
Abstract
Background:
Traditional eye medicine (TEM) is becoming more widely used across the world. Depending on the drugs used, TEM usage can be considered harmful or innocuous. The therapy may induce infection or irreparable blindness in the already injured eye.
The aim of the study was to determine the proportion of traditional eye medicine practices and associated factors among adult ophthalmic patients attending ophthalmic clinics in the governmental hospitals in the West Bank.
Design and methods:
A cross-sectional study conducted on 300 patients. The data was collected using a structured, self-administered questionnaire.
Results:
The results of the study revealed that 65.7% of people use TEM. The most common symptoms that necessitated the use of traditional eye practice were inflammatory symptoms of the eye (49.2%), blurred vision (15.7%), and allergic conjunctivitis (10.7%). The most common TEM used was tea (34.0%), followed by herbal products (25.4%) and vegetable slices (potato, cucumber, and onion) (14.7%). The most traditional eye treatment was the topical route (92.9%). The majority of prescribers of traditional eye practice were traditional healers (48.7%). Furthermore, the current study found that occupation and the income were predictors of using traditional eye practice among ophthalmic patients attending ophthalmic clinics in selected West Bank hospitals.
Conclusion:
The proportion of traditional eye medicine practice was high among ophthalmic patients in the West Bank. The predictors of using traditional eye treatment were occupation and the income. The most common TEM used was tea, followed by herbal products and vegetable slices (potato, cucumber, and onion).
Introduction
The eye is a sensory structure that reacts to light and receives sensory input from the retina’s rod and cone photoreceptor cells to enable light perception and vision, color differentiation, and depth perception. 1 Because the eye is so important in one’s life, one should do everything possible to keep it functioning properly. Traditional healers provide an awareness of eye diseases and community eye care based on cultural beliefs and practices, especially when patients are hesitant to seek treatment from professional eye care service providers. 2 Some eye care treatments can result in serious ocular complications and vision loss.
Traditional eye medicine (TEM) refers to biologically based therapies, practices, or partially processed organic or inorganic agents that can be administered via various routes to achieve the desired ocular therapeutic effect. 3 Traditional medicine is increasingly being used to treat eye diseases around the world. 4 Some 80% of the world’s population meets their drug needs with herbal drugs, which supports an estimated 80% of the developing world’s population’s reliance on herbal medicine. 5 Among the most well-known forms of TEM are herbal extracts, honey, breast milk, soil, human saliva, linseed (Linum usitatissimum), “damakesie” (Ocimum species), potato (Solanum tuberosum), milk, plant extracts, lemon juice, and some dried insect bodies.6 –9
Traditional medicine is still active in rural Saudi Arabia, India, and Africa.6,7,9,10 Affordability, low socioeconomic status, and a lack of formal education are the determinants of traditional eye medication use in these communities. 11 Traditional medicine is based on rules of knowledge and practice used to diagnose, prevent, and cure disease. This may be based on past experiences and observations transferred from generation to generation verbally, spiritually by ancestors, frequently in the form of stories, or, in modern times, in writing. 12 Traditional eye medicine are widely practiced in Palestine and the Arab world. 9 A study conducted in the Riyadh region among 1354 participants revealed a high prevalence (37.2%) of self-medication. 13 Another study reported the incidence of self-medicating with traditional eye medicine (TEM) in Taif city to be 35%. 14
It is thought to be an alternative form of health care and is popular in developing countries. It is a less expensive and more widely available alternative to pharmaceutical drugs. These treatments may cause irreversible ocular complications, such as blindness. 7 The use of harmful traditional eye practices that result in a sudden loss of vision rather than seeking professional eye care at the onset of an eye problem is a major concern. However, there is a paucity of published evidence on traditional eye medicine practices and the factors that influence them in ophthalmic patients. 15
Traditional eye medicine practices are very common in Palestine, where people prefer to use eye care before consulting an ophthalmologist. However, after searching different databases, there are no previous studies conducted on traditional eye medicine practice in Palestine. Therefore, the purpose of the study was to determine the proportion of traditional eye medicine practices and associated factors among adult ophthalmic patients attending ophthalmic clinics in the governmental hospitals in the West Bank.
Method
A cross-sectional study was conducted at the ophthalmic clinics of Rafidia and Hugo-Chaves hospitals in the period from January 15 to May 15, 2022. The Hugo-Chaves hospital is a governmental ophthalmic hospital located in the village of Turmus’aya near Ramallah, providing advanced eye care and surgery. The hospital consists of four floors with an overall area of 7300 m2. Rafidia hospital is a governmental hospital located in Nablus, in the north of the West Bank. It is considered a referral hospital for the northern area. It is composed of an ophthalmic ward for daycare.
Study population and sample
The study included all adult ophthalmic patients (approximately 20,000) with an age over 18 who were attending ophthalmic clinics in the Rafidia and Hugo-Chaves hospitals in the West Bank. The sample size was calculated using the Raosoft program with a population of 20,000, a confidence level of 90%, a margin of error of 5%, and a response rate of 50%. A total sample of 267 participants was needed to conduct this study. The study was conducted with a convenience sample (300 participants).
Inclusion and exclusion criteria
Patients who are above 18 years old and attend ophthalmic clinics were included. Also, participants who agree to participate were included. Patients suffering from severe mental illness or cognitive disorders, disoriented patients, and patients who have been complaining about their discomfort or pain during data collection were excluded.
Instruments of the study
A self-reported questionnaire was developed by the researchers and modified to match the study objectives. The instrument is composed of demographic data such as age, gender, religion, level of education, marital status, occupation, residence, health insurance, and monthly income. Medical history is composed of six questions answered with yes or no. Traditional eye medicine practice among ophthalmic patients composed of five questions. Types of traditional eye medicine practice or treatment used, and route of using the traditional eye medicine practice or treatment. Prescriber of traditional eye practice and treatment.
The validity of the questionnaire was assessed by an expert panel of five anonymous ophthalmology specialists’ with backgrounds in public health who have been working in the Palestinian health sector for a long period of time.
A pilot study was conducted at Rafidia hospital on 15 participants with a history of TEM use. Cronbach’s alpha value of Traditional eye medicine practice scale was (0.83). The pilot was excluded from the actual study. Cronbach’s alpha was (0.87) of Traditional eye medicine practice scale for the actual current study.
Data collection
After the investigators obtained the permission from the Palestinian ministry of health, they visited the targeted hospitals. The investigator approached the participants, the participants were greeted, and the investigator introduced himself and his intention of engaging the participant in a conversation. He administered the information document and explained in detail what the study entails. A participant who agreed to be enrolled in the study was given a consent form to be signed to participate in the study. The questionnaire was administered in a room near the ophthalmic clinic in the targeted hospitals to ensure privacy. The participants were given sufficient time to provide responses to fill out the questionnaire, and the investigator was available to explain or provide more information on the questionnaire. In the cases of participants who were illiterate, the investigator read out the questions and assisted the participants with filling out the questionnaire. The investigator administered the questionnaire through a face-to-face interview. The participants completed the questionnaire in the Arabic version. The questionnaire was translated by two independent bilingual translators.
Ethical consideration
Ethical approval was obtained from the Arab American University. A consent form was provided for every participant prior to the study. Voluntary participation was explained. No names were mentioned or any personal information about the participant was provided. All data was kept confidential and used for study purposes only. There are no harms or consequences due to participation refusal, such as care quality or privileges. A clear explanation was given to each participant about the study objectives and tools, and enough time was given for questions.
Data analysis
The data were analyzed using SPSS version 23.0 software. Frequency and percentage for descriptive data. Multiple logistic regressions were used. Differences with a p value of 0.05 are considered statistically significant.
Results
Participants’ characteristics
A total of 300 participants agreed to participate in the study and have completed the questionnaires. Of these, 143 (47.7%) were over 50 years old, and 171 (57.0%) were female. The majority of the participants, 242 (80.7%), are Muslims, and 182 (60.7%) are married. According to residence, the analysis revealed that 196 (65.3%) of the patients are from rural areas, and more than half of the participants 160 (53.3%) have health insurance. Also, 87 (29.0%) of their levels of education are primary school, and 109 (36.3%) are housewives. In addition, 153 (51.0%) had income below 2000 New Israeli Shekel (NIS) per month, as seen in Table 1.
Demographic characteristics of the participants (N = 300).

According to patients histories with eye care, 184 (61.3%) of the participants reported that they lack the accessibility to reach a modern eye clinic or hospital. Also, 207 (69.0%) of the participants reported that there is a traditional healer in their area, and 188 (62.7%) of them have a family history of traditional eye medicine practice. Although 206 (68.7%) of them reported that they had no knowledge about traditional eye medication, 197 (65.7%) have used traditional medication in the past 2 years, as seen in Table 2.
Patients History of eye practice (N = 300).

The analysis of the study results revealed that 166 (84.3%) of the participants believed that traditional eye medicine was beneficial. Also, 120 (60.9%) of the participants reported that traditional eye medicine practice was used for a week’s duration. In addition, 97 (49.2%) of them reported that inflammatory symptoms of the eye necessitated the use of traditional eye medicine practices or treatments. The majority of them, 183 (92.9%), reported that they used topical traditional eye medicine practice, and 96 (48.7%) of them reported that traditional healers prescribed traditional eye practice, as seen in Table 3.
Traditional eye medicine practice among ophthalmic patients (N = 197).

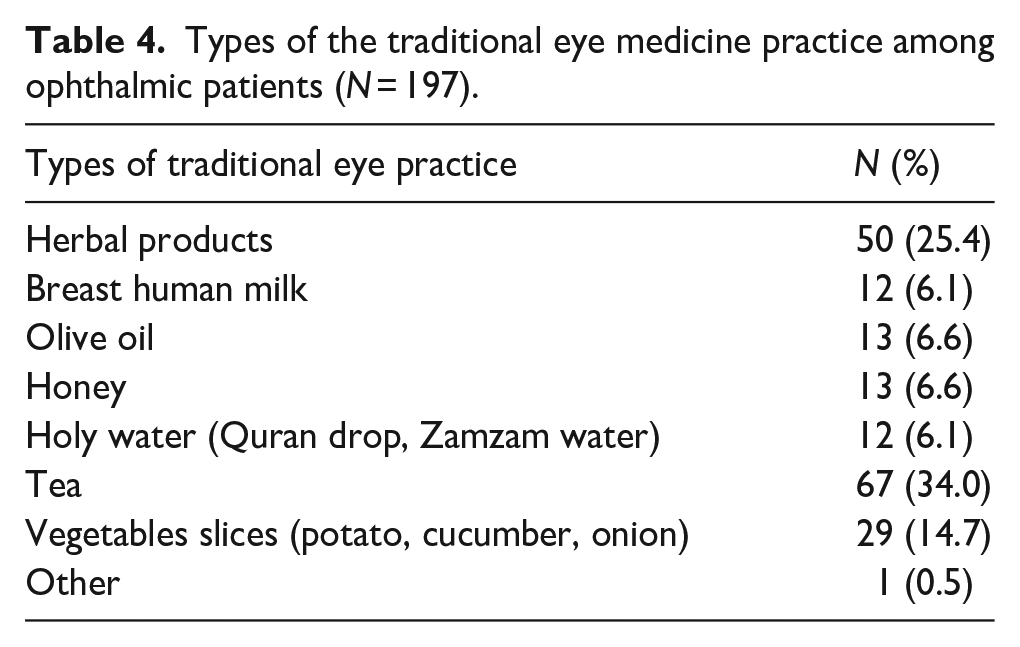
Also, the study results analysis revealed that tea was the most commonly used for traditional eye practice. One third of the participants, 67 (34.0%), used tea as a traditional eye practice, as seen in Table 4.
Types of the traditional eye medicine practice among ophthalmic patients (N = 197).
Logistic regression with enter step showed that among independent variables, occupation (student) (OR 0.013, 95% CI 0.001–0.146), and average income/ month (Below 2000 NIS) (OR 18.158, 95% CI 2.726–120.943) were the predictors of using the traditional eye practice among the ophthalmic patients attending the ophthalmic clinics in selected West Bank hospitals (Table 5).
Predictors of traditional eye medicine practice.

Discussion
According to the current study’s findings, 65.7% of people use TEM. This finding was supported by Jaya and Masanganise, who found that 61.5% of new patients in Zimbabwe had TEM. 16 This result, however, was higher than that of a hospital-based study in the Nigerian population, in which 48.7% of patients used TEM. 17 Also, this finding was higher than study conducted in Gondar, north-west Ethiopia, which discovered that 12.2% of people had used traditional eye medicine in the previous 2 years. 6 In other hospital-based studies in the same region, the reported prevalence of TEM use was 1.5% and 13.2%, respectively.18,19
In addition, a population-based study in Saudi Arabia found that 35% of patients preferred using traditional eye medications, and 38% of patients in India preferred using traditional eye medications.14,20 This variation could be explained by differences in the study setting and target population. The second reason could be due to cultural differences between nationalities.
In the current study, tea (34%), herbal products (25.4%), and (14.7%) vegetable slices (potato, cucumber, and onion) were the most commonly used traditional eye medicines. Similarly, a Zimbabwean study found that the most common category of TEM used was plants and plant products. 16 According to another study, the most commonly used TEMs were breast milk (40%) and plant products (29%). 20 In addition, in a facility-based study in North Central Nigeria, the extract from crushed leaves or roots (37.1%) that is instilled into the conjunctiva sac was found to be the most commonly used type of traditional eye medicine. 21 Overall, the differences in substances used for traditional eye treatment in various studies can be attributed to a combination of cultural, historical, environmental, and practical factors.
Simultaneously, a hospital-based study in Sao Paulo, Brazil, reported the use of homemade, traditional products such as boric acid, normal saline, and herbal infusions for ophthalmic emergencies. 22 A population-based study in India discovered that traditional eye medicine (surma/kajal), honey, ghee, rose water, and other plant, dairy, and animal products were commonly used (25.7%) in the rural population. 10 According to a population-based study in Saudi Arabia, the most commonly used traditional eye treatments were castor oil (49.3%), antimony (khohl alethmed) (40.6%), chamomile (19.6%), and green tea leaves (11.4%). 23
In the current study, 48.7% of participants consulted traditional healers, 14.2% consulted clergymen, and 12.2% consulted relatives. These findings were higher than those of an Indian population-based study, which found that only 8.4% of participants sought help for their ophthalmic problems from traditional healers, drug stores, non-registered practitioners, pharmacists, and chemists. 10 This could be attributed to a combination of cultural, economic, and healthcare system-related factors. In contrast, a Zimbabwean study found that in 95% of cases, the provider of TEM was not a formal traditional healer but rather a relative. 16 Furthermore, Oyediji et al. discovered that 65.7% of traditional eye treatment providers were primarily traditional healers in a facility-based study in north-central Nigeria. 21
According to the current study, 49.2% of participants reported that the most common symptoms necessitating the use of traditional eye medicine were inflammatory eye symptoms. These findings were in contrast to a hospital-based study conducted in the Zimbabwean population, in which ocular surface inflammation such as tearing (77.4%), redness (74.9%), itchiness (71.6%), and pain (70.3%) were the initial ocular symptoms prior to the use of TEM. 16
The current study’s findings also revealed that traditional eye medicine was administered topically 92.9% of the time. Similarly, 92.4% of TEMs were administered as topical eye drops in Zimbabwe. 16 These findings were in contrast to a study conducted in Nigeria that found 25% of patients treating eye conditions gave their medications topically. 12.5% were by incantations only, while 62.5% were by combining both. 24
The current study found that occupation (student), and the income were predictors of using traditional eye practice among ophthalmic patients attending ophthalmic clinics in selected West Bank hospitals. This finding was inconsistent with the findings of a study conducted in Ghana, which found that age was significantly associated with TEM use. 25 Furthermore, in a facility-based study in North Central Nigeria, it was discovered that patients’ residence, age, and occupation were all factors in their use of traditional eye medicine. 21 Aghaji et al. discovered that elderly adults used TEMs primarily because they were less financially capable than when they were younger. 26 Furthermore, Al-Akily et al. attributed TEM use to this age group’s adequate knowledge of medicinal plants. 27
A study conducted in southern Nigeria, however, found that the male gender, people from lower socioeconomic classes, and those with no formal education were more likely to use TEM. 11 Another study in North West Ethiopia discovered that having a positive family history of traditional eye medicine use, being unmarried, being illiterate, having limited access to modern eye care services, and the availability of traditional healers all had a significant association with the practice of traditional eye medicine. 6 These findings could be explained by differences in knowledge and attitudes toward traditional eye medicine among people of different literacy levels. Furthermore, financial issues may contribute to traditional eye medicine use because most people with less than a college education have fewer job opportunities and lower pay, which may lead to a preference for traditional eye medicine.
The current study has some limitations; it is geographically limited and does not represent the entire population of Palestine. The questionnaire was a self-reported questionnaire. Selection bias, as patients in ophthalmic clinic may not reveal their usage of TEM. Also, adding a qualitative component to this study (mixed method study) could have revealed more traditional eye practices which were not included in this survey instrument. The study was also based on respondent recall of events from the past few weeks, which predisposes the results to recall bias. Strikes by nurses during the study period limit the response rate.
Implications for clinical practice
There is a need for health education among the general public about the deleterious effects of traditional eye medicine. There is also a need to upgrade primary eye care programs with greater emphasis on eye care during the training of nurses and community health professionals. It highlights the need for effective execution and establishment of accessible, high-quality primary eye care services and an organized, healthcare referral network. Public awareness and regulatory legislation must be implemented to decrease the harmful effects arising from such practices.
Conclusion
The proportion of traditional eye medicine practice was high among ophthalmic patients in the West Bank. The most common TEM used was tea, followed by herbal products and vegetable slices (potato, cucumber, and onion). The current study confirmed that occupation and monthly income were predictors of using traditional eye medicine practices among ophthalmic study patients attending ophthalmic clinics in selected West Bank hospitals.
Footnotes
Acknowledgements
The authors would like to express their thanks to the patients who participated in the study
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.