
Abstract
Background:
Teenage pregnancy is an international phenomenon without a definite solution to date. Globally, an estimated 16 million girls aged 15–19 give birth each year. Husbands need to play their assistance role in order to thwart the negative impact of the outcome of teenage pregnancy.
Research objective:
To identify the effect of the development of Pregnancy Classes with the Husband’s Assistance on the Outcome of Teenage Pregnancy in the Dayak community, Central Kalimantan.
Research methods:
This was a quasi-experimental study with the posttest-only non-equivalent control group design involving the husband’s assistance in pregnancy classes. The respondents were 60 individuals where 30 of them were given the pregnancy class assistance intervention while the other 30 were not given any intervention (control group).
Results and discussion:
Pregnancy class with Assistance by the husband increases positive pregnancy outcomes 2.4 times compared to without the husband’s assistance. Family support increases positive pregnancy outcomes 2.5 times compared to pregnant women without support from the family. Pregnant women that are highly motivated regarding antenatal care are likely to have positive pregnancy outcomes 5.4 times greater than pregnant women with low motivation. Based on the analysis, then the variables that have no effect are the history of antenatal care, frequency of antenatal care, and support from health workers.
Conclusions:
Pregnancy class with husband’s assistance affects positive outcomes of teenage pregnancy. Other factors with meaningful influence on pregnancy outcomes include family support and motivation to seek teenage antenatal care. Furthermore, other factors that have no influence include the teenager’s age, history of antenatal care, frequency of antenatal care, and support from health workers. An intervention is needed that involves the husband/partner in the form of active assistance.
Introduction
Teenage pregnancy is a global issue that is related not only to the health of the mother and the baby to be born but also to the vital issue of societal development. 1 Every year, an estimated 21 million girls aged 15–19 in developing countries are pregnant and around 12 million give birth. 2 In Indonesia, according to the results of the Basic Health Research, 3 the proportion of teenagers aged 10–19 who had ever been pregnant was 58.8% and for those who were pregnant with their first child was 25.2%, the average age of girls at first pregnancy was 18 years with 46%, where the figure was in rural areas higher (51%) compared to urban areas. The results of SDKI 4 show7% of girls aged 15–19 years have become mothers, 5% have given birth and 2% are currently pregnant with their first child. BKKBN states that the pregnancy and birth rates among young women are still high, namely 48 out of 1000 teenagers. 5
Low-level education, low economic status, child marriage, and sexual abuse place girls at a higher risk of pregnancy. Knowledge gaps about pregnancy and misunderstandings about contraception among teenage girls result in early pregnancy. Sociodemographic and cultural factors such as limited education for women, low socioeconomic status, and belonging to ethnic or religious minorities increase the prevalence of teenage marriage and pregnancy in South Asia. 6 Other factors related to teenage pregnancy are low family income, marital status, lack of communications, and parents’ history of teenage pregnancy, low absorption of reproductive health services, juvenile delinquency, and social and cultural norms.1,7,8
In teenage pregnancy, there is an increased health risk to the mother and the baby to be born. 9 There are many negative impacts of teenage pregnancy, including anemia risk, the necessity of the baby being treated in the NICU, and postpartum complications. Several complications in infants include high rates of asphyxia, jaundice, hypothermia, neonatal tetanus, infection/sepsis, birth trauma, low birth weight, respiratory distress syndrome, and congenital abnormalities. Teenage pregnancy predisposes to recurrent pregnancy which affects the health of the mother and fetus and is economically unfavorable.10 –12 Pregnancy at a young age can result in disparities between mother and baby. 13
Pregnant teenagers hold a poor perception of social support. Support from friends and other close people is limited. The social support system is related to three important things, namely financial, emotional, and knowledge assistance related to their pregnancy health. Teenage pregnancy requires social support from friends and partners around them.14,15 Involving the young partner in teenage pregnancy may encourage them to increase measurable social support and commitment from family.16,17 Regarding the emotional support system, there needs to be a good relationship between a pregnant woman and her partner to improve pregnancy acceptance and strengthen the bond between them.
Partner or husband’s assistance system in Indonesia through the Suami Siaga program since 2010 is an important part of the maternal care movement in the utilization of health care during the period of pregnancy, childbirth, and postpartum. 18 There is a meaningful relationship between the husband’s involvement and the utilization of antenatal and delivery care. This statement means that pregnant women making use of pregnancy health care and delivery assistance by trained birth attendants are correlated with the involvement of the husband. 19 Spousal support is also an important matter related to pregnancy outcomes, where lack thereof may cause pregnant women to develop a negative attitude regarding the health of their pregnancy and result in unfavorable pregnancy outcomes.20,21 Women who reported at least one antenatal visit accompanied by their husband were more likely to deliver with a trained health worker than women who received antenatal care by themselves. 22 Teenage pregnancy class with the husband’s assistance is a face-to-face learning tool for mothers and husbands. Husband’s assistance especially in teenage pregnancy class allows creativity process (demand creation) by husbands and pregnant women with the aim of increasing understanding of pregnancy health and improving pregnancy outcomes.
Methods
Study design and population
This study employed a quantitative analytic research approach, using a quasi-experimental design with the posttest-only non-equivalent control group. The selection of designs aims to prove the effect of husband assistance on the class of pregnant women on pregnancy outcomes. The population of this study was all pregnant teenagers of the Dayak tribe in Kapuas and Gunung Mas Regencies. Kapuas Regency is located in Kapuas Hulu, Timpah, and Kapuas Tengah sub-districts while Gunung Mas Regency is located in Sepang and Tewah sub-districts. This location was chosen because it has a fairly high pregnancy cases in Central Kalimantan province, which is ranked third and fourth after Katingan and East Kotawaringin regencies. 23
Sample size
The study sample was adolescent pregnant women (aged 10–19 years). In this study, the number of samples using a minimal sample with a sample size for the minimum study is 30 samples. 24 The sample was 60 individuals, 30 of them were put into the treatment group while the other 30 were put into the control group. Sampling was performed with the simple random sampling technique, that is, using all the names of people included in the population are placed in a box, after everything is collected it is taken randomly as many as a predetermined sample from several populations.
Inclusion and exclusion criteria
The sample must meet the inclusion and exclusion criteria. The inclusion criteria are as follows: Adolescent pregnant women who are registered at the Puskesmas (local health center), adolescent pregnant women who are active in class activities for pregnant women and accompanied by their husbands, adolescent pregnant women with third trimester of pregnancy, and are willing to take part in this research in accordance with work procedures (informed consent). Exclusion criteria are pregnant women who moved their domicile within the study period and pregnant women who require treatment/treatment at the hospital. The independent variable was Husband’s Assistance while the dependent variables namely pregnancy outcome as external variables include history of ANC, frequency of ANC, motivation to attend pregnancy classes, support from health workers, and disorders/complications. The variables of adolescent pregnancy outcomes referred to in this study include maternal outcomes, childbirth outcomes, and perinatal outcomes.
Study tools
The instrument used was a questionnaire that has been tested for validity and reliability. The treatment group was given an intervention with the provision of the husband’s assistance pocketbook. The questionnaire was prepared by the author and the team based on reference sources related to family support, health worker support, and motivation of pregnant women in doing antenatal care.
The questionnaire was tested for validity and reliability on 30 pairs of adolescent pregnant women with similar characteristics. Validity and reliability tests were conducted on teenage pregnant women in North Barito District. The validity and reliability tests used the SPSS version 22 for the windows program. Item validity is based on the Pearson correlation between the item and the total answer which is compared with the r table. All question items were declared valid if the number indicated by r count >r table (0.05). There were 40 questions on the instrument before the validity test was carried out. Among the 40 question items, 7 question items that were canceled (Pearson correlation value less than r table, so 33 valid question items were obtained.
The instrument reliability test was also conducted to measure answer consistency among respondents based on the Cronbach Alpha score. In this study, the Cronbach Alpha score obtained is 0.868 or >0.7 25 so the instrument was interpreted as sufficiently reliable.
The questionnaire consisted of 33 questions, namely respondent characteristics 5 questions, family support 8 questions, health worker support 5 questions, and motivation 15 statements. The first part of the questionnaire was about information on the characteristics of pregnant women and husbands such as age at marriage, current age of mother and husband, ANC history, and ANC frequency. The next section was about family support and health worker support. Family support and health worker support statements were modified on a Likert scale of 1–4 if the statement was favorable: 4 = always, 3 = often, 2 = sometimes, and 1 = never, while on unfavorable statements: 1 = always, 2 = often, 3 = sometimes, and 4 = never. Then categories are made: 1 = not supportive (< median score) and 2 = supportive (≥ median score).
The third part of the statement is about motivation. For motivational statements, the Likert scale is modified from 1 to 4 if the statement is favorable: 4 = strongly agree, 3 = agree, 2 = disagree and 1 = strongly disagree, while on unfavorable statements: 1 = strongly agree, 2 = agree, 3 = disagree and 4 = strongly disagree. Then categories are made: 1 = Low (< median score) and 2 = High (≥ median score).
Data analysis
Data analysis used univariable, and bivariable analysis with Chi-Square test, and logistic regression analysis. Univariable analysis is carried out to describe the characteristics of each variable to be studied. The statistical measures used in this study are frequency distribution and percentage of each variable studied. The bivariable analysis is used to analyze the influence between independent and dependent variables. By using the Chi Square test (χ2). 24 Multivariable analysis is the development of bivariable analysis, this study aims to see the most influential factors on adolescent pregnancy outcomes using logistic regression analysis. 26
Ethical clearance
This research followed the ethical guidelines established by the Committee on Publication Ethics and was approved by the review board of the Ethics Committee of the Politeknik Kesehatan Kemenkes Palangka Raya (reference no. 077/III/KE.PE/2020). The participation of respondents was based on willingness to participate in this study and informed consent was obtained from all the participants.
Results
The results of the study and respondent characteristics are presented in the tables below:
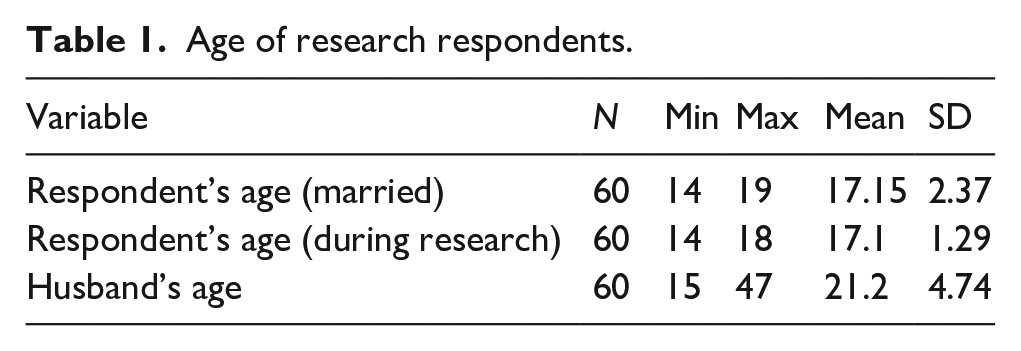
As seen in Table 1, the average age of the respondents when they were married was 17 years and the average age when they became pregnant was 17 years, while the average age of their husbands was 21 years.
Age of research respondents.
The results of characteristic univariate analysis in Table 2 show that 53.3% of pregnancy outcome was positive, 63% of the pregnant women received support during pregnancy from families, 51.7% had a regular ANC history, but 80% of them had low motivation, 78.3% had ANC frequency ≥4 times, and 78.3% received health worker support.
Respondent characteristics.

Below are the results of the bivariate analysis:
Based on the statistical analysis in Table 3, pregnancy class with the husband’s assistance (p-value 0.01 and OR = 2.443) has a significant effect on the outcome of pregnancy, so do family support (p value 0.05 and OR = 2.509) and motivation to have antenatal care (p-value 0.03 and OR = 5.417). Pregnancy class with the husband’s assistance increases positive pregnancy outcomes by 2.4 times compared to without the husband’s assistance. Family support increases positive pregnancy outcomes by 2.5 times compared to the absence of family support. Pregnant girls that are highly motivated in regard to pregnancy care showed positive pregnancy outcomes 5.4 times greater than those with low motivation. Upon analysis, it was found that the variables “history of ANC,” “frequency of ANC,” and “health worker support” had no significant effect.
Bivariate analysis of pregnancy outcomes.

The results of the multiple regression statistical test in Table 4 indicate that pregnancy class with husband’s assistance and family support have a more significant effect on the pregnancy outcome.
Multivariate analysis of pregnancy outcomes.

Discussion
Pregnancy class with husband’s assistance and teenage pregnancy outcomes
Based on the bivariate and multivariate tests, the husband’s assistance affects the outcome of teenage pregnancy. Pregnant teenagers that attended pregnancy classes with the husbands’ assistance had positive pregnancy outcomes compared to those that attended without their husband’s assistance. The pregnancy outcomes that were assessed in this study were perinatal conditions (prematurity, LBW, and other perinatal complications). For maternal outcomes, the method of delivery, complications of pregnancy, and complications of delivery were assessed. Assistance is related to the support that pregnant women received from their husbands (partners). Research of two economically and ethnically diverse groups in the Boston area highlights higher rates of antenatal anxiety, depression, and smoking among pregnant women who report low spousal support. Spousal support is an important intervention and has the potential to improve pregnancy outcomes. It particularly affects teenage pregnancy outcomes.17,27
Social support received from partners or other people is positively correlated with the subjective well-being of pregnant women. Social support offsets the negative changes in pregnant women. Research has found that spousal support during pregnancy can reduce the likelihood of depression, which can improve outcomes. 28 The study shows a chi-square p-value of 0.005, which indicates a significant relationship between the husband’s support and the behavior of pregnant teenagers to cope with pregnancy during the Covid-19 pandemic. Pregnant teenagers with spousal support are likely to prepare a more mature pregnancy and delivery program to ensure the safety of the mother and fetus. 29 Having support and a husband’s involvement during teenage pregnancy may reduce the likelihood of a poor birth outcome. 20
Several previous studies have found a significant relationship between the husband’s involvement and the use of antenatal and delivery cares. This statement means that pregnant women making use of pregnancy health care and delivery assistance by trained birth attendants is correlated with husband’s involvement and family support.19,30 Furthermore, spousal support is important in its connection to pregnancy outcomes, where lack thereof may cause pregnant women to develop a negative attitude regarding the health of their pregnancy and result in unfavorable pregnancy outcomes.20,21 Husband assistance in pregnancy classes can be a positive step to improve the knowledge, attitudes, and behavior of husbands/partners about pregnancy, especially teenage pregnant women so that they can provide positive support during pregnancy until childbirth. With a good partner’s understanding of pregnancy and positive support, teenage pregnant women can go through pregnancy safely without any anxiety about not being accepted and not supported.
Family support and pregnancy outcomes
Family support is highly correlated with decreased incidence of anxiety experienced by pregnant teenagers in dealing with their physical and psychological changes, which will affect teenage pregnancy outcomes. Family plays a role in providing support to teenagers in understanding risk factors for teenage pregnancy outcomes. Teenagers who understand and are well aware of risk factors for teenage pregnancy are likely to have positive pregnancy outcomes. When support is not received, it may result in poor pregnancy outcomes.
Recurrent pregnancy in teenagers can worsen the condition of teenage mothers. Social support affects care and welfare positively. Parents are the main source of support for teenage mothers; emotional and financial support from parents will delay the occurrence of recurrent pregnancies in adolescents. 31
In the study in Brazil aiming to identify pregnant teenagers’ perception of family support, of the 40 pregnant teenagers, 39 respondents have a low average perceived family support with a low level of education and live with the baby’s father. The lowest level of perception of family support was found among participants aged 16 and 17, especially among those living with their baby’s parents. 32 Family support is vital in staving off mental disorders in pregnant women. 33 Furthermore, family acceptance is very important (the family provides strength, in terms of supporting, educating, motivating, and growing the confidence of pregnant teenagers during pregnancy and childbirth). Teenage pregnancy that receives family support (emotional support, information support, instrumental support, and appraisal support) is likely to have positive outcomes.
Motivation to seek antenatal care and pregnancy outcomes
Providing antenatal care through pregnancy classes is intended to transform experiences, expectations, and meaning of care inside and outside ANC encounters, thus creating a cycle of self-reinforcement and motivation for better antenatal care. Partner can support their wife by motivating them to have pregnancy check-ups so that abnormalities and complications can be detected as early as possible. The motivation that pregnant women receive from their husbands as motivation from outside the individual pregnant women will help boost intrinsic motivation from within themselves. This condition will help pregnant women to maximize their efforts in pregnancy care, which is believed to help mothers strive for the health of their pregnancy (mother and fetus). The impact of this transformation ultimately reaches not only service providers and women but also their families and communities, thereby improving pregnancy outcomes. 34 The study also shows that antenatal care improves pregnancy outcomes among teenage girls. Understanding adolescent views and experiences about pregnancy and motherhood is important to ensure that antenatal care meets needs. Teenage girls’ main motivation for seeking treatment is to ensure the well-being of their babies. Appointment flexibility and accessible locations are also important. Continuity of antenatal care and full appreciation from health workers is very much what teenage pregnant women expect. 35
Pregnant teenage girls with good motivation to seek antenatal care will affect the outcome of their pregnancy. There is a relationship between the motivation given by the husband in the form of physical, psychological, emotional, and financial support to seek antenatal care so that it has an impact on healthy pregnancy outcomes. The role of the husband as the motivator of pregnant women is important for their health. The main motivation for pregnant teenagers to seek antenatal care is to ensure the well-being of their babies.35,36 Antenatal care is a crucial platform where all necessary health interventions during pregnancy are provided to reduce maternal and infant morbidity and mortality. Husband’s assistance in pregnant women’s classes motivates teenage pregnant women to be able to regularly carry out ANC so that pregnancy can be passed safely and safely for both mother and baby.
Age and pregnancy outcomes
Pregnant teenagers who were respondents to this study were in the age range of at-risk adolescents, with an average of 17.1 years. The results showed no difference in the incidence of positive pregnancy outcomes between respondents aged <17.1 and ≥17.1 years. Another study found that pregnancies at a very young age are at an increased risk of the incidence of preterm labor, childbirth, and postpartum hemorrhage (associated with unwanted pregnancies and unsafe abortions) as well as poor perinatal outcomes (LBW, IUFD, and intensive neonatal care). 7
The study conducted in Thailand on pregnant teens in the metropolitan city of Bangkok found many impacts of teenage pregnancy, including increased risk of adverse maternal outcomes (anemia, preterm labor, and postpartum complications), while the perinatal incidence of LBW babies and babies who have to be treated in the NICU have also increased.1,37 Another study in Saudi Arabia found teenage pregnancy has no relationship with poor pregnancy outcomes. Jeha et al. 38 found that there was an effect of teenage pregnancy on maternal outcomes, delivery outcomes, and neonatal outcomes. Thus, an effort is needed to provide the best treatment for teenage pregnancy. Maternal outcomes include anemia, gestational diabetes, placenta previa, infection, fever, and hypertension. Delivery outcomes include mode of delivery, postpartum hemorrhage, postpartum depression, and initiation of breastfeeding. Neonatal outcomes include prematurity, low birth weight, respiratory depression syndrome, congenital abnormalities, and autism. 38 Teenage pregnant women are highly discouraged because their growth and reproductive organs are immature, putting them at risk of poor outcomes for both mother and baby.
Frequency and history of ANC and pregnancy outcomes
Based on the bivariate and multivariate analyses, frequency and history of ANC (regular and irregular) were not associated with pregnancy outcomes. There is no difference between the pregnancy outcome of the pregnant women group with ANC frequency <4 times and that of the group with ANC frequency ≥4 times. Antenatal care (ANC) is one of the important determinants in lowering maternal and infant mortality rates. ANC aims to provide care centered on pregnant women and ensure that every meeting is carried out ineffective and integrated manners, provide relevant and timely information, and provide psychosocial and emotional support to pregnant women. It provides a positive experience in maintaining the health of women, children, and adolescents. The WHO recommends at least eight contacts during pregnancy. 39 Teenagers represent a vulnerable group and therefore need additional antenatal care such as sexual health screening, counseling on risk behavior, nutrition, maternity classes, birth planning, and postpartum contraception. ANC in teenagers aims to improve their pregnancy outcomes. 40
Antenatal care is both preventive and curative care administered during pregnancy. During pregnancy, health workers will carry out monitoring to assess unfavorable risk factors for the mother and her fetus and antenatal care will affect the coverage of deliveries by trained health personnel. 41 Specific and adequate antenatal care is needed by pregnant teenagers regarding special conditions and this pregnancy counts as a condition of a specific population. 42 Antenatal care given to teenagers is useful to detect complications and monitoring pregnant women’s health to achieve better pregnancy outcomes.
Health worker support and pregnancy outcomes
Based on the bivariate and multivariate analyses, support from health workers did not affect the outcome of teenage pregnancy. Support from health workers is useful for prenatal care and preventing recurrent pregnancies in adolescents. 43 Adolescent-specific antenatal services should be provided to raise awareness and reduce complications associated with adolescent pregnancy, such as premature birth, low birth weight, stillbirth, and neonatal death. Close collaboration must be established with various auxiliary services, including health-worker partnerships.35,40
Pregnant teenagers must receive support from health workers and regular training on the provision of youth-friendly antenatal care and be evaluated regularly to promote the provision of equitable and high-quality antenatal care for young women. 44 Prevention of maternal and perinatal complications common among teenage pregnancies needs to be supported and monitored by health workers so that pregnant teenagers receive quality midwifery services during pregnancy up to the postpartum period.
Our study had a few limitations. During the intervention process, of course, some data and samples of obstacles and obstacles were found, such as one pregnant woman and partner moving locations, and three husbands who did not attend pregnant women’s classes according to the predetermined time. For couples of pregnant women who moved locations, a replacement sample was sought so that it was fulfilled according to the number of samples and for those who did not attend, the next meeting was arranged.
Conclusions
(1). Pregnancy class with the husband’s assistance affects positive pregnancy outcomes in teenagers.
(2). Other factors that statistically influence pregnancy outcomes are family support and motivation to seek youth-friendly antenatal care.
(3). Other factors that have no effect are the teenager’s age, history of ANC, frequency of ANC, and support from health workers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.