
Abstract
Background:
According to the studies conducted, teen pregnancy and its related health issues are among the most significant issues. The purpose of the study was to develop a musculoskeletal health intervention training programme using an intervention mapping approach (IMA) for teenagers aged 12–14 years old.
Methods:
The present study is a study protocol where IMA has been used as a planning framework for developing a musculoskeletal health intervention training programme. Six steps of the intervention mapping process have been completed in the study. As the first step, needs assessment has been performed through systematic review and qualitative evaluation. In the second step, a matrix of change objectives was designed. Later on, after designing the programme and planning its implementation, the programme evaluation plan was developed.
Results:
IMA guided us in designing and implementing a control-oriented training programme with the participation of the participants, along with the definition of outcomes, performance goals, and determinants, theoretical methods, practical applications, an intervention programme, implementation, and step-by-step assessment.
Conclusion:
Intervention mapping is a participation-based approach to designing and implementing promotion programmes.
Introduction
According to the statute of the World Health Organisation (WHO), health is considered one of the most obvious human rights and needs. 1 Teenage is one of the most significant periods in every person’s life.2,3 According to a report by the WHO, one out of every five people is an adolescent. 4 Today, the backpack is one of the most popular kinds of bags among teenage students, which has been noticed by many researchers from different aspects since the backpack is one of the most important factors that creates musculoskeletal injuries in teenage students.5–8 A heavy backpack makes a person arch his or her back more than usual or bend his or her head and pull his body forward to tolerate the weight of the backpack. And the pressure on the muscles of the neck and back can cause fatigue, injury and, finally, anomalies of the spine. 9 The American Academy of Orthopaedic Surgeons stated that the properties of a good backpack are having two shoulder straps, back pads, a waistband, a low weight and wheels. 10 In different ages, the effect of cargo transportation has varied. During 12–14 years old, the spine is growing rapidly, and any kind of stress on the spine manifests itself as pain and discomfort. 11 These studies showed that when the weight of backpacks exceeds the specified standard, it leads to pain in the back and upper parts of the body. Also, carrying these bags, in the long run, leads to drooping shoulders and kyphosis. 12
In recent years, carrying and using tools and backpacks have been considered risk factors for musculoskeletal disorders.13–16 The findings of some studies show that between 40 and 88% of students complain about the pain on their shoulders, neck and back when they carry their backpacks. Moreover, between 30 and 80% of them believe that their musculoskeletal problems are related to carrying backpacks. 13
Training is a process that bridges the gap between health information and behaviour, and given the relationship between knowledge, attitude, and performance improvement in an intervention-training process, the significance of proper information provision and the provision of learning opportunities for teenage students becomes evident. 17 When designing a targeted intervention programme, it needs to use an evidence-based planning framework and the theory and curriculum for adolescent special education programmes. Different models have been developed by experts for the design, implementation, and evaluation of training programmes, one of which is the intervention mapping approach (IMA). 12 This approach is a planning approach based on the significance of developing evidence-based programmes that assess and intervene in health-related issues. 13
IMA aims to provide guidelines for effective decision-making during the development and adaptation of an intervention, integrating theory, empirical findings, and information from the target population. It also has a problem-solving-based approach and enables the implementation of the programme through six steps: need assessment, objectives matrix design, selection of theory and practical application-based intervention methods, production of components and materials of the intervention programme, adoption planning, implementation, sustainability and evaluation. 17 During a review of the literature, the studies conducted were intervention-oriented and according to the researcher’s designed protocol, and the intervention based on intervention mapping, which is based on the needs of the audience, has not been conducted in the field of musculoskeletal health of teenage students in Iran. This approach focuses on behavioural change and the individuals who are influential on the behaviour of those at risk, known as environmental agents, and individuals’ health issues at different ecological levels to make changes.15,16,18,19 The aim of the current study is to prepare an intervention plan to reduce musculoskeletal damage due to the use of a backpack in teenage students aged 12–14 years.
Methodology
Study design and study population
The present study is a description of a study conducted to develop a training-intervention programme using IMA in teenage students aged 12–14 in the year 2022. Intervention mapping has six steps and some tasks at each step, where the basic processes are used in completing each step to benefit from theories and models.
Step 1: Needs assessment
The researchers conducted a needs assessment based on the PRECEDE/PROCEED model (Predisposing, Reinforcing and Enabling Constructs in Educational Diagnosis and Evaluation. Second is an ‘ecological diagnosis’ (PROCEED, which stands for Policy, Regulatory, and Organisational Constructs in Educational and Environmental) to figure out what factors the programme should address.
In this step, data were collected through a literature review, focus group and in-depth semi-structured interviews. Three focus groups consisting of beneficiaries and influential people were first formed, and in-depth semi-structured interviews were then conducted with 10 parents, 5 School health care and 15 representative of teenage students 12–14 years to explain their opinions on barriers and strategies to reduce them, barriers and solutions to reduce them, facilitators, influential factors and supportive policy changes. Next, the literature was reviewed to identify determinants and strategies for successful interventions to teenage students’ musculoskeletal health. Finally, the current situation of 474 to teenage students was investigated and additional data was provided by researcher-made questionnaires including demographic variables, questions about predisposing factors (awareness and self-efficacy) enabling factors (getting a suitable backpack), reinforcing factors (encouragement) and policies and regulations (support organisational and environmental factors). First, the city was broken up into five areas: North, South, East and West, and Centre, and then through randomly selection, a number of clusters (high schools) proportional to the population of each region were selected. Finally, 474 students were selected randomly. The validity of questionnaire was determined by two methods of face validity and content validity, which confirmed by experts of health education, psychology, reproductive health. The total content validity index (CVI) in the ‘relevancy’, ‘simplicity’ and ‘clarity’ respectively equals 82.6, 92.9 and 90.7. The reliability of the questionnaire further evaluated through internal consistency (α = 0. 83) and test retest (r = 0.82).
Step 2: Matrix (identification of outcomes, performance objectives and change objectives)
The next step in the process involved the detailed specification of outcomes for the intervention. 20 Following the specification of outcomes, performance objectives for each of the specified outcomes were defined. Performance objectives are a means of identifying the precise behaviours that must occur to achieve the specified outcomes. The final stage in this process required that the objectives of the intervention be stated in terms of the actual changes that need to occur in the theoretical determinants of behaviour. This is vital as it allows the intervention developer to identify the exact constructs that need to change to have an effect on the performance objective and the programme outcome as a whole. 21 This process resulted in a matrix specifying the performance objectives, the theoretical determinants of that behaviour, and the change objectives. 22
Stage 3: Selecting methods and practical strategies
In the third step, while the planning team predicted the ideas of the plan, the theoretical methods affecting the determinants of change were selected, practical solutions were selected, and the evaluation programme was designed to implement the predicted theoretical methods.
Step 4: Programme production
At this step of designing the intervention programme, while holding a group meeting with the participants and considering their priorities and suggestions, the implementation, scope and implementation sequence themes of the programme were identified, along with the constraints. For instance, if one part of the programme had been planned for the school programme during the school year, the resources needed by the principal and teacher, along with the financial constraints of the programme and the stages of programme implementation, were determined. The planning team then decided on the intervention methods to achieve the goals of change and finally pre-tested the messages and other parts of the programme before final production.
Step 5: Programme implementation
At this step, the tasks of each person and what they need to do to make sure the goal is met and implemented in a good way were set. Then, similar to Step 2, matrix planning was defined to guide the intervention programme. In this matrix, the operational goals and determinants were determined for the adoption, implementation and maintenance of the programme. For instance, determinants responded to the question, ‘Why do decision makers decide to use the programme, and why do those in charge try to make sure the programme continues over time?’ The answers to these questions determine the adoption, implementation and maintenance of the programme.
Stage 6: Evaluation planning
In the final step, the assessment programme was defined to determine the effectiveness of the programme, and the extent to which the performance goals and objectives had been changed. Assessment questions were identified from the defined outcomes and objectives, and a criterion was identified at 19. The results of the first step need assessment. The results of a review of studies (15 related papers) showed that students’ knowledge of how to use a backpack and related injuries was low. Moreover, the majority of teenage students do not have a proper definition of a backpack or how to use it, or a variety of backpack bags. In this study, mothers and school health educators were the most reliable channels of information transmission.
Results
Results of the first step
Key findings emerged from the needs assessment
The first step of the intervention mapping process, conducting a needs assessment, is to identify the health problem and its related behavioural and environmental determinants for the at-risk population. The results were categorised into three outcomes: 1. Increasing student information about backpacks and musculoskeletal injuries 2. Increasing student information about all kinds of backpacks 3: Proper use of backpacks. Also the literature review suggests that there are a range of barriers. This mapping process revealed that the main barriers fell into the theoretical categories of knowledge, beliefs about capabilities (self-efficacy), environmental context, and resources. Facilitators reversal of these barriers; for example, if a barrier was a lack of knowledge about healthy behaviour about musculoskeletal health and how to use a school bag, a facilitator would be improved knowledge of what healthy behaviour about musculoskeletal health is or how to use a school bag, of course in simple language. However, other facilitators included the use of rewards, such as sticker charts for children.
1. Increasing student information about backpacks
The weight of the backpack and musculoskeletal symptoms related to backpack carriage on student. 21 Also, back pain is a common affliction and a leading cause of disability in adults, but only recently has back pain been documented in teenage students. 23 Ergonomics awareness and posture training are important preventive approaches to back pain. It is important for teenage students to learn about the structure of the spine and back care. 21 One common suspect for back pain in children is the school backpack, which has also received a great deal of attention in the past few years. 24 A study in Italy found that the average load of a student’s backpack was 22% of the student’s weight and that 1/3 of the students surveyed carried excess of 30% of their body weight at least once per week; their point prevalence for reporting back pain was nearly 16%. The estimated lifetime prevalence is 48%. 25
2. Increasing student information about all kinds of backpacks
A backpack is a cloth sack put on somebody’s back. It usually has two straps that go over the shoulders. People often use backpacks on camping trips, hikes or any other form of outdoor activity where they need to carry many things. Backpacks are also being used in the military by soldiers. It can also be used for school, or in this case, it is also called a book bag or backpack. 5 It is important to increase students’ knowledge of the types of backpacks and standard backpacks because most students choose their backpack according to its appearance, and studies show that most bags and school backpacks are not standard. 26
3. Proper use of backpacks
When the backpack load is greater than the carrying capacity of the muscled teenage students, there is overhead, reflecting on the spine, causing pain, structural changes or dysfunction 9 Special attention has been paid when the weight is more than 15% of their body mass. According to the Italian Backpack Study, in Italy, students carry backpacks with 22% of their body weight, and 34.8% of them carry backpacks with weight corresponding to 30% of their body weight, at least once a week, exceeding even the proposed limits for adults. They found that when carrying a backpack with a load of 15% of body weight major changes occur in the angles of the head and neck, which affect the posture. 25
Results of the second step
At the start of this phase, the planning team wrote the performance goals based on theories of planned self-efficacy and the three individual outcomes of the programme. Then, they got help from a three-person group, including a health education specialist, an adolescent psychologist and a health educator, to evaluate the validity, and based on their views, the drafted performance goals were revised (Tables 1 and 2).
(a). Individual-level matrix the first behavioural consequence: Increasing teenage student’s information about backpacks.

Interpersonal level matrix behavioural outcome: Positive family support.

Performance objectives
In order to specifically target behavioural change among teenage students, the research team next identified performance objectives that would clarify the exact behaviour and performance expected of an individual affected by the intervention. In this case, they asked themselves what the target population exposed to the intervention must do in order to engage.
Determinants of musculoskeletal health
Once the target behaviour and performance goals were set, the next step was to find the determinants, or the factors that were found to be linked to the behaviour. The research team undertook a review of the available evidence about determinants contributing to musculoskeletal health. Knowledge, beliefs about capabilities (self-efficacy), environmental context and resources were the most important determinants. Tables 1 and 2 provide an example of the matrix of the performance objectives, which is to plan musculoskeletal health.
Results of step three
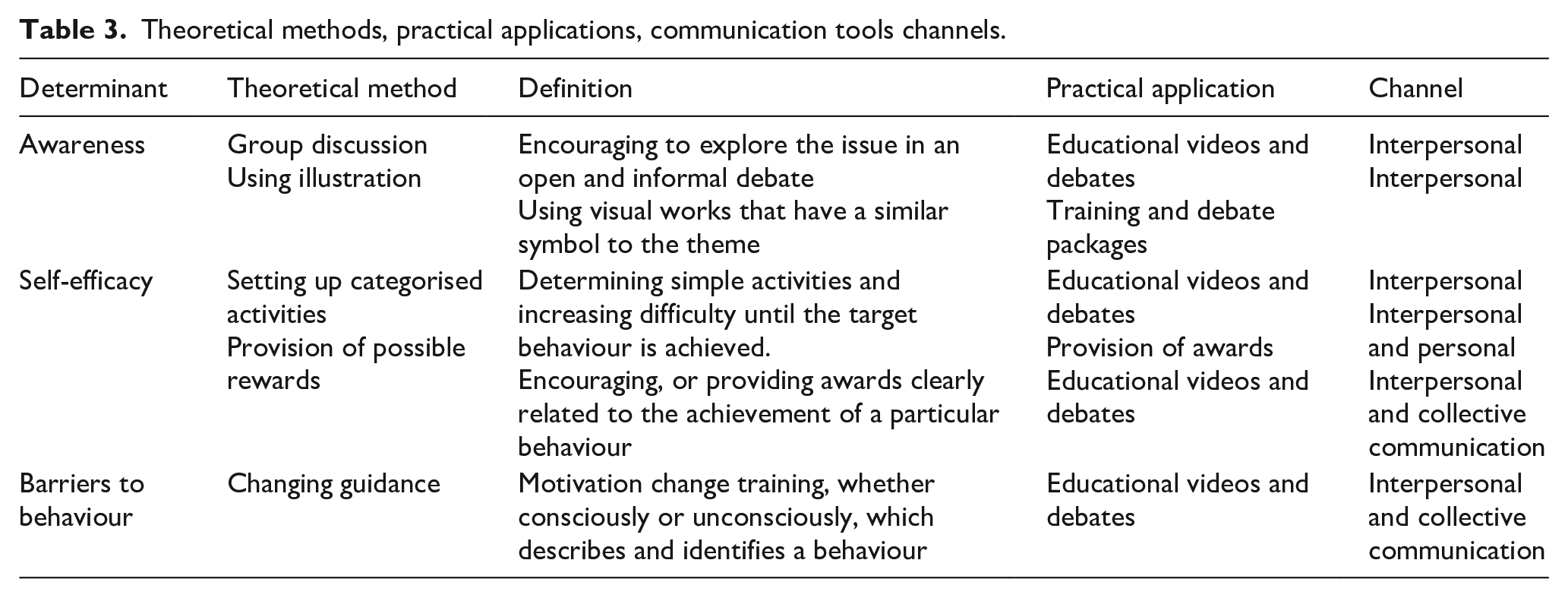
In this step, the theoretical methods and practical applications for each determinant were defined with the participation of the planning team (Table 3). When examining various behavioural theories that addressed behaviour barriers,2,4 the third step in intervention mapping consists of determining which theories and theoretically based methods would be most effective in achieving the intervention’s performance objectives and then deciding which practical strategies would best operationalise those theoretical methods. Considering these theoretical determinants, it was decided that practical strategies, such as using workbook activities and work/note books to allow mothers or teenagers to specify a series of implementation steps for healthy behaviours and encouraging the use of reminders and environmental cues to prompt healthy behaviours, may be useful. Furthermore, leaflets can be used to convey the costs and benefits of engaging in healthy behaviours not engaging.
Theoretical methods, practical applications, communication tools channels.
Results of step four
Step 4 of intervention mapping entails determining the scope and sequence of the intervention’s components and producing the materials for the intervention.27,28
The programme development involved two groups of people, including programme developers and health workers. The programme developers were recruited from the University of Medical Sciences on the basis of their expertise in curriculum development and experience in developing programmes related to musculoskeletal health. Health workers came from the University of Medical Sciences, the Department of Education or the school representative. These parties formed a programme development team that met on a regular basis to review progress on the programme development process until the programme was produced. The programme comprised five lessons delivered in five sessions over 7 h. The lessons were delivered in two modes. First, there were classroom sessions involving teacher and mother group discussions, story telling, role-plays, motion graphics and handbooks. Secondly, teenagers were given homework book (these books were prepared by experienced people) assignments to be accomplished at home with the help of mothers. Mothers were informed of the homework assignments by letters that were sent through their children. The aim of the homework book assignments was to foster. The plan involved implementation objectives, methods and strategies. The planning team involved researchers, teachers, students, and government officials from the health and health care fields. Prior to programme implementation, mothers and teachers were trained on the content and facilitation skills. Training activities included the administration of pre-test and post-test assignments. These were aimed at measuring teachers’ knowledge about teenagers and musculoskeletal health. The training programme was also used to pre-test the programme materials as well as teaching methods and strategies among mothers and teachers. Teachers were asked to comment on the attractiveness, completeness, suitability and relevance of the programme materials and methods to teenagers. A professional graphic designer was employed to draw illustrations to enhance their attractiveness and ease of understanding for the teenagers. The students, for example, advised on the suitability of the learning materials, while teachers advised on the appropriate time and mode of programme implementation. The health workers played a key role in that they were relevant to the social-cultural context of the implementation setting.
Results of step five
It has been recommended that health promotion interventions should provide a community-based intervention with regard to the universal intervention, and it was decided to deliver the intervention through officials and school health workers that already have regular contact with mothers and teenagers. In respect to the targeted programme delivered through parenting programmes, it was decided that the parenting programme facilitators would be best placed to deliver the intervention. 29
Results of the sixth stage
Since one of the significant goals of evaluation is to use evaluation results, 27 at this stage, the planning team identified the evaluation stakeholders, such as planners, study participants, programme managers and executives, to evaluate the effect of the programme and designed questions based on outcomes, performance goals and individual and environmental determinants (Table 4). In this study, 30 students were selected to participate in the performance. Those included attended training sessions for 4 weeks, once a week 29 (not more than 5% of participants should have been absent in each training session).
Evaluation of outcome, effect and programme process (sample questions).

Curriculum index: Individual and interpersonal performance change was determined. According to the studies conducted, the mothers and teenage students’ behaviour improvement index was considered to be 30% over one period of programme implementation. 28 Then, a measurement tool was designed to evaluate the outcomes, behaviours, and determinants at the personal and interpersonal levels. The evaluation programme was implemented 3 months later, and to examine the changes made, the experimental study design with randomly dividing the participants into intervention and control groups was used. 27
Discussion
This programme was done to design and develop how to use a backpack and reduce teenagers' musculoskeletal damage through a training programme using IMA. The results indicated that IMA is a good step-by-step framework for developing community-based programmes for teenage students. Moreover, IMA provides a practical and usable guide to adapt and promote health promotion programmes for other planners to be used elsewhere. 30 It has to be noted that IMA is highly practical and user friendly. 19 Our results indicated that IMA can help develop a theory-based and evidence-based problem-solving approach, 31 produce outcomes, performance goals, change objectives, determinants, theoretical change methods and practical applications and evaluation. In this study, practical steps of intervention design were applied to teenage students’ musculoskeletal health through an intervention mapping approach based on the literature review, need assessment, group discussions and interviews with the planning team. The first step was to collect detailed information about the problem; in other words, a needs assessment was done.
In the next step, the target audience was identified. Then, we were mobilised through direct interaction with decision-makers. Besides, attracting facilitators (such as student representatives) from among the participants caused motivation and increased trust in the participants, increasing their participation. The duration of the pilot intervention was 2 months. These interventions used tools to change behaviour. There is the highest priority for the field of research to create a new solution to the reduction of musculoskeletal injuries among teenagers and a vision for interventions based on the needs of the audience. 30 We decided to use a series of up-to-date measures, such as forming a WhatsApp group for discussion and the exchange of ideas, in addition to the measures taken in previous interventions. Because virtual space was one of the interests of this age group. Sun et al. in a study aimed at designing a web-based programme, stated that the design of a workplace-based PA programme should be done separately. 31 We have found that methods such as knowledge promotion, modelling, advocacy, regulation and policy are good ways to encourage audience participation. In other studies aimed at promoting youth health, methods such as goal setting, verbal persuasion, practise with feedback, creating new social media links, information matching, social network mobilisation and empowerment32,33 facilitation,9,32 environmental marketing and awareness-raising, 9 benefits and barriers, social support and problem-solving were used. It is important to pay attention to the existing parameters for the effectiveness of the methods and turn them into practical applications because, without such consideration, their effectiveness will be affected. In addition, the relevance of the practical applications of the methods to aspects such as the target population, culture, and context increases their effectiveness. 34 The present study used an IM framework to design an employee PA promotion programme and used traditional methods such as questionnaires and new methods such as Instagram, animation and motion graphics. In this study, 200 employees participated in ten departments of the Ministry of Health. According to the pilot study, it is possible to find.
Conclusion
Intervention mapping has been successfully used to plan, implement, and evaluate educational interventions. This study has provided a good understanding of the role of intervention mapping in designing educational interventions for teenage students and a good foundation upon which subsequent reviews can be guided.
Footnotes
Acknowledgements
Our grateful thanks go to all participants in the present study.
Author contributions
NN, AZ and SST conceived and designed the study and finalised the methodology and tools used. NN and AZ collected the data and analysed and drafted the manuscript. SST and JA helped with critical comments and drafting the final version of the manuscript. All the authors made significant contributions in the manuscript writing and finalising of the manuscript. The final manuscript has been read and approved by all the authors.
Availability of data and material
All the data supporting our findings have been presented in the manuscript; the datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was drawn from a research project (No. IR.AUMS.REC. 1397.064) sponsored by the Deputy of Research and Technology at AUMS. Participants were aware about the purpose of the study and provided informed consent prior to accessing the questionnaire and participated voluntarily. No compensation was provided, and all collected data stored securely
Patient consent for publication
Consent from the patient for the publication was taken before collecting the data from them.
Informed consent
Written informed consent was obtained from participation.