
Abstract
Background:
Rate and pattern of under-five mortality is a reflection of a society’s healthcare system and quality of life. This study is aimed at reviewing the causes of infants and under-five morbidity and mortality in Calabar, Southern Nigeria.
Methods:
This study used retrospective descriptive cross-sectional design. We did a retrospective collation of data on under-five morbidity and mortality from 2012 to 2017 of under-five patients admitted or died while in admission in University of Calabar Teaching Hospital. The causes of morbidity and mortality were reported based on International Classification of Diseases 10 (ICD-10). The morbidity, mortality and fatality rates were computed.
Results:
A total of 11,416 under-five admissions and 391 deaths were recorded within the study period giving a fatality rate of 3.4%. Age 1–4 years category represented 50.5% of the admissions while infants (<1 year) constitute majority of the deaths (64.7%). There were 5652 infant admissions and 253 infant deaths giving fatality rate of 4.5% within the study period. Males constituted majority (55.8%) of under-five morbidity whereas females constituted majority (51.2%) of the deaths. Conditions originating from perinatal period; and infectious and parasitic diseases were the leading broad cause of under-five mortality. Specific disease analysis showed sepsis/septicemia; congenital infectious and parasitic diseases; slow fetal growth, malnutrition and short gestation as the chief causes of both infant and under-five mortality.
Conclusion:
The leading causes of under-five deaths in the studied population are amenable. Improved healthcare and antenatal will be of immense benefit.
Background
Under-five mortality (U5M) refers to death of a child before the age of five. 1 Consequently, under-five mortality rate refers to the probability of a child dying between birth and exactly 5 years of age expressed per 1000 live births. 2 In 2020, 5.0 million children under 5 years of age died culminating to approximately 13,800 under-five children dying per day. The global under-five mortality rate has declined by 61%, from 93 deaths per 1000 live births in 1990 to 37 in 2020; however, the rate still remains very high in sub Saharan Africa (average of 73). Specifically, Nigeria recorded under-five mortality rate of 114 per 1000 live birth, which is the second highest globally (just behind Somalia: 115/1000 births).2,3 Also, Nigeria was the highest contributor to overall under-five deaths in 2020 with 844,321 under-five deaths overtaking India (783,314). This accounted for 16.72% of global under five deaths in 2020. 4
Child mortality mostly occurs in the first year of life, and death in this period is termed infant mortality. Infant mortality refers to the death of an infant before his or her first birthday.5,6 Infant mortality in Nigeria remains high (72 per 1000 live births) - the fourth highest globally (just below Sierra Leone: 80, Central African Republic: 78, and Somalia: 73) and as well fourth in Africa in 2020. 7 Numerically, Nigeria contributed second (541,477) to global infant death in 2020 (only second to India: 647,688), accounting for 14.3% of all global infant deaths. 8
Most of the under-five mortality has been attributed to communicable disease such as malaria, measles, diarrhea, cholera, and respiratory diseases. 9 The World Health Organization has reported pneumonia, diarrhea, malaria, and pre-term birth compilations as the leading causes of under-five mortality in 2020. 10 Causes of morbidity and mortality are relevant parameters for documentation of geographical burden of disease and public health planning and assessing health policies.11,12 Socio-demographic factors such as maternal level of education, maternal inhabitation (rural vs urban), socio-economic status of the family and environmental factors has been documented to affect under-five as well as adult mortality.9,13 There is paucity of data on the causes of infant and under-five mortality in southern Nigeria. The few attempts were not specific on infants and under-five events.11,14,15 Hence, this study sets off to anastomose this gap by reviewing data on causes of death in infants and general under-five in a hospital located in Southern Nigeria.
Methods
Study design
We made use of retrospective descriptive cross-sectional design to analyze causes of infants and under-five morbidity and mortality in University of Calabar Teaching Hospital from January 2012 to December 2017.
Study location
The study took place at University of Calabar Teaching Hospital. University of Clabar Teaching Hospital is a tertiary health institution in Calabar, Cross River State (Niger Delta Region) of Southern Nigeria. Calabar metropolis is a fusion of Calabar Municipal and Calabar South Local Governments. The hospital has 410 bed space capacity with 15 wards and 11 clinics.16,17 Though there is no published data on annual deliveries in the center, there is more than 2000 deliveries annually in the center. 18
Study population
We analyzed data for under-five patients admitted or died while in admission from 2012 to 2017 and we excluded patients who were brought in dead.
Ethical approval
This study was approved by the Health Research Ethics Committee of University of Calabar Teaching Hospital.
Data collection
We retrospectively extracted demographic data and causes of morbidity and mortality from the Health Records Department of University of Calabar Teaching Hospital where they are coded based on International Classification of Disease-10 (ICD-10). The staff of the Health Records Department were responsible for allocation of the ICD coding. Trained research assistants were enrolled to extract the data into spread sheet.
Definition of variables
Statistical analysis
We analyzed the curated data using SPSS version 25 (IBM Corps, Armonk, NY, USA). Categorical variables were represented as frequencies and percentage. Fatality rates were represented using trend line graphs. Specifically, admissions and deaths were represented in both frequencies and percentages while fatality rates were represented in percentages.
Patient and public involvement
Patients and public were not involved in the study owing to the retrospective approach used.
Result
We observe a total of 391 under-five deaths arising from 11,416 admissions, giving an average fatality rate of 3.4%. Of these, were 253 infant deaths resulting from 5652 admissions giving rise to infant fatality rate of 4.5%. Males constituted majority (55.8%) of the under-five morbidities while females constituted majority (51.2%) of the under −5 mortality. The ensuing fatality rate was higher (4.0%) for the females than the males (3.0%). Similarly, males dominated (54.2%) infant’s morbidity as well as mortality (53.4%). However, females retained the higher fatality rate (4.6%). The overall fatality rate for 1–4 years category was higher in females (59.4%). While males dominated the admission (57.4%) in 1–4 years age category, the females took the lead in number of deaths (59.4%) (Table 1).
Frequency of morbidity and mortality of the studied population based on gender and age category.
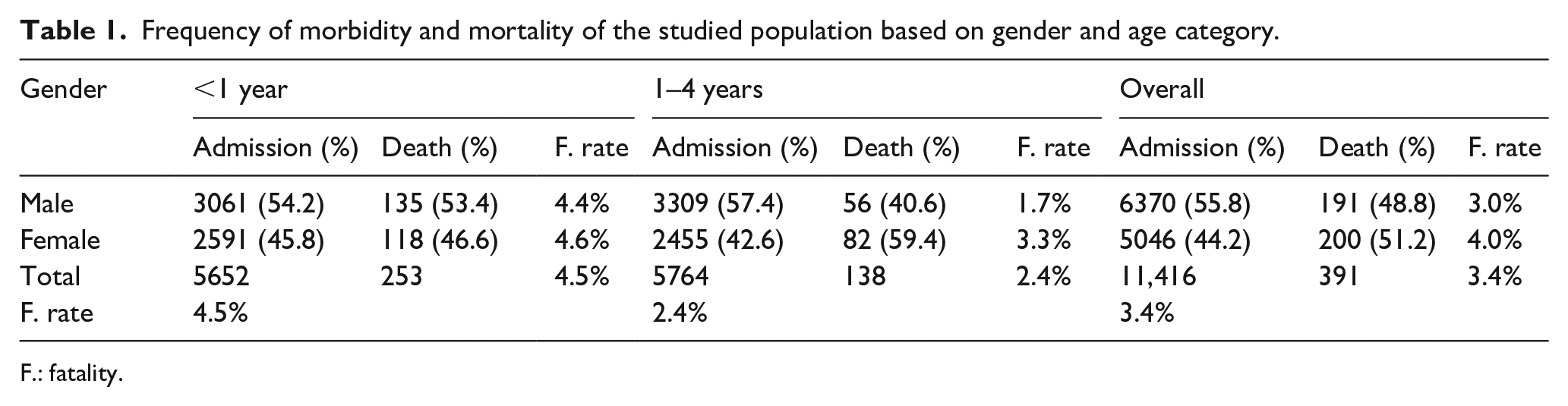
: fatality.
Figure 1 shows the trend of admissions and deaths of under-five children. There was a rise in admissions from 2012 which peaked in 2013 and declined till 2016. After 2016, the number of admissions increased till 2017. The number of deaths was fairly stable until 2015 when it declined to 2016 and rose again till 2017 (Figure 1).

Trend of admissions and deaths within the studied years (2012–2017).
The fatality rates for the years 2012, 2013, 2014, 2015, 2016, and 2017 were 2.0%, 1.9%, 3.0%, 3.7%, 0.1%, and 3.9% respectively. The trend was fairly stable from 2012 to 2013 but increased thereafter till 2015 before declining in 2016. There was a sharp rise after 2016 toward 2017 (Figure 2).

Fatality rates of the studied years (2012–2017).
Table 2 shows the distribution of morbidity and mortality of the under-five based on the broad ICD-10 categories. The broad ICD-10 leading causes of mortality are conditions originating in the perinatal period (27.6%), followed by infections and parasitic diseases (18.9%) and congenital malformations (7.9%). However, death per admission showed that diseases of the musculoskeletal system (21.7%) and neoplasms (17.5%) had the highest fatality rates. Concerning the infants, conditions originating from perinatal period (21.1%; n = 2407), infectious diseases (8.7%; n = 998) and respiratory system diseases (7.8%; n = 892) were the leading causes of morbidity while conditions originating from perinatal period (25.8%; n = 100); infections and parasitic diseases (9.0%; n = 35); and congenital malfunctions (6.1%; n = 24) represented the leading causes of mortality.
Distribution of causes of morbidity and mortality of the studied population by broad ICD-10 category.

ICD-10 classification, Adm.: admission.
Table 3 shows the distribution of morbidity and mortality data of the under-five children studied. Considering specific disease conditions, malaria (9.6%; n = 1094), Diarrhea and gastroenteritis (9.4%; n = 1068), acute pharyngitis and tonsillitis (7.6%; n = 899) and congenital infections and parasitic diseases (7.6%; n = 864) were the leading causes of under-five morbidity while sepsis/septicemia (7.4%, n = 29); congenital infections and parasitic diseases (5.1%; n = 20); slow fetal growth, malnutrition and short gestation (4.9%; n = 19); and Diarrhea and gastroenteritis were the leading causes of under-five mortality. Stratifying only the infants showed congenital infections and parasitic diseases (14.7%; n = 833); diarrhea and gastroenteritis (7.7%; n = 436) and pneumonia (6.9%; n = 387) were the leading causes of infant morbidity while slow fetal growth, malnutrition and short gestation (7.5%; n = 19), congenital infections and parasitic diseases (6.7%; n = 17), and sepsis/septicemia (6.3%; n = 16) were the leading causes of mortality. On the other hand, malaria (13.9%; n = 803), acute pharyngitis and tonsillitis (12.2%; n = 706), and diarrhea and gastroenteritis (11.0%; n = 632) were the leading causes of 1–4 years hospital admissions while sepsis/septicemia (9.4%; n = 13), malaria (8.0%; n = 11) as well as burns and corrosion (8.0%; n = 11) were the leading causes of 1–4 years mortality (Table 4). Disease of the liver (37.5%), acute nephritic syndrome (33.3%), renal tubule interstitial (18.8%) and burns and corrosion (16.9%) had the highest fatality rates among under-five children studied while acute nephritic syndrome (66.7%), renal tubule interstitial (42.8%), disease of the liver (37.5%), and HIV (18.4%) had the highest infant fatality rates (Table 3)
Distribution of causes of morbidity and mortality by broad ICD-10 classification and specific disease types.

Summary of the leading seven specific causes of mortality in the study.

Discussion
We observed a fatality rate of 3.4% with higher mortality and mortality rate in the infant population (4.5%vs 2.4%). Child mortality has been documented to occur more within 1 year of life.19,20
Conditions originating in the perinatal period, infections and parasitic diseases and congenital malformations constituted majority of the broad causes of mortality in under-five children. This trend is in consonance with reported global trend.1,2
Specific disease analysis showed sepsis/septicemia; congenital infectious and parasitic diseases; and slow fetal growth, malnutrition and short gestation; and diarrhea were the leading causes of under-five mortalities in this study. Onyeanugha et al. 21 and Ibeneme et al. 22 had both reported sepsis, malaria and diarrhea as the chief causes of under-five mortalities in Aba and Umuahia, Nigeria, respectively. On the other hand, Odejimi et al. 23 and Adewemimo et al. 24 reported malaria, diarrhea and pneumonia as the leading causes of mortality in north/southern Nigeria and 36 states of Nigeria, respectively. In a study done in Port-Harcourt in Nigeria, 20 George and colleagues reported HIV, bronchopneumonia and chromosomal abnormalities with cardiac effect as the leading causes of under-five death in Port-Harcourt while Abu et al. 25 reported malaria, complications of birth and measles as leading causes of death in Benue state, both being studies in Nigeria.
Studies performed in other African countries showed that malaria, diarrhea and pneumonia were the leading causes of U5 death in Ghana 26 while that in Kenya reported malaria, respiratory infections and anemia as the chief causes of U5 death. 27 Abraha et al. and colleagues in Ethiopia reported sepsis, prematurity and intestinal infectious diseases as leading causes of U5 death in Ethiopia, 28 while Agborndip et al. and Libwea et al.29,30 reported birth asphyxia, prematurity, sepsis and malaria, meningitis and sepsis, respectively as leading causes of U5 mortality in Cameroon. However, global data have preterm birth complications, birth asphyxia/trauma, pneumonia, diarrhea and malaria as the leading causes of U5 mortality. 31
Irrespective of the order, sepsis/septicemia; congenital infectious and parasitic diseases; and slow fetal growth were the three leading causes of mortality both in infants (infant mortality) and under-five (under-five mortality). These are followed by diarrhea and pneumonia. Sepsis/septicemia has been implicated as a chief cause of both adult and under-five mortality. 11 Sepsis is a life-threatening organ dysfunction caused by dysregulated host response to infection11,32 with bacteria being the most implicated, though fungi have been involved.33,34 Congenital infections and parasitic diseases refer to the vertical transmission of pathogens/parasites from the mother to the newborn. 35 Congenital infectious and parasitic diseases together with slow fetal growth, malformation and short gestation are complications originating in the perinatal period. On the other hand, diarrhea and gastroenteritis are attributed to rotavirus, Novovirus, Campylobacter, E.coli, Salmonella and more. 36 Pneumonia (acute lower type) could be caused by bacteria, virus, and fungi. Malaria is caused by infection with protozoan parasites belonging to the genus plasmodium transmitted by female Anopheles mosquitoes. 37 The infectious diseases noted above (Sepsis/septicemia, diarrhea, and malaria) can be prevented by less expensive means such as improved personal hygiene (sepsis/diarrhea) and use of insecticides treated nets (malaria). On the other hand, most of the conditions originating in the prenatal period can be prevented or at worst anticipated via adequate antenatal care attendance. 38 Consequently, the majority of the leading causes of U5 and infant mortality above are amenable mortality: deaths as a result of causes that otherwise shouldn’t result to death in the presence of effective medical practice. 38 This reflects low assess to quality health care in the studied population. 11 Amenable mortality are indicators of national levels of personal health care access and quality.11,39,40 This observation could be attributed to low expenditure on health as majority (76.1%) of health expenditure in Nigeria are via out of pocket, 41 consequently translating to low access to medical care including antenatal visits.
The causes of infants and under-five mortality are key indicators of the health care status of a society and convey quality of life. 19 Addressing the key causes of child mortality is key in attaining Sustainable Development Goals (SDG) three which aims at reducing infant and under-five mortality as well as end preventable death. 41 We thus make a call on policy makers in Nigeria to make and implement policies geared toward improving standard of living and access to healthcare.
Notwithstanding, the result of this study may be potentially prone to varying limitations, considering the study took a retrospective approach, certain inherent limitations of retrospective studies such as selection bias may not be ruled out. Secondly, autopsy is not routinely done in the study area (except in cases of jurisprudence or conflict), hence, causes of deaths were based on clinical and ancillary investigations.
Conclusion
This study shows that conditions originating in the perinatal period and infectious diseases to be the major broad causes of under-five mortality. Specific disease analysis showed sepsis/septicemia; congenital infections and parasitic diseases; slow fetal growth, malnutrition and short gestation; diarrhea and gastroenteritis; pneumonia and malaria were in the fore front of causes of under-five and infant mortality in the studied area.
Footnotes
Acknowledgements
Not applicable.
List of abbreviations
ICD: International classification of disease
U5: Under-five
SDG: Sustainable development goals
Authors’ contributions
Conceptualization: HUO. Data curation: HUO, UOE, IKU. Data interpretation: HUO, UOE, IKU,CPE, AFN, KA, NPN, EAU, KA. Validation: CPE, HUO, KA. Statistical analysis: HUO. Initial manuscript draft: HUO, EAU. Editing: UOE, CPE, NPN, IUM and SOA. All authors read and approved the final manuscript draft.
Availability of data and materials
Data sets generated in this study are available within the manuscript.
Consent for publication
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was approved by the Health Research Ethics Committee of University of Calabar Teaching Hospital.