
Abstract
Tobacco use and exposure has been known as one of the leading causes of premature mortality worldwide. Tobacco control measures have been considered one of the strategies for reducing the burden of NCDs, improving public health, and strengthening the health system’s response to threats and pandemics. The State of Qatar has put tobacco control a national public health priority as it has adopted various tobacco control measures that the WHO classified as high-impact measures. This has resulted in achieving tobacco control milestones which led to constant monitoring of tobacco use and the provision of smoking cessation services at all healthcare levels. However, there is still much work to be done to fill the gaps and respond to the emergence of novel tobacco products and market strategies in an effective way. This review highlights the status of tobacco use and exposure in the State of Qatar, and focus on the progress, and challenges in the implementation of tobacco control policies and smoking cessation services between 2002 and 2022.
Introduction
Tobacco use and exposure is one of the biggest public health epidemics that lead to many preventable diseases, including cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes for both the tobacco users and those who exposed to the secondhand smoke. 1 This put tobacco use and exposure as major cause for premature death. Globally, 1.18 billion people regularly smoked some form of tobacco, causing 8 million deaths a year, including around 1.2 million deaths from exposure to secondhand smoke.1,2 Although there has been a steady decline in any tobacco use during 2000–2020, the annual mortalities can be expected to keep increasing in some regions. 3
The direct and indirect costs of the tobacco attributable diseases put significant economic burdens on health care systems and governments. It is estimated that the total cost of smoking accounted for 1.5%–6% of national health expenditure and 0.22%–0.88% of GDP of countries. 4 Therefore, tobacco control measures have been considered as the best investment for improving global health. 5
The WHO Framework Convention on Tobacco Control (FCTC) is an internationally negotiated, legally binding package of measure to reduce the harms of tobacco through evidence-based measures intended to increase the awareness and reduce the demand and supply of tobacco. In 2008, the WHO has introduced a set of six cost-effective and high impact measures under the acronym of MPOWER to help countries in tobacco control. These measures include
In six Arabian Gulf countries, it is estimated that the prevalence of tobacco smoking among adults ranged from 7.8% to 19.3%, with a higher prevalence among males with a growing number of female youths who were willing to initiate tobacco use.8,9 In 2016, the economic burden of tobacco uses in these countries accounted for approximately $34.5 billion. 10
This review highlights the status of tobacco use and exposure, the progress, and challenges in implementation of tobacco control policies and the smoking cessation services in the State of Qatar, one of the Arabian Gulf countries.
Epidemiology of tobacco use and exposure in Qatar
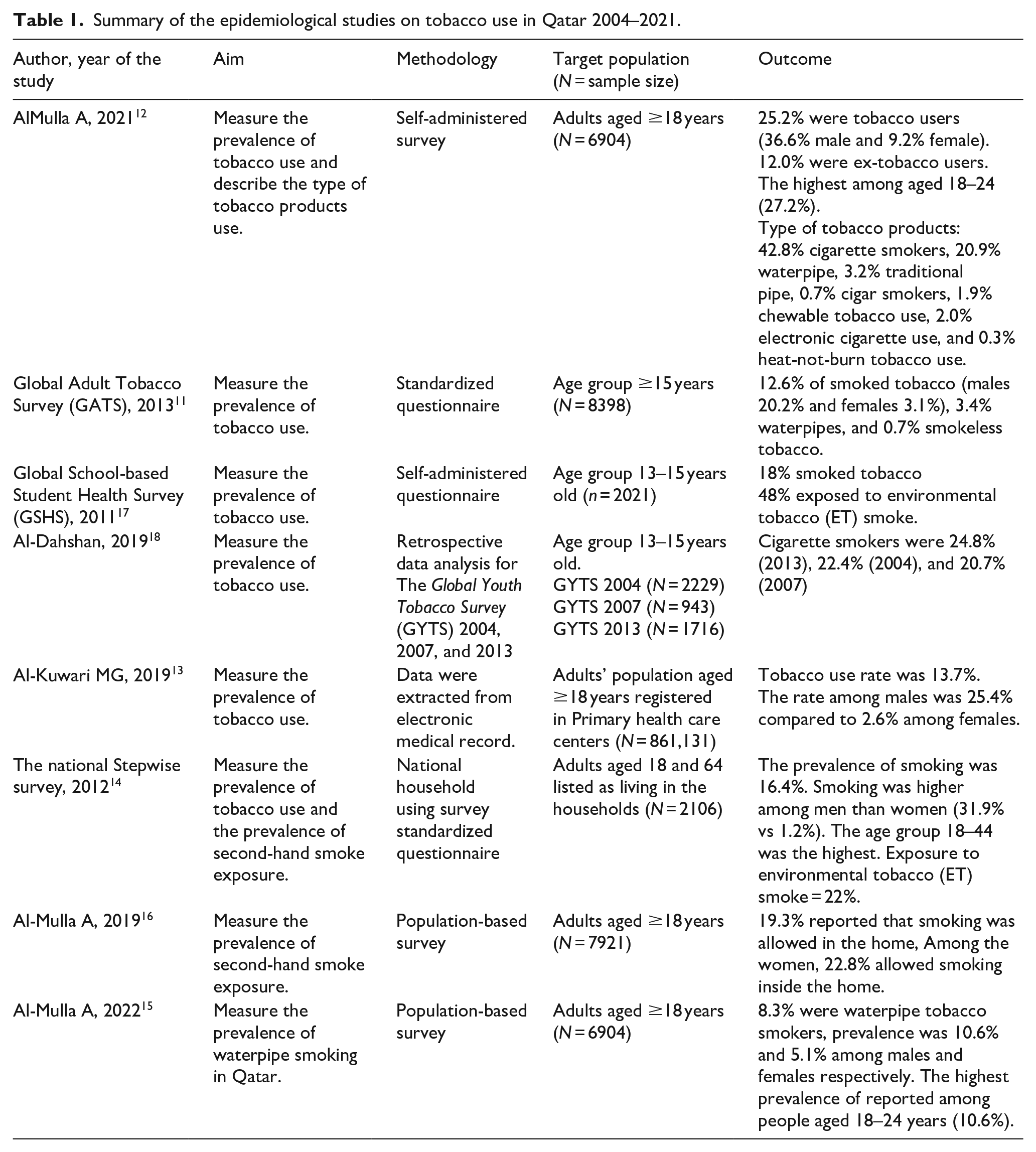
To implement and evaluate effective tobacco control interventions in the country, FCTC encourage countries to collect and share national data on the magnitude, patterns, determinants, and consequences of tobacco use and exposure. Between 2004 and 2021, Qatar reported tobacco use and exposure to secondhand smoke in different national surveys targeting adolescents and adults, as shown in Table 1. The adult surveys reveled that the prevalence of tobacco use ranged between 12.6% and 25.2%, with the highest tobacco use rate were found among males.11–14 However recent reports that tobacco consumption among females reached to 9.2%. 12 Young adults group 18–39 year reported tobacco use more than other age groups.12,14 A recent survey in 2022 reveled that the prevalence of waterpipe smoking was 8.3%. The prevalence of waterpipe smoking among males was twice the prevalence among females (10% vs 5%), which clearly show the tolerance of using the growing trend of using waterpipes among females. 15
Summary of the epidemiological studies on tobacco use in Qatar 2004–2021.
The status of tobacco control policies in Qatar in 2022.

The surveys in the last few years have been updated to include all the tobacco forms. The surveys showed that the smoked tobacco forms, for example, cigarettes, waterpipe, and cigar remain the main form among population in Qatar. Smokeless tobacco, for example, chewable tobacco and E. cigarette didn’t exceed 2% according to the national studies.11,12
Few studies measured the prevalence of the exposure to secondhand smoke. In 2012, the national STEPwise survey showed that 22.2% of the sample were exposed to environmental tobacco smoke at home. 14 A recent study published in 2019 showed the exposure to secondhand smoke was 19.3% among general population and increased to 22.8% among females. 16
Health authority conducted specific national surveys such as The Global Youth Tobacco Survey (GYTS) and Global School-based Student Health Survey (GSHS) to monitor the tobacco use among adolescents. The prevalence of tobacco use ranged between 18% and 24.8% especially among males.17,18 The GSHS revealed that the exposure to secondhand smoke among adolescents was 48%. 17
Although that review summarizes different surveys with different age groups and include different types of tobacco use. Gaps in some data remains as one of the main challenges is the sustainable implementation of community-based surveys such as monitoring the use of e-cigarette and smokeless tobacco. Also, the new trend of tobacco use needs to be well-studied especially among females and adolescents. Another challenge is assessing the knowledge and attitudes about the harms of the e-cigarette, heated tobacco, and chewing tobacco as they could be used by smokers as alternative to Cigarettes and waterpipes.
Implementation of tobacco control policies
Qatar was one of the first countries in Arabian Gulf to sign and ratify the FCTC during 2003–2004 and entered into force in 2006, 19 as shown in Table 2. Before that, the government has started some tobacco control legislative measures. The first measure was imposing the smoke free policy in the governmental health care premises in 1996, followed by law to increase the custom duties on imported tobacco products. 20 In 2002, Qatar issued the first comprehensive tobacco control law that encompasses a range of legislative measures starting from smoking bans in enclosed public places, banning advertising for tobacco products, and prohibition of selling tobacco products to minors. 20
Beside Bahrain, Qatar has comprehensive implemented FCTC measures compared to the other neighboring countries since 2006. 19 The smoke free policy has been implemented in indoor public places, with a 200 Qatari Riyals (QARs) fine for non-compliance, which is equivalent to 54.8 USD, as shown in Table 2. The country has banned all forms of direct or indirect advertisement of tobacco products and sponsorship of the events by tobacco industry. In 2019, the total taxation on tobacco products has been increased to 100% of retail price. 19 Nevertheless, the price of most sold brand (pack of 20 cigarettes) reminds affordable at 22.0 QARs (6.0 USD), while the cheapest brand price has been increased from 9 QARs (2.4 USD) to 14 QARs (3.8 USD). 21
All tobacco retail stores were required to post signage stating legal age ≥18 of purchasing tobacco. The pictorial warning standard that mandates presence of combined text and picture warning to occupies no less than 50% of the front and back of the tobacco products package has been introduced in 2012. However, the pictures used remain unchanged since the 2012 22 as shown in Figure 1.
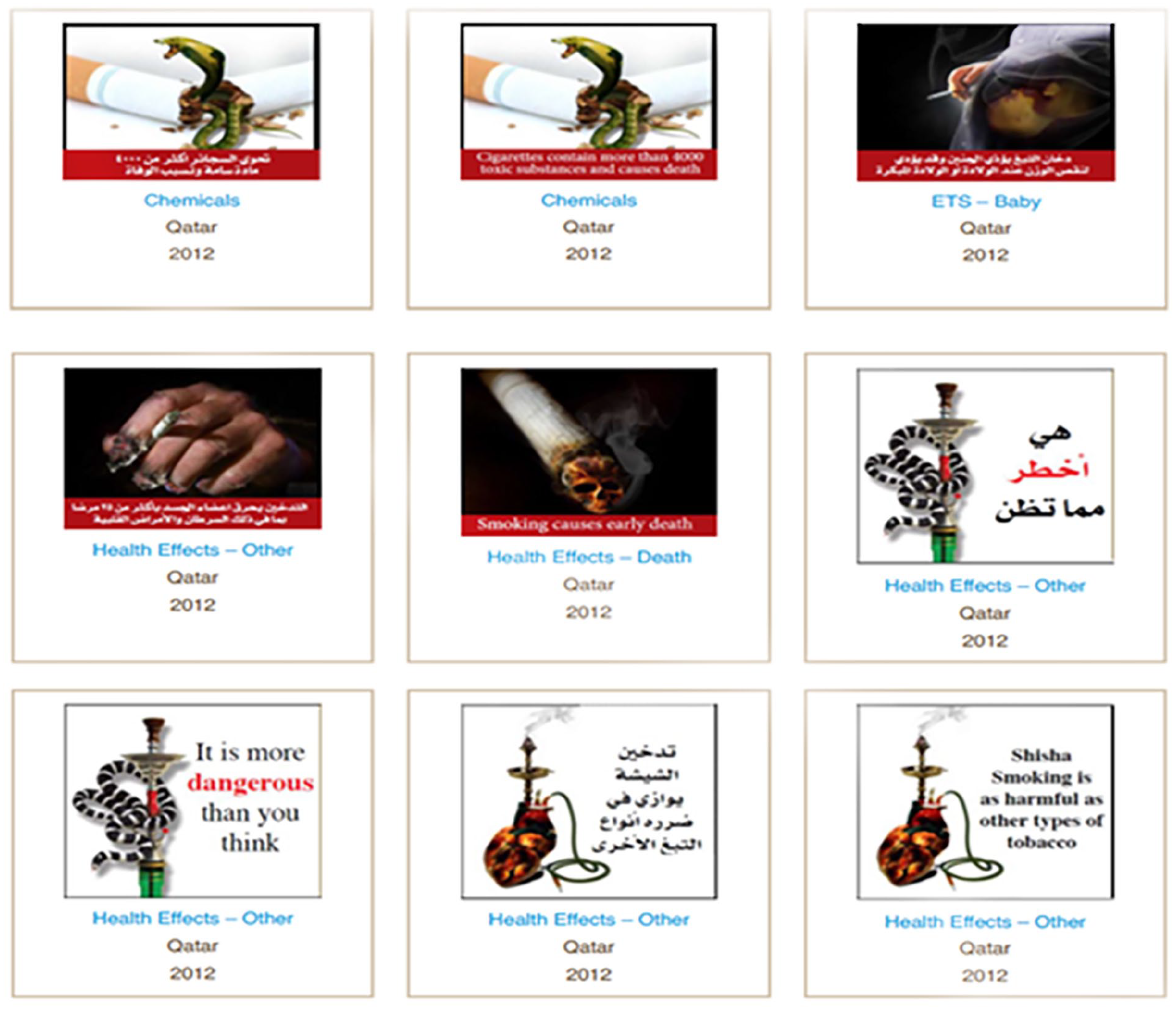
Labels of tobacco product packages, Qatar.
With the global increased use of electronic nicotine delivery systems (ENDS), for example, e-cigarettes and vaping devices, or vape pens especially among youth, 23 Qatar’s tobacco control law addresses some aspect to control the e-cigarettes. The Qatari law bans the import, display, sale, distribution, and manufacture of e-cigarettes but it doesn’t address the situation of using e-cigarettes in indoor public places, workplaces, or public transportation. 21
Based on the WHO reports on the Global Tobacco Epidemic from 2011 to 2019 on the activities of all countries in implementing the various WHO FCTC policies, Qatar one of six countries in the EMR scored more than 75% of the score in implementation on MPOWER. Qatar showed continuous improvement from score of 18 out of 37 in 2011 to 28 in 2019, with more improvement achieved in pictorial health warning and enforce ban on tobacco advertising. While areas such compliance to the smoke free policy and smoking cessation programs needs improvement. 24 For instance, updating the policies to include e-cigarettes will be important proactive step to control tobacco use among the new generation. Assessing the impact of pricing and taxation on the affordability of the tobacco products among different social levels will be good indicator for the effectiveness of that measure on high income community.
Smoking cessation services
Smoking cessation services was first introduced at hospital level in 1999. Then the service has been introduced to the primary health centers in 2011 with one clinic in one health center and expanded to 16 clinics in different health center in 2022. About 26 physicians have been trained on tobacco dependence treatment. The governmental health providers in primary health care centers and hospitals offers the smoking cessation medications free of charge and this includes bupropion, varenicline, and different forms of nicotine replacement therapy (NRT), for example, as nicotine gums, lozenges, and patches. 25
While the recommendations stressed on the importance of integrating smoking cessation services in different health care setting, primary care settings have been identified as important sites. In Qatar, the reports showed that the tobacco control center in the secondary care has an annual average of 1200 smoker patients who receive smoking cessation services. 26 Although expanding the smoking cessation service in primary care has offered a good accessibility to the patient with of annul average of visits ranging from 3200 to 3800 visits according to the report from 2019 to 2021, still the indicators showed the low uptake.27,28 Since primary care introduced the electronic medical records in 2015, the primary health care centers received visits from 81,202 smokers’ patients, only 4784 (5.9%) of them have utilized the smoking cessation services with high loss of follow up rate (50.8%).27,28
Smoking cessation programs still need more improvement to increase utilization and to decrease the no show rate and loss of follow up. A recent survey showed that only 22.5% of primary care physicians reported they always asked patients about smoking status and documented it in the patient record. 29 This supports considering tobacco use in the diagnosis list in the electronic medical records will help health care providers to advise patients to quit, assess their readiness and provide them the support and referral to smoking cessation service once the patients show their readiness to change.
Following up the patients in smoking cessation services is challenging with high relapse rate, particularly in the first 6 months. 30 Although the national guidelines stressed on the frequency of the follow up visits, using teleconsultation during Covid-19 pandemic provide good method to close follow up the patients.25,31 This might be used as a tool to reduce the loss of follow up and no-show rate among smoker patients. On the other hand, with the absence of the data on the quit rate, smoking cessation services in Qatar need to measure attempts rate and quit rate as part of their indicators to regularly monitor the outcome.
Conclusion
Over the last 20 years, there have been tremendous strides made in tobacco control in Qatar. The adoption of MPOWER measures such as taxation, health warning, and offering help to quit has seen inspiring progress. However, prevalence of tobacco uses and exposure still remains as major public health problem that needs more collective efforts of tobacco control at all levels.
Despite that, there have been challenges in implementation of tobacco control policies and uptake of smoking cessation services. This review highlight some of the recommendations to achieve better practice of tobacco control measures. At the policy level, expansion of free tobacco policy to include all public/indoor places as well as emerging tobacco products such as e-cigarettes is highly recommended. In addition, monitoring of all forms of tobacco use and exposure in the community still considered of utmost importance.
At the smoking cessation service level, the providers should adopt service enhancing strategy to increase the uptake and reduce the loss of follow up such as use the appointment reminder system, establishment of the help line, smoking status as vital sign, and expand use telephone consultations to increase the follow up especially in the early phase of treatment. The health authority needs to continue the community awareness and to educate population more on the effects new tobacco products and secondhand exposure. Lastly, researchers in Qatar need to conduct further research on prevelnce of e-cigarettes use and the evaluate quit rate among the users of the smoking cessation services.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.