
Abstract
Background:
Urticaria affects a wide range of daily activities and social relationships. It has a severe impact on quality of life (QOL) and causes psychological problems.
Objective:
was to assess the impact of chronic urticaria (CU) on quality of sleep, the levels of depression, anxiety, QOL and their interaction with each other and their relation to disease related factors.
Patients and methods:
The study included 25 patients with CU and 25 healthy controls. Urticaria Activity Score (UAS) was used for objective evaluation of the intensity of urticaria. Patients completed a 10-cm visual analogue score (VAS) indicating the overall severity of their itching over the previous 2 weeks. The Dermatology Life Quality Index (DLQI) was used to evaluate patients’ QOL. Patients were also assessed for anxiety and depression with the Hospital Anxiety and Depression Scale (HADS). Pittsburgh Sleep Quality Index (PSQI) was used for evaluation of sleep quality and sleep disturbances.
Results:
In our CU patients the mean of UAS7 score was 39.72 ± 2.76 and the mean of VAS score was 28 ± 1.34. The mean of DLQI score was 24.8 ± 4.37 indicating severe impact of QOL. CU patients had higher total HADS score when compared to controls; 72% of the patients had depression and 92% had anxiety. By using PSQI, CU patients had significantly longer sleep latency onset, shorter total sleep duration, lower sleep efficiency and higher PSQI scores compared to controls.
Conclusion:
CU highly affects the QOL of patients and is associated with higher levels of anxiety, depression and poor sleep quality.
Introduction
Urticaria is one of the most frequent dermatological complaints. It is a disease characterized by the appearance of wheals which disappear in 1–24 h. The clinical appearance of wheals is characterized by the sudden appearance of skin lesions and a central swelling of variable size which is associated with an itching or occasionally a burning sensation. Urticaria may occur with angioedema, the resolution of which can take up to 72 h and sometimes causes pain rather than an itching sensation. 1
Classification of urticaria is as acute (up to 6 weeks) or chronic (beyond 6 weeks of clinical course). Chronic urticaria (CU) is recurrent episodes occurring at least twice a week for more than 6 weeks. It affects 15%–20% of the population once or more during life. 2
CU is classified into subtypes as spontaneous (no specific eliciting factor involved) or inducible (specific eliciting factor involved) urticaria.3,4
Chronic spontaneous urticaria (CSU) is one of the common and frustrating diseases for both patients and physicians. It is a non-life-threatening disease though it has a major impact on quality of life (QOL) and may interfere with sleep and daily activities.5 –7 CU patients may suffer from considerable loss of energy, sleep disturbance, emotional upset and restrictions in the social life. CU can lead to depression and anxiety which can affect the QOL.7,8
Our study aimed to assess the impact of CSU on quality of sleep, the levels of depression and anxiety, and QOL as well as their interaction with each other and their relation to disease related factors.
Patients and methods
Study design
This case-control questionnaire based study was performed at the Department of Dermatology, Venereology and Andrology of Assiut University Hospitals (AUH), Assiut, Egypt. The Institutional Ethics and Research Committee approved the study which was conducted in accordance with the guidelines of the Helsinki Declaration. Each participant gave an informed consent prior to the study.
Participants
Fifty-five patients with CSU attending the Dermatology Outpatient Clinic, Assiut University hospital, Assiut, Egypt were randomly recruited. Among them, 32 fulfilled the inclusion criteria. Seven patients refused to fill the questionnaires and to participate in the study. Finally, 25 patients participated and completed the study.
The study included patients aged ≥18 years old with CSU defined as appearance of recurrent wheals more than twice a week for over 6 consecutive weeks.
Exclusion criteria included patients with chronic inducible urticaria, those who are unable to understand, or unwilling to complete the questionnaire, those with any psychiatric disorders, malignancy, central nervous system disease, cognitive impairment due to a current cerebral or psychotic illness. Patients on current psychotherapy, or glucocorticoid therapy during the last month were also excluded. Treatment with antihistamines was discontinued at least 72 h before evaluation.
A control group of 25 age and sex matched healthy adult volunteers; they were randomly recruited from individuals came to our dermatology department asking for cosmetic procedures.
Measures
Urticaria activity score
This is used for objective evaluation of the intensity of urticaria. It evaluates the main disease characteristics (itch, presence, and number of wheals) on a Likert-type symptom intensity scale (from 0 to 3). 9
The UAS7 is the sum score of 7 consecutive days, used in routine clinical practice to determine disease activity and response to treatment of patients with CSU. The urticaria activity score ranges from 0 to 42 for a week
Visual analogue scale
Patients also completed a 10-cm visual analogue scale (VAS) indicating the overall severity of their itching over the previous 2 weeks from 0 (none) to 10 (severe itching). 10
The dermatology life quality index
QOL was evaluated by the Dermatology Life Quality index (DLQI). 11 It consists of 10 questions subdivided into 6 domains (symptoms and feelings, daily activities, leisure, work/school, personal relationships and treatment). 11
Each question is scored on a scale which is ranging from 0 to 3 (very much). 12 The DLQI is calculated by summing the score of each question with a maximum of 30 and a minimum of 0; the higher the score, the worse the QOL. In addition to demonstrating its usefulness in assessing the most prevalent chronic skin diseases, the DLQI has been specifically validated for CU. 13
The hospital anxiety and depression scale
The levels of anxiety and depression were assessed by the hospital anxiety and depression scale (HADS). 14 It is a self-report rating scale of 14 items that contains two subscales designed to measure anxiety (HADS-Anxiety; HADS-A) and depression (HADS-Depression; HADS-D); seven items for each subscale. Responses to each item are indicated on a four-point Likert Scale from 0 to 3 (score range 0–21, for each subscale), with a high score indicating more symptoms. 14
Recommended cut-off scores are 8–10 for doubtful cases and ≥11 for definite cases for both HADS Anxiety and HADS Depression. 15
The Arabic version of HADS has been adopted from MAPI Research Trust (www.mapi-trust.org). The validity and reliability of the Arabic version have been established previously. 16
Pittsburgh sleep quality index
Sleep quality and disturbances were assessed by Pittsburgh sleep quality index (PSQI). It contains 19 self-rated questions, designed to measure seven aspects of sleep which areeach scored on a scale of 0–3, where a score of 0 indicates no sleep disturbance and a score of 3 indicates significant sleep disturbance. It differentiates ‘poor’ from ‘good’ sleep by measuring seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction over the last month.
Scores from all seven domains are then added to calculate the global PSQI score, which will lie in a range of 0–21, where higher scores indicate poor or worse sleep quality. A score of more than five is consistent with clinically significant sleep difficulty. 17
The Arabic version of PSQI was provided by MAPI Research Trust (www.mapi-trust.org) and has been previously validated.18,19
The HADS and the PSQI questionnaire form were also completed by 25 age and sex-matched healthy individuals who had no history of urticaria or other skin diseases or psychosomatic/psychiatric morbidity.
Statistical analysis
Data was analyzed using STATA version 14.2 (Stata Statistical Software: Release 14.2 College Station, TX, USA: Stata Corp LP.). Quantitative data was represented as mean, standard deviation and range. Data was analyzed using student t-test to compare means of two groups. When the data was not normally distributed Mann–Whitney test was used to compare two groups. Qualitative data was presented as number and percentage and compared using either Chi square test or Fisher’s exact test. Spearman correlation analysis was done. Odds ratios were obtained from logistic regression analysis for binary outcome. Linear regression analysis was done for predictors of continuous variable. Graphs were produced by using Excel or STATA program.
p-value was considered significant if it was less than 0.05.
Results
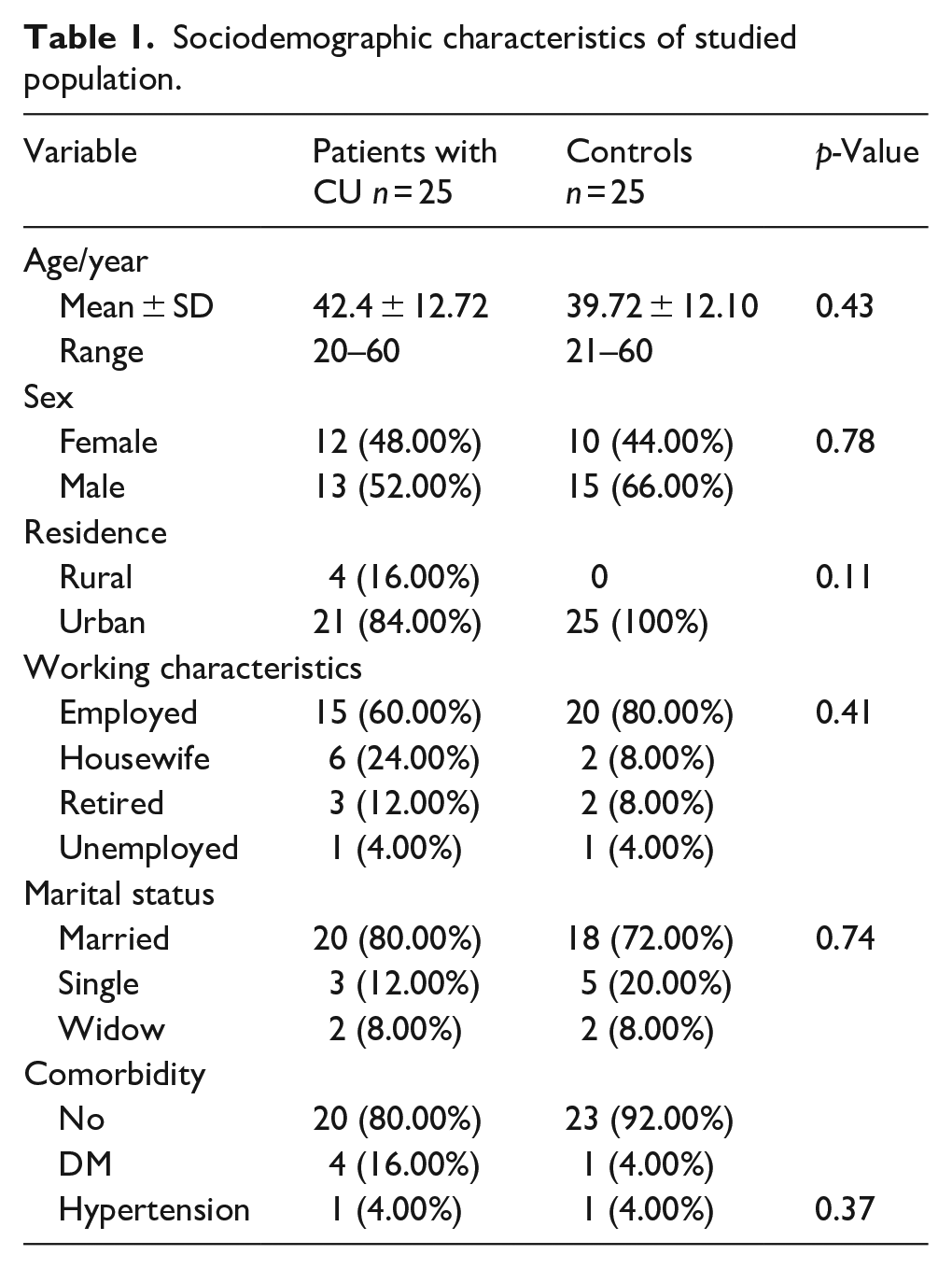
This study included 25 patients with CU (13 males and 12 females) with age ranged from 20 to 60 years old; the mean of their age was 42.4 ± 12.72 and 25 healthy controls (15 males and 10 females) with age ranged from 21 to 60 years old; the mean of their age was 39.72 ± 12.10. There was no significant difference with respect to sociodemographic characteristics between the groups of patients and healthy controls (Table 1).
Sociodemographic characteristics of studied population.
The mean duration of urticaria was 1.9 ± 1.21 years. There was a positive family history of urticaria in 20% of patients, and 40% of patients had history of angioedema. Sun exposure was the most common exacerbating factor (72%); other factors included foods, stress and exercise. Seventy-two percent (18 patients) had previous treatment with antihistamines (12 patients were treated with the standard dosing and 6 patients required up-dosing). Moreover, 20% of the patients were treated with systemic steroids. None of the patients were treated with immunosuppressives or omalizumab. The mean of the VAS for itching intensity was 28 ± 1.34. The mean of UAS7 score among patients with CU was 39.72 ± 2.76 (Table 2).
Clinical characteristics of patients with CU.

DLQI results
The mean of total DLQI score for the patients was 24.8 ± 4.37 with range 18–30; indicating severe impairment of QOL. According to scores of the different domains assessed by the DLQI questionnaire, there was more severe involvement in areas relating to work and school (question 7), Daily activities (questions 5, 6) and personal relationships (question 8) (Figure 1).

Frequency of the questionnaire dermatology life quality index (DLQI) answers according to the question evaluated.
PSQI results
Regarding sleep quality, the mean total PSQI score was significantly higher in CU patients than controls (p < 0.0001) indicating poorer sleep quality. CU patients scored higher for all PSQI domains in comparison with controls. All patients were characterized as poor sleepers (PSQI > 5). Sleep duration, habitual sleep efficiency, sleep quality and day time dysfunction were the more severely affected domains (Table 3).
Mean scores of Pittsburg sleep quality index (PSQI) domains among CU patients and controls.

PSQI: Pittsburgh sleep quality index; SD: standard deviation.
As regards sleep characteristics, patients showed shorter total sleep duration (2.72 ± 1.24 vs 6.72 ± 1.17 h, p < 0.0001), longer sleep latency (66 ± 26.93 vs 10.8 ± 4.71 min, p < 0.0001) and poorer sleep efficiency (35.52 ± 16.40% vs 91.68 ± 9.29%, p < 0.0001) in comparison to controls, as shown in (Table 4).
Sleep characteristics of studied population.

SD: Standard deviation.
HADS results
The patients group showed significantly higher total HADS score as well as HADS-A and HADS-D scores compared to controls (p < 0.0001 for all), 72% of patients were found to be depressed (HADS-D ≥ 11) and 92% had anxiety (HADS-A ≥ 11), this was presented in (Table 5).
Hospital anxiety and depression scale among CU patients and controls.

HADS: hospital anxiety and depression scale.
Regarding predictors of sleep outcomes, multiple linear regression showed that older age was associated with poorer sleep efficiency. In addition, higher HADS-A scores were associated with shorter total sleep duration. Male gender was associated with better sleep efficiency; however, this did not achieve statistical significance (Table 6).
Multiple linear regression: results for the continuous variables of Pittsburgh sleep quality index (PSQI) total score, sleep onset latency, total sleep duration and sleep efficiency.
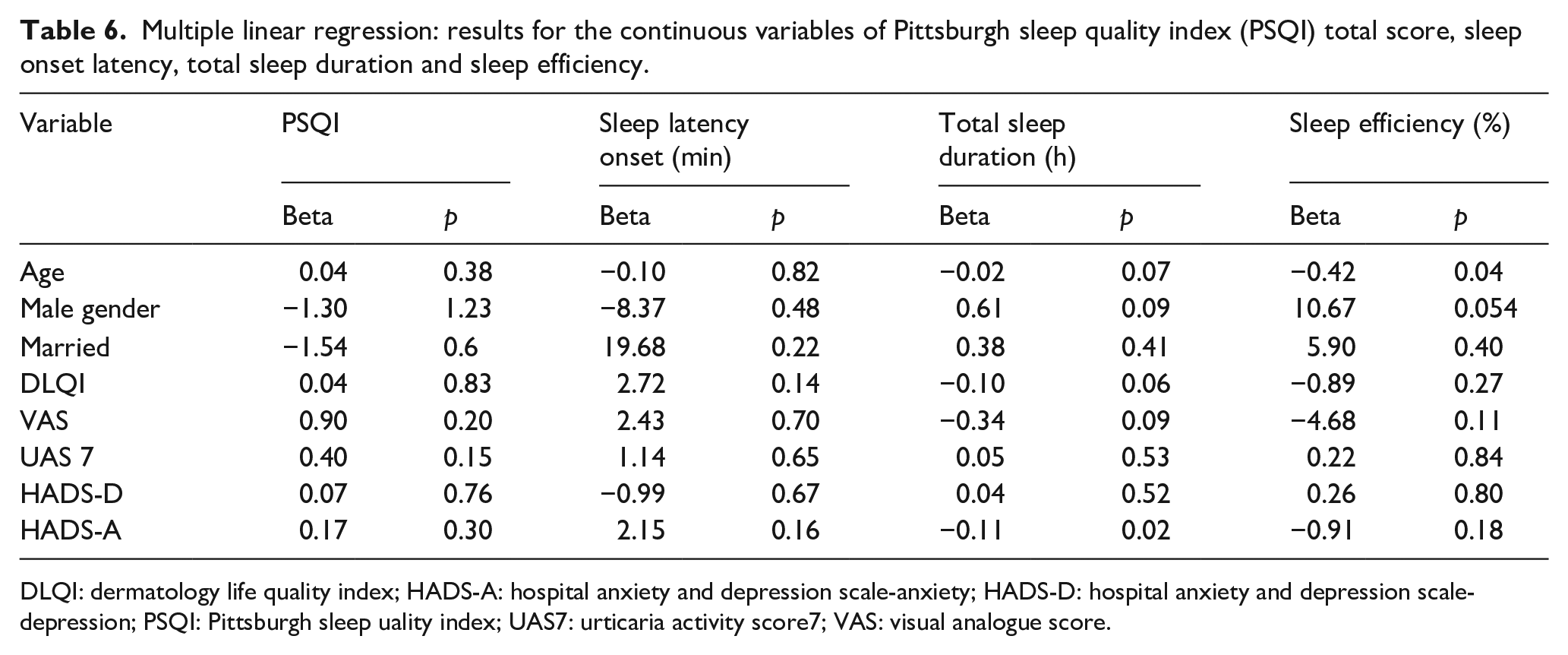
DLQI: dermatology life quality index; HADS-A: hospital anxiety and depression scale-anxiety; HADS-D: hospital anxiety and depression scale-depression; PSQI: Pittsburgh sleep uality index; UAS7: urticaria activity score7; VAS: visual analogue score.
There was no correlation between age or duration and any of HADS-A, HADS-D, DLQI and PSQI scores. Both DLQI and PSQI scores positively correlated with UAS7 score and VAS score; while HADS-A and HADS-D scores showed correlation with VAS score but not with UAS7 score. Also, there was positive significant correlation between DLQI and PSQI scores. In addition, there was significant positive correlation of HADS-A scores with PSQI and HADS-D scores, as shown in (Table 7).
Correlation of clinical and psychometric scores.
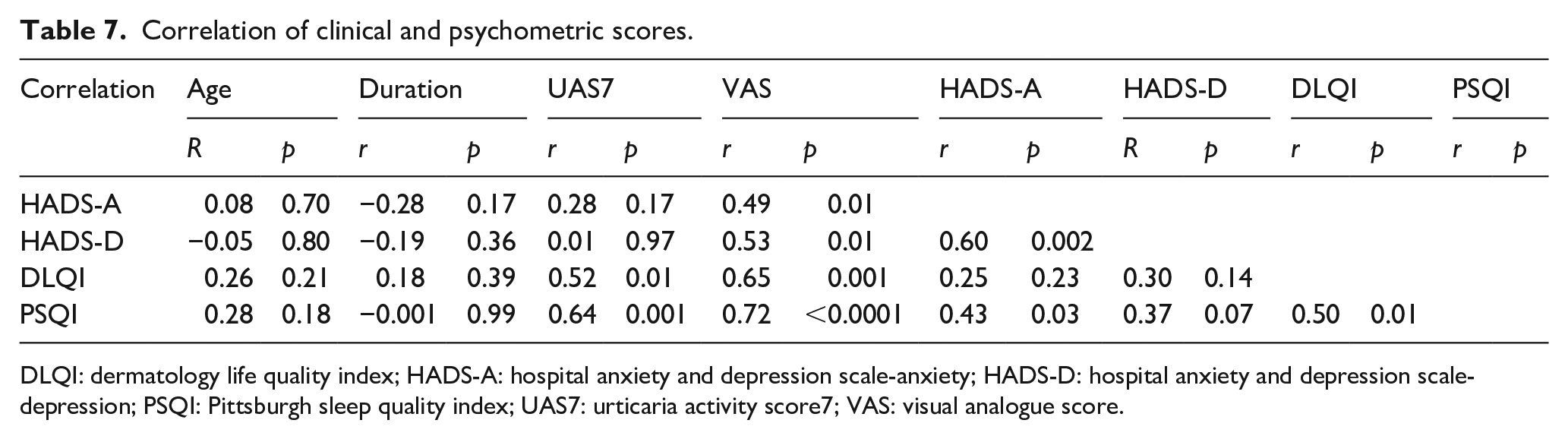
DLQI: dermatology life quality index; HADS-A: hospital anxiety and depression scale-anxiety; HADS-D: hospital anxiety and depression scale-depression; PSQI: Pittsburgh sleep quality index; UAS7: urticaria activity score7; VAS: visual analogue score.
Discussion
Depression and anxiety are the common psychiatric disorders found in CU patients, and these psychiatric disorders may in turn affect QOL.8,20
In the current study, all patients had severe urticaria as measured by UAS7 score with high DLQI scores, indicating severe impact on QOL. In accordance with our study, Silvares et al., 21 reported that CU seriously compromises the QOL of the patients evaluated at a university service in Brazil.
In another study, CU had moderate impact on the QOL of patients but involved different fields of life; including physical image, social life, quality of sleeping and eating. 22
In the current study, among the six DLQI domains, there was greatest negative impact on areas related to work and school and the lowest scores impact on areas related to leisure. A large cohort study observed that 41.6% of patients with CSU had DLQI scores of 10 or greater. The most affected domains were symptoms and feelings, daily activities, work and school. Almost 50% of patients had moderate to severe disease activity. The more severe degrees of QOL impairment in the present study could be attributed to severe disease activity where all patients had UAS7 scores above 28. 23
In this study, we found that patients with CU had higher HADS depression, anxiety and total HADS scores when compared to controls. These findings are consistent with those of previous studiesshowing that CU patients had higher levels of depression and anxiety.24,25
In the current study, 72% of patients were found to be depressed and 92% had anxiety. Choi et al. 26 observed a prevalence 48.1% and 38.0% of depression and anxiety in Korean CU patients.
A recent meta-analysis demonstrated that patients with CU had 3-fold risk of anxiety or depression, and patients with CSU had 6-fold risk of anxiety or depression, compared to the controls. 27 Meanwhile, another study failed to corroborate higher levels of depression or anxiety. 28 The heterogeneity of results could be partly attributable to variation in the measurement tools used for anxiety and depression in different studies and to the variation of severity of disease activity.
Studies supported the association of anxiety and depression with increased mast cell counts and degranulation. 29 The depression levels in patients with mastocytosis were found to be significantly associated with tryptophan levels, 30 suggesting that mast cells participate in the inflammatory pathway associated with depression. Mast cell activation also increases anxiety-like behavior. 31
In our study, CU patients had significantly impaired sleep quality as estimated with the PSQI questionnaire; they showed longer sleep latency onset, shorter total sleep duration, lower sleep efficiency and higher PSQI scores compared to controls. Also, patients were negatively affected in terms of sleep disturbance, quality and latency, habitual sleep efficiency, and daytime dysfunction.
Similar findings were observed by Latif, 32 who found a significantly higher overall score of PSQI in CSU patients than the healthy controls. Furthermore, the study showed a significant influence on sleep latency, sleep duration, sleep disturbance, and daytime dysfunction domains.
In a previous study, frequent interference with sleep (described as “often” or “every night”) was reported by more than 50% of patients with CU. Furthermore, sleep impairment was more problematic in patients with CU than in those with atopic dermatitis. 33
Using the insomnia severity index, Mann et al., 34 found that there is a high likelihood of sleep disturbance in patients with CU especially during a flare. The study results reported that pruritus is not the only reason for insomnia in CU patients.
Histamine is one of the neurotransmitters that provide alertness. Histamine H1 receptor in CNS is important for the control of arousal and regulation of the sleep-wake cycle. The level of histamine release increases in the evening and again in the early hours of the morning; which could explain the longer sleep latency and shorter total sleep duration in patients with CU. 35
According to a population-based data in Taiwan, it was found that the risk of CSU was higher in the patients with sleep disturbances than in the controls. 36
Moreover, obstructive sleep apnea syndrome (OSAS) was associated with CSU; suggesting that the inflammatory pathways activated in OSAS may contribute to the development and progression of urticaria.12,36
Increased inflammatory cytokines such as TNF-α and IL-6, has been also reported in patients with sleep disturbances, both playing an important role in the pathogenesis of CU. 37
Therefore, it seems that the relationship between sleep disorders and CU is bidirectional; where CU may interfere with sleep quality, and poor sleep may initiate or trigger CU development.
In the present study, there was no influence of age, gender, marital status, disease duration or presence of angioedema on depression or anxiety in CU patients. Also, there was no significant correlation between age or disease duration and QOL, depression and anxiety scores.
Similarly, Tat 24 reported that there was no significant correlation between age or disease duration and anxiety or depression scores.
In our study, QOL was unrelated to levels of depression or anxiety. However, DLQI correlated with both VAS and UAS7 scores; indicating that QOL is greatly influenced by itch intensity and disease activity. Other studies also revealed similar relations between CU severity, itch and QOL.38,39
In contrast, Engin et al., 20 showed that QOL was associated with levels of anxiety and depressive symptom rather than urticarial symptoms.
In our study, there was a correlation between HADS-A and HADS-D. Also, both anxiety and depression scores correlated with itching severity assessed by VAS score. However, the UAS7 did not show correlation with depression or anxiety scores.
Similar to our results, multiple studies have reported that the levels of depression and anxiety, were unrelated to UAS,20,40 indicating the absence of a significant relationship between disease activity and depression or anxiety. On the contrary, UAS7 had a significant effect on both anxiety and depression in another study. 24
In the present study, older age was associated with poorer sleep efficiency. However, unlike our study, it was suggested that younger patients with CU seemed to be troubled by impaired sleep. 34 Male gender was also relatively associated with better sleep efficiency. Although not significant, it might have achieved statistical significance in a larger sample.
We found that the severity of urticarial symptoms assessed with VAS and UAS7 scores significantly correlated with poor sleep quality assessed by PSQI scores. In line with our results, Mann et al., 34 found that CU patients with a higher DLQI score and a higher pruritus score were less satisfied with their sleep pattern.
Gimenéz-Arnau et al., 41 found a substantial improvement of sleep quality under omalizumab treatment, according to the results of three randomized, double-blind, placebo-controlled studies.
Our results also indicated that the levels of anxiety significantly correlated with poor sleep quality. It can be postulated that poor sleep could act as both an effect of anxiety and a risk factor for the development of anxiety.
In conclusion, CU seriously compromises the patients’ quality of life and is associated with higher levels of anxiety, depression and poor sleep quality. Impaired QOL positively correlates with disease activity, while anxiety and depression are associated with pruritus severity but not urticarial activity. The association between sleep disturbance and CU is directly related to the severity of urticarial symptoms and to anxiety levels.
Further research into objective measurements of sleep quality should be conducted to elucidate the nature of poor sleep in these patients. Further studies are required to clarify thoroughly the underlying mechanism linking sleep disorders and CSU.
Limitations
One of the limitations of our study was the small sample size. The use of self-report questionnaires could be limitations of the study because the patients tend to overestimate their answers.
Supplemental Material
sj-docx-1-phj-10.1177_22799036241243268 – Supplemental material for Does chronic urticaria affect quality of sleep and quality of life?
Supplemental material, sj-docx-1-phj-10.1177_22799036241243268 for Does chronic urticaria affect quality of sleep and quality of life? by Azza M Abdel-Meguid, Sara M Awad, Mostafa Noaman, Asmaa M Abdel Gawad and Doaa A E Abou-Taleb in Journal of Public Health Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.