
Abstract
Background:
During the mumps outbreak in Japan in 2016, 159,031 cases were reported. In a survey conducted in 2015, mumps vaccination rates for the first dose were 30%–40%. However, the rates for two or more doses were not determined. We assessed the mumps vaccination rates and mumps infection prevalence according to vaccine doses received.
Design and methods:
This was a multicenter cross-sectional study. Students from three universities participated in 2019. Informed consent was obtained from the students and their guardians. The primary outcome was the prevalence of breakthrough mumps infection according to the number of doses of vaccine received. We collected data on past illnesses of vaccine-preventable diseases and vaccination history using a questionnaire, photocopies of the Maternal and Child Health Handbook from the guardians, and virus antibody titers from the universities’ health centers.
Results:
This study assessed 2004 eligible students and included 593 (29.6%); of these, 250 (42.7%) had a mumps infection history. Furthermore, 264 (44.6%), 31 (5.2%), and 2 (0.3%) students received the first, second, and third doses of mumps vaccine, respectively. The mumps seropositivity prevalence was 43.2% (n = 127), 36.7% (n = 97), 26.7% (n = 8), and 100% (n = 2) for the no-, first-, second-, and third-dose groups, respectively (p for trend = 0.09). The mumps infection prevalence rates were 69.8% (n = 203), 11.3% (n = 28), 3.9% (n = 1), and 0% for the no-, first-, second-, and third-dose groups, respectively.
Conclusions:
Approximately 1 in 10 students who had received only one dose of mumps-containing vaccine had a breakthrough infection history.
Significance for public health
During the mumps outbreak in Japan in 2016, 159,031 people were infected, whereas in the United States, where multiple mumps vaccinations are routinely administered, only 6369 people were infected in the same year. Therefore, it is important to routinely administer mumps vaccines to prevent complications from its infection. However, to the best of our knowledge, no nationwide survey exists on rates of second and more doses of mumps vaccination. We assessed the mumps vaccination rate and mumps infection prevalence by a number of doses of vaccine received among university students using reminder records on mumps infection, vaccination records, and antibody measurements. Mumps vaccine coverage among university students in Japan remains considerably below the level required for herd immunity. A low mumps vaccination rate and high mumps infection prevalence was found. Furthermore, 1 in 10 students who had received 1 dose of vaccine had a breakthrough mumps infection.
Introduction
During the mumps outbreak in Japan in 2016, 159,031 people were infected, 1 whereas in the United States, where multiple mumps vaccinations are routinely administered, only 6369 people were infected in the same year. 1 Therefore, it is important to routinely administer mumps vaccines to prevent complications from its infection. Herd immunity, which can be achieved when 85%–90% of the population is immunized by the mumps vaccine, is required to suppress mumps outbreaks. 2 In Japan, the mumps-containing vaccine was discontinued in the routine vaccination program in 1993 owing to an unexpectedly high prevalence of aseptic meningitis as an adverse effect of the vaccine. Since then, the mumps vaccine has been provided voluntarily. 3 Centers for Disease Control and Prevention recommends a two-dose strategy in measles, mumps, and rubella (MMR) vaccinations. 4 This is because those who had received only one dose of MMR vaccine continued to develop infections that resulted in many outbreaks of measles in colleges and schools in the 1980s. 5 In a previous study, we surveyed mumps vaccination status among medical university students at a single center in 2008 and 2009 and reported that only 58% (552 students) received the mumps vaccine. 6 University and college students are prone to infectious disease outbreaks due to their high levels of activity. Therefore, we focused this survey on university students. In a Japanese survey conducted in 2015, the mumps vaccination rate for the first dose was only 30%–40%. 7 However, to the best of our knowledge, no nationwide survey exists on the rates of second and later doses of mumps vaccination. The extent of protection against breakthrough mumps infection provided by only one dose of mumps vaccine is unclear. Therefore, we assessed the mumps vaccination rates and mumps infection prevalence according to the number of doses received among university students. The main objective of this study was to clarify the hypothesis that receiving only one dose of mumps vaccine could result in a breakthrough infection rate of 5.3% or more among university and college students.
Design and methods
Study design and participant population
This cross-sectional study involved three centers. The target population was university students. To be representative of Japanese university students, we included three universities from three areas: Hyogo College of Medicine in an urban area, Faculty of Medicine of Saga University in a suburban area, and The University of Shimane Izumo campus in a rural area. Hyogo College of Medicine was converted into Medical University in 2022. The University of Shimane Izumo campus comprises a Nursing and Dietetics school. We invited 2018 students to participate in the study, without applying any exclusion criteria; however, students who were on vacation were excluded. The students who wished to participate were provided envelopes containing an informed consent form and were asked to write the address of their guardians. Subsequently, we mailed the envelopes and asked their guardians to complete the questionnaire and consent form and add photocopies or images of the Maternal and Child Health Handbook (MCHH) in the envelope and mail them back to us.
Outcomes and definitions
The primary outcome of this study was the prevalence of breakthrough mumps infection according to the number of vaccine doses received.
Separately, the effects of subsidies by local government for mumps vaccination were also investigated.
Informed consent and institutional review board
Informed consent was obtained from both the students (through a lecture) and their guardians (through the letter) for inclusion in the study. This study was approved by the Ethics Committee of Hyogo College of Medicine (Hyogo Medical University at present; 3307), Faculty of Medicine of Saga University (R1-35), and The University of Shimane Izumo campus (299). All procedures were conducted as per the code of ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Data collection
We collected data on past illnesses of vaccine-preventable diseases, vaccination history, and educational status of the student’s parents from the self-administered questionnaire. Information on vaccination (dates, locations, kinds, and lot numbers) and other perinatal data was collected from photocopies of the MCHH. In Japan, the MCHH is issued primarily in the pre-and post-natal periods by the local government at the guardians’ residences, by MCH Law, and the vaccinations are recorded there by medical professionals. 8 Because higher parental education had been reported to be associated with parental decision to vaccinate their children, 9 we collected data about the educational background of the students’ parents. The educational level of the parents of students in Japan has been reported previously. 10 This information enabled us to assess selection bias in the population responding to this survey. We also collected information on the measles, rubella, mumps, varicella, and hepatitis B antibody titer measurements (measured value, date, location, and infection type), which were submitted to the universities by the students’ guardians on each occasion.
Some local governments aim to improve the vaccination rate by offering subsidies to reduce the economic burden of voluntary vaccination. In addition to collecting information on students and guardians, we also collected information on whether mumps vaccination was subsidized at the location of the student’s residence by checking local government websites or via email or phone and compiling a database of local government subsidies by locality. We collected information on whether the local government subsidized vaccination, when subsidies were started, and the ages at vaccination, number of doses, and payment amount covered by local government subsidies (Supplemental Table 1). The survey was conducted from 1 July to 15 September 2021. The prefectures and municipalities of local governments were classified according to the codes set by the Ministry of Internal Affairs and Communications. 11
Definitions of variables
We transformed the variables according to the following definitions: we measured the serum immunoglobulin (IgG) antibody titers (U/mL) against mumps by enzyme immunoassay (EIA) as a surrogate method for neutralization tests. We used 4.0 U/mL as the cut-off titer to define seropositivity to mumps based on the results of a high antibody positivity rate.12,13 We had no information on the types of commercial Ig EIA test kits used to measure the antibody titers because details on the commercial laboratories that performed the assays were not provided. Furthermore, the date of antibody titer measurements and vaccinations were recorded to clarify their order because many students had their antibody titers against the five viral infections measured several times. The health centers at all three universities required that students submit mumps antibody titer results. Students who did not satisfy the cut-off antibody titer measurement were required to have an additional vaccination and then submit an updated antibody titer measurement. We used the most recent result in participants with two or more antibody titer results. We converted the unknown history of infection to no history of past mumps infection. We classified the father’s and mother’s years of education into the following five grades: 9, 12, 14–15, 16, and 18 years and above, as with the questionnaire based on the Japanese education system. We defined the primary outcome as the prevalence of breakthrough mumps infection after each dose of mumps vaccination, excluded before vaccination, using the dates of the mumps vaccination and infection. We set the prevalence of mumps infection in unvaccinated participants as the reference value. Seropositivity to mumps, mumps infection without vaccination, and post-vaccination mumps infection were defined as binary variables.
Statistical analysis
We hypothesized that the prevalence of breakthrough infection would be 5.3% in participants who had received only the first dose based on the results of our previous study that showed the number which the prevalence of breakthrough infection was.
Descriptive statistics were expressed as medians with interquartile ranges for continuous variables and as numbers and percentages for categorical variables. Furthermore, we used the Cochran–Armitage trend test for binary variables or the Jonckheere–Terpstra trend test for continuous variables.
For the sample size calculation, we calculated the sample size to show statistical significance for the proportion of mumps antibody positivity among students who had never been infected with mumps and were unvaccinated or had received only one dose of vaccine, using data from our previous studies. Subclinical mumps infection reduces the difference in susceptibility between unvaccinated individuals and those who have received only one dose of vaccine. Using mumps antibody positivity rates, we estimated that a sample size of 1100 students would be required based on the assumption that 65.4% of unvaccinated students and 55.7% of students who had received one dose of vaccine would be seropositive for mumps antibody. 6 In order to achieve the required sample size of 1100 students, a minimum participation rate of 55% among the 2018 eligible students in the three universities was required. A response rate above 50% is the minimum level required for an academic survey. 14 We also conducted a sensitivity analysis comparing the characteristics of participants and non-participants.
All analyses were performed using the Stata 17.0 software (Stata Corporation, College Station, TX, USA). All significance tests were two-tailed, and statistical significance was set at p < 0.05.
Results
The target population was 2018 students in three universities. Students who were on vacation from the university were excluded. Overall, 2004 students were eligible, of these, we excluded those who could not be contacted due to the COVID-19 pandemic and could not provide consent. Finally, we included 1653 (82.5%) students. Among them, 1214 (60.3%) students granted informed consent, and we mailed the required forms to their guardians. Finally, the guardians of 593 (29.5%) students returned the completed forms (Figure 1).

Study flowchart.
Table 1 shows the distribution of students in the four schools among the three universities. The participation rates were different among the three universities. The participation rate of Hyogo College of Medicine was 32.1%, the School of Medicine, Faculty of Medicine, Saga University was 36.8%, the School of Nursing, Faculty of Medicine, Saga University was 9.2%, and the University of Shimane Izumo was 24.5%. The number of male participants was 260 (43.8%). The median age of the participants was 21.6 years (interquartile range [IQR], 19.8–23.3 years). No medical school students and fifth- and sixth-year students from the School of Nursing, Faculty of Medicine, Saga University, and The University of Shimane Izumo campus were included in our study. A difference was found in the parents’ education levels in the four schools. The median years of education of the fathers was more than 18 years, 16 years, and 12 years for students at Hyogo College of Medicine; the Faculty of Medicine, Saga University School of Medicine and School of Nursing; and the University of Shimane Izumo campus, respectively. The median years of education of the mothers was 16 years for students at Hyogo College of Medicine and 14–15 years for those at the other institutions. The guardians of 592 (99.8%) students submitted the history of vaccination, and 462 (77.9%) submitted photocopies of the MCHH. With consent, we obtained the virus antibody measurements of 591 (99.7%) students from the healthcare centers at each university.
Characteristics of participants.

IQR: interquartile range; MCHH: Maternal and Child Health Handbook; SD: standard deviation.
Values are expressed in numbers (percentage) for binominal variables and mean (SD) or median (IQR) for continuous variables.
Table 2 shows the background characteristics of the university students who agreed and did not agree to participate in this study. There were significant differences in grade (p < 0.001) and major (p = 0.003) between the groups, but no significant differences in sex (p = 0.58) or university/college student status (p = 0.59).
Personal factors among university students with or without agreement to participate in the study.

Pearson’s chi-squared test for categorical variables.
The immunization status against mumps is summarized in Table 3. Of the 592 students who submitted their history of vaccination, 295 (49.8%) did not receive the vaccination, 297 (50.2%) had received the mumps vaccine, 264 (44.6%) had received the first dose, 31 (5.2%) had received the second dose, and 2 (0.3%) had received the third dose. The median mumps antibody titers (U/mL) were 7.1 (IQR: 5.0–11.0), 6.6 (4.2–10.5), and 4.0 (2.9–8.6) for the no, first, and second doses, respectively, and the mean titer was 4.1 for the third dose (p-value for trend = 0.042). Furthermore, 232 (39.3%) students showed seropositivity against the mumps virus. The mumps seropositivity rates were 43.2% (127 students), 36.7% (97 students), 26.7% (8 students), and 100% (2 students) for the no, first, second, and third doses, respectively (p-value for trend = 0.09). Moreover, 250 (42.7%) students had experienced a mumps infection. Among the 250 students, 203 (69.8%), 41 (15.7%), 6 (19.4%), and 0 had received no dose, the first dose, second dose, and third dose, respectively (p-value for trend <0.001).
Immune status for each dose of mumps vaccination among university students.
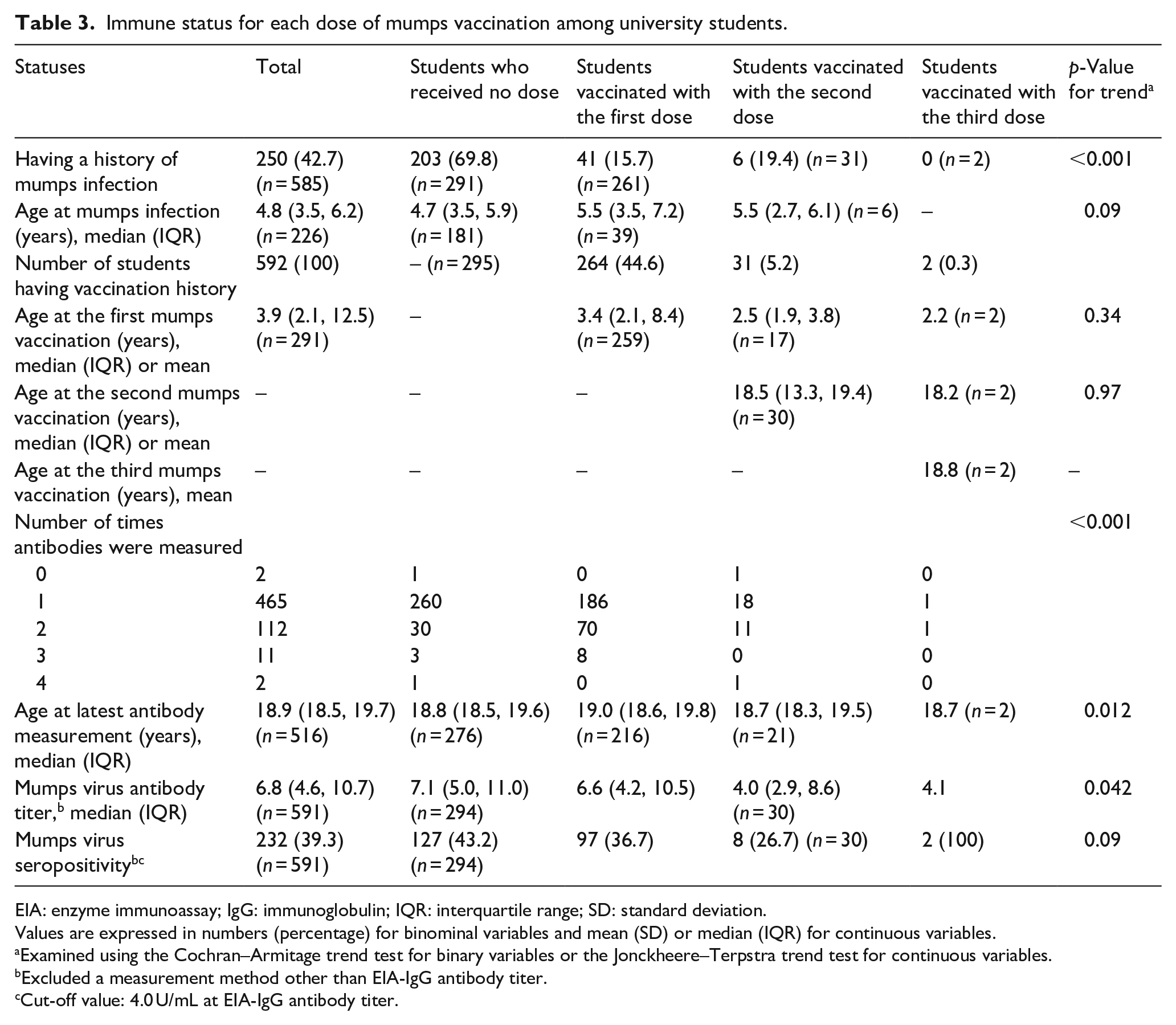
EIA: enzyme immunoassay; IgG: immunoglobulin; IQR: interquartile range; SD: standard deviation.
Values are expressed in numbers (percentage) for binominal variables and mean (SD) or median (IQR) for continuous variables.
Examined using the Cochran–Armitage trend test for binary variables or the Jonckheere–Terpstra trend test for continuous variables.
Excluded a measurement method other than EIA-IgG antibody titer.
Cut-off value: 4.0 U/mL at EIA-IgG antibody titer.
The prevalence of mumps infection among unvaccinated participants and according to the number of doses of mumps vaccine received is presented in Table 3. The mumps infection prevalence was 69.8% (203 students), 11.3% (28 students), 3.9% (1 student), and 0% among students who were unvaccinated (the reference) and those who had received the first, second, and third doses of the vaccine, respectively, as shown in Table 4.
Mumps infection prevalence according to the number of doses of vaccine received among university students.

Values are expressed in numbers (percentage).
Discussion
We surveyed the mumps vaccination and infection prevalence among students at three universities and described their characteristics, including their parents’ information. We found a low mumps vaccination rate and high mumps infection prevalence. Furthermore, we found that the 11.3% incidence of breakthrough mumps infection exceeded the hypothesized value of 5.3% for the alternative hypotheses.
Mumps vaccine coverage among university students in Japan remains below the level required for herd immunity. Only 5.6% (33 students) of the sample had received two or more doses. The mumps infection prevalence was 42.8%, and 39.3% of the students had seropositivity against the mumps virus. These trends were similar to those in our previous surveys in 2008 and 2009 of university students of health provider professional courses, where the rate of second or later doses of mumps vaccination was also only 1.5% (14 students), the mumps infection prevalence was 27.5% (241 students), and seropositivity against mumps virus prevalence was 40.9% (358 students). 6 In this study, we found that the mumps vaccination rate among medical university students who received two or more doses was 4.6%. Other researchers reported a rate of 4.3% (11 students) among 1st-year Japanese university students without a mumps infection history. 15 The rates of second and later doses of mumps vaccination have remained low for a decade and do not satisfy the 85–90% requirement for herd immunization. 2 The World Health Organization recommends the second dose of MMR vaccinations. 16 The low rates of vaccinations for second or later doses have led to the population becoming highly susceptible to mumps infection, which has increased the effective reproductive rate of the virus; such a situation can result in a mumps outbreak, as was found in Japan in 2016. 7 In this study, the antibody titer was highest in the unvaccinated participants, indicating that the antibody titer given by the natural infection lasts longer than that produced in response to vaccination. Therefore, the mumps vaccine strain does not provide a high level of protection against infection for long periods. More than 10% of the students who had received only one dose of mumps vaccine experienced breakthrough mumps infection. Therefore, to maintain adequate levels of protection repeated vaccination is necessary.
Administering only one dose of the mumps vaccine did not provide adequate protection against infection. Some students who were vaccinated with two or more doses of the mumps vaccine also did not have sufficient antibody levels to prevent infection. These students may be considered to have mumps vaccine failure. Moreover, some students vaccinated with the first dose did not receive a second dose for 10 years or more. Mumps virus antibody titers decreased during this time. Mumps antibody titers in students who received second and later doses could not be evaluated because it was not measured after the latest mumps vaccination. However, the students vaccinated against the mumps virus have antigen-specified memory B-cell against mumps for a long period. 17 During an outbreak among university students in the United States, the third dose of mumps vaccine in students who had received the second dose before the outbreak contributed to the control of the outbreak. 18 These reports support our results that mumps infection post-vaccination might decrease as the number of doses of vaccine increased. Therefore, based on our study results, we recommend administering two or more doses of the mumps vaccine that will enhance individual immunity.
In Japan, routine or subsidized vaccination is necessary locally to enhance individual immunity against mumps infection and herd immunity. In 2019, only 26.2% (456 of 1739) of local governments in Japan subsidized mumps vaccination. 19 We reported a positive association between recommending behavior of primary care physicians regarding mumps vaccine for children and the vaccine uptake by the residents where local subsidies were granted (adjusted odds ratio, 2.42; 95% CI, 1.57–3.71). 20 The recommendations for mumps vaccination could increase if subsidized vaccinations are provided. Therefore, if the central government cannot implement routine mumps vaccination immediately, local authorities should start implementing subsidies for mumps vaccination. Subsidizing the second and later doses of mumps vaccination for an individual would also ensure enhanced immunization of the target population. The results of cost-effectiveness analysis in Japan have shown that the mumps vaccination program is effective. 21 A two-dose mumps vaccination program is more effective than a single-dose vaccination program. Expanding the voluntary mumps vaccination throughout Japan eventually could replace voluntary vaccination with routine vaccination. Thus, further studies are needed to evaluate the contribution of subsidies toward preventing mumps infection. The exploratory analysis in this study revealed that 5% (22 of 110) of the local governments surveyed already subsidized mumps vaccination. However, none of the university students had benefited from the vaccination subsidy because of the young age limits covered by the subsidies. Therefore, if a survey is conducted again in the future, it will be possible to assess the effect of the mumps vaccination subsidy by local governments because children who received subsidized vaccination during childhood will have reached the age of university students by the 2030s.
This study had some limitations. First, a selection bias may have occurred since a major proportion of the eligible population did not agree to participate in the study. The students and their guardians who participated in this study might have been interested in vaccination. Subsequently, we conducted the sensitive analysis comparing differences in the characteristics between the participants and students who were eligible but declined the invitation to participate. The analysis showed significant differences by grade and major between participants and non-participants, suggesting some selection bias. Specifically, the lower participation rates among students in lower grades and nursing major students could have biased the results. Additionally, the target population was students training to become health professionals, who may have been more health-conscious than other university students. Second, a previous study reported that the prevalence of asymptomatic mumps infection was 24%. 22 Moreover, some students with higher mumps IgG due to vaccination were not aware of having mumps infection. 23 The mumps infection prevalence based on the guardian-reported data differed from this number; therefore, the possibility of measurement and recall bias cannot be eliminated, and the history of subclinical mumps infection in our sample may have been underestimated. In the future, however, digitized individual medical information will be recorded in Japan. Digitization is also being considered for the MCHH from which the vaccination information was collected in this study. 24 Digitization of information and implementation of a policy in which medical information and maternal and child health information, including vaccination information, is collected and integrated over the life span, would overcome some of the limitations of this study. 25 Third, we did not compare the prevalence of mumps infection among students who had never been vaccinated and students who had been vaccinated according to the antibody titer, because students who had been vaccinated had little time from the vaccination to the last antibody measurement. Therefore, were did not conduct statistical tests of the relationship between the antibody titers and susceptibility to infection.
In conclusion, we found that approximately 1 in 10 students who had only received one dose of vaccine had a history of breakthrough mumps infection.
Supplemental Material
sj-docx-1-phj-10.1177_22799036241246702 – Supplemental material for Mumps vaccination and immune status among Japanese university students: A multicenter cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036241246702 for Mumps vaccination and immune status among Japanese university students: A multicenter cross-sectional study by Jiro Takeuchi, Iwata Ozaki, Kokichi Hata, Manami Nozawa, Kanami Fukushima, Norio Fukumori, Mie Imanaka, Yuta Sakanishi, Masayuki Shima and Takeshi Morimoto in Journal of Public Health Research
Footnotes
Acknowledgements
Author contributions
J.T. conceptualized and designed the study, obtained the funding, acquired and managed the data, performed the statistical analyses, interpreted the results, and drafted the manuscript; I.O. designed the study, acquired and managed the data, and critically reviewed the manuscript; K.H. designed the study, acquired and managed the data, and critically reviewed the manuscript; M.N. acquired and managed the data, and critically reviewed the manuscript; K.F. acquired and managed the data, and critically reviewed the manuscript; N.F. acquired and managed the data, and critically reviewed the manuscript, M.I. acquired the data, managed the data, and critically reviewed the manuscript; Y.S. designed the study, interpreted the results, and critically reviewed the manuscript; M.S. designed the study, interpreted the results, and critically reviewed the manuscript; T.M. designed the study, interpreted the results, critically reviewed the manuscript, and supervised the whole study process. All authors read and approved the final manuscript.
Data accessibility
Data cannot be shared for privacy or ethical reasons.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (Grant Numbers JP19K19445).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.