to implementation were reported in 25 studies,24–49 representing the five levels of the socio-ecological model (SEM): individual (n = 68), interpersonal (n = 27), organizational (n = 61), community (n = 19), and society/policy (n = 8) (Table 2). Barriers were also sorted into 12 categories (Table 2) based on major themes that were established through similarity of barriers highlighted across studies at the various levels of SEM. Some barriers fit into the SEM levels, and thus generated more than one theme. Most cited barriers (n = 46) sorted into the category of “Recruitment, Measurement, and Delivery Challenges.” A majority of studies also cited “Limited Healthcare Accessibility, Affordability, and Quality” (n = 26), “Misconceptions and Negative Assumptions about Breast Cancer Screening” (n = 21); “Generalizability” (n = 15), and “Structural and Regulatory Challenges in Healthcare Settings” (n = 14). Other barrier categories included Funding and Reimbursement Challenges (n = 7); Lack of Integration with Cultural and Religious Values (n = 11); Lack of Adequate Knowledge about Patient Suitability for Breast Cancer Screening (n = 9); Social Norms and Family Related Issues (n = 9); Communication and Health Literacy Challenges (n = 8); Geographic and Transportation Challenges (n = 7) and Distrust (n = 5) (Table 2).
Breast cancer screening & treatment implementation strategies
All ERIC domains (n = 9) were represented, and all extracted D&I strategies were matched to relevant ERIC strategies (Table 3). However, not all ERIC strategies were represented in the included studies. Two hundred and forty-three D&I strategies (n = 243) were identified, corresponding to 69 (95%) of the ERIC strategies. The remaining 5% of ERIC strategies (n = 4) that lacked representation were as follows: “Develop disincentives” (#60), “Place innovation on fee for service lists/formularies” (#63), “Use capitated payments” (#64), and “Change accreditation or membership requirements” (#66). Each study revealed a diverse range of one to sixteen strategies. The predominant ERIC strategy, featured in a noteworthy 84% of studies, was “Tailor strategies” (#16), which belongs to the “Adapt and tailor to context: culture, language, data analysis, collection” domain. The next top five ERIC strategies reported were “Promote adaptability” (#15), “Distribute educational materials” (#41), “Obtain and use patients/consumers and family feedback” (#8), “Intervene with patients/consumers to enhance uptake and adherence” (#53), and “Develop educational materials” (#40).24–49
Discussion
This scoping review identified major barriers hindering the effective dissemination and implementation of evidence-based breast cancer screening and treatment programs for at-risk U.S. women aged ≥40 years. Lessons learned from included studies can guide future successful D&I initiatives to improve adherence to breast cancer screening guidelines and recommended treatment plan in the U.S.24–49
D&I models
Seven of the twenty-five studies (28%) included in the scoping review utilized D&I models to address health disparities. One such model, the Consolidated Framework for Implementation Research (CFIR), attempts to provide a foundation on which research findings may be applied by utilizing an array of 39 constructs proven to impact implementation. 50 CFIR allows for the prediction of barriers or other factors to further guide strategies for successful implementation. This strategy is especially useful in designing interventions for underserved women with regard to cancer prevention, sexual health, and other chronic diseases. Another study utilized the CDC Socio-Ecological Model, a four-level model including the individual, their relationships, their community, and their society. 51 It acts as a holistic framework in understanding multi-level underlying factors hindering screening and treatment among women with breast cancer. With this said, these models are not without their limitations. CFIR and the CDC Socio-Ecological model both struggle in their inability to distinguish between the respective importance of constructs or factors. 52 Yet, these models’ ability to illuminate barriers and influence implementation outweigh the posed limitations. With additional research, these models may be adapted to facilitate a more inclusive consideration of the weight assigned to respective constructs.50,52 Overall, D&I models provide guidance in designing evidence-based interventions with a systematic approach to addressing health issues and their routine adoption can dramatically improve health outcomes.50,52,53
Identified D&I barriers
The barriers most frequently cited were under the individual (n = 68) and organizational (n = 61) levels of the socio-ecological model (SEM). Individual barriers to breast cancer screening include fears, beliefs, education, geographical accessibility, transportation, and insurance coverage. A study by Khazaee-Pool et al. 54 highlighted how deep-seated beliefs can undermine evidence-based interventions. The qualitative study included Iranian women aged ≥30 years without mammography history and limited breast cancer knowledge. This cohort attributed the emergence of breast cancer to mammography itself, a perception that hindered their willingness to undergo the procedure. 54 Another challenge that individuals face is overcoming geographical and financial barriers to healthcare access. On a geographic level, when primary care clinics and medical practitioners are not readily within reach, breast cancer screening, diagnosis, and treatment become difficult. This disproportionately affects underserved communities, as geographic disparities forces women to undertake arduous journeys to access critical services. 55 Parallel to issues of accessibility is the constraint imposed by health insurance coverage and associated costs. A recent study by Mootz et al. 56 revealed socioeconomic and insurance-related disparities in cancer outcomes, with those lacking insurance or with inadequate coverage experiencing graver outcomes. 56
On an organizational level, barriers include health literacy issues within clinics, limited number of hospitals offering translation services, a shortage of physicians, and inadequate time to engage with patients for a thorough understanding of their needs. 57 Women with low health literacy are associated with a lower probability of mammography screening; they are also more likely to report poorer physician-patient communication and higher levels of decision regret regarding their breast cancer decisions. 57 Moreover, substantial disparities in the time taken for diagnostic follow-up of abnormal mammograms have been identified in facilities catering to larger proportions of non-English speaking patients, where the delays were observed to be the most prolonged. 58 A study by Beauchamp et al. 59 utilized two randomized control trials to demonstrate that the implementation of an intervention strategy, which involved utilizing translated mammography reminder letters and conducting in-language phone calls, led to notable improvements in mammography screening rates. 59 Physician scarcity has also reduced access to breast cancer care, including screening, diagnosis, and treatment. 60 Another constraint is the limited time available for physician-patient interactions. Clinicians often neglect to inquire about their patient’s concerns, significantly reducing the chance of addressing individual priorities during clinical encounters. 61
The most frequently cited category was Recruitment, Measurement, and Delivery Challenges (n = 46). Barriers in this category include issues like “Limited data about non-Caucasian participants,” 38 “Particularities in the sample, e.g., English-speaking, mosque-going women,” 41 and “Outcome based on self-reports; future study should verify with medical records.” 31 These barriers significantly impact both study quality and data collection, making it more difficult to assess associations and restricting the scope of assumptions. Similar challenges were faced in a study conducted by Brown et al. 62 when exploring barriers to cervical cancer screenings. The study’s online format skewed recruitment towards younger adults with higher educational attainment, a group associated with higher screening rates. 12 Additionally, the assessment of screening behavior was done retrospectively via self-reports rather than validation through cervical screening registries, potentially leading to an underestimation of the count of women overdue for screening in comparison to registry data. 12 The next most cited barrier theme was Limited Healthcare Accessibility, Affordability, and Quality (n = 26). This category encompassed obstacles like “Cost of mammography services,” 26 “Lack of insurance and cost of healthcare,” 24 and “Lack of primary care provider.” 24 The third most common barrier theme was Misconceptions and Negative Assumptions about Breast Cancer (n = 21). Some barriers included in this theme are “Fear of finding cancer” 27 and “Mammograms are uncomfortable or painful.” 25 These barriers are exacerbated by the Lack of Integration with Cultural and Religious Values (n = 11) 31 and the Lack of Adequate Knowledge about Patient Suitability for Breast Cancer Screening (n = 9). 30 Finally, generalizability (n = 15) emerged as an additional barrier influencing the quality of evidence within the studies. Small sample sizes impact both internal and external validity. Internally, they can introduce sampling bias and reduce statistical power, potentially leading to inaccurate or non-significant results. 63 Externally, the generalizability of findings becomes limited due to inadequate representation of diverse characteristics within the target population. This can hinder the applicability of study results to different settings, groups, or contexts. 63 This constraint in generalizability becomes evident in the context of breast cancer screening, as reflected in the USPSTF’s recommendations for women at average risk. 64 These recommendations, primarily derived from studies involving non-Hispanic (NH) White women, raise inquiries about their relevance to ethnically and racially diverse groups. 64
ERIC-adapted D&I strategies
Our review found that the most cited ERIC strategy was #16 “Tailor strategies” (84% of studies). The primary reason that tailoring strategies are important for breast cancer prevention is perceived relevance. 65 Messages about health promotion that are tailored to a group such that they address the unique needs of individuals tend to have higher perceived personal relevance of risks and use of interventions, in turn increasing the likelihood of behavioral changes such as getting screened for breast cancer. 66 By tailoring strategies, researchers can also address the lack of integration with cultural and religious values, a barrier noted in several studies reviewed by this paper (n = 11). For example, for ethnic minority women such as Afghan women, who comprise the largest refugee population in the world, targeting three levels—Person, Extended Family, and Neighborhood—is important as these women are part of a collectivist culture. 67 Building off these levels, researchers developed interventions such as “tea parties” with groups of women to reduce social isolation and integrated the interventions with Islamic constructs for religious relevance. 67 Male family members, with the permission of the women, were invited for educational sessions to help promote them from gatekeepers of women’s breast health to advocates. 67 Similarly, strategies to increase breast cancer screening amongst African American women targeted “black radio” (radio stations targeting African American audiences), and church-based interventions given the church’s role as a vital institution culturally, religiously, and socially, amongst African American populations at all levels of vulnerability. 66
The next top five strategies noted in our review were #15 “Promote adaptability” (80% of studies), #41 “Distribute educational materials” (80% of studies), #8 “Obtain and use patients/consumers and family feedback” (80% of studies), #53 “Intervene with patients/consumers to enhance uptake and adherence” (72% of studies), and #40 “Develop educational materials” (72% of studies). A patient navigation program in Chicago’s Chinatown emphasized the value of promoting adaptability, illustrating that tailoring strategies to cultural needs were important, but more important was ensuring that it was a constantly iterative process. 68 Researchers used feedback to make adaptations, like increasing the intensity of work related to health insurance, during the implementation process. 68 This was much like the Helping Her Live model, also located in Chicago, which consistently sought feedback from Community Health Workers to manage its navigation protocol. 69 Highlighting the value of developing educational materials is the “Cancer Cooking School,” developed by The Georgia Breast and Cervical Cancer Cancer Program in partnership with organizations like the American Cancer Society. 70 Researchers found that this publicly accessible, 3-h class on healthy dietary guidelines and healthier life choices like smoking cessation led to 80 women being screened for breast cancer out of the 125 eligible attendees, and 40 of these women had not been screened in the prior 5 years, if ever. 70
Not only is the development of educational materials important, but so is the distribution of these materials as reported by the Ohio Breast and Cervical Cancer Project, which saw a 32% increase in screening enrollment following a mass media campaign consisting of television commercials, radio ads, and print ads. 70 This percentage went up to 40% when a live information session was added in, illustrating the importance of the method by which materials are distributed as well. 70 While tailored educational materials, including but not limited to interactive education sessions and printed brochures, have been developed for Korean American women, studies have found that these interventions have had limited impact on increasing breast cancer screening uptake in this population as they are hard to reach. 71 In turn, this has emphasized the importance of appropriate delivery of information and has prompted considerations for new delivery methods like mobile health navigation apps. 71
Regarding intervening with patients to improve adherence, a systematic review of patient-provider communication on screening adherence found that patient-provider interaction was important and significantly more effective at increasing uptake when factoring in nuances of these interactions. 72 Findings illustrated that patient perception of provider encouragement and enthusiasm was one of the strongest indicators of screening adherence. 72 Also important to such interventions is the use of patient feedback. This can be done through shared decision-making (SDM), where patients and clinicians work together to jointly make informed healthcare decisions. 73 The importance of using feedback extends beyond just these patient-provider interactions, with studies illustrating that patient feedback can fill gaps at a policy level on how to even define SDM and what core elements should be involved in national SDM guidelines and recommendations. 74
Strengths and limitations
Although this study is of high value for public health, medical, and community health experts through the identification of common barriers and effective mitigating D&I strategies for breast cancer screening programs for at-risk U.S. women, several limitations need to be taken into consideration. First, this study did not include case reports, case studies, and literature reviews from the grey literature. It also did not encompass tracing of the reference lists from included studies. However, a comprehensive search of the literature in relevant psychosocial databases was carried out and involved an initial, secondary, and tertiary screening led by the senior author and the co-authors. Second, the evaluation of the quality of the evidence as part of this scoping review was integrated as part of the barriers identified in the different studies including generalizability, and recruitment, measurement, and delivery challenges. A theoretical approach (SEM) rather than an analytical approach was used to assess the quality of the associations made, the methodology adopted, and the findings shared. Future systematic reviews are recommended to ensure an analytical evaluation of the evidence shared to account for limitations of the study designs and their impact on relevant outcomes. Third, matching the extracted D&I strategies to the ERIC strategies was a challenge due to the diversity of the terminology used to describe dissemination and implementation strategies adopted for breast cancer screening and adequate follow-up. It would be critical for experts in the field of dissemination and implementation science to work on a standardized methodology encompassing specific nomenclatures to address diverse types of chronic diseases.
Conclusion
This scoping review describes D&I barriers and strategies to the effective delivery of evidence-based breast cancer screening programs and adequate follow-up for at-risk U.S. women aged ≥40 years. The existing diversity in the cultural backgrounds, beliefs, and values of patients calls for a more culturally competent approach for future breast cancer screening D&I initiatives. This study can guide researchers, physicians, and community workers in improving accessibility, affordability, and quality of breast cancer screening and adequate follow-up opportunities through D&I strategies and models improving the reach and sustainability of evidence-based programs in at-risk female populations.
Supplemental Material
sj-docx-1-phj-10.1177_22799036241268841 – Supplemental material for Dissemination and implementation science frameworks and strategies to increase breast cancer screening for at-risk women in the United States: A scoping review
Supplemental material, sj-docx-1-phj-10.1177_22799036241268841 for Dissemination and implementation science frameworks and strategies to increase breast cancer screening for at-risk women in the United States: A scoping review by Meera Rao, Sebastian Densley, Adeife Marciniak, Sara Burgoa, Yasmine Zerrouki, Goodness Okwaraji, Diana Lobaina, Vama Jhumkhawala, Michelle Knecht, Panagiota Kitsantas and Lea Sacca in Journal of Public Health Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.