
Abstract
Background:
The prevalence of stunting in Indonesia has decreased gradually. The strategy to reduce stunting is currently prioritized on improving socio-economic levels, fulfilling food intake, and sanitation conditions. This study aims to analyze the association between sociodemographics, nutrition, and sanitation on stunting in rural West Java Province in Indonesia.
Design and methods:
A cross-sectional study was conducted in May–August 2022 among 247 mother-children pairs, selected by systematic random sampling from a rural area of West Java Province in Indonesia. The sociodemographic characteristics were measured using a structured questionnaire. The nutritional status of the children under five was assessed by length/height-for-age (HAZ), and was calculated using WHO Anthro software. Sanitation is assessed using observation and interviews with a structured questionnaire.
Results:
The prevalence of stunting in children under five was 20.7% (5.3% severely stunted and 15.4% stunted). Binary logistic regression analysis using SPSS version 22.0 show that mother’s height as the dominant factor associated with stunting in children under five (AOR = 3.45, 95% CI: 1.12–4.67, p = 0.008). In addition, children’s age (AOR = 0.250, 95% CI: 0.104–0.598, p = 0.002); balanced diet practices (AOR = 1.57, 95% CI: 0.965–2.56, p = 0.069), and building materials (AOR = 1.869, 95% CI: 0.87–4.00, p = 0.108 are also related to stunting in children under five.
Conclusions:
Efforts to improve maternal nutrition need to be carried out from the period before pregnancy to the first 1000 days of life. Education on healthy home indicators, especially the use of this type of building materials for houses, needs to be done to improve sanitation as an effort to prevent stunting in children under five.
Introduction
Stunting prevention is carried out massively in various countries including Indonesia. The government is conducting convergence to accelerate nutrition improvement as an effort to reduce stunting rates through a multi-sector approach. The strategy for reducing the stunting rate in this country is stipulated through Presidential Regulation of the Republic of Indonesia Number 72 of 2021 concerning accelerating the reduction of stunting in a holistic and integrative manner, which includes both nutritional and non-nutritional aspects including improved sanitation. This regulation is also in line with one of the objectives of the Sustainable Development Goals, namely eliminating all forms of malnutrition, particularly stunting. The national target for reducing the stunting rate is to reach 14% by 2024. However, the decline in stunting prevalence has only reached 6.4% over 5 years, from 37.3% (2013) to 30.8% (2018). 1 Efforts to reduce stunting rates need to be continued to prevent stunting since the pre-conception period, and especially in the first 1000 days of life. Failure to prevent stunting has an impact on the occurrence of nutritional problems across generations. Stunted children experience chronic malnutrition resulting in growth failure, where this condition is characterized by height that is not appropriate for their age. 2 They are at risk for physical and cognitive disorders, metabolic disorders that cause degenerative diseases, and socio-emotional development disorders.3 –5 This condition has the potential to create a cycle of poverty for the next generation and increase the economic burden for the country. Stunting is also a risk factor that contributes to child mortality, where malnutrition is also an indicator of inequality in human development.1,2
The magnitude of the impact of stunting on the nutritional and health conditions of toddlers has resulted in malnutrition being a priority health problem that must be addressed immediately. Stunting prevention efforts are focused on the causative factors. Stunting is directly caused by nutritional intake and health status, while indirectly caused by low food security, conditions of the social environment, health environment, and residential environment. 6 Therefore, efforts to prevent stunting are focused on these causal factors which are carried out through the integration of nutrition-specific interventions and nutrition-sensitive interventions.7,8 Nutrition-specific interventions are the interventions which address the immediate cause of malnutrition such as food intake, infection, nutritional status of the mother, infectious diseases, and environmental health. This interventions are largely delivered by the health sector. Some of the examples of nutrition-specific interventions are maternal micronutrient supplementation and disease prevention, support for exclusive breast-feeding and complementary feeding, micronutrient supplementation, and other similar programs. Whereas nutrition-sensitive interventions are those interventions whose primary objective is not nutrition, but that which have potential to improve food and nutrition security of beneficiaries. This interventions are largely delivered by the education, agriculture, livestock, water and sanitation, women and children and other sectors. the form of activities in Nutrition-sensitive intervention includes improvements in the agriculture, clean and water sanitation, and healthcare improvement.7,8 Previous studies have shown that the integration of the two interventions can significantly prevent and reduce stunting rates in many countries. In general, efforts to prevent stunting are associated with nutritional aspects as direct factors, and socio-demographic and sanitation as indirect factors of stunting.9 –11 Scientific evidence shows that socio-demographics, nutrition, and sanitation are predictors of stunting.9,12
Sociodemographic problems are related to the low level of the economy which has an impact on the purchasing power of food at the household level. Li et al. in 2020 reported the Demographic and Health Survey (2007–2018) in 35 low- and middle-income countries which showed that more than a third of children (38.8%) aged 12–59 months were stunted. According to the study, it was reported that the dominant factor associated with stunting was socioeconomic conditions. Children under five who come from poor families have low purchasing power of nutritious food. In addition, they have mothers with low education and do not apply proper parenting, especially in feeding practices. 13 The high problem of stunting especially in rural areas is also associated with low levels of economy, education, and mother’s knowledge regarding balanced nutrition practices in children under five. 14 Study by Das et al. in Mumbai, India (2020) who reported that stunting was more common in mothers with lower education. In addition, mothers who are exposed to physical violence from their husbands are associated with a higher probability of stunting, where this can reduce the focus of mothers on child feeding practices. Failure to practice feeding in the first 1000 days of life results in not fulfilling the nutritional intake needed to achieve the growth and development of children under five. 15
Previous studies strongly prove that nutrition is main cause of stunting in children under five. A study by Permatasari and Chadirin in rural areas of Bogor District in Indonesia shows that almost a third (29.7%) of children under five are stunted. Stunting in this region is dominantly caused by the occurrence of chronic malnutrition experienced by mothers long before the time of pregnancy which is characterized by a short mother’s height, and the lack of energy intake in children under five. 16 During the period of rapid growth, namely during pregnancy and the first 2 years of life, macronutrients, especially energy and protein, and micronutrients are needed which are higher than at other ages. It is necessary to accelerate cell division and DNA synthesis during growth. Therefore, chronic malnutrition at this time causes the growth of toddlers who are not in accordance with their age, and has lower intelligence than children who are not stunted. Poor nutrition during the window of opportunity also causes many nutritional and health problems in the next period of life, especially the occurrence of various degenerative diseases such as diabetes mellitus.17 –19
Poor sanitation also contributes strongly to stunting in children under five. A study by Das et al. in Bangladesh reports that there is a link between infectious diseases such as childhood rotavirus and diarrhea, climate factors, and the incidence of malnutrition in children under five. Infectious diseases are associated with the availability of clean water which is used as a source of drinking water, food processing, and personal hygiene such as hand washing and self-cleaning activities. Water polluted by bacteria increases the risk of transmitting infectious diseases to children under five. In addition, the availability of inadequate sanitation facilities such as the availability of inadequate latrines and inappropriate waste management at the household level are risk factors for the transmission of infectious diseases to children under five. The study also shows that climate factors, namely uncomfortable ambient temperature and humidity, average rainfall, and sea level pressure, are associated with the risk of developing infectious diseases in children under five. 20 In line with study by Permatasari et al. in rural area in Bogor district, Indonesia shows that most of the stunted children live in homes with poor sanitation conditions. Availability of clean drinking water sources and thermal comfort at home are related to stunting. Children under five who experience stunting mostly live in homes that have uncomfortable ambient room temperature (<20.5°C and >27.2°C) and home’s relative humidity (<40% and >70%). 16 Tusting et al. 21 reported that house conditions contribute to children’s growth. Poor housing conditions such as inadequate building conditions and thermal comfort at home are associated with the occurrence of malnutrition in children. 21 An increase in temperature exposure for 470 h above 30°C increased the risk of waste by 3% and stunting by 6%. 22
Stunting is a health problem that is associated with household characteristics. Li et al. 13 reported that children under five from poorest household wealth are 1.7 times more at risk of experiencing stunting than children under five from rich families. Malnutrition is generally more common in rural areas where economic conditions tend to be lower than in urban areas. 23 Differences in household characteristics can also be seen between urban and rural areas. A study by Cardenas et al. 23 in Colombia using data from the 2015 National Nutrition Situation Survey the Yun’s statistical decomposition technique reports that there is a city-rural gap in stunting of around 7.2 percentage points. This gap is influenced by three determinants which explain most of the gap in the occurrence of stunting, which is equal to 92%, where each factor which includes household wealth (54%), mother’s education (26%), and utilization of health services (12%) of the characteristic effect. 23 In line with study by Endris et al. 24 in rural Ethiopia with extracted from the 2014 Ethiopian Mini Demographic and Health Survey (EMDHS) by including a total of 3095 children aged 0–59 months showed that as many as 48.5% of children in rural areas experienced malnutrition caused by child’s age, mother’s education, region, and wealth status. In the study it was reported that more than half (50.5%) of children from poor families, where the households with poor economy can increase the occurrence of malnutrition in children under five in rural areas. 24 A similar study by Seboka et al. using Ethiopian Demographic and Health Survey for the survey 2005, 2011, and 2016 years showed that the risk of stunting was higher among older children, was in rural areas, had low birth weight, had mothers with underweight, and had parents without formal education. 25 Based on survey analysis in 2005, 2011, and 2016, it shows that the prevalence of malnutrition is high in rural areas, namely 57.35%, 54.32%, and 49.2%, respectively. In Indonesia, the results of Basic Health Research (2018) show that the prevalence of stunting is higher in rural areas (34.9%) than the prevalence of stunting under five in urban areas (27.3%). The results of Basic Health Research in Indonesia in 2018 show that the prevalence of stunting is higher in rural areas (34.9%) than the prevalence of stunting under five in urban areas (27.3%). Conditions are associated with economic and educational status, access to nutritious food intake, access to adequate sanitation facilities, and better nutrition and health services in urban areas than in rural areas. 26 Widyaningsih et al. 27 reported the results of data analysis from the Indonesian Family and Life Survey (IFLS) wave 5, conducted in 2014 that the prevalence of stunting was higher in children living in rural areas (children from poor families) than in urban areas (children from non-poor families). The factors of mothers who are short and have low education are factors that can increase stunting in both regions. Likewise, poor sanitation and nutrition services are also the main determinants of stunting in toddlers living in urban and rural areas. 27
The identification of the factors that cause stunting still needs to be proven, including information on sociodemographic conditions, nutrition, and sanitation. These three aspects have an important role in the occurrence of stunting in various countries, including in Indonesia. Analysis of these three aspects of the occurrence of stunting is needed as a basis for policy making and efforts to integrate nutrition-specific and nutrition-sensitive interventions that are appropriate in preventing stunting in children under five. Efforts to prevent stunting are simultaneously carried out in various countries including Indonesia, but data reported by UNICEF-WHO-World Bank Joint Child Malnutrition Estimates for 2021 shows that the reduction in stunting prevalence has not been evenly distributed. Most countries have shown progress in reducing the prevalence of stunting according to the target, but a few others have not shown good progress. 28 Therefore, WHO recommends strategies to prevent stunting through nutrition-specific and nutrition-sensitive interventions including improving sociodemographic conditions, nutrition, and sanitation. WHO also defines nutrition and sanitation as essential criteria in assessing children’s growth. 29 In Indonesia, various stunting prevention efforts have also been carried out such as the “Nutrition Awareness Family” program, a national movement in balanced nutrition practices, as well as other efforts carried out in a multi-sectoral manner that are adjusted to the multifactorial causes of stunting, especially related to sociodemographic conditions, nutrition and sanitation. 30 Therefore, this study aims to analyze the relationship between sociodemographic characteristics, nutrition, and sanitation on stunting in children under five in rural areas of West Java Province in Indonesia. These three factors have a main role in the occurrence of stunting in children under five. This research can strengthen scientific evidence regarding the role of sociodemographic, nutrition, and sanitation so that appropriate policies and interventions can be established to prevent stunting through the integration of nutrition-specific dan nutrition-sensitive interventions. This research is expected to contribute to reducing stunting rates in Indonesia, especially in rural areas.
Methods
Study area and period
West Java Province is in a strategic position adjacent to the national capital, namely DKI Jakarta Province. This province has a heterogeneous administrative area, consisting of areas with urban and rural characteristics. This study was conducted in Bogor District in West Java Province in Indonesia which is one of the areas with rural characteristics that has extensive agricultural and livestock land, where most of the population has a livelihood as farmers, ranchers, laborers, and a small number of others are private and government workers and employees. In study areas, raising livestock is one of the main livelihoods. In the study area shows that chicken and goat coops around the residents’ houses so the environment looks shabby and a lot of animal waste is found on the ground. Most homes have less sunlight, humidity, and poor ventilation. In addition, garbage is scattered in the empty garden area and burning garbage is often found around the road. Residential houses are mostly made of wood. There is a river that is also used for bathing, washing, and defecation. The population of Bogor District reaches more than 5 million people in 2019, where this number ranks highest in West Java Province, as well as the district with the largest population in Indonesia. Nearly 10% of the population are children aged 0–4 years, where the under-five mortality rate in this district is still high. 31 Bogor Regency is included in the 100 priority areas for stunting reduction in Indonesia which are carried out in an integrated (specific and sensitive) intervention. The prevalence of stunting in this region is in the high category based on the WHO category. 32 That is, almost a third of children under five are stunted in this region (32.9%) in 2018. This district has 40 sub-districts with some sub-districts including a stunting locus. 33
Design and samples
A cross-sectional study was conducted from May to August of 2022 in rural areas of West Java Province in Indonesia. The urban area is represented by Bogor City and the rural area is represented by Bogor Regency. A total of 247 pairs of mothers and children under five participated in this study. Participants came from one sub-district consisting of three villages as the locus of stunting. Participants who met the inclusion criteria and exclusion criteria were selected by systematic random sampling.
Inclusion and exclusion criteria
Participants in this study are mothers with children aged 0–59 months who have lived for at least six months or more in a rural area. Thus, the study could obtain homogeneous exposure to people’s lifestyles, as well as access to information and health services in rural areas. Other inclusion criteria were that the children were not undergoing intensive health care or suffering from serious illnesses that affect their nutritional status. The exclusion criterion ruled out children who had congenital abnormalities from birth.
Sample size determination
The sample was calculated using the one–sample test of proportions with a two-sided alternative hypothesis, with the following assumptions: 5% level of significance, 90% power, 32.0% undernutrition among rural children (P1) based on a previous study, and P2 10% smaller than P0,and 10% contingency for loss to follow-up. Therefore, the minimal size is 242. 34 in this study obtained as many as 247 mothers-child pairs.

Sampling technique and procedure
Participants were selected from urban and rural areas (three working areas of the community health center for each area). Eligible participants were selected using a systematic random sampling technique in illustrated Figure 1.
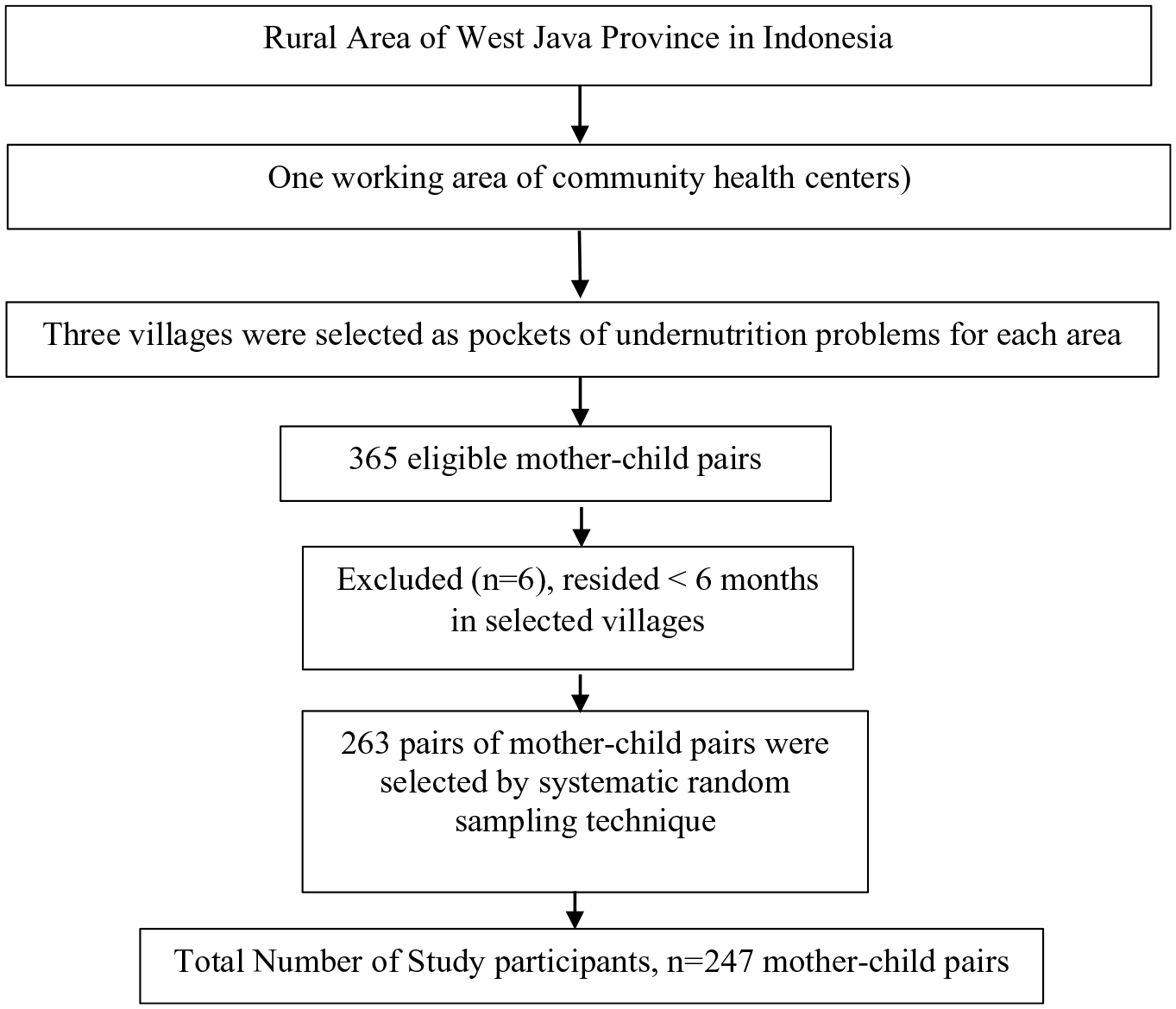
Sampling procedure of mother-child pairs.
Data collection and measurements
Sociodemographic characteristics
The structured questionnaire used to assess the sociodemographic including mothers and children characteristics was measured by direct interviews. In this study, the questionnaire used to assess the characteristics of mothers and children referred to a standard questionnaire, which was derived from the 2018 Basic Health Research questionnaire developed by the Ministry of Health of the Republic of Indonesia, where this questionnaire can be accessed and used in general without a license. 35
Mother’s characteristics
The mother’s age is categorized based on the mean age (35 years) of the mother, that is, (1) the mother’s age is below 35 years, or (2) the mother’s age is equal to or more than 35 years. A mother’s height is categorized based on the mean value, that is, (1) short, if the height is less than 150 cm, and (2) tall, if more than or equal to 150 cm. Mother’s education is categorized as (1) low, for those who never attended school and have a primary school education, or (2) high, for those who have at least a high school education. A mother’s employment status is grouped into (1) not working, and (2) working.
The level of family income is the amount of income received by the family per month. It is then grouped based on the regional minimum wage in Bogor District in 2022 (IDR 4,217,206), that is (1) low income, if less than the regional minimum wage, or (2) high income, if equal to or greater than the regional minimum wage. Parity is the number of children born to the mother, grouped into (1) primipara, if the mother has given birth to only one child, (2) multipara (mother has given birth to 2–4 children), and grand multipara (the mother has given birth to more than four children).
The mother’s nutrition knowledge questionnaire has been developed in this study and used, being valid and reliable. Prior to use, the questionnaire was reviewed through expert judgment, then validity and reliability tests were carried out with the number of respondents as much as 10% of the total number of study participants. Respondents who were involved in the validity and reliability tests came from other villages that had the same characteristics as the respondents in this study. Analysis was performed with SPSS Version 22.0, namely with Pearson Product Moment and Corrected Item-Total Correlation. Furthermore, the calculated r value is matched with the product moment r table at a significant level of 5%. If the r count is greater than the 5% r table. Then each item is declared valid. While the reliability test is carried out by assessing the value of Cronbach’s Alpha, which is stated to be reliable, if the calculation results (r count) are greater than the table value at a significant level of 5% (in this study, the corrected item-total correlation was between 0.712 and 0.756 and Cronbach Alpha was 0.857).
Data regarding the mother’s knowledge was measured by asking 20 questions about balanced nutrition and the undernutrition of children. Mothers were asked to answer with a choice of “true” or “false” for each statement. The sex of a child is categorized into (1) boy or (2) girl. A child’s age is categorized into (1) below 24 months or (2) equal to or more than 24 months. Immunization history is the provision of complete basic immunizations that must be given to infants from birth to 9 months of age and categorized into (1) ungiven, if the baby from the beginning of birth to the age of 9 months was not given any immunizations at all, (2) incomplete, if the baby had not been fully immunized and was not 9 months old, or (3) complete, if the baby was given all types of immunization from birth to 9 months of age. Early Initiation of Breastfeeding (EIB) is categorized into (1) No, if the baby was not given breast milk immediately after birth for the first hour, or (2) Yes, if the baby was breastfed immediately after birth until the first hour after birth.
Child’s characteristics
The anthropometric measurement using the length/height-for-age index was applied to assess stunted children. For children under 2 years old or unable to stand, length is measured using a SECA 210 length board with a measuring range of 10–99 cm and graduation (measuring rod) of 5 mm. Nutritional status categorization is the child’s growth standards according to WHO (World Health Organization). Based on the z-score, nutritional status was categorized into the following: severely stunted (<−3 SD); stunted (−3 SD to <−2 SD); normal −2 SD to +3 SD; tall (>+3 SD).36,37
Environment sanitation and clean living behavior
The questionnaire used to measure sanitation conditions refers to the 2018 Basic Health Research questionnaire developed by the Ministry of Health of the Republic of Indonesia and the Regulation of the Minister of Health of the Republic of Indonesia Number 1077/MENKES/PER/V/2011 concerning Guidelines for Air Sanitation in Home Rooms, it is stated regarding healthy home indicators, namely including efforts to improve indoor air pollution including efforts to improve physical, chemical and biological pollutant sources.35,38
Sources of drinking water were categorized into (1) Other than Gallon packaging, and (2) Gallon packaging. Water treatment were categorized into (1) No treatment, if the water used is not treated such as cooking it at boiling temperature before use, and (2) Yes, if cooked at boiling temperature before use. Meanwhile, information regarding the sanitary condition of the house includes building materials, floor conditions, walls, ceiling, ventilation, and potential housing conditions being disease-transmitting animals are asked according to the indicators of a healthy house, namely there are answer choices with categories (1) no, if the indicators for a healthy home meet, and (2) yes, if they do not meet the indicators for a healthy home.
Quality assurance of data collection
Three nutritionists served as data collectors and one supervisor has a job description in this study. Data collection was carried out directly via face-to-face interviews home visits by data collectors, and supervision to ensure the accuracy of data collection was conducted by supervisors. All instruments used in this study were calibrated before use. The questionnaire used was confirmed to have been reviewed by experts and tested for validity and reliability tests on 10% of the number of participants in other stunting loci that had similar characteristics to the study area. Once the data was collected, it was verified and checked for completeness by the data collector. Furthermore, the complete data will be verified by the supervisor and submitted to the research coordinator.
Data processing and analysis
All items in the questionnaire were checked for missing values, including mother’s and child’s characteristics, nutrition, and sanitation. Data was coded and input into statistics software using SPSS version 22.0. The bivariate analysis uses the chi-square test, where the variables are categorical data. A 95% confidence level and a value of p < 0.05 are used to assess statistical significance. Binary logistic regression analyses are used to analyze the dominant factors associated with stunting both in urban and rural areas.
Results
Table 1 shows the mothers and child’s characteristics. According to Table 1, out of 247 there is more than half of mothers have health insurance (59.9%) from the government, the majority of mothers (60.3%) mothers live in their own homes. A third of mothers educated up junior high school level (32.4%), 28.3% of mothers have senior high school levels education. Nearly half of fathers (43.7%) have an education at the senior high school level. The mother’s occupation is majority by the housewife (82.6%) while the father’s occupation is dominated by the laborer (41.3%). The percentage of family income below the regional minimum wage (80.2%) is higher than above the minimum wage (19.8%). Most of the mothers were multiparous and under 35 years of age (76.1%). The mother’s height is not much different between height <150 cm (51.4%) and 150 cm (48.6%). Nearly half of the mothers gave birth assisted by a midwife (43.3%). As many as 40.5% mothers consume less than 90 tablets of blood, and as much as 29.6% mothers does not consume blood supplementation (Fe tablets) during pregnancy. Sources of nutrition and health information were mostly obtained by mothers from the integrated service post cadre (55.9%). Most mothers made antenatal visits more than 4 times during pregnancy (69.2%) and midwives were the most sought-after health workers compared to other health workers. Decision-making in the family is largely the decision of the father and mother (64.0%). Most child development checks are carried out at the Integrated service post (74.1%). The mother’s nutritional knowledge in this study is mostly good (60.3%) and very good (39.7%).
Mothers and toddler’s characteristics (n = 247).

Characteristics of children under five obtained the sex of girls and boys are almost the same. Children aged over 24 years are more than those aged under 24 years. Almost all children have a normal birth weight above 2500 g (94.3%). The prevalence of stunting in this study was 20.7% (5.3% of children were severely stunted and 15.4% of children were stunted). Most of the children had a complete immunization history (55.5%) and did not have any history of infectious diseases such as diarrhea and acute respiratory infections (61.1%). Early initiation of breastfeeding and exclusive breastfeeding are carried out by most mothers. Most children are introduced to complementary food when they are over 6 months old (70.7%). Nutrition factors show that the practice of balanced diet is not carried out by most children (as much as 52.6% did not implement balanced diet at all, and 24.3% only applied a small portion of the practice). Consumption of energy (89.1%) and protein (87.4%) above 3 times a day is found in most children. More than half of mothers have implemented good parenting (53.1%). Sanitation factors show that the source of cooking water and drinking water is more than half using dug wells (50.2%), and for water treatment most of them do not carry out the processing (72.5%). As many as 39.7% of building materials are not easily overgrown with microbes/become a source of dust, 13% floor of their house does not meet the criteria for a healthy home, namely watertight and easy to clean), 19.8% walls does not meet the criteria for a healthy home, namely watertight and easy to clean, as many as 33.6% ceiling of their house does not meet the criteria for a healthy home, namely easy to clean and doesn’t collapse). ventilation (sufficient availability). In addition, most houses also do not have ventilation that meets the criteria for a house (64.2%).
Table 2 shows that the factors related to the incidence of stunting in children under 5 years old (p-value < 0.05) are maternal age, maternal height, type of delivery, age of toddlers, and vitamin A administration. Mothers aged over 35 years have more children. stunting compared to mothers under 35 years of age. Mothers with a height below 150 cm have more stunting children than mothers with a height above 150 cm. Mothers with normal delivery (induction) had more stunting children compared to mothers with normal (spontaneous) and cesarean section deliveries. Toddlers aged over 24 months have more stunting children than children aged under 24 months.
The factors associated with stunting under 5 years in rural area of West Java Province in Indonesia.

p value <0.05 (significant).
Furthermore, to see the dominant factors that influence the incidence of stunting, a bivariate selection was carried out. Variables included in the bivariate selection were variables with a p-value < 0.25, namely residence ownership status, mother’s education, parity, maternal age, maternal height, type of delivery, knowledge of maternal nutrition, age under five, LBW, infant age, MP- Breast milk, balanced nutrition practices, carbohydrate consumption, protein consumption, mother’s upbringing, and building materials are not easily overgrown with microbes/a source of dust. Then these variables are entered into the multivariate modeling stage. After experiencing several stages of modeling, the final multivariate model with binary logistic regression analysis was obtained as follows (Table 3):
Final model of binary logistic analysis.

Binary logistic regression analysis showed that the dominant factor influencing the incidence of stunting in children under 5 years of age was maternal height with an AOR of 2940 (95% CI: 1.333–6.484) which indicated that mothers with a height below 150 cm were about 3 times more at risk of having children with stunting compared with mothers who have a height above 150 cm. In addition, stunting is also influenced by the age of the child, where children younger than 24 months have a 0.250 times (95% CI: 0.104–0.598) time being prevented from experiencing stunting compared to children aged more than 24 months. Children who take vitamin A supplements regularly are 2 times a year. In the final multivariate model, it can be seen that balanced nutrition practices and building materials for child’ homes are confounding factors because they have a change in OR > 10% (Table 3).
Discussions
Stunting and influencing factors
The findings of this study indicate that the rates of stunting in children under five were 20.7%. This figure shows that the prevalence of malnutrition in this study is in the medium category, referring to the cut-off values for public health significance set by WHO. Based on the results of a study on the nutritional status of Indonesia in 2021, the findings in this study indicate that the prevalence of stunting under five is lower than the national rate. Stunting is still a priority to be addressed in Indonesia, including in rural areas. In this study, the most dominant factor associated with stunting is the mother’s height. Short mothers (height below 150 cm) have a 2.940 times greater risk of having stunting children than tall mothers (height equal to or more than 150 cm). This result is in line with a study in Northern Ghana, which showed that mothers who are less than 150 cm in height were about four times more likely to have stunted children than tall mothers. The short mothers who have experienced undernutrition in the past may experience macronutrient and micronutrient deficiencies during pregnancy and lactation, so they are at risk of having stunted children. 39 WHO categorized a mother’s height as less than 150 cm as short stature. This condition is associated with sociodemographic characteristics in the study area, where most of the families are poor, namely those whose income is below the regional minimum wage. Most of the mothers also had low education, that is, mothers generally had education up to the junior high school level. This low economic condition is the cause of low purchasing power of food. Mothers cannot afford nutritious food intake and have low diversity of consumption, so that they experience malnutrition for a long time, namely the period long before the period of pregnancy. The mother was unable to meet the needs of macro and micro nutrients at her past growth stages, which resulted in growth failure where this condition is characterized by short height. These results also strengthen the evidence that short mothers cause nutritional problems across generations, which increases the risk of having stunted children.
Previous studies have proven that mother’s dietary diversity from the past is associated with current nutritional status. Where the nutritional status of the mother, especially the mother’s height, is associated with the risk of stunting in toddlers. Dietary diversity is a major factor in fulfilling maternal nutrition, especially in the pre-pregnancy period, because no single food has complete nutrition to meet the nutritional needs of the mother. Dietary diversity is associated with socio-economic conditions and mother’s knowledge of the importance of balanced nutrition practices. 40
The other finding in this study shows that child’s age is also associated with stunting in children under five. Previous studies show that a child’s age has a high contribution to stunting. Older children aged 24–59 months are at a higher risk of stunting than younger children aged 0–24 months Stunting occurs when toddlers are malnourished during the first 1000 days of life. This stunting begins to appear when the baby is 2 years old. Inadequate feeding at this age leads to unfulfilled nutritional needs.31,32,41 This is also associated with an increase in children’s nutritional needs along with their growth due to increased physical activity as well. 42 Another similar study involving 330 toddlers in rural areas in West Java Province in Indonesia reported similar results, namely the prevalence of stunting in older toddlers (25–59 months) was higher (37.4%) compared to younger toddlers (0–24 months) that is as much as 17.6%. 16
Controversely, Das et al. reported his study involving 3578 children in 2014–2015 in Mumbai, India reported that 38% of toddlers aged 0–23 months were stunted. Of this percentage, children aged 0–11 months (52.0%) are slightly more stunted than older children aged 12–23 months (48%). This condition could be caused because in the study it was reported that at less than 11 months, the fulfillment of nutritional intake was low, especially during the breastfeeding period, where more than half of babies were not given early initiation of breastfeeding (55%), and more than a third (38%) babies do not get exclusive breastfeeding. 15
In line with the study conducted by Das et al., Titaley et al. 12 reported an analysis of data from the 2013 Indonesian Basic Health Survey, where the results showed that 33.7% of the 24,657 children who were analyzed were stunted under five. Titaley et al. reported that younger toddlers (0–24 months) are more at risk of stunting than older toddlers (more than 24 months). Apart from the age of the child, the study also reported that other predictors of stunting included household and housing characteristics, characteristics of the mother and father, and antenatal care services. 12
This study found that balancing diet practices is a confounding factor in stunting. A study conducted by Yunitasari et al. shows that stunting children come from families that provide wrong parenting and consumption that is not under balanced nutrition practices, where there is influence from the habit of consuming sweetened condensed milk is a significant contributor to malnutrition in children. Therefore, this study also reported that sanitation facilities, water treatment, and clean living behavior are determined by stunting. 43 Also, previous studies conducted in Indonesia showed that poor environmental sanitation conditions include building materials that are easily overgrown by microorganisms, as well as the lack of house ventilation. This condition is significantly associated with the incidence of pneumonia in children under five. Toddlers who experience infectious diseases such as pneumonia and tuberculosis are the direct cause of undernutrition including stunting.19,44 In addition, other home thermal comfort conditions such as the level of sunlight, temperature, types of walls, and ceilings are also sanitary factors that are associated with an increased risk of infectious diseases of the respiratory tract. 19 Strong scientific evidence showing the role of nutrition and sanitation in stunting is the basis for the need for appropriate prevention efforts from an early age, especially in the first 1000 days of life. 45 This research can strengthen scientific evidence regarding the role of sociodemographic conditions, nutrition, and sanitation in the incidence of stunting on children under five in rural areas. These three aspects are the determining factors for the occurrence of stunting, so the results of this study can be used as a basis for establishing appropriate policies and interventions to prevent stunting. Integration of nutrition-specific and nutrition-sensitive interventions that can be carried out to improve these three factors are: (1) sociodemographic factors, namely by improving economic conditions, for example, by optimizing the use of agricultural land which can increase family income to improve food purchasing power, (2) nutritional factors, namely by continuously educating parents, especially mothers regarding balanced nutrition practices and increasing skills in diverse food based on local food, and (3) conducting outreach programs regarding clean living behavior and assisting the community so that they can live in homes that meet the indicators healthy homes especially regarding the use of safe building materials (not easily overgrown by microorganisms). Fulfillment of these three aspects is also carried out by involving multi-sector cooperation from both the health and non-health sectors. Thus the results of this study can assist the target of reducing the prevalence of stunting in Indonesia, especially in rural areas.
Conclusions
The dominant determinant that causes stunting is the mother’s height. short mothers are 2.940 times more likely than tall mothers to have children who experience stunting. In addition, the child’s age also shows a significant association with stunting. There is a need for sensitive multi-sectoral nutrition interventions and specific nutrition interventions to improve the nutrition of mothers and children in the first 1000 days of life to prevent stunting in children under five
Limitations of the study
This study only uses one district in a rural area of West Java Province, Indonesia. However, it is necessary to expand the research location, so that it can represent conditions in the population.
Footnotes
Acknowledgements
We extend our highest appreciation and gratitude to all research respondents. We also thank the data collectors and supervisors for their outstanding contributions. We are grateful to cadres in the four villages who have helped during data collection in the community. We also thank The Health Office and the Faculty of Medicine and Health, University of Muhammadiyah Jakarta, for facilitating this research.
Authors’ contributions
TAEP: originated study ideas, drafted and designed research, performed statistical analysis and interpretation of results, and drafted a manuscript. The author reviewed and approved the manuscript. YCH and ERN: compiled and designed the study, providing direction and supervision in measuring environmental sanitation, analyzing and interpreting measurement results, and preparing the manuscript. FBE and BAP: supervise, and data analysis. The author reviewed and approved the manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We extend our highest appreciation and gratitude to all research respondents. We also thank the data collectors and supervisors for their outstanding contributions. We would like to thank the Lembaga Penelitian dan Pengabdian Universitas Muhammadiyah Jakarta, Faculty of Medicine and Health UMJ, IPB University, LLDIKTI Region III, Directorate of Research, Technology, and Community Service, Directorate General of Higher Education, Research, and Technology, Ministry of Education, Culture, Research, and Technology (Kemdikbudristek) Republic Indonesia have funding and supported implementation of Penelitian Dasar Unggulan Perguruan Tinggi (PDUPT) on the year 2022 with contract number 155/E5/PG.02.00.PT/2022.
Ethics approval and consent to participate
The Ethics Commission of Health Research of the Faculty of Medicine and Health, Universitas Muhammadiyah Jakarta, acceded to this study (approval number 115/PE/KE/FKK-UMJ/VI/2022). The Health Office of Bogor District and all community health centers in the study area also granted permission. All participants in this study expressed written consent and signed the consent form after obtaining complete information about the study. The data provided by participants were kept confidential by excluding personal identifiers from the data collection form. Participant convenience was a priority in this study during data collection, and we respected their rights as participants. The authors confirm that all methods were carried out under the relevant guidelines and regulations (Helsinki Declaration).
Patient consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Significance for public health
The finding of this research can strengthen scientific evidence regarding the factors that cause stunting which is used as the basis for determining policies and interventions to prevent stunting in children under five by integrating specific nutrition interventions covering nutritional aspects, and specific nutrition interventions covering non-nutritional aspects, especially sanitation.