
Abstract
Background:
Urinary Tract Infections (UTIs) during gravidity are among the most preponderant contagion globally and can culminate in fetal and maternal mortality. Lack of awareness and poor preventive practices can exacerbate this outcome. This study assessed the knowledge and preventive practices of antenatal mothers’ towards UTIs in pregnancy.
Design:
This was a cross-sectional descriptive survey involving antenatal mothers in selected health care facilities in Ekiti State.
Methods:
A pre-tested adapted questionnaire was used for data collection. Data was analyzed using descriptive statistics and Chi-square at p < 0.05.
Results:
The mean respondents’ age was 24.6 ± 2.1 years and barely less than half (43.8%) were multigravida. The findings of the study revealed that 64.0% of the respondents had good knowledge of UTIs. Overall, majority (78.9%) of the respondents exhibit good preventive practices toward UTIs in pregnancy, although the prevalence of UTIs among the studied subjects was found to be high (54.1%), with nearly half (48.7%) of the respondents reported been tested once for UTIs in the current pregnancy. Furthermore, there was a statistically significant relationship between educational level and respondents’ knowledge on the prevention of UTIs in pregnancy (p = 0.00; p < 0.05).
Conclusions:
Respondents had good knowledge and good preventive practices toward UTIs. However, the high prevalence of UTIs reported among respondents justifies the need for implementation of knowledge enhancement program, routine testing and prompt treatment of UTIs among antenatal mothers.
Introduction
Urinary Tract Infections (UTIs) are among the most significant health challenges affecting females of reproductive age groups in third world nations. Pregnant women are more vulnerable to UTIs owning to an agglomeration of hormonal, physiological and mechanical changes which aid urinary stasis and vesicoureteral reflux. 1 Also, significantly aggrandize during gravidity is acute pyelonephritis. 2 These changes, along with an already short urethra (roughly 3–4 cm in females) and awkwardness in hygiene attributed to a protruded pregnant belly; help make UTIs the most preponderant bacterial infections during pregnancy. Factors like diabetes, indigence, multiparity, history of repeated urinary tract infection, increasing maternal age, and anatomical malformations of the urinary tract have also been attributed with a double rise in bacteriuria during pregnancy. 2
Worldwide, UTIs prevalence in pregnancy ranges between 13% and 33% with symptomatic bacteriuria occurring in 1%−18% while asymptomatic cases are observed in 2%−10% of females. 3 The prevalence has remained fairly constant and a large proportion of observational studies, including those emanating from poor economy countries, enunciated approximately similar rates. 2 UTIs refer to the presence of pathogenic bacteria within the urogenital tract which often may be diagnosed from the symptoms and laboratory investigation. From clinical point of view, manifestation of UTIs differs but the common exhibited symptoms include odoriferous urine, idiopathic pyrexia, and lower abdominal pain. 4 The commonest (80%–90%) causative organism of UTIs among pregnant women is Escherichia coli while the remaining (10%–20%) cases are ascribed to Klebsiella and Enterobacter. 5 UTIs if untreated can result into complications viz preeclampsia, abortion, chronic pyelonephritis, preterm labor, and solemnly renal dysfunction. 6 Past history of UTIs heightens the probability of recurrent infection by 50%, presence of asymptomatic bacteria intensifies the chance by 25% and deformity in the renal tract is observed about 25%. It has been enunciated that circa 2%–10% of adolescent females are at risk of being asymptomatic in pregnancy on routine screening. If not discovered at onset and treated punctually, this infection complicates 1%–3% of pregnancies. 4 Nearly 7 million outpatient cases and 1 million emergency cases during pregnancy were attributed to urinary tract infection as articulated in a 1997 survey.3,5
According to the World Health Organization (WHO) report, 20%–50% of gravid females will experience bacteriuria during child-bearing, with about 5%–10% of these cases been vulnerable in their primigravida. 7 Studies are replete with evidence that UTIs in pregnancy can result in maternal and fetal morbidity. Therefore, gravid females should be informed about the physiological changes during gravidity which may be one of the probable risk factors for the occurrence of urinary tract infection and also about its preventive measures. The knowledge of UTIs is very momentous in the prevention of its occurrence and recurrence. 8 The relevance of this issue cannot be overstress because of the significance impact it has on the health of pregnant women and their fetus, which in worst situations claim the lives of its victims. Evidently, African literature has a paucity of studies that investigate the erudition, attitude, and practices of pregnant women toward UTIs prevention. To our knowledge, there are limited studies in our locality that addresses this crucial subject. Base on the aforementioned gap, this study was therefore carried out at two selected health facilities (State Specialist Hospital Ikere Ekiti and Comprehensive Health Center Oke Iyinmi, Ado Ekiti), both located in Ekiti State, Nigeria, to assess the level of knowledge, attitude and practices regarding UTIs and its prevention among pregnant women.
Methods
Study design
We conducted a descriptive cross-sectional survey among antenatal women across two selected health facilities in Ekiti State, to assess their knowledge, attitude and current practices toward the prevention of urinary tract infection in pregnancy.
Study settings
The study was conducted at the State Specialist Hospital Ikere (SSHI) Ekiti and Comprehensive Health Center Oke Iyinmi (CHCOI), Ado Ekiti both located in Ekiti State, Nigeria. The SSHI is located along Ise-Ekiti road, Ikere Local Government Area, Ikere Ekiti, Ekiti state, Nigeria. 9 This health facility provides general medical care and health services. The hospital comprises of different wards which include; surgical ward, medical ward, labor ward, antenatal clinic, and accident and emergency unit.
The CHCOI was founded in 2012. It is located in Ado Local Government Area, Ekiti State. 9 It is a comprehensive health center that comprises of a consulting room, delivery room, recovery room, pharmacy and health record room. The facility has one full time doctor, three full time nurses, two full time midwives, and three community Health Extension Workers (CHEW). Other facilities include improved water supply, electricity, vaccine freezers, and improved sanitation. Some of the basic services provided are antenatal clinics, family planning, malaria treatment, maternal health delivery, measles immunization, emergency transport, and skilled birth attendants.
The choice of selection of SSHI is due to its fame, being the most popular state-owned hospital in the state while CHOI was selected because it has the highest patronage and is located in the core of the state capital (Ado Ekiti) and patronized by the indigenous people of Ekiti State, where it is accessible to most rural populace.
Study population
The study population consists of women of reproductive age group (15–49 years) who are pregnant and are attending antenatal clinic in SSHI and CHCOI.
Inclusion Criteria: This include consenting pregnant women who are between age 15 and 49 years and are attending the chosen primary health centers, within the study time frame, were recruited for the study.
Exclusion Criteria: Pregnant women who were sick and were on admission were excluded from the study, and we excluded also those who were unwilling to participate.
Sample size determination
One hundred registered pregnant women were attending SSHI and 300 registered pregnant women were visiting CHCOI as at the period of study, constituting a total of 400 people. From this sample frame, 230 respondents were recruited for the study, but only 210 of the participants completed and correctly filled the questionnaires, yielding a response rate of 91.3%. The sample size was calculated as shown below:

Where,
n = sample size,
N = population size,
e = sampling error (0.05 as acceptable error)
in this study,
N = 400
e = 0.05
n = 400/[1 + 400 (0.05 × 0.05)]
n = 200
Hence, the minimum sample size required for the study was 200. However, the respondents recruited into the study was increased to 230 to accommodate for non-respondent rate.
Sampling technique
Proportional sampling technique was adopted in the determination of the number of subjects for the study from the subpopulations (SSHI and CHCOI) while random sampling was employed in the selection of participants from each subpopulation. This is explained below:
The proportion of pregnant women in SSHI (100) to CHCOI (300) is 1:3. Hence, the number of respondents recruited from each stratum is calculated below: Number of respondents selected from SSHI = ¼ × 230 = 57.5 = 58 participants. Number of respondents selected from CHCOI = ¾ × 230 = 172.5 = 172 participants.
Hence 58 + 172 = 230 participants
Instrument for data collection
Data collection was done through a pre-tested well-structured, self-administered questionnaire adapted from previous study. The components of the questionnaire were categorized into four sections namely: Section A: socio-demographic information of respondents (pregnant women) vis age at last birthday, marital status, level of education, Section B: Obstetric history of respondents, Section C: deals with the knowledge of pregnant women about UTIs and its prevention, Section D: deals with the attitude of pregnant women toward prevention of UTIs, Section E: assessed pregnant women’s practices to prevent urinary tract infection, and Section F: deals with questions that assess the prevalence, period of treatment and frequency of testing for UTIs among respondents.
Validity and reliability of the instrument
This study ensured the use of external and content validity. The researchers and two other experts in the field of study closely examined the items in the questionnaire to ensure that they could accurately measure the intended variables. Test-retest method was used to assess the reliability of the instrument. Internal consistency of items showed an intra-class correlation coefficient of 0.81. The questionnaire was administered to 230 respondents who attended the antenatal clinic of the health care facilities.
Data collection procedure
Data was collected from April 2 to May 17, 2018. The data was collected over a period of 6 weeks, and it was done either by interviewer-administered or through self-administration of the questionnaires. To ensure that we collect accurate information, the self-administered format was only permitted to respondents with tertiary education and who indicated willingness to do so.
The consenting pregnant women were recruited into the study after thorough explanation of the research. Participants were informed of their right to voluntary withdrawal from the research at any instance, if they desire to discontinue without any penalty; and that there was no benefit attached to participation except for findings obtained from the study.
Data analysis
After data collection, the questionnaires were properly checked for completeness. The collected data was entered manually and analyzed using Statistical Package for Social Science (SPSS) version 25. Analyzed data were summarized and presented in the form of frequency tables, percentages, charts and descriptive statistics (mean and standard deviation). Knowledge of the prevention of UTIs was scored based on 10 items with each correct answer attracting 2 marks. The total marks were 20, the mean score was 12. Less than 12marks was an indication of Poor Knowledge while 12 marks and above was an indication of Good Knowledge. The attitude scores were based on eight items with correct answers attracting 3 marks and overall mark was 24, mean score was 16 marks. Lesser than this was indicated negative attitude while equal to or greater than 16 marks was indicated positive attitude. Practice toward the prevention of UTI in current pregnancy was assessed using 16 items with correct answers attracting 2 marks each, the overall total was 32 marks, and the mean score was 20 marks. Less than 20 marks was indicated as poor practice while 20 marks and above was indicated as good practice.
Inferential statistics such as Chi-square (χ2) and bivariate regression analysis was employed in testing association between variables. Statistical significance was place at one-tailed, p-value less than 0.05 for all inferential analysis.
Ethical considerations
Ethical approval for the research was obtained from the Research and Ethics Committee of Afe Babalola University, Ado-ekiti. Approval was also obtained from the Chief Matrons of Oke Iyinmi Comprehensive Health Centre and State Specialist Hospital Ikere Ekiti respectively. Also, informed verbal consent was obtained from all participants after thorough explanation of the research before recruited into the study. The right to privacy and anonymity of the participants in the study were strictly adhered to by the researchers and respondents were assured that information provided would be used for research only.
Results
A total of 230 questionnaires were administered and of which only 210 were completed, returned and subsequently analyzed giving a response rate of 91.3%.
The baseline socio-demographic characteristics and obstetric history of respondents are presented in Tables 1 and 2 respectively. The mean respondents’ age was 24.6 ± 2.1 years. Majority (74.8%) of the respondents were married and barely less than half (46.7%) had attained tertiary education. Regarding number of previous pregnancies, nearly one-third (33.8%) of the respondents were first-timers (i.e. had never been pregnant before) while majority (66.2%) are multi-gravida. Most (76.7%) of the respondents were in their second trimester. About one-third (35.2%) of the respondents were nulliparous while the remaining (64.8%) constitute primiparous, multiparous and grand multiparous respectively.
Socio-demographic characteristics of respondents.

Obstetric history of respondents.

The results of respondents on knowledge on UTIs is presented in Table 3. Almost all the respondents (90.0%) had heard about urinary tract infection (UTIs) and majority (74.8%) knew that UTI is an infection that affects any part of the urinary system. Most of the respondents reported the following as symptoms of UTIs: pain (62.9%), hematuria (67.1%), frequent urination (81.9%), and fever (73.1%). The two major complication of UTI reported by the respondents were preterm delivery (53.3%) and neonatal UTIs (48.6%). Figure 1 showed the source of information of UTIs among respondents. Less than half (46.0%) of the respondents acquired their erudition of UTIs from educational facilities, (15.3%) from books, (15.3%) from friends/family, (12.9%) from internet, and (10.5%) from media. As depicted in Figure 2, the following predisposing factors were enunciated for the occurrence of UTI by the respondents: sexual activity (93.3%), short urethra in females (85.1%), suppressed immunity (84.3%), pregnancy (76.0%), catheter usage (56.2%), and menopause (52.1%).
Knowledge about urinary tract infection.

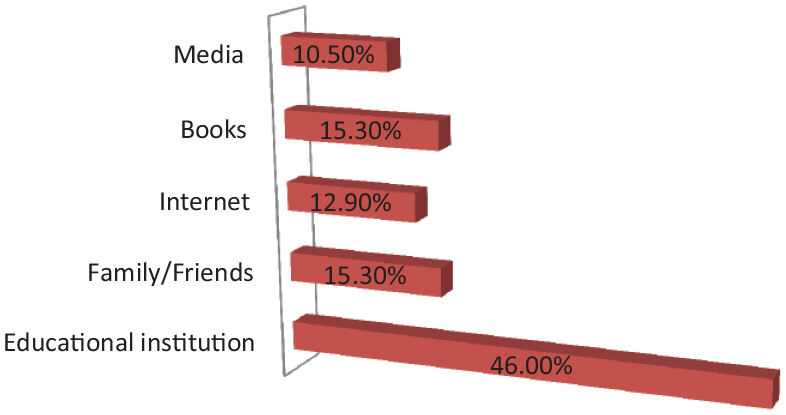
Source of information of urinary tract infection.

Risk factors for urinary tract infection.
Table 4 depicts the knowledge of the respondents on prevention of urinary tract infection during pregnancy and overall summary index for knowledge prevention of UTIs. Most (70.0%) of the respondents reported emptying of bladder every 4 h forestall UTI, 68.6% have knowledge that increasing fluid intake prevents UTIs, and nearly half (48.1%) concur to the application of estrogen cream as a preventive measure of UTI. Also, about 62.9% know that urinating after sexual intercourse impede UTIs, however more than half (58.0%) of the respondents lack erudition that washing of vagina anteroposterior inhibit UTIs occurrence. The respondents’ have knowledge that the following practices make gravid women susceptible to urinary tract infection: wearing tight underwear (73.8%), cleansing of the urogenital tract with soap (76.2%), immoderate intake of caffeine (48.6%), wearing squalid underwear’s (72.8%), and douching (45.7%). Overall summary of knowledge of respondents on UTIs revealed that more than half (64.0%) the respondents had a good knowledge on the prevention of UTIs in pregnancy while approximately a-third (36.0%) had poor knowledge of UTIs prevention in pregnancy.
Knowledge about the prevention of urinary tract infection.

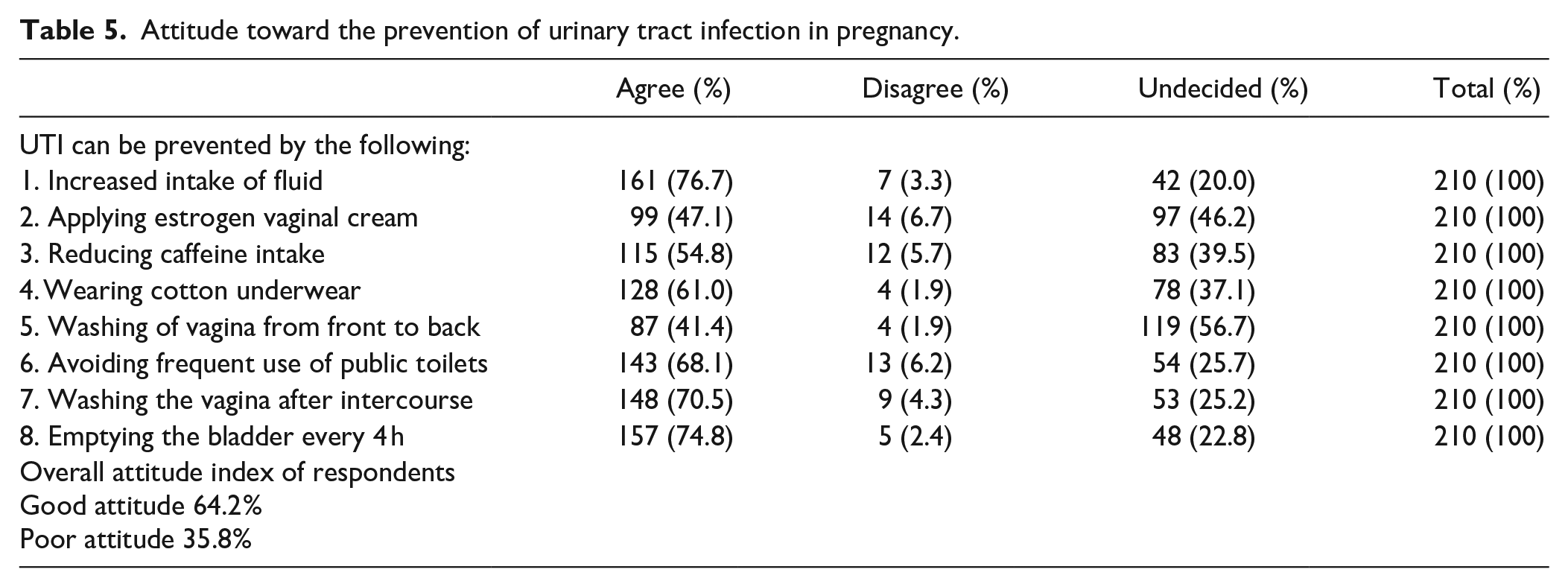
Regarding Attitude of Respondents toward the Prevention of UTIs in Pregnancy (Table 5), a higher proportion of the respondents agree that UTIs can be prevented in pregnancy through the following: increased intake of fluid (76.7%), applying estrogen vagina cream (47.1%), mitigating caffeine intake (54.8%), wearing cotton underwear (61.0%), avoiding frequent use of public lavatories (68.1%), cleansing of vagina after copulation (70.5%), and emptying the bladder every 4 h (74.8%). However, more than half (56.7%) of the respondents disagree that cleansing of the vagina anteroposteriorly prevents UTIs (Table 5). Overall, the composite score for attitude shows that 64.2% of the respondents had positive attitude toward the prevention of UTIs in pregnancy.
Attitude toward the prevention of urinary tract infection in pregnancy.
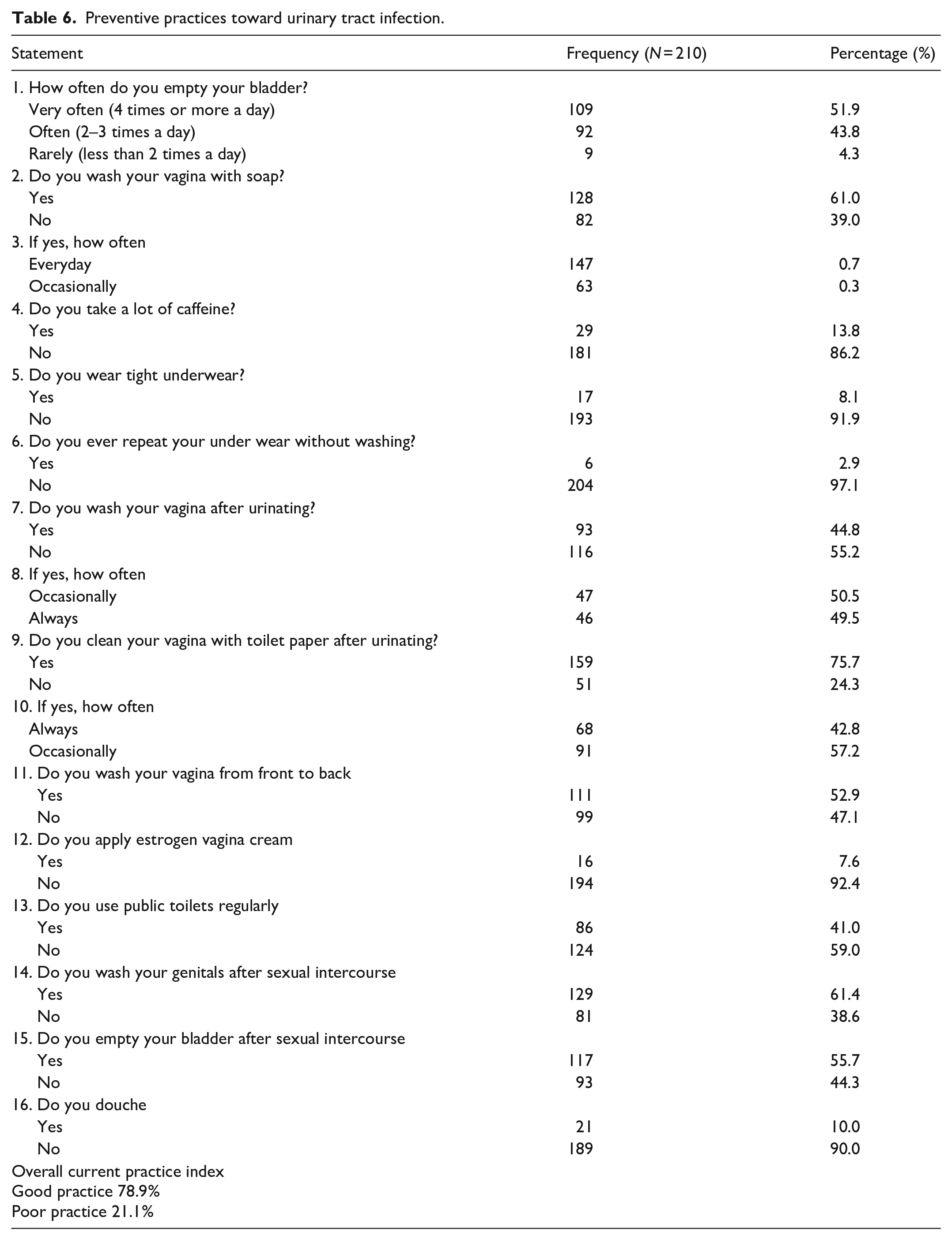
Results on the preventive practices on respondents toward UTIs is presented in Table 6. The proportions of respondents that empty their bladder four times or more a day and likewise wash their vagina with soap were 51.9% and 61.0% respectively. The following practices were reported by the respondents: do not take caffeine (86.2%), do not wear tight underwear (91.9%), do not repeatedly wear unwashed undies (97.1%), do wash vagina after micturition (55.2%), clean vagina with tissue paper after urination (75.7%), wash vagina anteroposteriorly (52.9%), do not apply estrogen vagina cream (92.4%), do not use public toilet regularly (59.0%), wash genital after copulation (61.4%), empty bladder after sexual intercourse (55.7%), and do not douche (90.0%) as showed in (Table 6). Overall preventive practice index of respondents revealed that 78.9% of the respondents exhibit good preventive practices toward UTIs.
Preventive practices toward urinary tract infection.
Prevalence of UTIs among respondents is shown in Figure 3 where about 54.1% of the respondents had been treated of UTIs previously. Barely more than half (52.0%) of the respondents have been treated at adolescent, one-quarter (25.0%) reported been treated at previous parturiency while 23.0% were treated during their current conception as shown in Figure 4.

Prevalence of urinary tract infection among respondents.
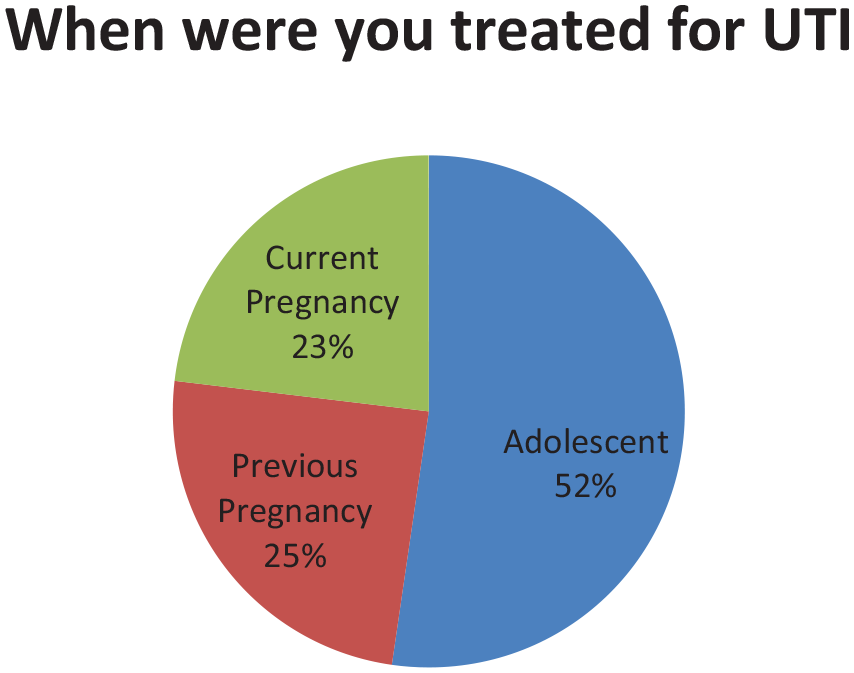
Time of treatment for urinary tract infection.
The number of times respondents have been tested for urinary tract infection in current pregnancy is depicted in Figure 5. Nearly half (48.7%) of the respondents reported been test once for UTIs in current pregnancy, 23.4% of the respondents reported tested twice, 1.5% had been tested three times and barely one-quarter (26.4%) had never been tested at all.

Number of times respondents have been tested for urinary tract infection in current pregnancy.
Moreover, there is a significant relationship between respondents’ level of education and prevention of urinary tract infection (UTIs) in pregnancy (p < 0.05). This is presented in Table 7.
Relationship between level of education of respondents and prevention of urinary tract infection.

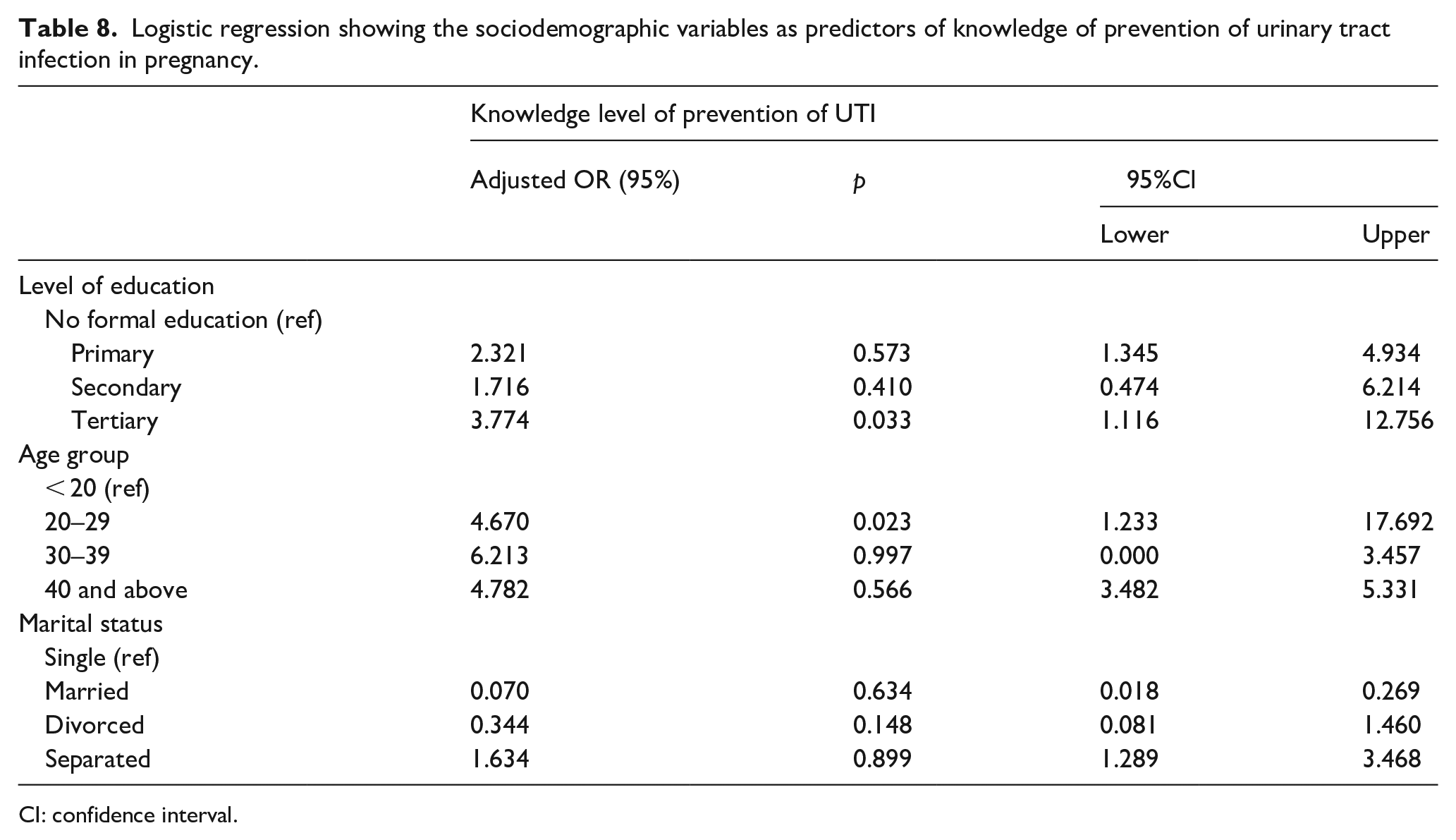
Additionally pregnant women with tertiary education were 3.7 likely to have good knowledge about prevention of urinary tract infection more than those with no formal education (adjusted OR 3.77, 95%CI 1.116–12.756; p = 0.033). Also, pregnant women whose age were between 20 and 29 years were 4.67 likely to have good knowledge of urinary tract infection more than those that were less than 20 years (adjusted OR = 4.670, 95%CI 1.233–17.692; p = 0.023) as presented in Table 8.
Logistic regression showing the sociodemographic variables as predictors of knowledge of prevention of urinary tract infection in pregnancy.
CI: confidence interval.
Discussion
It has been affirmed that UTIs is a common contagion among males and females but the incidence as earlier stated is quite preponderant among women due to their physiology and shorten urethra; with the prevalence higher among gravid females owning to the expansion of the uterus and unhygienic practices. 10 In our present study, majority (65.7%) of the pregnant mothers were in the age group of 20–29 years with a mean age of 26.4 ± 2.3 years and most (74.8%) of them were married. This is expected as it is considered the ideal age group for marriage in most part of Africa. A similar study conducted in other part of sub-Saharan African reported that majority of the respondents were married and within the age group 20–35 years. 10 Studies conducted in third world countries such as Nepal, shown that 4.46% of participants were in between the age group of 22 and 25 years and another in Brazil reported that 67% of the gravid mothers were in the age group of 20–29 years. All these surveys were in consonance with this present study. 11 Regarding the educational status of the survey participants; barely less than half (46.7%) of the respondents had tertiary education. This is not surprising as Ekiti state is famous for having a high proportion of literates. This finding negate that reported by other authors, El Sayed 12 and Sania et al. 13 who enunciated that more than half of the studied pregnant women had secondary education only. From present study 39.1% of the respondents were multiparous and 76.7% of the pregnant mothers were in their second trimester. This report was in accordance with that of Godwe and Alfred 14 who reported that nearly half of their studied participants had two or more births and that majority of the pregnant women were in more than 3 months of gestational age. Also, a study conducted by Foxman 15 in Al-Mukalla district affirmed that the frequency of bacteriuria increases with gestational age, with nearly half of the study participants in the third trimester and about 75.6% of infected women been multiparous.
Knowledge of respondents on urinary tract infections and prevention
Knowledge refers to the awareness or understanding of a subject matter (person or thing) such as objects (acquaintance knowledge), facts (propositional knowledge), or skills (procedural knowledge). 13 Majority (90%) of the respondents had heard about UTI and barely less than half (46.6%) of them heard about it from educational facilities. Most (74.8%) of them knew that UTI is an infection that affect any part of the urinary system. Generally, most of the respondents know the causative factors of UTI. Some of the predisposing factors pointed out by the respondents include: sexual activity, compromised immunity, catheter use, menopause, gravidity, and menopause. Out of the whole respondents, 70.0% know that frequent emptying of the bladder prevents UTI, 62.9% know that urinating after copulation aids in the prevention of UTI, 68.6% have the erudition that adequate fluid intake prevents UTI, however 58.0% do not know that cleansing of the perineum anteroposteriorly prevents UTI occurrence. All these point to the fact that most of the respondents have knowledge of urinary tract infection and are also aware of the various preventive measures which serves as impediment to UTI occurrence. These figures were corroborated by the good knowledge level on the prevention of UTI displayed by a higher proportion (64.0%) of the respondents in this study. This finding is in consonance with that reported by Bhat et al. 16 that 77.3% of their studied participants had average knowledge on UTI prevention. This present study is further aggrandized by a more recent study conducted by Mafuyai et al. 10 the authors reported a higher (80.3%) knowledge level on the prevention of UTI by the respondents. However, the findings from this study contravene that reported by Adhkari and Dhakai, 17 who revealed 64.63% of pregnant women had no information about UTI and its prevention; and also, another study conducted by Sania et al. 13 who enunciated that less than a quarter of their respondents had good knowledge of UTI prevention.
Attitude of respondents toward urinary tract infections
Regarding the summative attitude of the studied subjects about urinary tract infection; most (64.2%) of the pregnant women had positive attitude, with just barely one-third having negative attitude about UTI prevention. These findings are consistent with that of Sania et al. 13 who carried out a study on the knowledge and attitudes of pregnant women regarding UTI at a tertiary health facility in Egypt and enunciated that about four-fifth of their respondents had positive attitude about UTI. This report is also supported by Bhat et al. 16 who denoted that majority of their studied participants had positive attitude on the prevention of UTI. Also, corroborating this study is the report of Santoso et al. 18 who enunciated that more than 50% of their studied respondents showed a total positive attitude.
Practice of respondents toward urinary tracts infections prevention
The study also depicts that respondents empty their bladder four or more times per day (51.9%), clean their perineum anteroposteriorly (52.9%), wash vagina with soap (61.0%), wash genital after copulation (61.4%), do not wear tight underwear’s (91.9%), wash the perineum after micturition (55.2%), empty bladder after sexual intercourse (55.7%), and do not repeatedly wear dirty undies (97.1%). This study implies that most of the subjects have erudition of the different preventive measures of UTI and at the same time practice them. These findings are in concordance with that reported by Mafuyai et al. 10 where most of their respondents know about UTI prevention and likewise practice them. The overall current practice level of the respondents on the prevention of UTI in pregnancy was very good and high (78.9%) and this was in agreement with the findings of several authors.10,14,19
Urinary tract infection is a common infection among women and is followed by numerous complications. 20 Among the aims of this study, was to determine the prevalence and frequency of testing for UTI during current pregnancy among respondents. About 54.1% of the respondents had history of encounter and treatment with UTI at least once in their lifetime and while some had it during their current gravidity. In addition, nearly half (48.7%) of the studied women have been tested at least once for UTI in their current pregnancy. These findings were in harmony with those reported by Amiri et al., 21 Lele et al., 22 and Sania et al. 13 who enunciated high prevalence of UTI among their studied subjects during pregnancy and had been hospitalized at least once. This may be ascribed to the unwholesome hygiene practices by the studied subjects during pregnancy, as well as inadequate information on the health consequences of UTI to both mothers and fetal.
Relationship between knowledge on UTI prevention and respondents’ socio-demographic characteristics
There is statistically significant association between certain socio-demographic variable (age and educational level) and respondents’ knowledge of UTIs. It was found that there was a statistically significant relationship between the two variables and respondents’ knowledge of UTI. Further analysis using bivariate analysis revealed that Pregnant women with tertiary education were 3.7 likely to have good knowledge about prevention of urinary tract infection more than those with no formal education. This denotes that pregnant mothers with higher education are more knowledgeable and aware on UTIs and its prevention vis-à-vis those respondents with less educational background hence are less prone to UTIs complications. This finding was corroborated by Gondwe and Alfred 14 who reported that pregnant mothers who did not finished secondary education and those from the penurious background tend to be ignorant of the symptoms of UTIs and consequently suffer its complication vis premature births, low infant birth weight and aggravated perinatal mortality.
This study also revealed that pregnant women whose ages were between 20 and 29 years had good knowledge of urinary tract infection more than those that were less than 20 years. This may be due to the fact that most women in African setting marry at this age and every married woman wants to give birth 9 months after wedding (typical of the African culture) which may encourage them to learn more on UTIs and other hindrances/barriers to pregnancy. This is in line with a study among women in sub-Saharan Africa that most of the women married at age 20–35 years. 10
Conclusion
The study revealed that more than three-fifth of the respondents had good knowledge and positive attitude about the prevention of urinary tract infection in pregnancy. Also, a higher proportion of the studied pregnant women show good current practice toward the prevention of urinary tract infection in gravidity. This study also reported a statistically significant relationship between respondents’ knowledge on UTIs prevention during pregnancy and educational level and age of respondents. Although respondents in this study demonstrated good knowledge and current practice level on the prevention of UTIs, there was still high level of prevalence of UTIs among the studied subjects.
Hence this study recommends that educational programs should be designed and implemented to increase awareness on UTIs and decrease the susceptibility of UTIs among the female population. Secondly, there should be knowledge enhancement program related to UTIs in the course of pregnancy which may help in attitudinal change. Conclusively, Government should put in place necessary facilities in health institutions to allow for routine UTIs test and treatment, as this would enable females who had early encounter with UTIs to seek prompt medical treatment before it relapses.
Strengths and limitations of the of study
The original and primary data collection from a randomly selected antenatal mothers sub-population formed the strength of our study. However, the study was limited by the size of the antenatal mothers studied and the self-report nature of the study. This could limit the generalizability of our findings.
Footnotes
Acknowledgements
The researchers appreciate the antenatal women who participated in the study.
Authors’ contributions
DTE and BO designed the study. DTE and BO, POA implemented the research. AAS, DTE, CBB, analyzed and interpreted the data. AAS and DTE, wrote the manuscript and POA proof-read the manuscript. DTE arranged to journal specifications. DTE and OIO critically reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.