
Abstract
Background:
Substance use and misuse have a negative impact on health care outcomes, specifically in the older adult population. Older adults are at risk due to several factors occurring toward the end of life such as changing family dynamics, loss of friends and loved ones, and chronic diseases. Substance use in older adults with chronic diseases in rural areas remains poorly studied. This study examines older adults greater than 55 of age in the state of Tennessee, U.S.A.
Design and methods:
Data was extracted from the 2019 National Behavioral Risk Factor Surveillance System (BRFSS) with a subsample for the State of Tennessee (N = 6242) and individuals over age 55 (N = 3389).
Results:
At least 33.7% (N = 1143) of older adults have a chronic disease, and 24.4% (N = 828) have at least two or more chronic diseases. Alcohol use in the past month was reported in 29.4% of older adults; however, chronic disease status was not associated with alcohol use. Marijuana use and smoking in the past month were significant for older adults with two or more chronic diseases. Low income and less high school education were associated with chronic disease and smoking.
Conclusions:
Marijuana use and smoking were found to be significant in older adults with chronic disease, but not with alcohol use. Preventative measures such as screening tools, education, and providing resources to patients should be targeted to populations at risk to promote overall health outcomes.
Background
Substance use and misuse has been known to negatively impact health care outcomes involving a variation of mental health disorders, nutritional deficiencies, and social and legal issues. An area of increasing concern is the elderly population as the “baby boomer” generation ages and advances in technology is increasing longevity. In 2018, almost 1 million adults greater than 65 years old were burdened with a substance use disorder. 1 Substances such as marijuana and alcohol can put older people at increased risk of respiratory conditions, diabetes, hypertension, congestive heart failure, memory impairment, mood problems, and liver and bone issues. 2 Nicotine is associated with an increased risk of cancer, respiratory conditions, and heart disease. 2 Addictive behaviors may stem from death of friends or a spouse, changing family dynamics, retirement, and worsening medical problems such as chronic illnesses. Illicit drugs may be misused in attempts to reduce psychological, physical, and emotional stress. 3
Chronic diseases such as chronic obstructive pulmonary disease, congestive heart failure, diabetes, hypertension, and chronic kidney disease are leading causes of health care expenses and are the leading causes of deaths in the U.S. 4 In addition, substance use disorders are contributing to rising death rates in 2016. 5 Though there is limited research, a recent study, using electronic health records from North Carolina, found that 48.3% were diagnosed with at least one chronic disease. The study found that patients diagnosed with at least one substance use disorder, were at higher odds for chronic disease. 6 Chronic illnesses may be the cause of substance misuse or can be exacerbated by substance use. Chronic diseases in the elderly can complicate management of substance use disorders and may mask symptoms of substance use making it difficult to diagnose and treat. 7 Older adults with chronic diseases and substance abuse are of increasing concern in rural settings.
Rural areas face unique challenges as they may lack access to health care needs, have higher poverty rates, and various cultural and social norms influencing health outcomes. 8 Management of chronic diseases may be a challenge as the elderly needs increased physician contact. 9 An average of one in five older adults greater than 65 years old live in rural areas. 10 Higher rates of substance use are significant in rural areas as they have limited resources in recovery, treatment, and prevention. As Tennessee is mainly rural populated (93%), an estimated 335,000–496,000 people greater than 26 years old reported using illicit drugs in the past month in 2019.10–12 No studies were found on substance use in the elderly population in Tennessee, Appalachian region, or Southeast U.S.
Older adults are heavily burdened with chronic diseases, and substance use is on the rise in this age group. Adults older than 65 comprise 15.2% of the US population which is one in every seven Americans. 13 Rural regions such as Tennessee are found to have higher incidents of substance use as well as older adults residing in these areas. Limited research was found examining older adults with chronic disease and substance use. To date, there are no studies on older adults with chronic conditions and substance use within Tennessee. As addiction with substance abuse is seen as a chronic relapsing condition, more research is needed to manage it as a chronic condition with care models to optimize health outcomes. In the current study, we will explore the association between chronic diseases and substance use among older adults in Tennessee.
Methods
Design
We used data from the 2019 Behavioral Risk Factor Surveillance System (BRFSS) conducted by the Centers for Disease Control and Prevention (CDC). The BRFSS is an annual collection of health-related telephone survey data from all 50 states, the District of Columbia and the three U.S. territories. Participants were randomly dialed on mobile phones and landlines and surveyed about health-related risk behaviors, chronic disease, and utilization of health services. The CDC de-identified data allowing it available for secondary analysis. The current study included all individuals aged 55 and older (N = 3389) in general population samples from the state of Tennessee (N = 6547). Per Code of Federal Regulations Common Rule 45, Institutional Review Board (IRB) review is not required for the study, since uses publicly available de-identified data.
Outcome variables
Our primary outcomes of interest include: (1) current alcohol use (2) current smoker (3) current marijuana use. Current alcohol use was based on participant report of past month alcohol use and coded binary, based on participant response. Participants were queried on their status as a current smoker with the following question: “Frequency of days now smoking,” and coded binary with 1 representing current smoker and 0 representing non-smoker. To assess marijuana use, participants were queried on the following: “During the past 30 days, on how many days did you use marijuana or hashish?” Participants who reported one or more days of smoking marijuana in the past month were categorized as current marijuana users, while those who did not smoke marijuana in the past month were coded as non-users.
Independent variables
To assess chronic disease status, participants were queried if they have ever had any of following diseases: cancer, diabetes, heart disease, COPD, and chronic kidney disease. An index score was used to calculate the number of chronic diseases from 0 to 5, based on the sum of the number of chronic diseases. Chronic disease was dummy coded into three variables including (1) two or more chronic diseases, (2) one chronic disease, and (3) no report of chronic disease (referent group).
Controls
Household income, educational attainment, age, gender, and race were used as controls in our analysis. Household income was coded binary as: <$35,000 per year, and ≥$35,000 per year. Education was coded binary as: did not complete high school, and completed high school. Gender was coded dichotomously for male and female. Race/ethnicity was dummy coded into the following race groups: White-Non-Hispanic (referent), Black Non-Hispanic, Hispanic, Asian, and other race/ethnicity. Numeric age of the participant was also included in the model as a control variable.
Analysis
Descriptive statistics for the sample are presented in Table 1. Logistic regression analysis was used to assess the association between chronic disease status and three outcomes including: (1) current alcohol use (2) current smokerer (3) current marijuana use. Each outcome was assessed separately. The following independent variables were included in the model: Two or more chronic disease, one chronic disease, along with controls. Table 2 presents results from the logistic regression model, using current alcohol use as the primary outcome, while Table 3 used current smoker as the primary outcome. All analyses were conducted in STATA 15.1 (Copyright 1985-2017 StataCorp LLC).
Descriptive characteristics of sample (N = 3389).
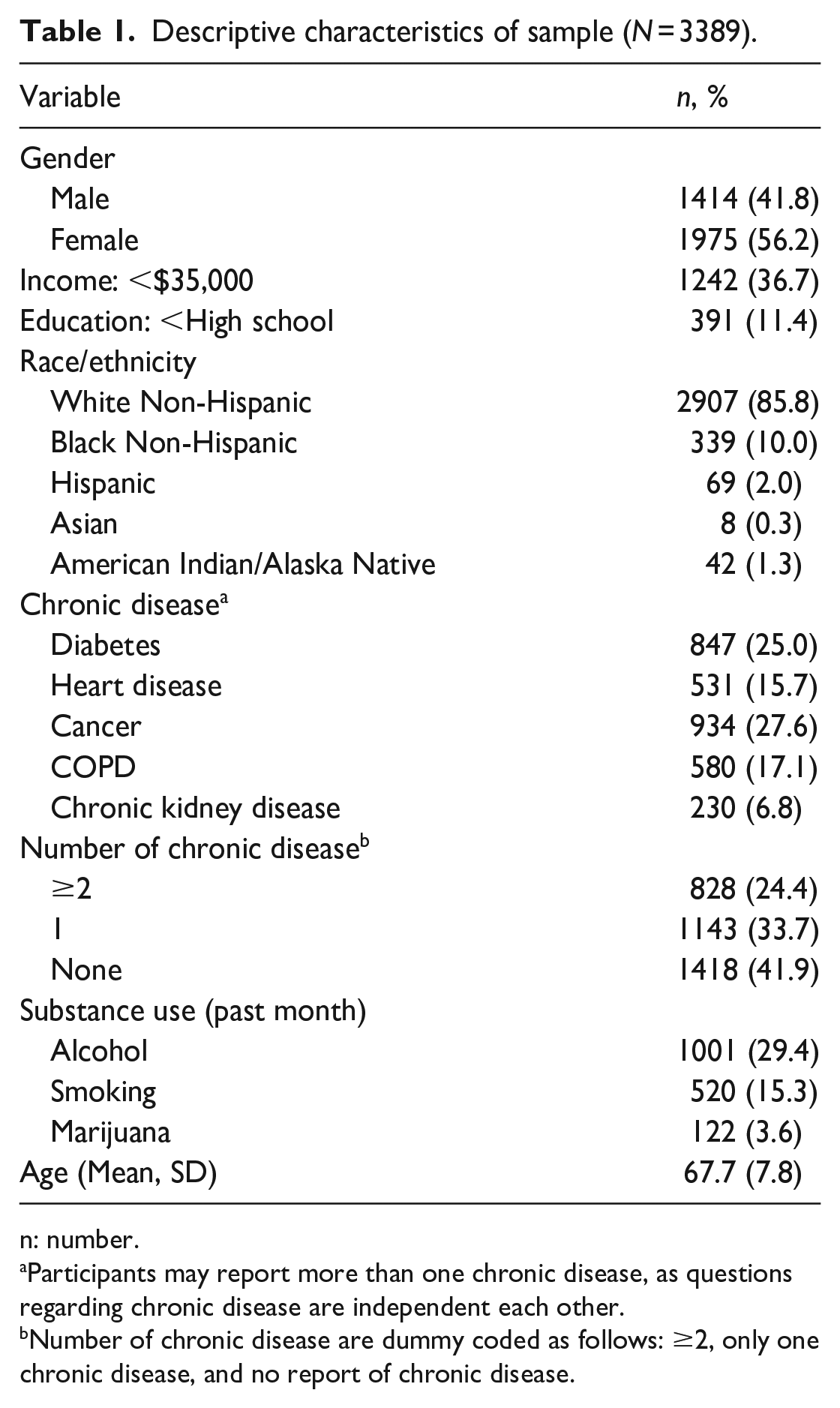
n: number.
Participants may report more than one chronic disease, as questions regarding chronic disease are independent each other.
Number of chronic disease are dummy coded as follows: ≥2, only one chronic disease, and no report of chronic disease.
Association between chronic disease status and past month alcohol use.

CI: confidence interval; OR: odds ratio; Significant values are marked in bold.
p < 0.05.
Association between chronic disease status and past month smoking.

CI: confidence interval; OR: odds ratio; Significant values marked in bold.
p < 0.05.
Results
Descriptive statistics were presented in Table 1. Overall, 24.4% (N = 828) reported two or more chronic disease, while 33.7% (N = 1143) reported one chronic disease, and 41.9% (N = 1418) did not report any level of chronic disease. Current substance use included 29.4% that were current drinkers, 15.3% identified as current smokers, while 3.9% reported past month marijuana use.
The association between chronic disease and alcohol use was presented in Table 2. Participants with two or more chronic diseases were at lower risk for current alcohol use (AOR = 0.49; 95% CI, 0.39, 0.61, p < 0.001). Current smoking as an outcome was presented in Table 3. Two or more chronic diseases (AOR = 1.61; 95% CI, 1.26, 2.04, p < 0.001) and one chronic disease (AOR = 1.30; 95% CI, 1.03, 1.69, p = 0.04) were associated with higher odds of current smoking. Marijuana as an outcome was presented in Table 4. Two or more chronic diseases predicted higher odds of marijuana use (AOR = 1.77; 95% CI, 1.12, 2.79, p = 0.01), while one chronic disease was not associated with current marijuana use.
Association between chronic disease status and past month marijuana use.

CI: confidence interval; OR: odds ratio; Significant values are presented in bold.
p < 0.05.
Discussion
Substance use and misuse are a growing healthcare concern, specifically with the older adult population. Substance abuse has negatively impacted health care outcomes putting the elderly at increased risk for respiratory conditions, diabetes, hypertension, congestive heart failure, memory and mood instability, as well as several other diseases. 2 The findings from this study demonstrate the correlation between substance use among older adults with chronic diseases in Tennessee. This is consistent with an earlier study demonstrating more than half of the older adult population with a chronic disease, and substance use was significantly associated with chronic diseases. 6 No prior research was found on chronic disease and substance use in Tennessee among older adults. Rural areas represent a healthcare disparity due to a lack of healthcare access and higher poverty rates. 8 As substance misuse and chronic diseases have heightened levels of healthcare costs and deteriorating health impacts, more studies are needed to address interventions and optimize individual outcomes.
Our findings specific to Tennessee and substance use including smoking, marijuana, and alcohol expand on prior studies of older adults and substance misuse. The study found that marijuana use in the past month was significant for older adults with two or more chronic diseases. Results determined that nearly one in four older adults have two or more chronic diseases. Prior research concluded that people with substance use disorders have increased risk of having medical comorbidities.14,15 Screening and educating patients on substance misuse should be conducted by clinicians in primary care visits and should not be overlooked in the older adult population. However, there appears to be a stigma associated with substance misuse and that treatment is not necessary for older adults. 16 Barriers associated with patients and providers have been identified in prior studies including the discomfort of screening patients and the patient’s feeling of shame surrounding substance use.16–18 As the findings of this study have shown older adults with chronic disease have a significant association with substance misuse, attention is warranted.
In the current study, nearly 30% of older adults reported past month alcohol use. To surprise, alcohol use was found to be associated with a lower risk of two or more chronic disease statuses and alcohol use in this sample. Additionally, findings show that having a chronic disease revealed an increased association with smoking. The survey question specifically asks about smoking in the previous month, but the patient may have smoked at a young age that was not a direct result of the chronic disease. The survey question was not explicit in whether the person was taking prescribed forms of marijuana. Some cancer patients take medical marijuana, or dronabinol, a form of marijuana, to stimulate their appetite and relieve nausea. 19 This would not be categorized as a form of substance abuse. These findings are similar to those of another study that used data from the US National Survey on Drug Use and Health and discovered an increase in substance use rates among adults with one or more chronic conditions. Cigarette smoking was the most commonly reported, and it was linked to anxiety, depression, and substance abuse. 20
Low income and a low high school education seem to be common factors associated with chronic disease and smoking.21,22 Similar to our findings, people experiencing financial difficulties was associated with substance misuse. 22 Further, older adults having lower education increased the incidence of substance use.23,24 As it has been well established that rural areas face challenges to adequate health care needs and higher poverty rates, 8 screening older adults in rural, underserved areas may increase awareness to older adults misusing substances. Early prevention on substance use and its effects on health outcomes is essential in each patient encounter. Provider education should be directed to decrease stigmatization when discussing substance use with older adults.
There are several strengths of the study including use of a national database with responses from a large representative sample including individuals from various races, ethnicity, and age groups. The novelty of the research findings is specific among older adults as there are not many studies of substance use in this population. Additionally, substance use data is from the past 30-day use, reflecting current trends. Another strength is that the study examines a state with poor overall health which may lead to targeted interventions.
Our findings should be interpreted with caution, given the following limitation. First, The BRFS surveys used a pre-established database and pre-determined survey questions, limiting the ability to determine variables, and data is cross-sectional. Second, the BRFSS survey demonstrated self-reported bias which is based on participants instead of screening individuals. Third, there is election bias to adults who speak English or Spanish only, and other languages spoken were not included in the survey. Only five chronic diseases were reported, and not all substances were included such as heroin, cocaine, and opioids. Fourth, the results reflected substance use only within the past month, and does not consider past year or lifetime use. Fifth, there exists a risk for underreporting of marijuana use as the recreational or medical use of marijuana is currently prohibited in the state of Tennessee. A previous study examining marijuana use prior to and after legalization suggested that, when survey participants are questioned, marijuana use may be underreported due to fear of legal consequences or its designation as an illicit substance. 25 Previous research has also suggested a greater prevalence of underreporting of individuals ages ≥30 associated with changing family roles and social stigmatization of substance misuse; however, these conclusions are not absolute.26,27 Finally, the study does not assess the magnitude or length of the chronic disease leading to inconsistent measures. Future research omitting variables with specific questions regarding substance use may help determine the significance with chronic disease status.
Future directions
Research
Further studies examining substances specifically with opioid use, sedatives, and non-medical prescriptions may help determine an association with the older adult population. As older adults are more likely to experience pain with chronic diseases such as Degenerative Joint Disease and neuropathy, they may be prone to misusing opioids and sedatives other than prescribed. Some older adults have experienced trauma over their life which increases their risk of substance use related to degenerated physical pain exposing them to opportunities to misuse opioids. 28 Not many studies were found targeting older adults, and this population is at risk of substance use from their chronic illnesses, changing social and family dynamics, and death of friends of family leading them to find ways to cope. Tennessee data may be compared with national data on substance use and chronic diseases in the elderly as there may be more areas of the U.S. at risk. As we know chronic diseases are associated with substance use among older adults, researchers may compare which diseases and gender is associated with a higher risk. Future studies should address timing of onset of chronic disease and substance use as well as other factors including length of disease, magnitude, and burden of the disease. Solutions for substance use should be investigated despite multiple chronic diseases in the older adult population.
Practice
Health clinicians should screen and assess older adults at risk for substance use. In addition to depression screenings, substance use screenings such as Tobacco, Alcohol, Prescription medication, and other Substance use (TAPS) tool was developed to briefly screen primary care patients. 29 The U.S. Preventative Services Task Force recommends clinicians to screen for alcohol misuse and briefly provide counseling and interventions for those engaged in risky drinking to reduce alcohol misuse. 30 The National Institute of Drug Abuse (NIDA) is a quick screen for substance use disorders including alcohol, tobacco, prescription drugs for non-medical reasons, and illegal drugs. 31 Risk of underreporting for substance use may be mitigated by requesting patients confirm previous responses. 26 Screening may help educate those at risk and prevent substance misuse. Each patient encounter provides an opportunity for a clinician to educate patients on the harms of substance use, provide counseling, medications, and refer for community resources. Clinics may have pamphlets or bulletins to provide education for substance misuse and how to seek counseling by offering websites or providing 24/7 hotlines. The provider should assess their literacy level to ensure education effectiveness. Education may be directed toward promoting healthy lifestyle choices with chronic disease patients as well as how substance use negatively affects one’s health. Providers should openly discuss whether low income is a deciding factor in health care such as working with insurance approvals for therapy sessions and using online coupons for medications. Implementing telehealth by videoconferencing with a clinician or messaging via emails may increase access to care, especially in rural areas. 32
Routine follow up and telephone calls may encourage a trusting patient-provider relationship and reduce the stigma associated with substance misuse discussions. As patients should be educated on substance use, so should providers. Substance misuse may display atypical or non-specific symptoms in older adults complicated by the presence of comorbidities or similarities to common aging-related issues. 33 Providers must maintain both a communicative relationship with patients and knowledge of substance misuse warning signals in older adults. Online webinars, educational modules, and toolkits are available for clinicians including guidance of long-term opioid therapy, withdrawal protocols, and medications for alcohol use disorders. 34 Organizations may provide training for providers on substance use protocols and how to perform motivational interviewing.
Conclusion
Our findings demonstrate more than half of older adults have a chronic disease, and there is an association between substance use and chronic disease in older adults. Smoking and marijuana use were significant with chronic diseases though it negatively impacts health care outcomes. Preventative measures including screening tools are essential to detect those at risk of substance use and provide necessary education and resources to patients. Populations at risk of substance use are older adults, those with chronic diseases, and those residing in rural areas. Patient education should be aimed at reducing and refraining from substance use as well as ensuring they have appropriate community resources. Health care clinicians should have applicable knowledge in screening patients and treat those at risk. As older adults are living longer and have chronic illnesses, risks for substance use need to be explored. More research is needed on older adults and substance use and deciphering which chronic diseases pose the most risk for negative health care outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.